
Abstract
Background
The incidence of human epidermal growth factor receptor 2 (HER 2) positive breast cancers is rapidly rising worldwide. Although there have been many studies on HER 2 breast cancer treatment and management in recent years, there is a lack of comprehensive reports on the treatment outcomes and disparities within the available literature. Hence, this review aimed to determine the treatment outcomes and their associated factors among patients with HER2-positive breast cancer.
Methods
A computer-based systematic literature search was conducted using PubMed, EMBASE, and Google scholar databases of articles published from 2000 to 2020. The following key terms (HER 2 positive breast cancer, predictor, determinant, associated factor) and Medical Subject Headings (MeSH) terms (breast neoplasms, treatment outcome, and risk factors) were used to search the English language published articles.
Results
In most studies, trastuzumab was the most commonly used treatment regimen used in combination with chemotherapeutic agents. Generally, most of the studies (15 studies) showed that the overall survival outcome was relatively higher after treatment among HER2 positive breast cancer patients. Nonetheless, two studies showed that the absence of significant change in the overall survival despite adequate treatment was given to the study participants. In addition, three studies demonstrated a partial response after treating HER2-positive breast cancer patients.
Conclusion
Generally, the overall survival outcome was relatively higher after treatment among HER2 positive breast cancer patients. The addition of trastuzumab in most of the studies has shown improvement in the overall survival and the disease-free survival rate of the study patients.
Introduction
Globally, cancer poses a major menace to public health and a fastidious threat to developing countries with healthcare systems ill-equipped to deal with complicated and expensive cancer treatments. 1
Due to the tremendous incidence of concurrent co-morbidities & complex treatment regimens in cancer patients, the risk of drug-related problems that ultimately influence the favorable treatment outcome is very significant. 2 Moreover, the development of secondary solid malignancy after long-term chemotherapy and radiotherapy is an emerging hurdle to health care providers. 3
Breast cancer is one of the most common forms of cancer among women globally. 4 There are five distinct molecular subtypes of breast cancer, which have been identified based on gene expression studies. These include luminal A, luminal B, human epidermal growth factor receptor 2 –enriched, basal-like, and normal breast-like. 5
Breast cancer can be further classified into distinct phenotypes based on the histopathological markers presented like estrogen receptor (ER), progesterone receptor (PR), and HER 2 activity. 6 The heterogenetic nature of breast cancer is essential in ensuring that the therapeutic regimen for a particular patient is tailored explicitly to make sure that the treatment is effective.
According to Asif et al., 7 approximately one in every five women newly diagnosed with breast cancer worldwide will have HER2-positive breast cancer. Amplification of the HER 2 activity is often seen in about 15%–25% of the total breast cancer cases. Overexpression of the receptor is considered an adverse prognostic factor that usually results in a more aggressive disease and a decreased disease-free survival period. 8
A significant breakthrough in managing this condition was targeted therapy initiation using biological agents such as trastuzumab. The drug is a recombinant monoclonal antibody targeting the HER2 receptors. Blocking the HER2 receptors will interfere with the typical signaling cascade and thus prevent the overexpression of the receptor activity. There has been an improvement in patients' therapeutic outcomes with metastatic, early node-positive, and node-negative HER2-positive (HER 2) invasive breast cancers when this drug was used. 8 The response to therapy is also enhanced when the drug is added to other chemotherapeutic regimens. 9
Although there have been several studies on HER 2 positive breast cancer over the past few years, much remains unknown due to the lack of comprehensive reports and the disparities present within the available literature. The major barriers to achieving the desired treatment success in HER2 breast cancer patients include the cost of treatment, HER 2 therapy resistance, non-adherence to the treatment regimen, and a general lack of extensive knowledge about the disease. 10 Therefore, this review aimed to determine the treatment outcomes and associated factors among HER 2 positive breast cancer patients.
Methods
A systematic search of the literature was conducted to identify relevant published studies between 1st January 2000 and 17th September 2020 focused on the treatment outcomes of HER2 positive breast cancer patients. The review protocol was registered in the International Prospective Register of Systematic Reviews (PROSPERO) (Registration number: CRD42020206527), and the published methodology is available from https://www.crd.york.ac.uk/prospero/display_record.php?RecordID=206527 (11)
Inclusion and exclusion criteria
Articles published in the English language between the years 2000 and 2020 on HER 2 positive adult (≥18 years) breast cancer patients with the focus of treatment outcomes were included in the review. Nonetheless, a patient population with unknown HER2 status, studies with a lack of comprehensive report in treatment outcomes, studies with limited access to the full articles, and published in other languages were excluded.
Data sources and search strategies
A computer-based systematic literature search was carried out using PubMed, EMBASE, and Google scholar databases of articles published from 2000 to 2020 with reference to the PRISMA (Preferred Reporting Items for Systematic reviews and Meta-Analysis) guidelines. The following key terms (HER 2 positive breast cancer, predictor, determinant, associated factor) and MeSH terms (breast neoplasms, treatment outcome, risk factors) were used to search the English language published articles. Boolean operators such as “OR” and “AND” were used to join related items during the search of the relevant studies (Appendix 1). All search results from each database were saved in the individual electronic databases and exported into Covidence software for screening.
Article screening process
Records from different electronic sources have been exported to Covidence software. After removing duplicate records, both authors (AY and AD) did the initial title and abstract screening using three categories (yes, no, maybe). Both authors (AY and AD) carried out the full-text screening separately, and a consensus was reached after a thorough examination of any discrepancies.
Data extraction and synthesis
Using a structured data abstraction format in Microsoft Excel, two authors (AY and AD) independently extracted the relevant data. The data obtained included the study's characteristics (name of the author, study design, sample size, study population, treatment regimen, tools used to assess treatment outcomes), and the findings (overall treatment outcomes and associated factors). Any inconsistencies during the data extraction process were resolved through rigorous discussion.
Methodological quality assessment of studies
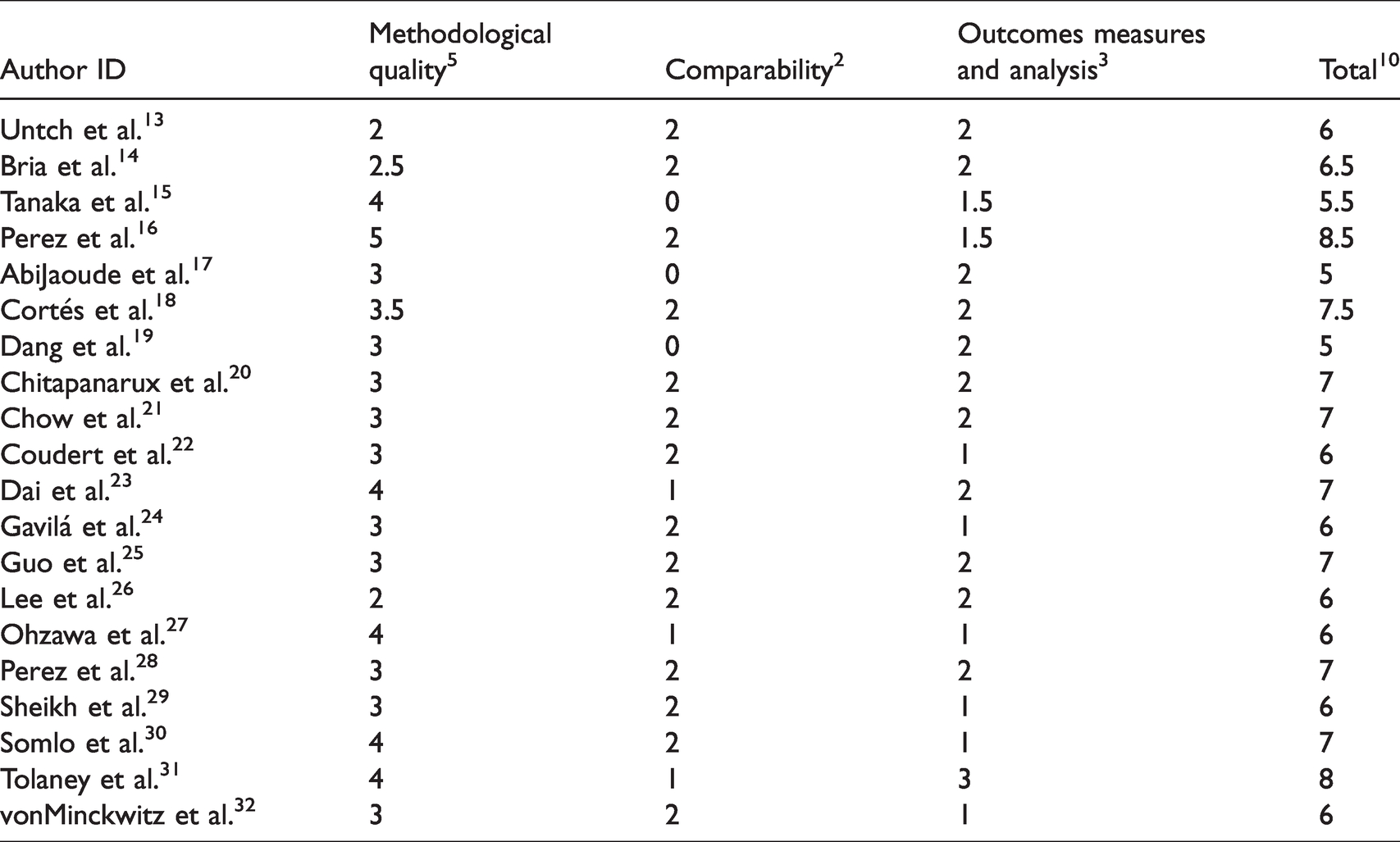
The methodological consistency and risk of bias of the included studies (AY and AD) were independently evaluated by two authors using the Newcastle-Ottawa scale, 12 which rates study quality out of 10 points. The instrument contained significant indicators classified into three major domains for ease of evaluation. The first section measures the methodological quality of a study of up to five stars. The second section considers the comparability of the study and takes two stars, and the remaining section assesses the outcomes of studies with related statistical analysis. This critical review was undertaken to determine the internal and external validity of the included studies. The mean score of two authors (AY and AD) was taken for the final decision and studies with a score of five and above were included in the final analysis (Table 1).
Quality assessment of included studies using Newcastle-Ottawa scale.
Outcome measures
The overall treatment outcomes were determined using overall survival rate, rate of progression or metastasis, pathologic complete response, progression-free survival, and the disease-free survival rate.
Data analysis
The data retrieved from the studies included were entered in an excel spreadsheet and summarized in tabular form. The potential predictors of treatment outcome were summarized from the regression analysis report from all the included studies.
Results
General description of the included studies
From 169 articles imported for screening, 70 studies were removed due to duplication. Out of 99 articles screened for title and abstract, 36 articles were irrelevant and excluded in the full-text screening. Sixty-three full-text studies were assessed for eligibility, and then 43 of the studies were excluded due to the wrong outcome (38 studies), study design (2 studies), and study population (3 studies) (Figure 1).
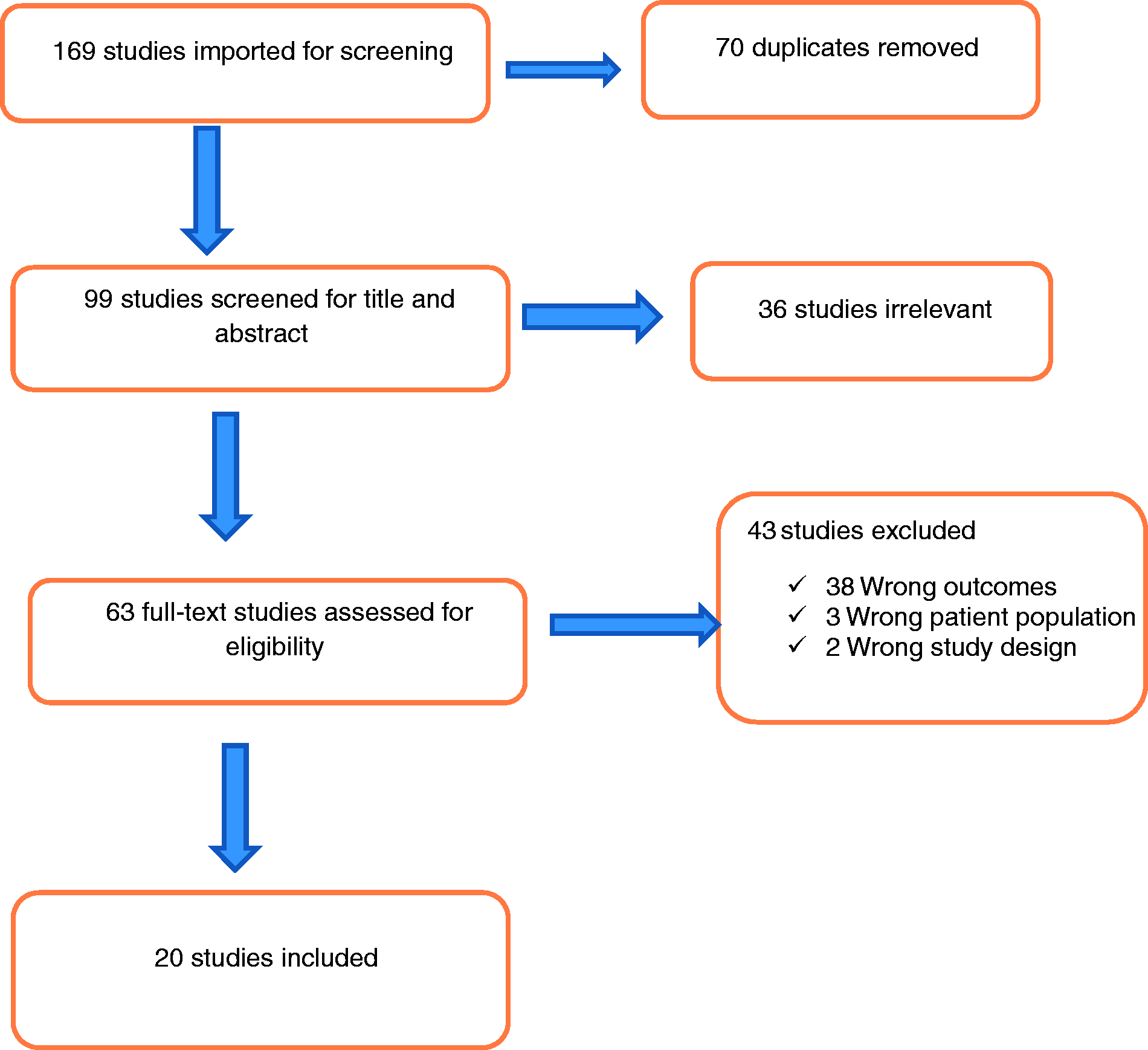
Flow diagram of study identification and selection.
A total of 20 studies encompassing 12,015 participants were included. The number of participants varied, with the largest number being 4045 patients and the smallest number being 24 patients. The earliest published work was in 2007 and the most recent having been published in 2019. Besides, most of the studies were randomized controlled trials, and the population ranged from early-stage to the metastatic stage of HER2 positive breast cancer patients (Table 1).
Treatment outcomes among HER 2 positive breast cancer patients
In most studies, trastuzumab was the most commonly used treatment regimen used in combination with chemotherapeutic agents. Furthermore, there was significant heterogeneity in the treatment outcome measuring parameters among the studies. The mean percentage of pathologic complete response among the four studies was 35.175%. Another two studies showed that the triple combination of chemotherapy had a high pathologic complete remission rate among HER2 positive breast cancer patients. Besides, few studies (3 articles) demonstrated that the progression-free survival time was long after chemotherapy in those patient populations. The present review also revealed that the trends of survival rate were relatively higher across the studies. Generally, most of the studies (15 studies) showed that the overall survival outcome was relatively higher after treatment among HER2 positive breast cancer patients. In addition, the addition of trastuzumab to the treatment regimen has been shown to increase the overall survival rate for the patients and increase the duration of the recurrence-free survival period. Nonetheless, two studies showed that the absence of significant change in the overall survival despite adequate treatment to the study participants. In addition, three studies demonstrated a partial response after treating HER2 positive breast cancer patients (Table 2).
General characteristics of the included studies and treatment outcomes among the study participants.

RCT: randomized controlled trial; HER-2: human epidermal growth factor receptor 2; CMF: cyclophosphamide, methotrexate and fluorouracil; AC: doxorubicin and cyclophosphamide; CEF: cyclophosphamide, epirubicin and 5-fluorouracil.
Predictors of treatment outcome
Although most of the studies did not report the predictors of treatment outcomes, the present review revealed that neoadjuvant lapatinib therapy, trastuzumab combination therapy, and heat shock protein 90 overexpression were the most commonly identified positive predictors of treatment outcome among the HER2 positive breast cancer patients. Nonetheless, pertuzumab monotherapy and type 2 diabetes co-morbidity had a negative impact on treatment outcomes (Table 3).
Predictors of treatment outcomes of HER 2 positive breasts cancer patients.

(+)Positive impact on treatment outcomes.
(−)Negative impact on treatment outcome.
Discussion
Based on the 20 articles reviewed, the treatment outcome was measured using the overall survival rate, the recurrence rate, rate of metastasis or disease progression rate, and the disease-free survival rate. Hence, this systematic review will provide the overall survival outcomes of treatment in HER2-positive breast cancer patients. Most of the studies were randomized controlled trials, and the population ranged from early-stage to the metastatic stage of HER2 positive breast cancer patients. Treatment-wise, the predominant proportion of the studies showed the frequent use of a trastuzumab-based monoclonal antibody in combination with the other chemotherapeutic agents. This review's finding is in line with the previous report, which showed that the trastuzumab-based regimen was the most effective and tolerable treatment regimen in this type of breast cancer. 33
Traditionally, HER2-positive breast cancer has been associated with a poor prognosis. Nevertheless, treatment with HER2-targeted therapy has altered the natural history of this disease. 34 Similarly, most of the studies (15 studies) in this review showed that the overall survival outcome was relatively higher after treatment among HER2 positive breast cancer patients. Furthermore, the trends of survival were relatively higher across the studies. This could be probably due to the inclusion of targeted therapies in the treatment regimens among the patient population. A previous study showed significant improvement when trastuzumab was combined with other chemotherapeutic regimens. 35 The patients, in this case, showed an increased survival rate and had an overall reduction in the risk of recurrence of the disease by 40–50%. Gullo et al. 36 also reported that HER 2 positive metastatic breast cancer patients could achieve complete remission after co-administration of chemotherapy and trastuzumab.
Likewise, this systematic review showed that the addition of trastuzumab-targeted therapy to the treatment regimen had been shown to increase the overall survival rate for the patients and increase the duration of the recurrence-free survival period. This review finding is similar to another systematic review, which showed that lapatinib's addition to trastuzumab could significantly improve overall survival in patients with HER2-positive breast cancer. 37 Besides, another systemic review also reported that the combination of trastuzumab with chemotherapy demonstrated a lower risk of death and relapse in the early stage of HER2 positive breast cancer, 38 which corroborates the frequent use of this combination therapy in most of the included studies in this review. Nonetheless, two studies showed that the absence of significant change in the overall survival despite adequate treatment was given to the study participants. In addition, three studies demonstrated a partial response after treating HER2 Positive breast cancer patients. This variation could probably be due to the study subjects' clinical characteristics such as performance status, co-morbidity status, and age.
Although most studies did not report the predictors of treatment outcomes, neoadjuvant lapatinib therapy and trastuzumab combination therapy was the main positive predictors of treatment outcome. Correspondingly, a similar systematic review reported that the combination of lapatinib plus capecitabine was the key determinant of overall survival of HER2 positive breast patients. 39 Nonetheless, pertuzumab monotherapy and co-morbidity (type 2 diabetes) were the significant negative predictors of treatment outcomes. In contrast, a previous meta-analysis showed that the combination of pertuzumab, trastuzumab, and docetaxel was a positive predictor of overall survival in HER2 positive breast cancer patients. 40
Strengths and limitations
The systematic search of multiple databases and methodological quality assessment using standard tools were the main strengths of this systematic review. Inconsistencies in the methodologies and reporting system of the results were the major limitation. Besides, the fact that the review did not include articles written in other languages may have resulted in the omission of pertinent information.
Conclusion
Generally, the overall survival outcome was relatively higher after treatment among HER2-positive breast cancer patients. The introduction of targeted therapy has resulted in a safer and more efficient treatment alternative for HER 2 positive breast cancer patients. The addition of trastuzumab in most studies has shown dramatic improvement in the overall survival and the disease-free survival rate of the study patients.
Footnotes
Acknowledgments
The authors would like to acknowledge United States International University-Africa for their internet support towards this systematic review.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Data availability
The datasets used during the current review are available from the corresponding author on a reasonable request.