
Abstract
Introduction
Low-dose, weekly cisplatin (40 mg/m2) regimens are currently utilized at Eskenazi Health in Indianapolis, Indiana for the treatment of head and neck cancer due to enhanced tolerability. This retrospective analysis analyzes the incidence, severity, and risk factors for AKI in patients who received this regimen.
Methods
A retrospective chart review was conducted including patients with head and neck cancer treated with weekly, low dose cisplatin (40 mg/m2) with concurrent radiotherapy (RT). From this criteria, 22 patients were identified and included in the final analysis. AKI was defined by the Common Terminology Criteria for Adverse Events (CTCAE) version 4.03.
Results
Of the 22 patients included, 12 (54.5%) experienced AKI, with 10 patients (45.5%) experiencing grade 1 AKI and 2 patients (9.1%) experiencing grade 2 AKI. Six patients (27.3%) required dose adjustments or delays due to renal adverse events, all of which had initial cisplatin total weekly doses of >70 mg. Those receiving a total weekly cisplatin dose of >70 mg were found to have a higher risk of developing an episode of AKI compared to the group receiving <70 mg (p = 0.029).
Conclusion
This analysis showed patients receiving weekly doses >70 mg of cisplatin as their initial treatment dose for head and neck cancer were more likely to experience AKI. There are inconsistencies in the frequency of AKI in our study compared to published literature; however, this comparison is difficult due to the small sample size of our trial. This demonstrates the need for further investigation into the issue.
Introduction
Cisplatin is a platinum-based antineoplastic drug indicated for the treatment of multiple solid-organ cancers. Cisplatin is used in combination with radiotherapy (RT) in the treatment of cervical cancer and head and neck cancers. Toxicities of cisplatin treatment include ototoxicity, nausea/vomiting, mucositis, myelosuppression, allergic reactions, electrolyte abnormalities, and nephrotoxicity. Nephrotoxicity is recognized as a dose-limiting side effect of cisplatin. One of the more serious and common manifestations of cisplatin renal toxicity is AKI, but renal toxicity due to cisplatin can present in numerous ways. 1
Cisplatin is eliminated in the kidneys by both glomerular filtration and tubular secretion. Receptor-mediated uptake is primarily mediated by the CTR1 copper transporter and organic cation transporter (OCT2) proteins. These transporters are both highly expressed in the proximal tubules of the kidneys, and can allow for cisplatin accumulation in the renal tubules. Multidrug and toxic compound extrusion (MATE) proteins MATE1 and MATE2 alongside P-glycoprotein play an importantrole in the efflux of organic cations out of the endothelial cells. MATE1 which is especially linked to the clearance of cisplatin is subject to drug interactions and saturation with cisplatin accumulation, and can lead to endothelial damage and toxicity. 1--2
Enzymatic metabolism in renal cells leads to the formation of conjugated intermediates which can be further metabolized to reactive thiols. 1 These reactive thiols mediate cytotoxic damage to proximal tubule cells. The cytotoxic effect of cisplatin is derived from its ability to intercalate into DNA and RNA and induce inter- and intrastrand crosslinking. Accumulation of cisplatin in the renal tubules increases susceptibility to both nuclear and mitochondrial DNA damage leading to renal cell death. Through this mechanism, death receptor activation, and endoplasmic reticulum stress response, necrosis and apoptosis can occur. Renal damage leads to an inflammatory response which can further exacerbate renal toxicity, making AKI a primary concern in patients treated with cisplatin, especially when given a high dose. 1
High-dose cisplatin (≥75 mg/m2) every 3 weeks, with concurrent RT, is considered the preferred therapy in the treatment of head and neck cancer. 3 However, in the treatment of locally advanced head and neck cancers, the use of weekly cisplatin at a lower dose of 40 mg/m2 is commonly used with fractionated RT. This approach has shown similar efficacy as well as better tolerability than high-dose regimens, and is now one of the recommended regimens in the treatment of head and neck cancer by the National Comprehensive Cancer Network (NCCN).3–5 This low dose cisplatin regimen with concurrent RT is also used in cervical cancer; however, the cervical cancer guidelines also have a weekly dose cap of 70 mg cisplatin weekly, which is not present in the head and neck cancer guidelines.3,6,7
A recent meta-analysis was published comparing both high and low-dose cisplatin treatment regimens for the treatment of locoregionally advanced non-pharyngeal head and neck cancer across 52 studies. This meta-analysis found no significant differences in treatment efficacy between the regimens and found significantly less nausea/vomiting, severe neutropenia, and nephrotoxicity in the low dose, once-weekly group. 8 With other surmounting evidence supporting increased tolerance and similar efficacy of the once-weekly regimen, this has been the preferred treatment regimen for patients with head and neck cancer at Eskenazi Health.4,5,8–11
Although clinical data have been collected surrounding the incidence of AKI in patients with head and neck cancer treated with concurrent cisplatin with RT, most studies included patients being treated with high dose cisplatin given every 3 weeks. Information is limited surrounding the incidence and severity of AKI in patients treated with weekly 40 mg/m2 cisplatin with concurrent RT for head and neck cancer.
In this retrospective chart review, we determined the incidence and severity of AKI in patients treated with weekly cisplatin at our institution with the intent of identifying common risk factors.
Methods
Patients
This study was a retrospective chart review of all patients with head and neck cancer treated with weekly low-dose (40 mg/m2) cisplatin with concurrent RT who completed treatment at Eskenazi Health in Indianapolis, IN between October 1, 2016 and May 30, 2019. Subjects were excluded if weekly cisplatin was used for indications other than head and neck cancer or they did not receive a dose of cisplatin during the study period. Twenty-two patients were identified from this criteria and included in the final analysis. Information was obtained using Eskenazi Health’s electronic medical record and included demographic information, chemotherapy treatment regimens, delays or adjustments in treatment, and renal function at baseline and throughout treatment. This protocol #1906420652 received exempt approval by the Indiana University Health Institutional Review Board.
Outcomes
AKI was defined by the Common Terminology Criteria for Adverse Events (CTCAE) version 4.03 specified in Table 1. 12 Creatinine clearances were calculated using the Cockcroft-Gault equation to estimate renal function at baseline and throughout treatment. This calculation was performed with ideal body weight unless the patient’s actual body weight was less than ideal, or if actual body weight was >130% of their ideal body weight. If the latter was the case, an adjusted body weight was utilized. A minimum serum creatinine of 0.7 mg/dL has been recommended by NCCN in the dosing of carboplatin, especially in elderly or cachectic patients.13 This minimum was not used as part of our analysis, however, only 4 patients in our study had a serum creatinine < 0.7 mg/dL. Of these 4 patients, one patient was 62 years of age with a weight of 44.6 kg and may have had an over-estimated creatinine clearance. The other 3 patients were younger with heavier body weights, making the risk for over-estimation of renal function lower. Dose reductions were not included if they were based on changes in body surface area (BSA).
Common Terminology Criteria for Adverse Events Version 4.03.

Statistical analysis
Statistical analysis was performed using the MiniTab(R) software. The normality of all demographic data points was assessed using the Anderson-Darling test. All continuous variables are represented as a mean (standard deviation) for normal data and a median (interquartile range) for non-normal data. All ordinal variables were represented as a number (percentage). Risk factors for AKI were compared using Mann-Whitney U tests for non-normal data, two-sample T tests for normal data, and Fisher’s Exact tests for ordinal data. An alpha of 0.05 was utilized to determine the statistical significance of results.
Results
Enrollment and baseline characteristics
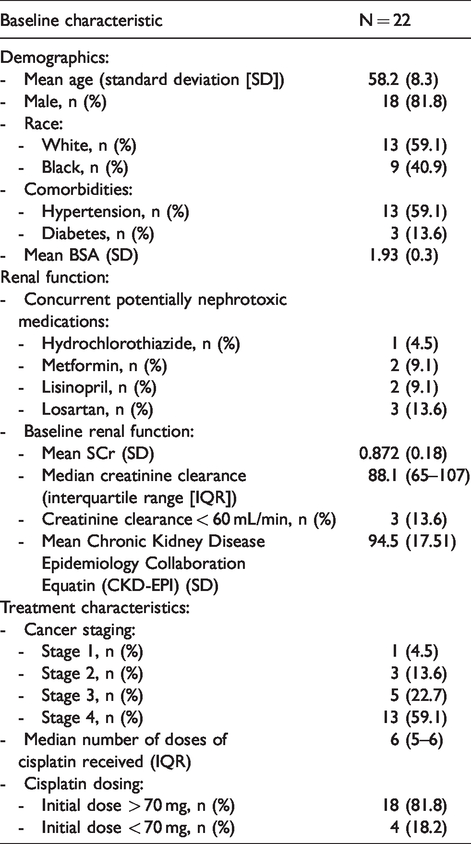
A total of 31 patients diagnosed with head and neck cancer and receiving weekly cisplatin were identified at Eskenazi Health. Twenty-two of these patients met eligibility criteria and were included in the final analysis. Thirteen patients (59.1%) had stage 4 disease and the average baseline serum creatinine (SCr) was 0.87 (+/− 0.18) with median creatinine clearance of 82 mL/min (IQR 65–107). Only 3 patients (13.6%) had a creatinine clearance < 60 mL/min. Table 2 displays the complete demographic characteristics of all patients included in the analysis.
Patient Demographics.
Toxicity events
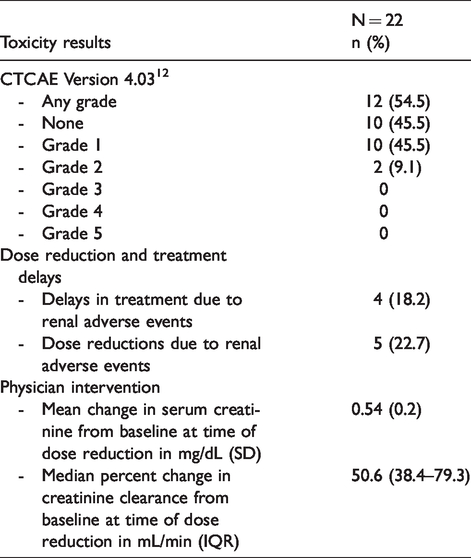
Among the 22 patients included in the study, 12 patients (54.5%) experienced AKI of any grade. Ten patients (45.4%) experienced grade 1 toxicity and 2 patients (9.1%) experienced grade 2 toxicity as determined by CTCAE version 4.03. 12 Dose reductions due to renal events occurred in 5 patients (22.7%), and delays in treatment due to renal events occurred in 4 patients (18.2%) . Seven patients (31.8%) were hospitalized during their treatment, however only 1 patient was found to have AKI upon admission. This patient was primarily admitted due to intractable chemotherapy-induced nausea and vomiting and thus was not classified as a grade 3 AKI. All toxicity events are reported in Table 3.
Toxicity Outcomes.
Risk factor analysis
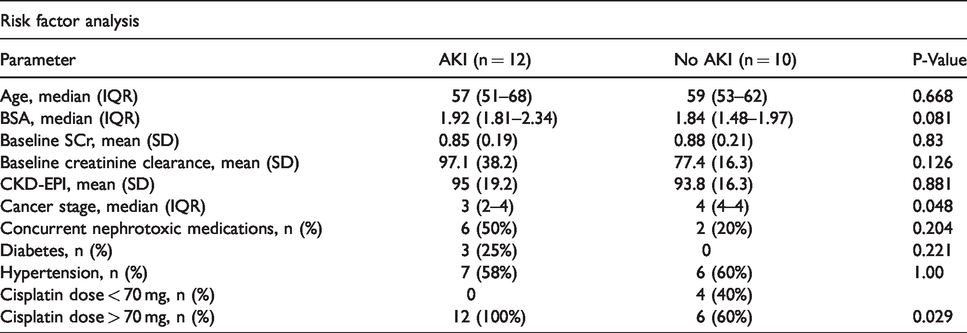
To better understand risk factors associated with AKI in the study population, all baseline characteristics were analyzed to identify differences between patients who experienced AKI and those who did not. The only statistically significant differences found between groups were stage of disease and cisplatin dose.
The median cancer stage was lower in patients who developed AKI compared to those who did not develop AKI (p = 0.048). This is not thought to be clinically significant.
A total weekly cisplatin dose >70 mg was found to be a significant risk factor for developing an AKI (p = 0.029). Every patient who developed an AKI received >70 mg cisplatin weekly. The median BSA was also found to be larger in patients who experienced AKI, but this was not found to be statistically significant (p = 0.081). This difference in BSA and the consequently larger cisplatin dose may have led to an increased risk of AKI.
During the treatment period, 6 patients (27.3%) required dose adjustments or delays in therapy due to renal adverse events. All 6 patients had initial total weekly doses of cisplatin > 70 mg. This may be clinically relevant, but it was not statistically significant (p = 0.541). Statistical analysis showed that approximately 27 patients would be needed in each group to detect a 33.3% difference in the rate of dose adjustments or delays.
Complete results of the risk factor analysis are included in Table 4.
Risk Factor Analysis.
Physician intervention
Through our analysis we were able to assess what changes in SCr from baseline occurred that led to reduction of cisplatin doses. Dose reductions occurred with a mean increase in SCr of 0.54 mg/dL (0.2), or with a median percent change in SCr from baseline of 50.6% (38.4–79.3). Total weekly cisplatin doses were reduced by 30–50% in response to AKI. Physician responses to AKI are included in Table 3.
Conclusion
Literature discussing the incidence and severity of AKI in patients with head and neck cancer treated with weekly, low dose cisplatin and concurrent RT are limited. Most literature has primarily focused on patients treated with high dose cisplatin (70 mg/m2) every 3 weeks.
Comparing collected data to other primary literature sources are difficult because little published information exists regarding the incidence of AKI in patients receiving low dose cisplatin. A retrospective analysis by Chanal et al. included 144 patients compared the rates of AKI in patients receiving 100 mg/m2 or 40 mg/m2 using the CTCAE version 4.03. 10 In this study, 68.3% (n = 71) of patients experienced Grade 1 AKI and 6.7% (n = 7) experienced Grade 2 AKI. 10 Comparatively, a retrospective analysis by Ghosh et al. showed a 17.1% Grade 1 and 1.7% Grade 2 AKI rate using CTCAE version 4.0. 14
Comparing these published frequencies to this study show inconsistencies. The frequency of AKI for both Grade 1 (45.4% vs 40% vs 17%, respectively) and Grade 2 (9.1% vs 52% vs 1.7%) are not consistent between studies.10,13 These differences in AKI rates could potentially be due to variance in pre-medications and hydration with treatment. Each study had a low number of participants so that also could contribute to differences in AKI rates as well. The true rate of AKI in patients with head and neck cancer receiving low-dose weekly cisplatin with RT will continue to be unknown until a larger study is conducted.
A summary of the results of these studies compared to our study are included in Table 5.
Comparison to Published Literature.

Patients who experienced AKI were found to have a lower median stage of disease compared to those with a higher stage of disease. Although this difference was found to be statistically significant, the clinical relevance of this result is limited as all patients receive the same treatment regimen regardless of staging.
Patients with a total weekly cisplatin dose of >70 mg were found to have a statistically significant increased risk for the development of AKI. We performed analyses of doses above and below 70 mg due to the 70 mg dose cap utilized in the treatment of cervical cancer.
Low-dose weekly cisplatin (40 mg/m2) with concurrent RT is one of the preferred regimens for treatment of cervical cancer; however, cisplatin has a dose cap of 70 mg when used for cervical cancer.6,7 The results of our study, despite its small population, encourages the further analysis of cisplatin use in patients with head and neck cancer to determine if a dose cap of 70 mg should also be employed to improve patient outcomes and decrease toxicity.
More patients who received >70 mg cisplatin weekly had dose adjustments and delays due to renal events compared to patients who received <70 mg cisplatin. This was not found to be statistically significant, but further supports the use of a dose cap when treating head and neck cancer.
This study has several limitations. First, the small population of this study limits extrapolation of this data to larger, more diverse populations. The selection of eligible patients was limited by a narrow search window based on initiation of Eskenazi Health’s current electronic medical record. Second, this study is limited in its retrospective nature. Treatment duration and supportive medications were determined by the treatment team on a patient-specific basis which could confound the results of this study. However, patients received a median of 6 cycles of cisplatin and pre-medications, including intravenous hydration as well as chemotherapy-induced nausea and vomiting (CINV) prophylaxis. These medication choices were consistent across almost all patients. Third, no prospective recommendations were made regarding response to acute toxicities. Although this decreases the internal validity of the study, it is more representative of current clinical practice and real-world clinician response to AKI toxicities in this treatment population. Through our analysis of physician intervention to acute toxicities, we hoped to better delineate common responses to guide physicians in the future.
Risk factors for the development of AKI in patients receiving low dose cisplatin with RT have not been well described in current literature and total weekly doses of cisplatin greater than 70 mg was the only clinically and statistically significant risk factor found during our study. Although this study helps fill some of the gaps in literature regarding AKI in once weekly cisplatin in patients with head and neck cancer, larger, prospective studies are still needed to further determine the incidence and severity of AKI in this population. Further research should also focus on the potential utilization of a 70 mg weekly cap.
Footnotes
Acknowledgements
All authors contributed equally to the concept and design of the work, analysis and interpretation of the data, and the writing and editing of the manuscript.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.