
Abstract
Background
Vascular endothelial growth factor (VEGF) inhibitors are known to cause hypertension. The purpose of this study was to assess the impact of blood pressure (BP) elevations on outcomes in patients receiving VEGF inhibitors.
Methods
This retrospective chart review analyzed patients receiving treatment with VEGF inhibitors. The primary endpoint was time to progression (TTP) in those with or without significant increase in BP (increase in systolic BP greater than 20 mm Hg or greater than 10 mm Hg increase in diastolic BP). Secondary endpoints included treatment interruption, therapy discontinuation due to documented adverse effect, and time to BP elevation. Subgroup analyses were completed in those receiving bevacizumab and oral tyrosine kinase inhibitors.
Results
A total of 155 patients were included and 93 patients (60%) experienced a significant increase in BP. Median time to development of an elevated BP was 47 days. Patients with significant increases in BP had a longer median TTP compared to patients without (8.1 months vs 4.4 months, p = 0.002). No differences were present between groups in treatment interruption or discontinuation due to a documented adverse effect and outcomes were similar in those receiving bevacizumab and oral tyrosine kinase inhibitors. In the analysis of the impact of severity of BP elevations, those with severe BP elevations were more likely to have treatment interrupted but discontinuation rates were similar across groups.
Conclusion
Development of significant BP elevations may be a marker of therapeutic response to VEGF inhibitors and does not limit treatment duration, even in those with severe elevations.
Introduction
Background
Vascular endothelial growth factor (VEGF) is a signaling protein that promotes angiogenesis. 1 Controlling angiogenesis is of particular interest in the oncology setting as new blood vessels provide nutrients to tumor cells, thus promoting tumor cell growth. VEGF inhibitor therapies prevent the proliferation of endothelial cells and the formation of new blood vessels, slowing the growth of tumor cells. Inhibitors of the VEGF pathway are utilized in a variety of cancer types including colorectal cancer, renal cell carcinoma, non-squamous non-small cell lung cancer, and ovarian cancer, to name a few. Drugs with varying mechanisms with which they inhibit VEGF are routinely used in clinical practice. Monoclonal antibodies, such as bevacizumab, target and neutralize the VEGF ligand or receptor. Orally administered tyrosine kinase inhibitors (TKI) such as axitinib, lenvatinib, pazopanib, regorafenib, sorafenib, and sunitinib block VEGF receptor signaling by binding to the tyrosine kinase domain on the intracellular protein of VEGF receptors. 2
Along with therapeutic advantages of VEGF inhibitors, these agents are also associated with a variety of adverse events. One common toxicity is hypertension. Common Terminology Criteria for Adverse Events (CTCAE) Version 5.0 defines hypertension as a blood pressure greater than 120/80 mm Hg and severity is graded as outlined in Table 1. 3 The prevalence of hypertension associated with VEGF inhibitors varies for each medication in the class. The incidence of bevacizumab-induced all grade hypertension is reported to be approximately 24% with 8% being severe hypertension (grade 3 or 4) and has been shown to be dose-dependent. 4 Sunitinib has a reported incidence of all-grade hypertension of 22% with a grade 3 or 4 hypertension rate of 7%. 5 Within the class of VEGF inhibitors, hypertension usually arises within weeks of starting therapy and despite similar incidences in some studies, it remains unclear if any agent is associated with a greater incidence of all-grade or grade 3 or 4 hypertension over others.6,7
CTCAE grading scale for hypertension.
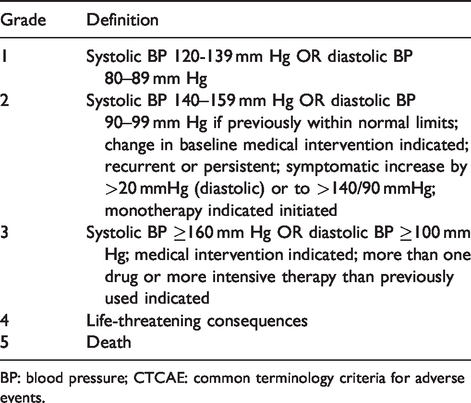
BP: blood pressure; CTCAE: common terminology criteria for adverse events.
Hypertension may represent a surrogate marker for VEGF inhibitor therapeutic effects and treatment response. In patients being treated with bevacizumab for colorectal cancer, a correlation between the development of grade 2 or 3 arterial hypertension and increased progression-free survival has been noted. 8 This has not been consistently reported within or across different types of cancers, as multiple studies did not demonstrate a benefit in those experiencing hypertension. 7 Patients with persistent and worsening hypertension may require discontinuation of the VEGF inhibitor and this may result in decreased benefit of treatment. Understanding the impact of hypertension as an adverse event and potential marker of response to various VEGF inhibitors across multiple malignancies in everyday clinical practice is important to inform its management and therapeutic outcomes. The purpose of this study was to assess the impact of increases in blood pressure on outcomes in patients receiving VEGF pathway inhibitors.
Methods
Study design
This retrospective study of patients receiving anti-VEGF therapy was conducted as a review of patients who received outpatient treatment at a community hospital in Indiana with bevacizumab or an anti-VEGF TKI (axitinib, lenvatinib, pazopanib, regorafenib, sorafenib, or sunitinib). Patients were included if they received at least one dose of medication from January 1, 2017 through January 1, 2019 and were at least 18 years of age. Patients were excluded if they did not receive a dose of anti-VEGF therapy during the study period. Data was collected from the time of anti-VEGF therapy initiation until discontinuation of the drug or for a total of 6 months if the drug was not discontinued before June 30, 2019. The local institutional review board provided approval for this research.
The primary endpoint of this study was time to progression (TTP), defined as the time from treatment initiation to documentation of disease progression, in those with or without a significant increase in blood pressure. A significant increase in blood pressure was defined as an increase in systolic blood pressure (SBP) greater than 20 mm Hg or greater than 10 mm Hg increase in diastolic blood pressure (DBP) above baseline at the start of therapy. Increases in blood pressure were utilized instead of CTCAE based grading to quantify hypertension due to the inability to retrospectively assess all criteria associated with CTCAE grading based on documentation in the medical record as well as to allow quantification of the impact of blood pressure increases in those with baseline hypertension. Blood pressure elevations were further classified as moderate if SBP increased greater than 20 mmHg but less than 40 mmHg or DBP increased greater than 10 mm Hg but less than 20 mm Hg and severe if SBP increased greater than 40 mm Hg or DBP increased greater than 20 mm Hg. The clinical practice of the site was to measure blood pressure at each patient visit. In order to provide a conservative estimate of the impact of increases in blood pressure, a single blood pressure measurement after starting anti-VEGF therapy meeting the definition above was required for classification as developing a significant elevation in blood pressure from baseline. Secondary endpoints included a description of time to development of a significant increase in blood pressure, and comparisons of treatment interruption for any reason and treatment discontinuation due to an adverse effect between those with and without a significant increase in blood pressure. Subgroup analyses were completed to determine the impact of severity of blood pressure increase on clinical outcomes (TTP, treatment interruption or discontinuation for any reason, and time to a significant increase in blood pressure), and impact of treatment type (bevacizumab or TKI) on TTP in those with and without significant increases in hypertension.
Data collection
Demographic data collected included age, sex, oncologic diagnosis, anti-VEGF regimen received, line of therapy, baseline systolic and diastolic blood pressure, pertinent past medical history (documented history of hypertension, diabetes, chronic kidney disease, or cardiovascular disease), and administration of prior lines of anti-VEGF therapy.
Data collected pertinent to the primary endpoint included time from treatment initiation to documented disease progression. Additional data collected for the assessment of secondary endpoints included blood pressure throughout therapy, time to first onset of a significant increase in blood pressure, treatment interruption, and treatment discontinuation due to a documented adverse effect.
Statistical analysis
The independent samples T-test and ANOVA were utilized to compare parametric continuous data, while the Mann-Whitney U and Kruskal-Wallis tests were utilized to compare non-parametric continuous data. Nominal and ordinal data were compared via the Chi-square and Wilcoxon rank sum tests, respectively. Time-to-event analyses were completed via Kaplan-Meier estimates and log-rank tests. Patients were censored at data cut-off date (July 30, 2019) or at the time of discontinuation for reasons other than disease progression. Post hoc analyses were completed using the Tukey test for equal variances, the Games-Howell test from non-equal variances, and Dunn’s multiple comparison test. P-values less than 0.05 were considered statistically significant. All statistical analyses were completed via IBM® SPSS® Statistics 25 software.
Results
Patient characteristics
Two hundred twenty-five patients were identified with orders for anti-VEGF therapy. Upon the exclusion of 70 patients for reasons including not starting the anti-VEGF therapy or being less than 18 years of age, 155 patients were included in the final analysis. The overall median duration of anti-VEGF therapy was 5.6 months. Ninety-three patients (60%) experienced a significant increase in blood pressure while on a VEGF inhibitor. Of those, 51 patients (55%) experienced a moderate increase in blood pressure and 42 patients (45%) experienced a severe increase in blood pressure. Overall, 53.5% of the patients were male, the average age was 64.5 years, and average baseline systolic and diastolic blood pressures were 131 mm Hg and 74 mm Hg, respectively. There were no statistically significant differences in baseline characteristics between those who developed a significant increase in blood pressure compared to those who did not (Table 2).
Baseline characteristics.
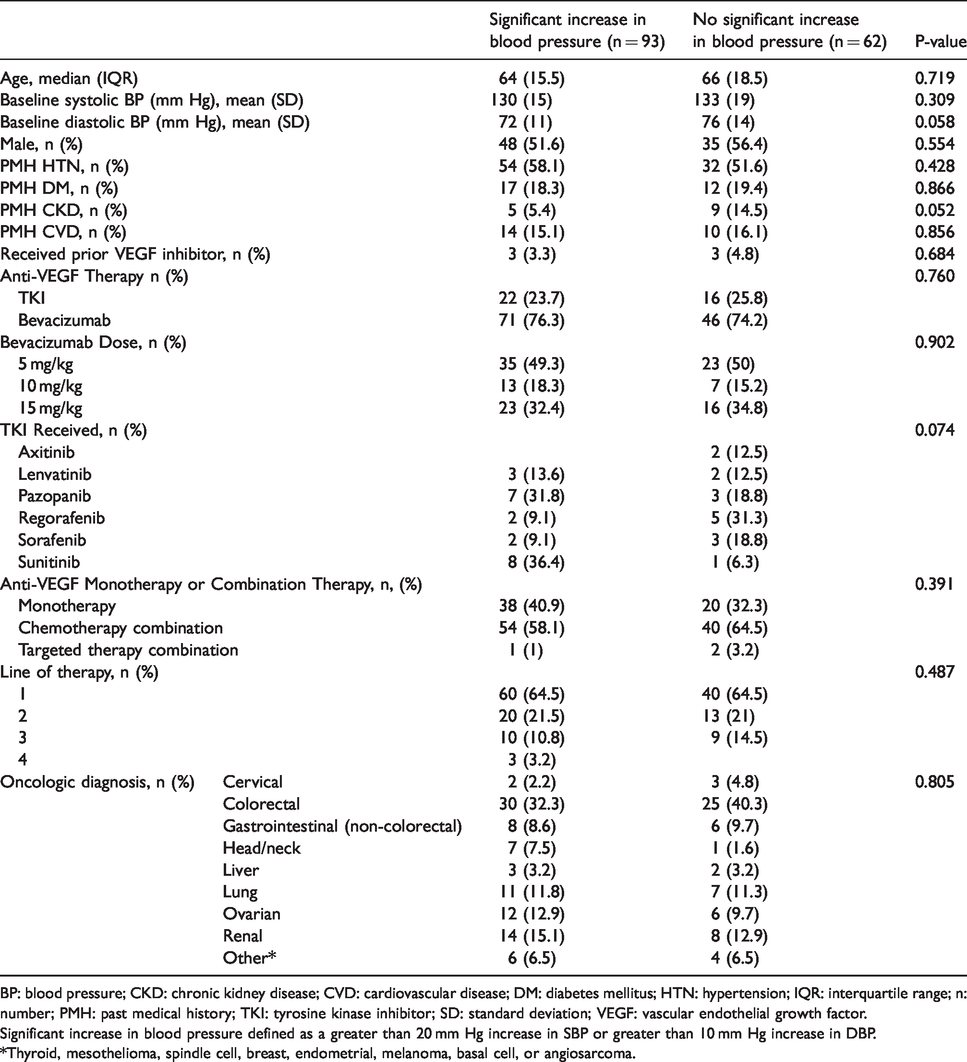
BP: blood pressure; CKD: chronic kidney disease; CVD: cardiovascular disease; DM: diabetes mellitus; HTN: hypertension; IQR: interquartile range; n: number; PMH: past medical history; TKI: tyrosine kinase inhibitor; SD: standard deviation; VEGF: vascular endothelial growth factor.
Significant increase in blood pressure defined as a greater than 20 mm Hg increase in SBP or greater than 10 mm Hg increase in DBP.
*Thyroid, mesothelioma, spindle cell, breast, endometrial, melanoma, basal cell, or angiosarcoma.
Outcomes
The primary endpoint, TTP, for the entire study population was 6.8 months. Patients experiencing a significant increase in blood pressure had a median TTP of 8.1 months [95% Confidence Interval (CI): 7.0 – 9.2 months] whereas patients without a significant increase in blood pressure had a median TTP of 4.4 months (95% CI: 3.3 – 5.6 months) (p = 0.002) (Figure 1). The median time to development of a significant increase in blood pressure in patients receiving anti-VEGF therapy was 47 days. No significant differences were present in the proportion of patients who had their treatment interrupted (45% in those with a significant increase in blood pressure vs 37% in those without, p = 0.319) or discontinued due to any documented adverse effect (14% vs 18%, respectively, p = 0.526).
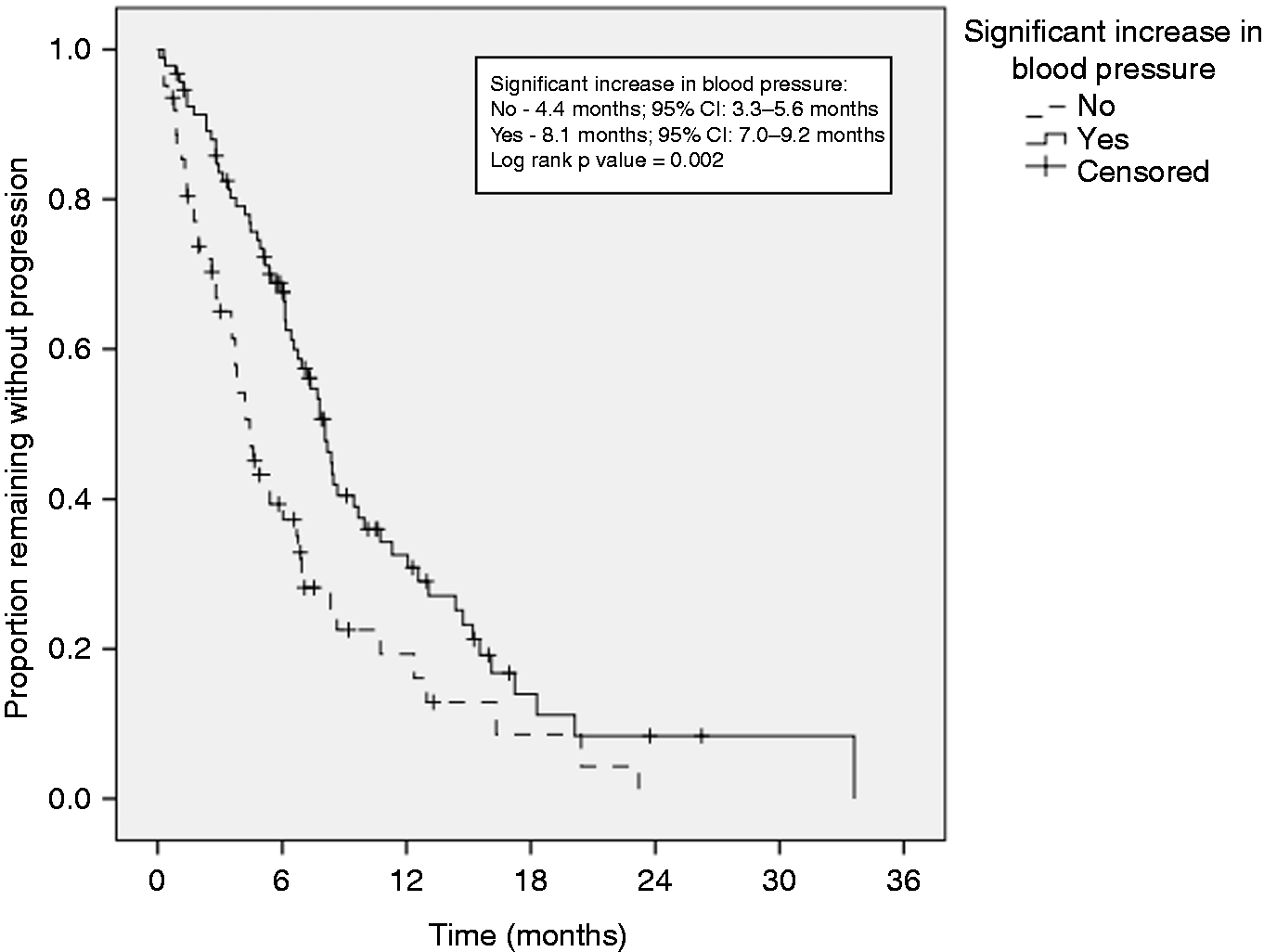
Time to progression in those with or without a significant increase in blood pressure.
Subgroup analysis – Impact of severity of blood pressure increase
When patients were analyzed based on the severity of blood pressure increase, baseline DBP was significantly different between those without a significant increase in blood pressure, those with a moderate increase in blood pressure, and those with a severe increase in blood pressure (76 mm Hg vs 74 mm Hg vs 69 mm Hg, respectively, p = 0.012). Post hoc analysis determined the difference existed between those experiencing severe increases in blood pressure compared to those who did not experience an increase in blood pressure (p = 0.011). All other baseline characteristics were similar (Table 3). Patients experiencing moderate or severe increases in blood pressure had significantly longer TTP than those without a significant increase in blood pressure (9.5 months, 95% CI: 6.3 – 12.6 months vs 7.2 months, 95% CI: 5.1 – 9.4 months vs 4.4 months, 95% CI: 3.3 – 5.6 months, respectively, p = 0.005) (Figure 2). Median time to a significant increase in blood pressure was similar between those with moderate and severe increases in blood pressure (56 days vs 42 days, respectively, p = 0.599). While patients experiencing severe increases in blood pressure were more likely to have treatment interrupted compared to those without an increase or with moderate increases in blood pressure (p = 0.024), rates of discontinuation due to documented adverse events were similar among the three groups (Table 3).
Impact of hypertension grade on outcomes.
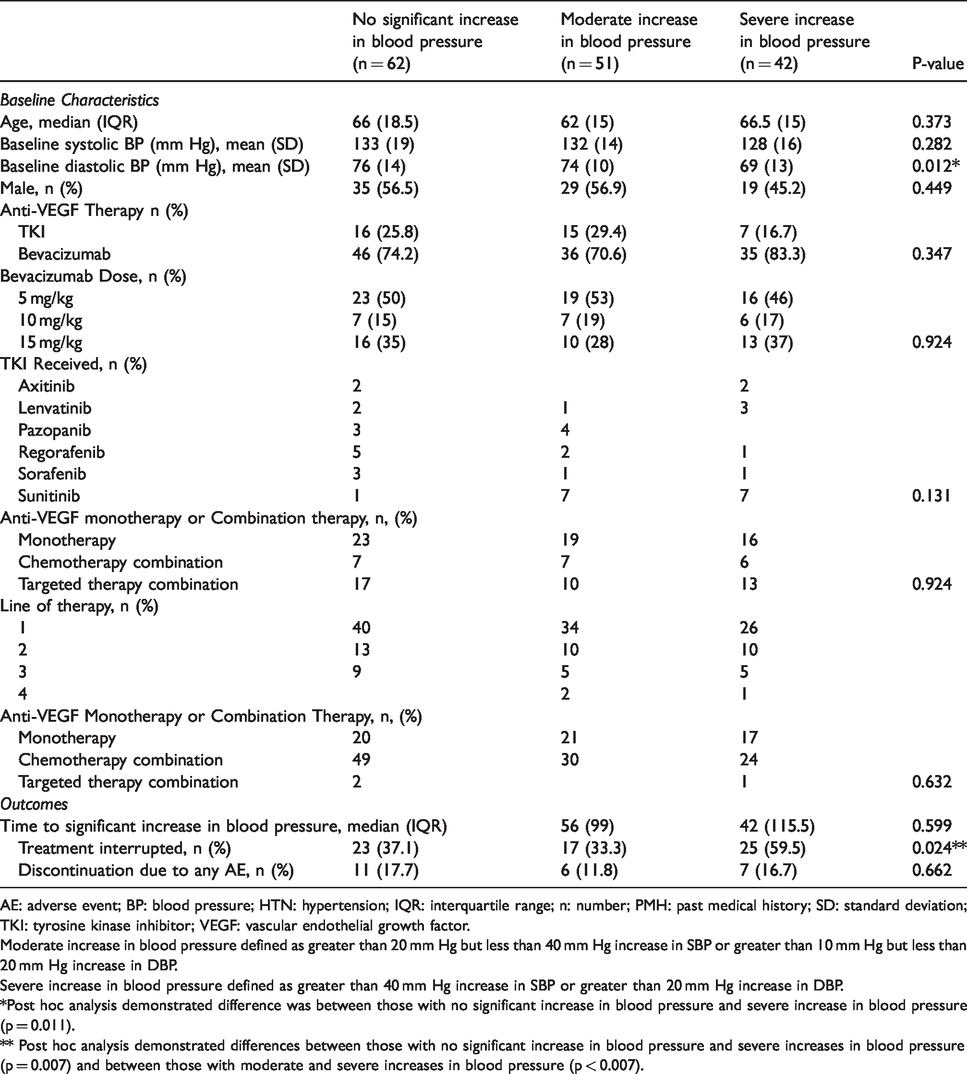
AE: adverse event; BP: blood pressure; HTN: hypertension; IQR: interquartile range; n: number; PMH: past medical history; SD: standard deviation; TKI: tyrosine kinase inhibitor; VEGF: vascular endothelial growth factor.
Moderate increase in blood pressure defined as greater than 20 mm Hg but less than 40 mm Hg increase in SBP or greater than 10 mm Hg but less than 20 mm Hg increase in DBP.
Severe increase in blood pressure defined as greater than 40 mm Hg increase in SBP or greater than 20 mm Hg increase in DBP.
*Post hoc analysis demonstrated difference was between those with no significant increase in blood pressure and severe increase in blood pressure (p = 0.011).
** Post hoc analysis demonstrated differences between those with no significant increase in blood pressure and severe increases in blood pressure (p = 0.007) and between those with moderate and severe increases in blood pressure (p < 0.007).
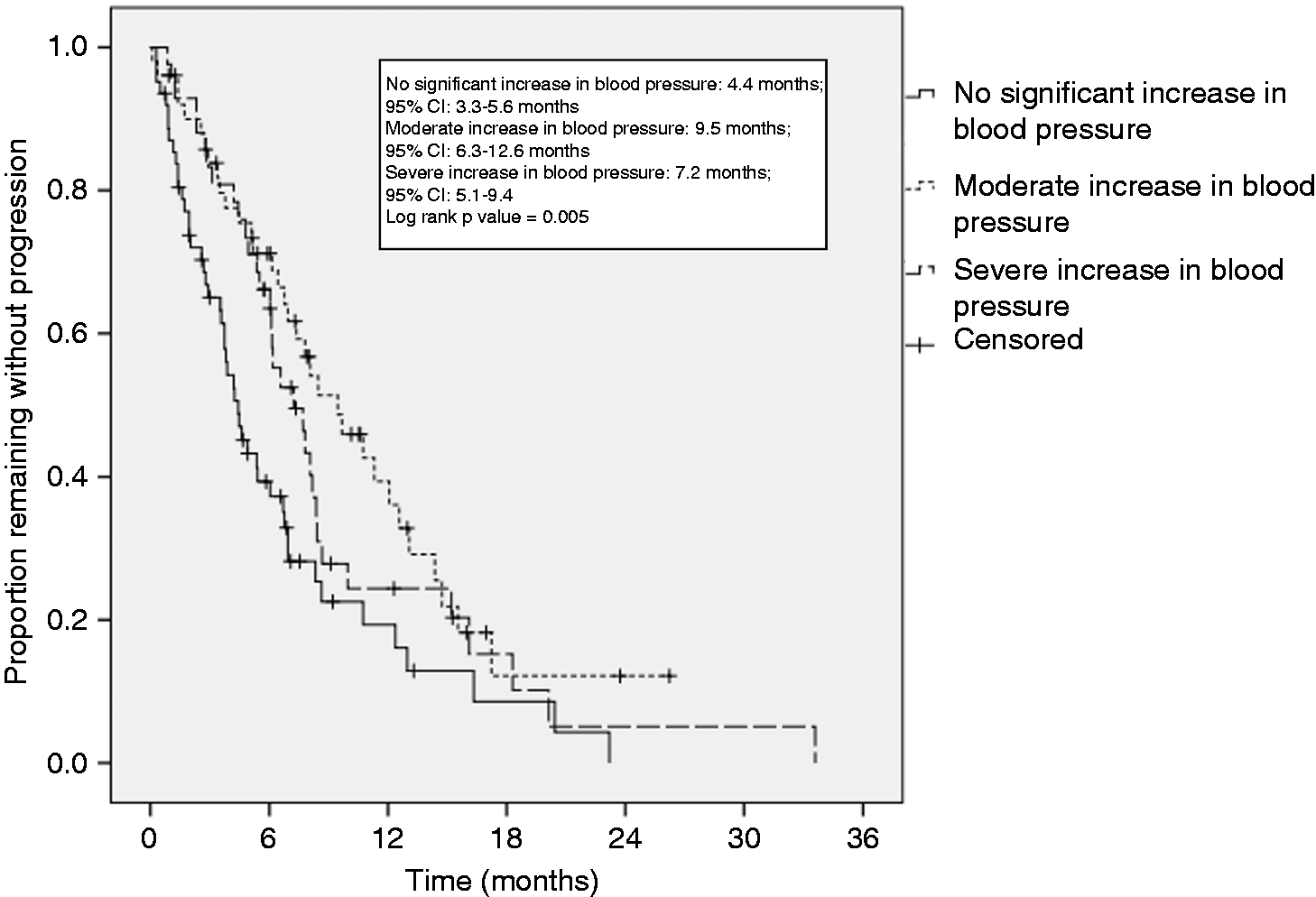
Impact of severity of blood pressure elevations on time to progression.
Subgroup analysis – Impact of treatment received (bevacizumab vs. TKI)
The majority of patients included in this study received bevacizumab treatment (75.5%). The primary outcome, TTP, was significantly longer for those with significant increases in blood pressure in both those receiving bevacizumab and those receiving TKIs (Figures 3 and 4). Time to development of a significant increase in blood pressure was similar between those receiving bevacizumab and those receiving a TKI (49 days vs 36.5 days, respectively, p = 0.212).
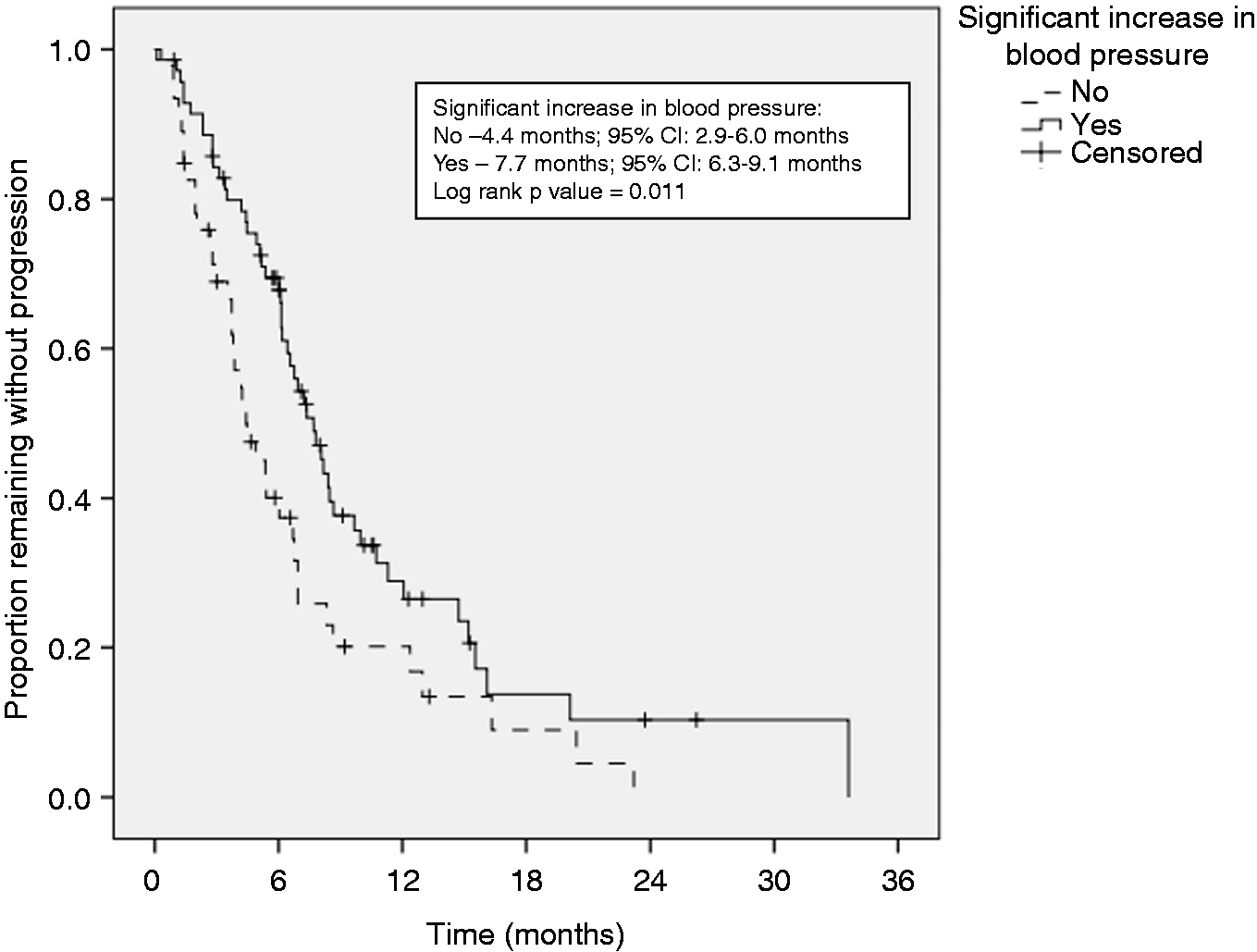
Bevacizumab Subgroup: Time to progression in those with or without a significant increase in blood pressure.
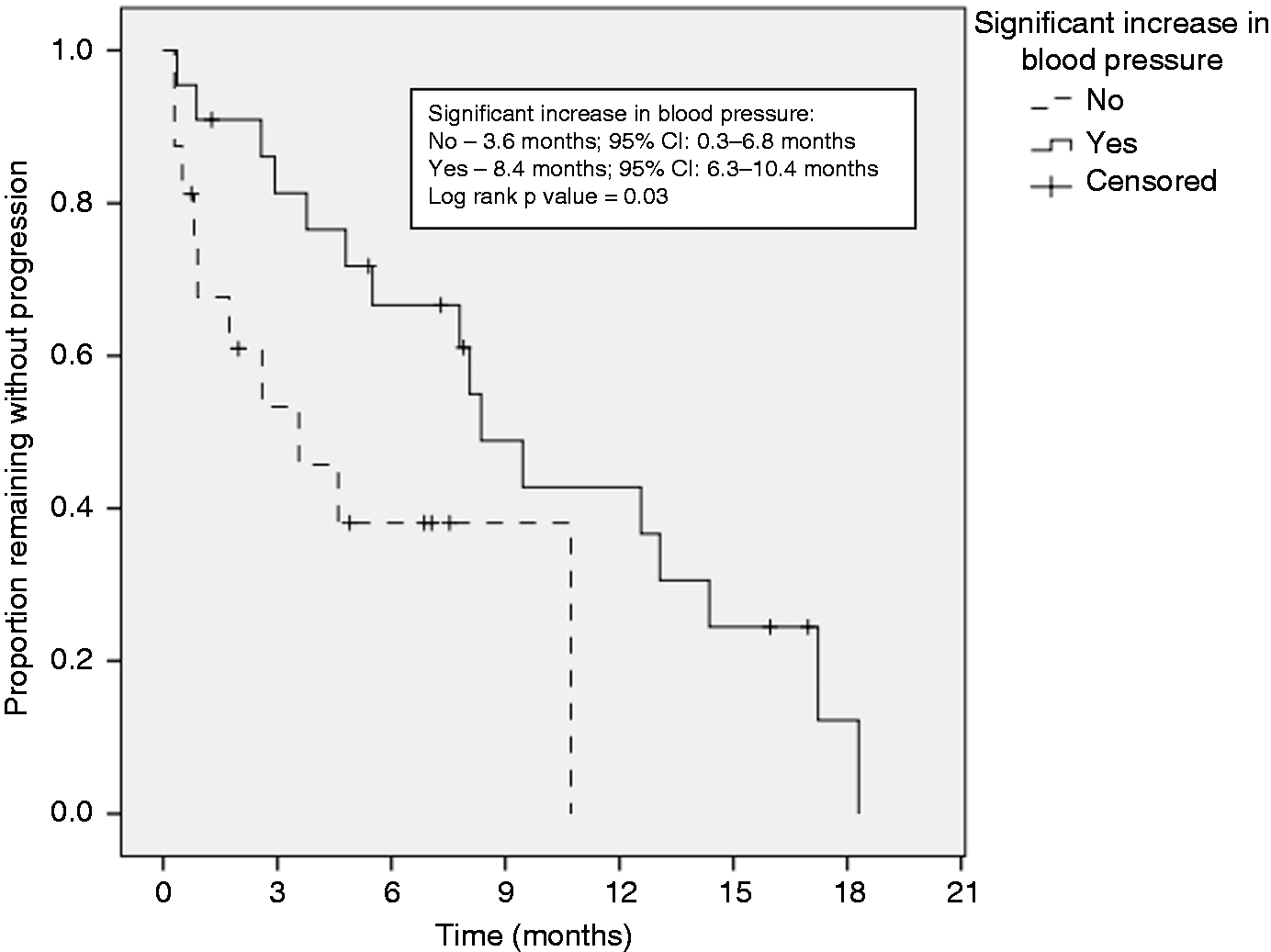
Tyrosine Kinase Inhibitor Subgroup: Time to progression in those with or without a significant increase in blood pressure.
Discussion
This study supports the hypothesis that patients experiencing elevated blood pressures may be more likely to respond to VEGF inhibitor treatment, as an increase in TTP was observed for patients experiencing a significant increase in blood pressure. Despite the presence of an adverse effect (elevated blood pressure), no difference was present in the incidence of discontinuation due to a documented adverse event. These results support the findings of a previous study of 39 patients receiving bevacizumab in combination with FOLFIRI for metastatic colorectal cancer which demonstrated a significant increase in PFS in those who developed grade 2 or 3 hypertension compared to those who did not (14 months vs 3 months). 8 Additional studies also document an increase in overall survival in patients experiencing hypertension due to anti-VEGF therapy. For example, a phase 3 trial investigating the addition of bevacizumab to paclitaxel in metastatic breast cancer patients (n = 363) demonstrated that those developing grade 3 or 4 hypertension had a greater overall survival (39 months vs 25 months). 9 Other small non-randomized, single arm studies with similar results have been reported with bevacizumab in patients with pancreatic cancer (n = 52), colorectal cancer (n = 39), and renal cell carcinoma (n = 43).8,10,11 However, in an analysis of seven phase 3 trials of treatment with bevacizumab, early hypertension (within 60 days) was noted to correlate with PFS in only one of the studies analyzed. 12 The results of that analysis may vary from others in that it focused on early hypertension development based on patient specific blood pressure values instead of CTCAE criteria. Likewise, the investigators postulated the differences were due to variability between trials and more intensive data capture and monitoring. While there is data supporting the correlation between development of hypertension and response to bevacizumab in the literature, the studies are limited to the addition of bevacizumab to chemotherapy regimens in one specific cancer type. 13 Our study investigated elevations in blood pressure at any time while on treatment and included patients with multiple diagnoses. In addition, this study utilized elevations in blood pressure instead of CTCAE criteria, similar to the analysis of early hypertension in 7 studies described above.
TKIs have also previously demonstrated correlations between the development of hypertension and response, with sunitinib demonstrating an increased overall survival in patients developing hypertension in one study of patients with renal cell carcinoma (median overall survival 30.9 months vs. 7.2 months).7,14 Our study supports this trend as the TTP was greater in those who experienced significant increases in blood pressure while receiving TKIs. Our study also included multiple oral TKIs beyond sunitinib, demonstrating that this association between hypertension and response may be a class effect.
Risk factors previously reported for the development of hypertension on treatment with a VEGF inhibitor include pre-existing hypertension, age greater than 60 years, and BMI > 25 mg/m2. 15 In our study, baseline characteristics were similar, including age and past medical history of hypertension. The only statistically significant difference was a lower baseline DBP noted in patients who experienced severe increases in blood pressure compared to those without significant increases in blood pressure. This might signify that patients with a lower initial diastolic pressure are at higher risk of developing more severe elevations in blood pressures which is opposite of the risk factors exhibited in prior studies. It could also be due to the fact that patients with lower baseline DBP had more room for which the DBP could increase; however, baseline DBP was similar between those with moderate increases in blood pressure and those without.
The incidence of significant elevations in blood pressure in this study was slightly higher than the incidence of hypertension in other studies. In a meta-analysis, grade 3 or 4 hypertension occurred in 0-19% of patients receiving treatment with bevacizumab or targeted therapies, compared to 27% with significant elevations in blood pressure in our study. 4 Similarly, another study reported 20% of patients treated with bevacizumab experienced grade 2 or 3 hypertension, compared to 60% in this study with significant elevations in blood pressure. 8 The incidence of hypertension with an anti-VEGF TKI may be higher than that reported with bevacizumab. In an analysis of 1,908 patients from 10 clinical trials with axitinib, all grade and severe hypertension occurred in 40% and 13.1%, respectively. 16 Discrepancies between our results and prior studies may be due our study utilizing an increase in blood pressure instead of CTCAE criteria for hypertension; however, it could indicate that hypertension may be more common in clinical practice when these agents are used outside of the controlled clinical trial setting.
Though patients with severe elevations in blood pressure required more therapy interruptions, discontinuation rates due to documented adverse effects were similar between groups. This may indicate that, with proper management, patients may be able to continue therapy and may not be at increased risk for additional adverse effects. Management of hypertension was not analyzed in this study; however, recommended therapies have included angiotensin converting enzyme inhibitors (ACE-I), angiotensin receptor antagonists (ARB), and dihydropyridine calcium channel blockers with a goal blood pressure of < 140/90 mm Hg.17,18 Recently, the efficacy of ACE-I and ARB therapy for the treatment of anti-VEGF therapy induced hypertension has been called into question. In a retrospective study of 316 patients with renal cell carcinoma receiving anti-VEGF TKI, the most effective blood pressure reducing agents were calcium channel blockers and potassium-sparing diuretic agents which were associated with 5.6 and 9.9 mm Hg decreases in SBP and 2.1 and 4.8 mm Hg decreases in DBP, respectively. 18 Usage of ACE-I and ARB therapy was not associated with improvements in blood pressure. Due to the increased duration of response demonstrated in patients experiencing hypertension, proper management of blood pressure is necessary to prevent premature discontinuation in a patient otherwise benefiting from therapy.
Limitations of this study include its retrospective nature, reliance on documentation within the electronic health record, and limited number of patients receiving oral TKIs. Despite these limitations, this study included multiple VEGF inhibitors used to treat a variety of oncologic diagnoses and contained comparable patient characteristics between groups. Even though the subgroup of patients receiving oral TKIs was relatively small, a TTP benefit was observed in those with significant increases in blood pressure. Including a variety of cancer types and multiple agents allowed this study to include a greater number of patients than many of the previously reported studies.
Conclusion
Development of significant increases in blood pressure may be a marker of therapeutic response to various VEGF inhibitor therapies and does not appear to limit treatment duration based on similar discontinuation rates due to adverse effects among groups, even in those with more severe blood pressure elevations. Additional studies are necessary to determine the impact of the development of hypertension on other patient outcomes, such as cardiac outcomes, and to determine the optimal management of this adverse effect.
Footnotes
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.