
Abstract
Urothelial carcinoma is the sixth most common cancer type in the United States. Although most patients present with early stage disease which is associated with improved outcomes, many will progress to locally advanced or metastatic disease. Immune checkpoint inhibitors have significantly impacted the treatment paradigm for patients and have resulted in improved survival rates. Despite their proven efficacy, many ongoing clinical trials continue to refine combinations with chemotherapy, sequencing of therapies and the role of ligand expression. Additionally, novel targets have been identified for advanced urothelial carcinoma and have led to the approval of the antibody-drug conjugate, enfortumab vedotin, and the fibroblast growth factor receptor-targeted, erdafitinib. Enrollment in a clinical trial is strongly encouraged for all stages of advanced or metastatic disease. Numerous ongoing clinical trials are likely to impact the treatment armamentarium for patients. In this manuscript, we highlight key updates in the clinical management for patients and outline ongoing trials.
Urothelial carcinoma (UC), a common genitourinary cancer, is the sixth most common cancer type comprising 4.5% of all new cancer cases and 3% of cancer-related deaths in 2020. 1 Despite effective treatments for early stages of disease, non-muscle invasive and muscle-invasive, many patients progress to advanced or metastatic UC (mUC). 2 In recent years, the role of immunotherapy for the management of mUC has become widely utilized, yet, as data matures the agent of choice, sequencing of therapies, and ligand-expression become a complex topic. Additionally, UC being one of the top mutated cancers, several therapeutic targets and combinations are likely to impact the treatment armamentarium. 3 , 4 Our prior reviews have highlighted numerous updates in the management of locally advanced and mUC; however, multiple trials have significantly impacted treatment selection and ongoing trials are likely to affect the treatment of patients with metastatic disease.5–8 This manuscript will provide a high-level overview of selected late-phase trials in patients with UC.
Immune checkpoint inhibitors for urothelial carcinoma: Landmark trials
Keynote-057: Pembrolizumab for early-stage urothelial carcinoma
Despite the extensive role of immune checkpoint inhibitors (ICIs) for locally advanced and mUC, the Keynote-057 trial (ClinicalTrials.gov identifier NCT02625961) demonstrated efficacy of pembrolizumab in patients with non-muscle invasive bladder cancer (NMIBC). On January 8, 2020, pembrolizumab was approved by the Food and Drug Administration (FDA) for the treatment of patients with Bacillus Calmette-Guerin (BCG)-unresponsive, high-risk, NMIBC with carcinoma in situ (CIS) with or without papillary tumors who are ineligible for or have elected not to undergo cystectomy. 9
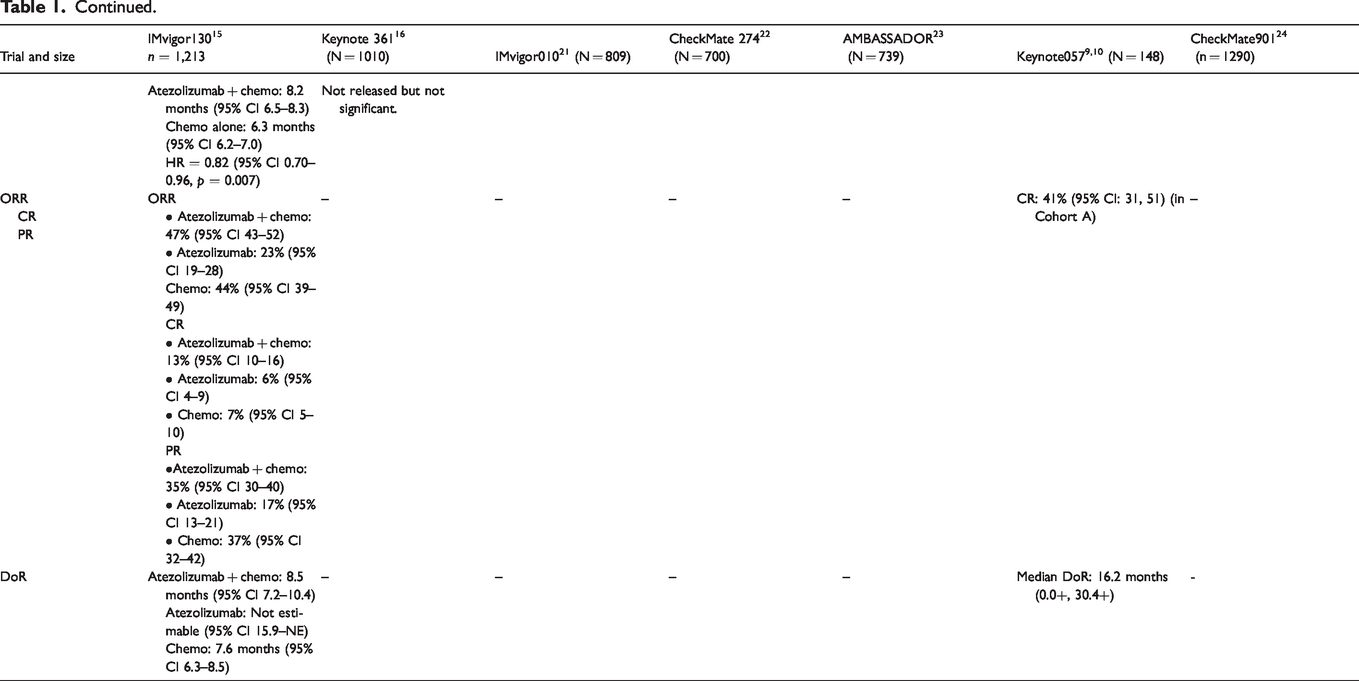
Keynote-057, a multicenter, single-arm trial enrolled 148 patients with high-risk NMIBC, 96 of whom had BCG-unresponsive CIS with or without papillary tumors. Patients received pembrolizumab 200 mg every 3 weeks until unacceptable toxicity, persistent or recurrent high-risk NMIBC or progressive disease, or up to 24 months of therapy without disease progression. 9 , 10 The major efficacy outcome measures were complete response (CR), urine cytology, and computed tomography urography and duration of response (DoR). The CR rate in the 96 patients with high-risk BCG-unresponsive NMIBC with CIS was 41% (95% CI: 31, 51) and median response duration was 16.2 months (0.0+, 30.4+). Forty-six percent of responding patients experienced a complete response lasting at least 12 months.
To date, there is no data to demonstrate efficacy outcomes in patients who may have had pembrolizumab for early-stage NMIBC who later require treatment for advanced, mUC with an ICI.
JAVELIN Bladder 100: Avelumab maintenance for advanced urothelial carcinoma
On June 30, 2020, avelumab was granted FDA approval for the maintenance treatment of patients with locally advanced or mUC that has not progressed with first-line platinum-based chemotherapy, based on the results of the JAVELIN Bladder 100 trial (NCT02603432). 11 JAVELIN Bladder 100 is a phase III, multi-center, multinational, randomized, open-label, parallel-arm study that evaluated anti-PD-L1 immunotherapy, avelumab, as maintenance therapy following first-line platinum-based chemotherapy in patients with advanced UC. 11 , 12 The trial enrolled 700 patients with unresectable locally-advanced or mUC that achieved response or stable disease after four to six cycles of platinum-based chemotherapy (gemcitabine with either cisplatin or carboplatin). Eligible patients were randomized 1:1 to receive maintenance avelumab (10 mcg/kg IV every 2 weeks) with best supportive care (BSC) or BSC alone, initiated within 4-10 weeks after the last chemotherapy dose. Enrolled patients were stratified by the presence of visceral vs non-visceral disease when initiating first-line chemotherapy and best response to first-line chemotherapy (partial/complete response vs stable disease). The primary efficacy outcome measure was overall survival (OS) in all patients and in patients with PD-L1-positive tumors, as identified by the Ventana SP253 assay. The secondary outcomes included progression-free survival (PFS), objective response rate (ORR), and safety measures.
Of the 700 patients randomized to maintenance avelumab and BSC (n=350) or BSC alone (n=350), 51% (n=358) had PD-L1-positive tumors. 11 , 12 Study participants in the maintenance avelumab and BSC and BSC alone treatment groups were followed for 19.6 and 19.2 months, respectively. The median OS for the avelumab and BSC arm and BSC alone arm was 21.4 months and 14.3 months, respectively (HR, 0.69; 95% CI, 0.56, 0.86; P=0.001). This demonstrated a significant prolongation in OS for the avelumab and BSC arm vs BSC alone. In patients deemed PD-L1-positive, avelumab and BSC also significantly prolonged OS vs BSC alone (HR 0.56; 95% CI, 0.40, 0.79; P<0.001). For the 39% of patients with PD-L1-negative tumors, an exploratory analysis was performed to determine OS (HR 0.85; 95% CI, 0.62, 1.18). A benefit in OS was observed across all subgroups included in the trial. A blinded, independent, central review determined the PFS with avelumab and BSC vs BSC alone in all randomized patients (HR 0.62; 95% CI 0.52, 0.75) and in patients with PD-L1-positive tumors (HR 0.56; 95% CI 0.43, 0.73). In the study arms treated with avelumab and BSC vs BSC alone, the most common adverse effects grade ≥3 were urinary tract infection (4.4% vs 2.6%), anemia (3.8% vs 2.9%), hematuria (1.7% vs 1.4%), fatigue (1.7% vs 0.6%), and back pain (1.2% vs 2.3%). All-causality adverse effects were reported at grade ≥3 in 47.4% vs 25.2%, and at any grade in 98.0% vs 77.7% of patients randomized to the avelumab plus BSC arm vs BSC alone arm, respectively. In the patients that received avelumab, 28% had serious adverse reactions and one died from sepsis. The dose of avelumab recommended is 800 mg as an intravenous infusion over 60 minutes every 2 weeks until disease progression or unacceptable toxicity. 13
This landmark trial is likely to have a significant impact on the current standard of care for first-line treatment of advanced mUC due to significant benefits observed in OS and PFS across all sub-groups and regardless of PD-L1 expression. This is, also, likely to limit the use of ICIs in the second line-setting if avelumab is used as maintenance treatment. To date, atezolizumab, nivolumab, durvalumab, avelumab, and pembrolizumab are all approved second-line options with pembrolizumab being a Category 1 option by the National Comprehensive Cancer Network due to OS benefit in the Keynote-045 trial. 2 , 5 , 6 , 14
Keynote-361 and IMvigor130 updates: Pembrolizumab and atezolizumab for front-line advanced urothelial carcinoma
The Keynote-361 study (NCT02853305) is a phase 3, randomized, open-label trial that is evaluating the efficacy and safety of pembrolizumab as monotherapy or in combination with chemotherapy versus chemotherapy alone in patients with unresectable or mUC. Similarly, the IMvigor130 trial (NCT02807636) is a phase 3, randomized, double-blind, placebo-controlled study investigating the efficacy and safety of atezolizumab (a PD-L1 inhibitor) as monotherapy or in combination with chemotherapy versus chemotherapy alone in patients with previously untreated locally advanced or mUC. Initially, both of these trials limited the approval for pembrolizumab and atezolizumab in the front-line setting requiring either PD-L1 positivity in patients who are cisplatin-ineligible or for any patient who is platinum-therapy ineligible. 6
Recently, results of IMvigor130 demonstrated no significant difference in OS for atezolizumab with or without platinum-based chemotherapy compared to platinum-based chemotherapy alone, regardless of PD-L1 status. 15 However, IMvigor130 did show increased PFS in patients receiving atezolizumab with platinum-based chemotherapy compared to platinum-based chemotherapy alone (8.2 months [95% CI 6.5, 8.3] vs. 6.3 months [95% CI 6.2, 7.0], respectively; HR for death =0.82 [95% CI 0.70, 0.96, p = 0.007]). Duration of response were comparable in the chemotherapy-containing regimens with or without atezolizumab (8.5 months [95% CI 7.2, 10.4] vs. 7.6 months [95% CI 6.3-8.5], respectively), while the median DoR for the atezolizumab monotherapy group was not estimable at conclusion of the trial. Similarly, on June 9, 2020 Merck & Co. released an update to Keynote 361 stating that pembrolizumab in combination with chemotherapy failed to show improved OS or PFS when compared to chemotherapy alone. 16 Testing of the monotherapy arm was not completed due to the combination arm failing to show superiority in its primary endpoints. There was no new safety information to report as the safety profile was similar to previous studies.
Other notable trials
DANUBE (NCT02516241), a phase 3, randomized, open-label, active-controlled study, evaluating the efficacy and safety of durvalumab monotherapy and durvalumab in combination with tremelimumab (CTLA-4 Inhibitor) versus SOC chemotherapy in previously untreated patients with unresectable, stage 4 UC reported that the trial did not meet the primary endpoints for patients with high levels of PD-L1. 17 , 18 Durvalumab monotherapy did not improve OS versus SOC chemotherapy and durvalumab plus tremelimumab did not improve OS versus SOC chemotherapy
CheckMate901 (NCT03036098) is phase 3, randomized, open-label trial evaluating the efficacy and safety of nivolumab in combination with ipilimumab in combination with standard-of-care (SOC) chemotherapy versus SOC chemotherapy alone in patients with previously untreated inoperable or meUC. 19 An estimated 1290 participants will enroll in the trial. The primary outcomes of the study are: OS in cisplatin-ineligible randomized patients, OS in PD-L1-positive (≥1% by immunohistochemistry) randomized patients, PFS by blinded independent central review (BICR) in cisplatin-eligible patients, and OS in cisplatin-eligible patients. Primary completion of the of this trial is anticipated in January 2023.
NILE (NCT03682068), a phase 3, randomized, open-label, active-controlled trial is evaluating the efficacy and safety of durvalumab in combination with SOC chemotherapy or durvalumab in combination with tremelimumab and SOC chemotherapy versus SOC chemotherapy alone in patients with unresectable locally advanced or mUC. 20 An estimated 885 patients will be enrolled in the study. The primary endpoints of the NILE study are PFS and OS. Primary completion of the study is anticipated in April 2022.
Select trials evaluating the role of ICIs for UC are outlined in Table 1.
Select ongoing trials of immune checkpoint inhibitors for urothelial carcinoma.
Antibody drug conjugates for urothelial carcinoma
EV-103: Enfortumab vedotin monotherapy and combinations for muscle-invasive and metastatic urothelial carcinoma
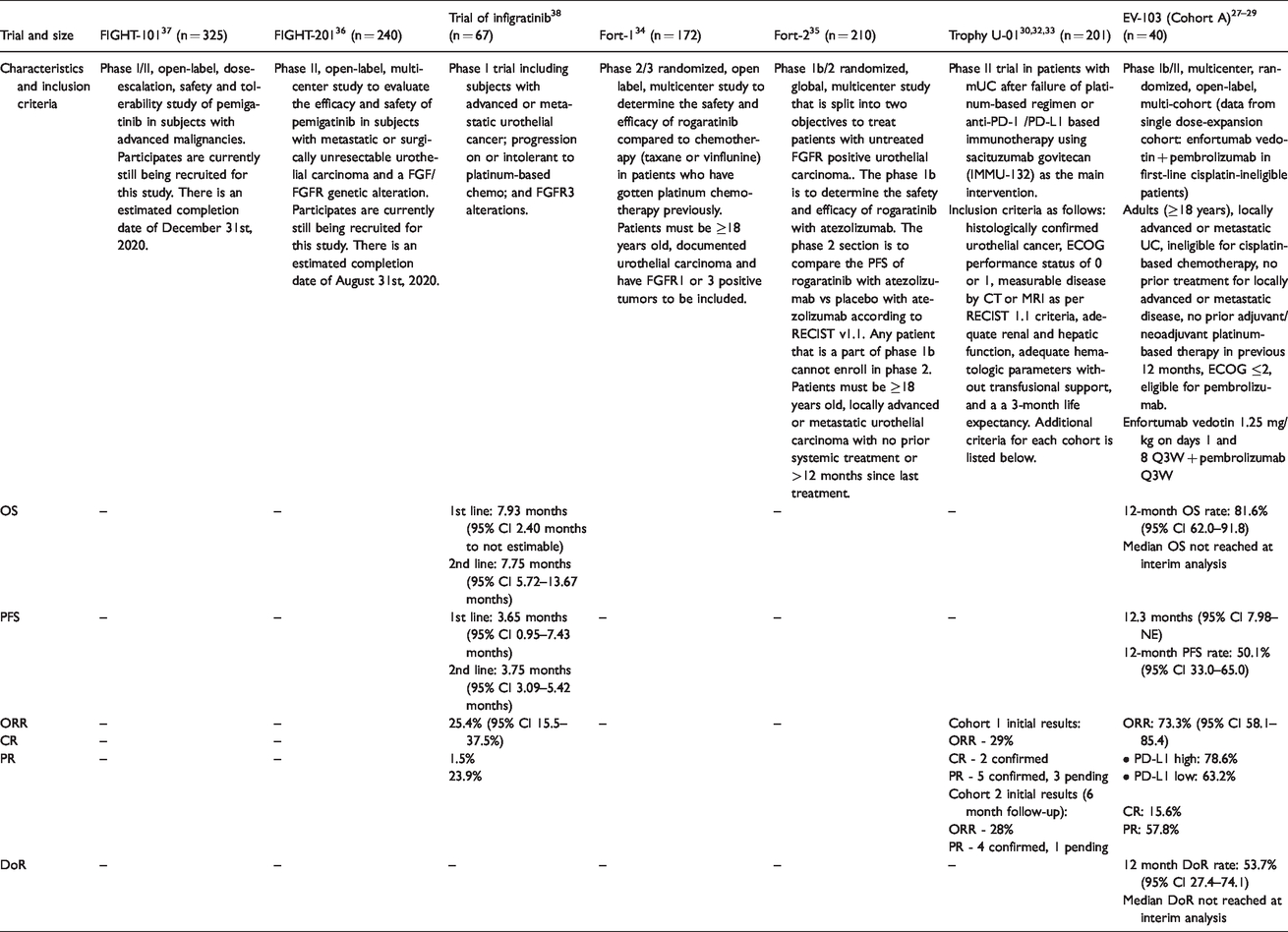
Enfortumab vedotin, an antibody-drug conjugate targeting the cell surface protein nectin-4 and linked monomethyl auristatin E, was first approved in December 2019 for use in adult patients with locally advanced or mUC who have previously received a PD-1 or PD-L1 inhibitor and platinum-based chemotherapy in the neoadjuvant, adjuvant, locally advanced, or metastatic setting based on the findings from EV-201. 25 , 26 An ongoing phase Ib/II cohort trial, EV-103 (NCT03288545), is evaluating safety and efficacy of enfortumab vedotin in patients with locally advanced or mUC either alone or as part of a combination regimen.27–29 Separate cohorts in EV-103 are evaluating survival and response rates when treated with enfortumab vedotin monotherapy or enfortumab vedotin plus pembrolizumab, cisplatin, carboplatin, or gemcitabine. Preliminary results from a single dose-expansion cohort of 40 participants receiving first-line enfortumab vedotin plus pembrolizumab show a 12-month OS rate of 81.6% (95% CI 62.0, 91.8), while the median OS was not reached at the time of analysis. Median PFS was 12.3 months (95% CI 7.98, NE) with a 12-month PFS rate of 50.1% (95% CI 33.0-65.0). The study also demonstrated promising response rates and durability, with an ORR of 73.3% (95% CI 58.1-85.4) and 12-month DoR rate of 53.7% (95% CI 27.4-74.1). Median DoR was not reached at the interim analysis point. Of the responders, 15.6% had a complete response and 57.8% had a partial response. Rate of response was slightly higher in patients with high PD-L1 expression (ORR = 78.6%) compared to patients with low PD-L1 expression (ORR = 63.2%). EV-103 is ongoing with an estimated primary completion date of July 2023.
TROPHY U-01: Sacituzumab govitecan for metastatic urothelial carcinoma
TROPHY U-01 (NCT03547973), a phase 2, multicenter, open-label, parallel trial is evaluating the efficacy and safety of sacituzumab govitecan in patients with metastatic urothelial carcinoma after failure of a platinum-based regimen and/or anti-PD-1/L1-based therapy. An estimated 201 patients will enroll in the study. 30 Sacituzumab govitecan (IMMU-132) is an antibody-drug conjugate with a humanized anti-Trop-2 monoclonal antibody attached to SN38. 31 Trop-2 is a cell surface glycoprotein that is highly overexpressed by a variety of epithelial carcinomas with limited expression in normal tissues. SN38 is the active metabolite of irinotecan, a cytotoxic chemotherapy drug. When the antibody binds to Trop-2 on the surface of cancer cells, the toxin is internalized, which results in cell death. The study consists of two arms: sacituzumab govitecan (IMMU-132) 10 mg/kg intravenously on Days 1 and 8 of a 21 day cycle, and sacituzumab govitecan (IMMU-132) 10 mg/kg intravenously on Days 1 and 8 of a 21 day cycle followed by pembrolizumab at the standard dose (200 mg) only on Day 1 of a 21 day cycle. 30 The first arm is subsequently divided into two cohorts: cohort 1 consists of subjects with UC, after platinum-based regimen (cisplatin or carboplatin) and anti-PD-1/anti-PD-L1 based therapy and cohort 2 consists of subjects in second line therapy of urothelial cancers, ineligible for platinum-based therapy and anti-PD-1/anti-PD-L1 based therapies failure. Cohort 3 is interchangeable with the second arm and consists of subjects who have had progression or recurrence of UC following a platinum-containing regimen in the metastatic setting, or progression or recurrence within 12 months of completion of platinum-based therapy as neoadjuvant or adjuvant therapy. The primary endpoint of this study is ORR. Primary completion of the study is anticipated in September 2021.
Initial results for cohort 1 of the TROPHY U-01 trial were presented at the 2019 European Society for Medical Oncology Congress. 32 Thirty-five patients in cohort 1 with at least 1 post-baseline response assessment were evaluated at a median 4.1 months follow-up. At the time of this pre-planned interim analysis, the ORR was 29% (n = 10/35). There were 2 confirmed CR, 5 confirmed PR, and 3 unconfirmed PR (all awaiting radiographic confirmation).
Early results of cohort 2 at median follow-up of 6 months, ORR was 28% (5/18) with 4 confirmed PRs, and 1 PR pending confirmation. 33 The majority of patients (61% [11/18]) had target lesion reduction. The safety profile was consistent with prior reports. Key grade ≥3 treatment-related adverse events were neutropenia (39%), fatigue (33%), diarrhea (28%), leukopenia (22%), anemia (17%), and febrile neutropenia (11%). No events of interstitial lung disease, ocular toxicities, or grade > 2 neuropathy were reported. There were no treatment-related deaths. In conclusion, the preliminary data for the use of sacituzumab govitecan in patients with mUC after failure of platinum-based regimen or anti-PD-1/PD-L1 based immunotherapy show a manageable safety profile with an ORR of 28% in comparison to an ORR of ∼23-29% for currently approved first-line treatment.
Other ongoing studies for urothelial carcinoma
Numerous ongoing trials are also evaluating the role of targeted therapies for advanced UC. Table 2 provides an overview of select trials.
Select ongoing trials of targeted therapies for urothelial carcinoma.
The THOR trial (NCT03390504) is phase 3, randomized, open-label study evaluating the efficacy and safety of erdafitinib versus standard of care (chemotherapy or pembrolizumab) in patients with advanced UC and selected FGFR alterations who have progressed on or after 1 or 2 prior lines of therapy. 39 The primary endpoint of the THOR study is OS.Primary completion is anticipated in November 2020. An estimated 631 patients will enroll in the study.
The FORT-1 trial (NCT03410693) is a phase 2/3, multicenter, randomized, open-label study to evaluate the efficacy and safety of rogaratinib versus chemotherapy in patients with FGFR-positive locally advanced or mUC who have received prior treatment with a platinum-based chemotherapy. 34 One hundred seventy-five patients are enrolled in the study. Patients randomized to the rogaratinib group receive treatment orally twice daily, and patients randomized to the chemotherapy group receive investigator’s choice of docetaxel, paclitaxel, or vinflunine intravenously on Day 1 of 21-day cycles. The primary outcome measure of the trial is overall response rate, defined as the percentage of patients with complete or partial response. Primary completion of the study is anticipated in November 2020. In preliminary results reported at ASCO 2020, the efficacy of rogaratinib was comparable to that of standard chemotherapy, with an overall response rate of 19.5% for rogaratinib and 19.3% for standard chemotherapy (1-sided P=0.56). For patients with FGFR3 DNA alterations, exploratory analysis showed overall response rates of 52.4% and 26.7% for rogaratinib and standard chemotherapy, respectively.
FORT-2 (NCT03473756) is a phase 1b/2 study of rogaratinib in combination with atezolizumab in cisplatin-ineligible patients. 35 Patients with untreated mUC were eligible if they exhibited overexpression of FGFR mRNA. In preliminary results reported at ASCO 2020, treatment-emergent adverse events led to discontinuation in 45.5% of patients receiving 800 mg rogaratinib and 12.5% of patients receiving 600 mg rogaratinib. In 23 evaluable patients, 39% had an ORR, 13% had a CR, 26% had a PR, and 26% had stable disease.
FIGHT-201 (NCT02872714), a phase 2, multicenter, single-agent, open-label trial is evaluating the efficacy and safety of pemigatinib in patients with surgically unresectable or mUC harboring alterations in fibroblast growth factor (FGF) or FGFR and who have failed at least 1 previous treatment for their disease (including either chemotherapy or immunotherapy) or have not received chemotherapy due to poor ECOG PS or insufficient renal function. 36 An estimated 240 patients will be enrolled.
Discussion
The treatment paradigm for UC management has significantly expanded over recent years with ICIs being at the forefront across several lines of therapy. Despite numerous advances, enrollment in a clinical trial is strongly encouraged across all stages of locally advanced and mUC. 2 Early stages of bladder cancer, are often adequately managed with a transurethral resection of the bladder tumor followed by intravesicular chemotherapy or immunotherapy for NMIBC. For patients who are BCG-refractory are cystectomy-ineleigble, pembrolizumab offers a new treatment option in this setting based on findings from Keynote-057. 9 , 10
The role of immunotherapy and targeted therapy for locally advanced or mUC continues to evolve. To date, the most notable impact of ICIs for front-line advance disease is avelumab maintenance following platinum-based chemotherapy based on the OS and PFS benefits observed in the JAVELIN Bladder 100 trial. 12 It is likely that avelumab maintenance will become a SOC option for patients limiting the role of ICIs in the second-line setting. Despite the efficacy of avelumab, it is important to note that it is dosed twice weekly whereas other ICIs have a longer dosing interval and requires premedications prior to infusion when patients initiate therapy. 13 Additional notable findings include the lack of OS benefits with atezolizumab and pembrolizumab when combined with chemotherapy. 15 , 16 Patients who do not receive avelumab maintenance and progress following front-line therapy, should receive pembrolizumab. Although, five ICIs are approved in this setting, pembrolizumab is the only category 1 recommendation and the only ICI to demonstrate an OS benefit in this setting. 2 , 14 Additional options for advanced UC include enfortumab vedotin, erdafitnib, taxane combinations, and enrollment in clinical trials. 2
Numerous notable trials highlighted in this manuscript are likely to expand and/or shift the current landscape of treatment for advanced disease. Additionally, the role of PD-L1 expression in advanced UC remains ambiguous and several factors should be evaluated prior to treatment selection. Patient comorbidities, prior lines of therapy, time to progression, availability of a clinical trial, ligand expression in select cases, and cost and logistics of therapy administration should all be considered. With the proven efficacy of ICIs and antibody-drug conjugates, it is likely that the cost of care will continue to rise and should be balanced with the safety and efficacy of the selected treatments.
Conclusion
In recent years, novel therapeutic advances have been observed in the management of early stages and advanced or metastatic stages of UC. As a result, therapeutic options have led to an increased OS and PFS for patients with advanced disease. Numerous ongoing, clinical trials are further evaluating novel targets, combinations and sequences of therapies in aims to further improve outcomes for patients. The future landscape of UC will continue to evolve, and it is crucial to maintain knowledge of this rapidly evolving disease.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.