
Abstract
The aim of this paper was to assess the drug costs of the different biotechnologies (intranasal fentanyl spray (INFS), oral transmucosal fentanyl citrate (OTFC) and fentanyl buccal tablet (FBT)) in the treatment of breakthrough cancer pain (BTCP). We have calculated the mean drug costs (expressed in euros (€)) for patients treated for BTCP. INFS resulted the less expensive towards OTFC and FBT, with 697 440 €versus (vs.) 809 552 €vs. 779 662 €every 100 patients treated for BTCP, respectively. In conclusion, combining drug costs of different biotechnologies (INFS, OTFC and FBT) with the measure of efficacy represented by the reduction of BTCP avoided (incremental cost-effectiveness ratio, ICER), INFS resulted in better cost-effectiveness.
From the literature we know that the prevalence of breakthrough cancer pain (BTCP) ranged from 40 to 80% in the different trials. The recent introduction of rescue medications with high bioavailability, strong effect and short half-life has radically changed the approach to BTCP.
1
The use of new biotechnologies has made known molecules more interesting, such as intranasal fentanyl spray (INFS), oral transmucosal fentanyl citrate (OTFC) and fentanyl buccal tablet (FBT). In the literature, there is only one study direct comparing the different biotechnologies carrying fentanyl and BTCP control in favour of INFS.
2
The introduction of these active new biotechnologies for the treatment of BTCP is associated with a relevant increase of costs and it is therefore important to make a balance between the costs of treatment and the added value represented by the percentage of BTCP avoided. The aim of this paper was to assess the drug costs of the different biotechnologies (INFS, OTFC and FBT) in the treatment of BTCP (about 90% of overall costs [3]). We have calculated the mean drug costs (expressed in euros (€)) for patients treated for BTCP. As reference papers we have considered the only experiences in the literature considering costs of BTCP.
3
,
4
The percentage of BTCP avoided versus (vs.) placebo was 55% for INFS, 29% for OTFC and 31% for FBT,
3
based on data from six randomized controlled trials (RCTs),
2
,5–9 including 557 patients and anlalyzed in a meta-analysis.
10
In particular, the mean drug costs for each patient treated for BTCP was quantified in 5034 €for INFS and OTFC and 4348 €for FBT [3]. Differently, the mean drug costs for each patient with untreated for BTCP was quantified in 9346 €(
The different biotechnologies (INFS, OTFC and FBT) in the treatment of BTCP and the drug costs for patients with treated and untreated BTCP.
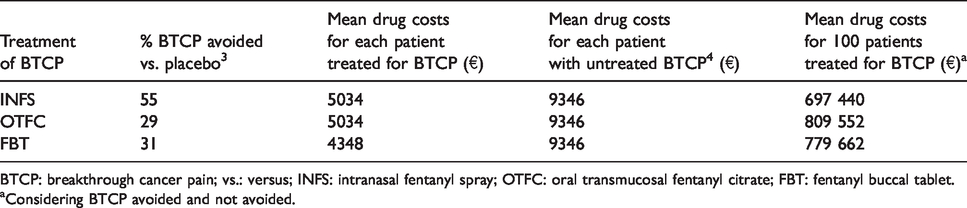
BTCP: breakthrough cancer pain; vs.: versus; INFS: intranasal fentanyl spray; OTFC: oral transmucosal fentanyl citrate; FBT: fentanyl buccal tablet.
aConsidering BTCP avoided and not avoided.
From the data presented it is easy to see that the pharmacological costs were influenced by two main factors: the efficacy of the therapies (strictly associated with the patient's inclusions criteria) and the price of drugs used. We decided to limit our evaluation to data from phase III RCTs first of all because phase II trials looking for effective combinations are plagued by patient's selection biases, that significantly reduce the possibility to define “credible” measures of efficacy. Furthermore, we needed randomized trials to allow comparison of efficacy between the arms of each trial. Despite this, our analysis has several limitations, such as cross-trial comparisons. Moreover, we have considered only the direct costs, but there are other important cost elements that are not considered here (e.g. outpatient/inpatient administration costs or treatment-related adverse event costs or health-related quality of life between different first-line treatments). 11 However, this problem is partially overcome by taking into consideration on the one hand that approximatelly 90% of overall costs were attributable to drug acquisition 3 and in the other hand considering the total annual health care costs in the evaluation.
To this we must add that, to our knowledge, this is the first time an analysis of the drug costs of different biotechnologies, such as INFS, OTFC and FBT, is linked to a reduction of BTCP avoided.
In conclusion, combining drug costs of different biotechnologies (INFS, OTFC and FBT) with the measure of efficacy represented by the reduction of BTCP avoided, INFS resulted in better cost-effectiveness. The price of newly registered oncologic drugs is continuously increasing posing a serious treat to the sustainability of the National Health Systems, especially in Countries in which the public control and oversight over the prices is limited. Medical Oncologists and the society as a whole are becoming more and more concerned with the issues of the costs of the cure of cancer patients and are able to bring attention to the “just price” of new treatments that must reflect the reality of their true benefits and societal and personal costs.
Footnotes
Authors’ contribution
All authors contributed equally to (1) conception and design, acquisition of data, or analysis and interpretation of data; (2) drafting the article and revising it critically for important intellectual content: and (3) final approval of the version to be published.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.