
Abstract
Introduction
There is a need for an economic evaluation of the use of closed system (CSTD) in chemotherapy compounding, especially in resource-constrained settings.
Objective
The objective of this study was to assess the cost saving of the management of cancer drug leftovers before and after introduction of CSTD associated with an extension of the beyond-use date (BUD) of cancer vials. A secondary objective was to estimate the level of minimization of drug wastage.
Materials and methods
This was a prospective, single-center study with two periods of two months each. The cost of drugs saved by using conventional systems (syringe and needle) without a closed system in the first period was compared to the cost of drugs saved by using the CSTD Chemoclave® system in the second period. The drug waste minimization rate compared actual drug waste to potential waste in Period 2.
Results
In Period 1, the amount of drug saved accounted for an average of 10.3% of the amount used in milligrams and the amount of drug wasted accounted for an average of 18.7%. In period 2, these proportions were 15.2% and 6.4% respectively. The CSTD generated an extra cost of 11,962.5 USD compared to the conventional system. The drug saved cost related only to the CSTD and the acquisition cost of the CSTD was a deficit of -7,444.95 USD and the cost saved from the compounding (CSTD and syringes) was a gain of 1,722.01 USD. The waste minimization represented an average of 72.5% ± 24.4% of potential waste.
Conclusion
The use of CSTD to extend the BUD allowed to reduce waste due to microbiological instability without adding an economic profit.
Introduction
The incidence of cancer is continuously increasing worldwide.1,2 Each year approximately 3,00,000 new cases of pediatric cancer are diagnosed in children aged 0–19 years.3–5 In developed countries with robust health systems, survival rates are better due to early, accessible detection and quality treatment. Low- and middle-income countries, in contrast, have difficulty managing this scourge. The survival rate for children with cancer in these countries varies around 20% and is four times lower than in high-income countries. This is because a large number of cancer patients do not have access to timely and quality diagnosis and treatment. 6 Indeed, the context of low and middle-income countries is characterized by limited health care resources, in terms of surgical, radiotherapy and drug treatments. This affects mortality rates. 7 Survival in these countries would depend mainly on annual public health expenditure per capita. In Morocco, the survival rate is estimated at 30%, which reflects the considerable efforts made since 2010, particularly the implementation of the National Cancer Prevention and Control Plan (NCPCP).8,9
The price of anticancer drugs has been rising steadily with the introduction of new molecules in the last decade. In addition, the prolonged disruption of cancer drugs in oncology pharmacy practice has significant clinical and economic impacts.10,11 At the same time, chemotherapy compounding continues to generate significant waste due to the physical-chemical instabilities of most anticancer drugs associated with the need for aseptic compounding. This situation generates enormous public health expenses and requires cost control solutions. Different strategies have been adopted over the years and have involved the centralization, the grouping of patients by therapeutic protocol, the appropriate selection of drug dosages, the use of closed-system transfer device (CSTD) and dose rounding.12–14
A previous study found that 6.1% of the annual cytostatic drug budget was wasted during the chemotherapy compounding process. This study assessed the practice of centralization and did not take into account the possibility of extending the microbiological stability of anticancer drugs. 15 The amount of drugs wasted accounted for an enormous burden on the annual drug budget. This situation demanded for ways to minimize anticancer drug waste in order to optimize the use of resources.
The CSTDs would extend the BUD and have been recommended for the compounding of anticancer drugs. 16 Thus, various studies have assessed the economic value of CSTDs for the compounding. The contexts, types of drugs, types of CSTDs, and the methods adopted for cost assessment were heterogeneous and the results not easily comparable.17,18 Most authors recommended that studies in a wide range of settings be carried out. Moreover, data in this regard are rare in low- and middle-income countries, especially in Africa.
The Rabat Children's Hospital is one of the three hospitals with a centralized chemotherapy preparation unit (CCPU) and benefiting from the NCPCP out of the ten hospitals that make up the Ibn Sina Hospital Center. It was the first hospital to introduce CSTD in the compounding of anticancer drugs in Morocco. The objective of this study was to assess the cost saved by reusing leftover cancer drugs before and after the introduction of CSTD in the compounding of chemotherapy. Our secondary objective was to estimate the level of drug waste minimization.
Materials and methods
Setting of the study
This was a prospective, single-center study carried out by the pharmacy of the children's hospital. Prior to February 2019, nurses and pharmacy technicians performed the chemotherapy compounding under the responsibility of the clinical department. The remains of vials were discarded immediately after the necessary dose was taken. Since March 2019, the hospital pharmacy has taken over this activity with the establishment of the CCPU led by a pharmacist and procedures for compounding and provision. This study has received the approval of the hospital administration.
Study period
The study was conducted in two periods of two months, April – May 2019 (Period 1) and July – August 2019 (Period 2). During the study, the pharmacist performed pharmaceutical analysis of prescriptions prior to compounding, and the release of batches.
In period 1, the compounding was done with conventional injection syringes equipped with needles following a written, validated and procedure-related guide of physico-chemical stability of anticancer drugs. This guide was designed based on the recommendations of the French Society for Oncology Pharmacy and European Society of Oncology Pharmacy, 19 the stabilis® database 20 and manufacturers' information. The required quantities of drugs for a compounding batch were deployed. The leftovers were reused within six hours.
In period 2, the preparation was carried out using a closed Chemoclave® system consisting of Spike (vial adaptor), spiros® connector (syringe adaptor) and an extension kit. 21 An additional secure, closed system delivery tubing was provided with the chemotherapy. The remaining drugs were reused considering an extension of microbiological stability from six hours to seven days while respecting the physico-chemical stability of each drug.
Data collection
In the first period, the following data were collected in milligrams (mg) for all anticancer drugs for each prescription: the prescribed dose, the amount of drug used, the amount of drug saved (AS1) by grouping the compounding, and the amount wasted.
In the second period, in addition to data collected in the first period, the amount of drug saved before conservation (ASB) within six hours was collected. The ASB is therefore derived from the grouping of the compounding whereas the amount saved (AS2) here is derived from the grouping and conservation by the CSTD. The ASB is the equivalent of AS1 of the first period. The amount saved by the closed system alone (ASC) is the difference AS2 and ASB (Figure 1). The extra cost or surcharge of materials is the additional cost generated by the CSTD i.e., the Spike, spiros® connector and extension kit for compounding; and the secure delivery tubing used for drug administration.
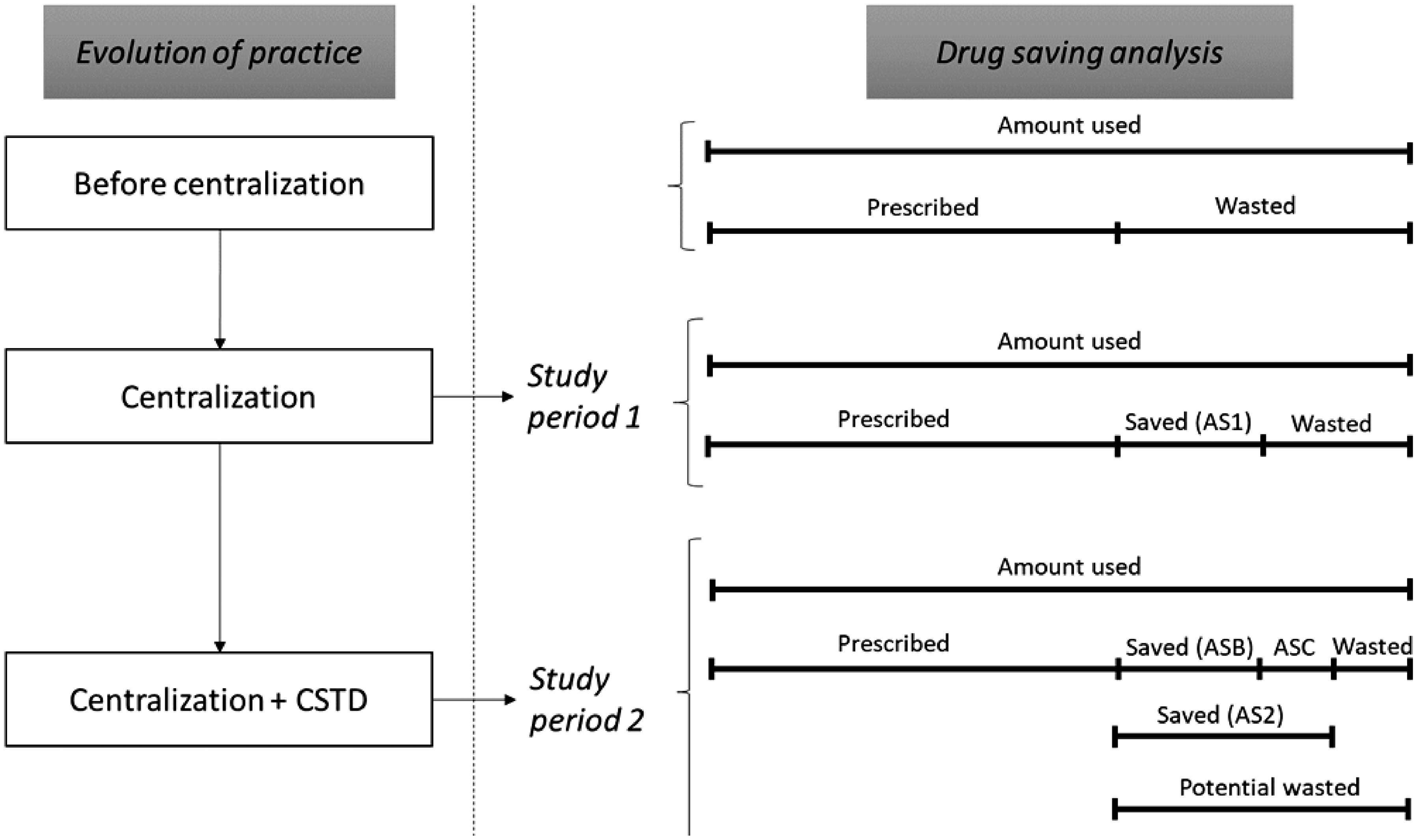
Flowchart of the study periods and drug saving analysis. AS1: Amount saved in period 1, AS2: Amount saved in period 2, ASB: Amount saved before conservation, ASC: Amount saved by CSTD.
Cost saving analysis
The savings were calculated based on the amount of drugs saved and the 2019 public hospital price of each product (Table 1). This cost is then expressed in US Dollars (1 USD = 9.62 Dirhams; year 2019). The cost saved by the use of the CSTD was obtained in two ways: in scenario 1, by deducting only the extra cost of the CSTD from the ASC and in scenario 2, by deducting the material acquisition cost (syringes and CSTD) from the AS2.
Drugs, dosages and prices used in the study.
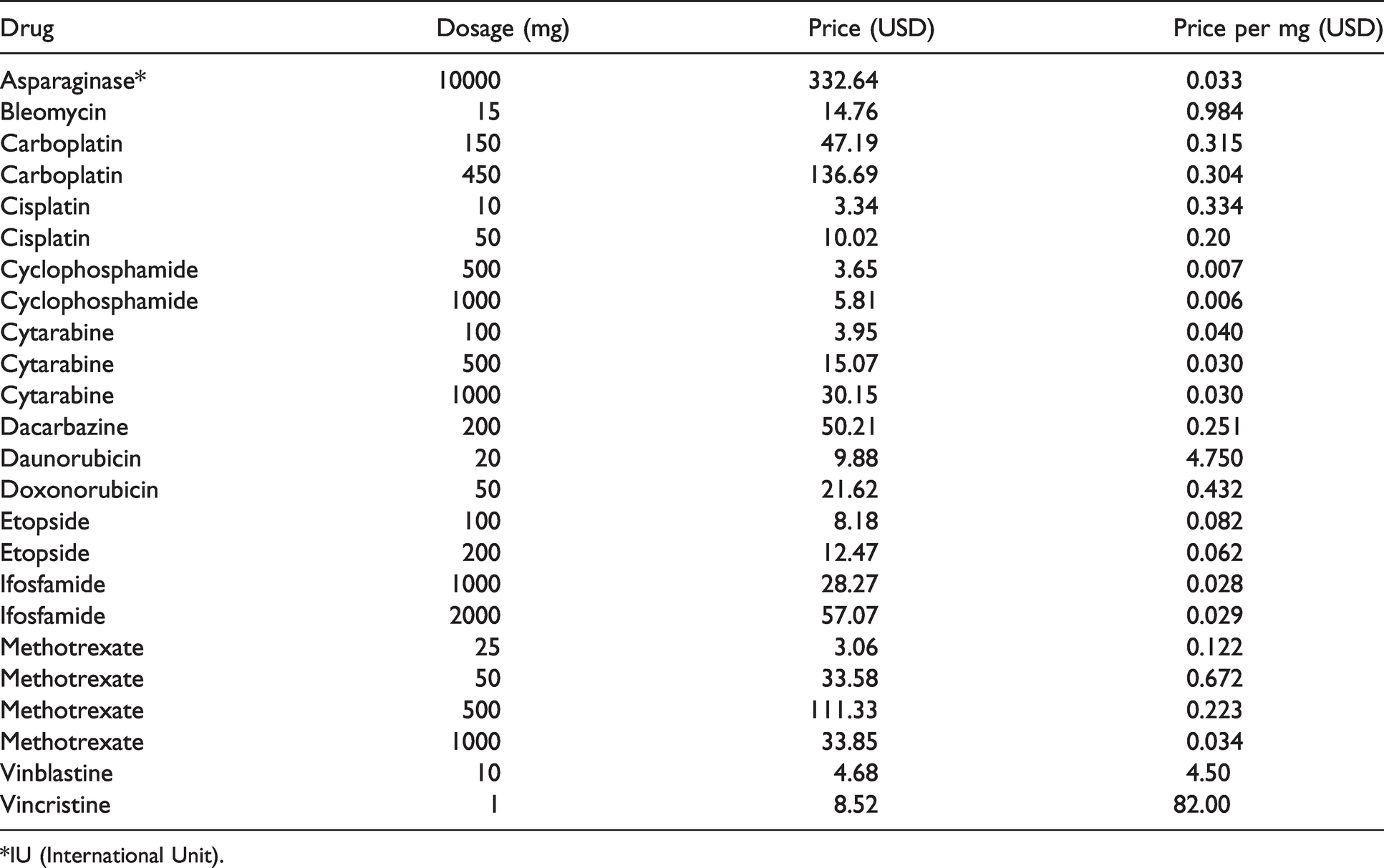
*IU (International Unit).
Drug waste minimization analysis in period two
Drug Waste minimization was a relative difference considering the potential waste (PW) in mg of drug without CSTD and the real waste (RW) in mg with CSTD during the second period of the study. It concerned all the drugs included in the study except two drugs that were not reused after preservation. These were asparaginase because of its physicochemical stability of 24 hours and vinblastine because of its low frequency of administration (less than one per week).

Results
During the first study period, the total amount of drug used was 877149 mg (141,260.4 USD) corresponding to 1446 preparations. The amount of drug saved by the centralization AS1 was 65841.16 mg (8,602.7 USD). This amount accounted for an average of 10.3% of the amount used in milligrams (Table 2). This represented over one year, 1.24% of the cytostatic drug budget for the year 2019. The amount of drug wasted had an average of 18.7% of the amount used. The distribution of the amount wasted per drug is shown in Figure 2.
The amount of drug saved, its proportion and the associated cost during the first period of the study.
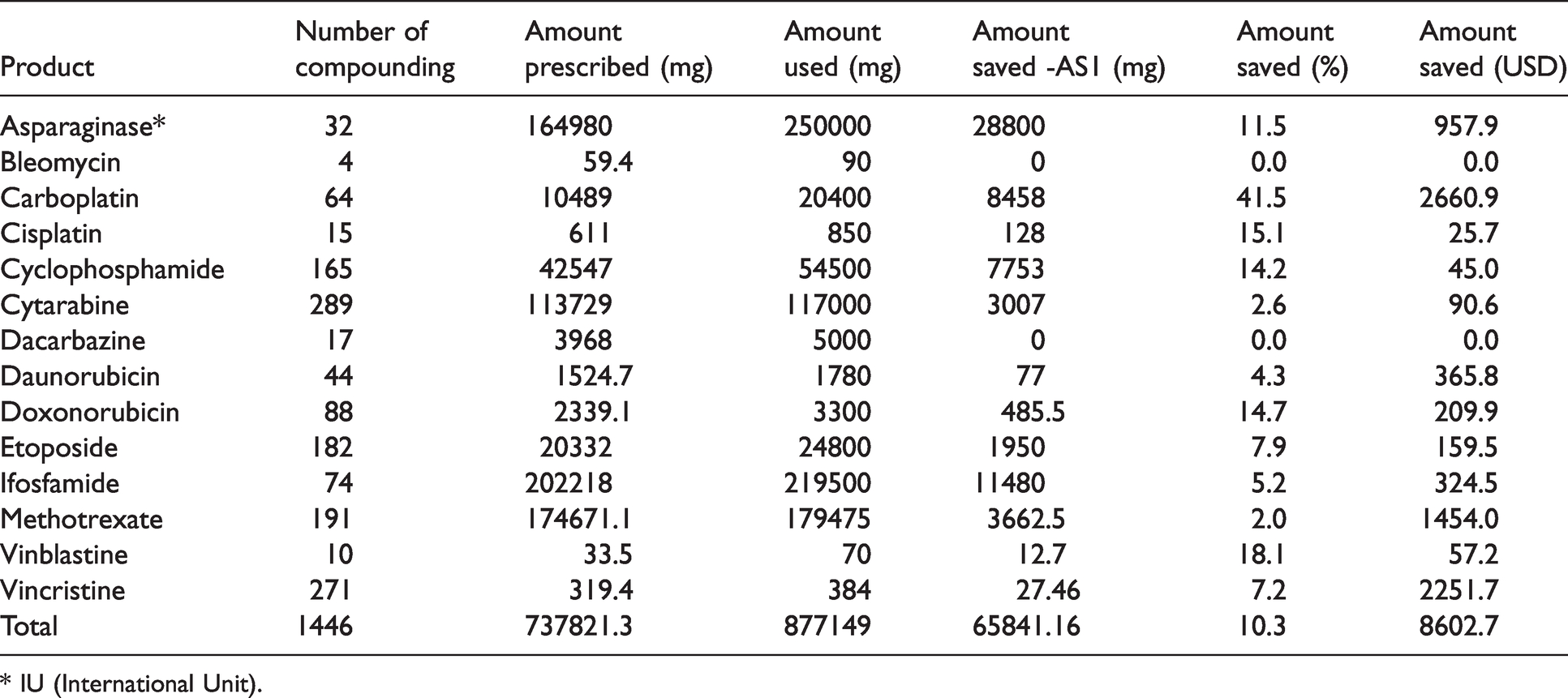
* IU (International Unit).
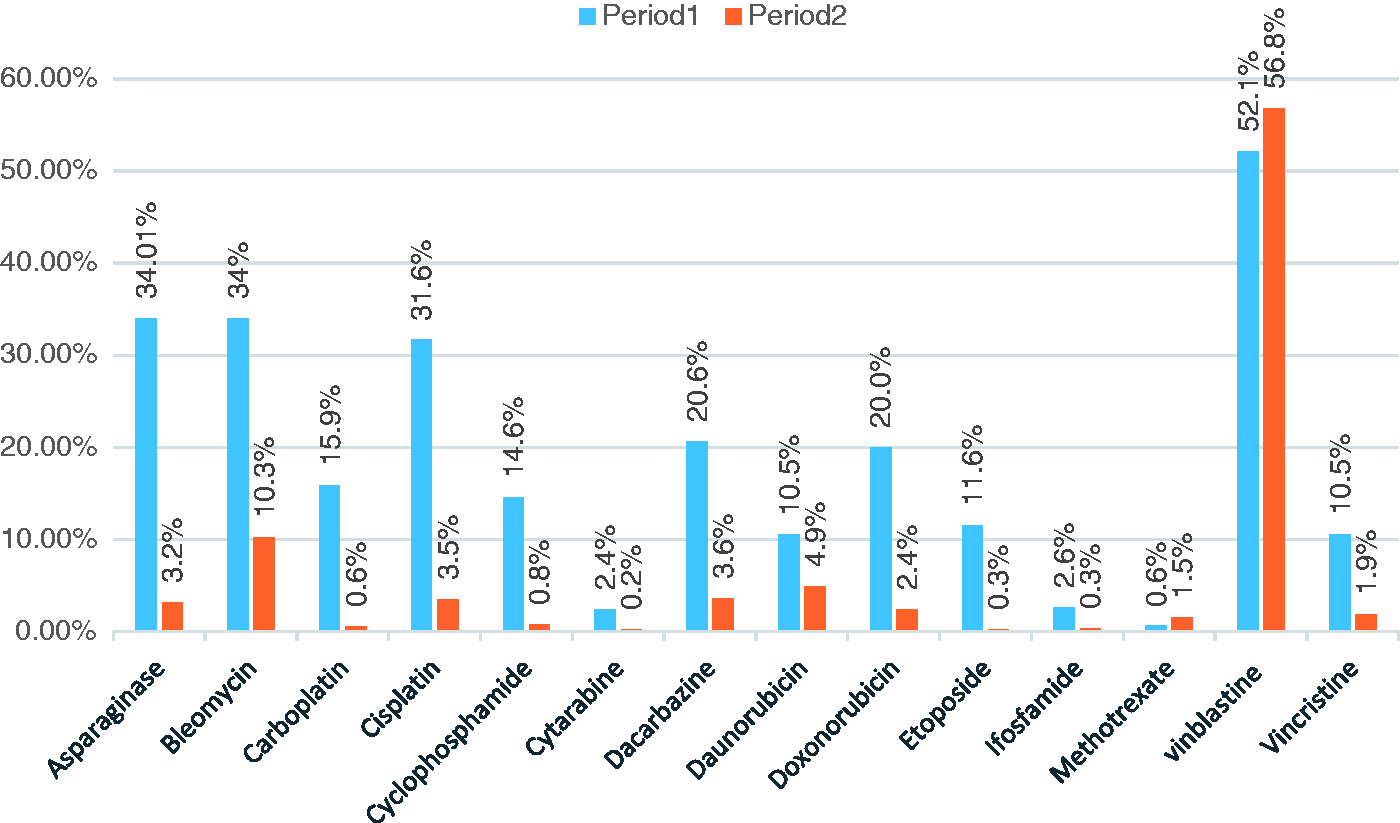
Variation of drug waste percentage from period one to period two.
In period two of the study, the total amount of drug saved AS2 was 98746.3 mg (13,684.5 USD); this was an average of 15.2% of the amount used. This amount represented over one year 1.97% of the cytostatic drug budget for the year 2019. The amount of drug saved before taking into account microbiological preservation using CSTD (ASB) was 56936.7 mg (9,167 USD). The amount saved by the closed system alone ASC was therefore 41809.6 mg (4,517.5USD) (Table 3). Taking into account the acquisition cost of the CSTD of 19,493.7 USD and that of the conventional system (syringes and delivery tubing without closed system) of 7,531.3 USD, the CSTD generated an additional cost of 11,962.5 USD. The secure delivery tubing generated 37.8% of this additional cost. The cost- saved related to the CSTD alone in scenario 1 was a deficit of -7,444.95 USD and the cost-saved of the compounding (centralization and CSTD) in scenario 2 was 1,722.01 USD. The amounts of drug wasted represented on average 12.7% and 6.4% of the amount used without and with the CSTD respectively.
The amount of drug saved before and after conservation, and the additional cost generated by the CSTD per product.
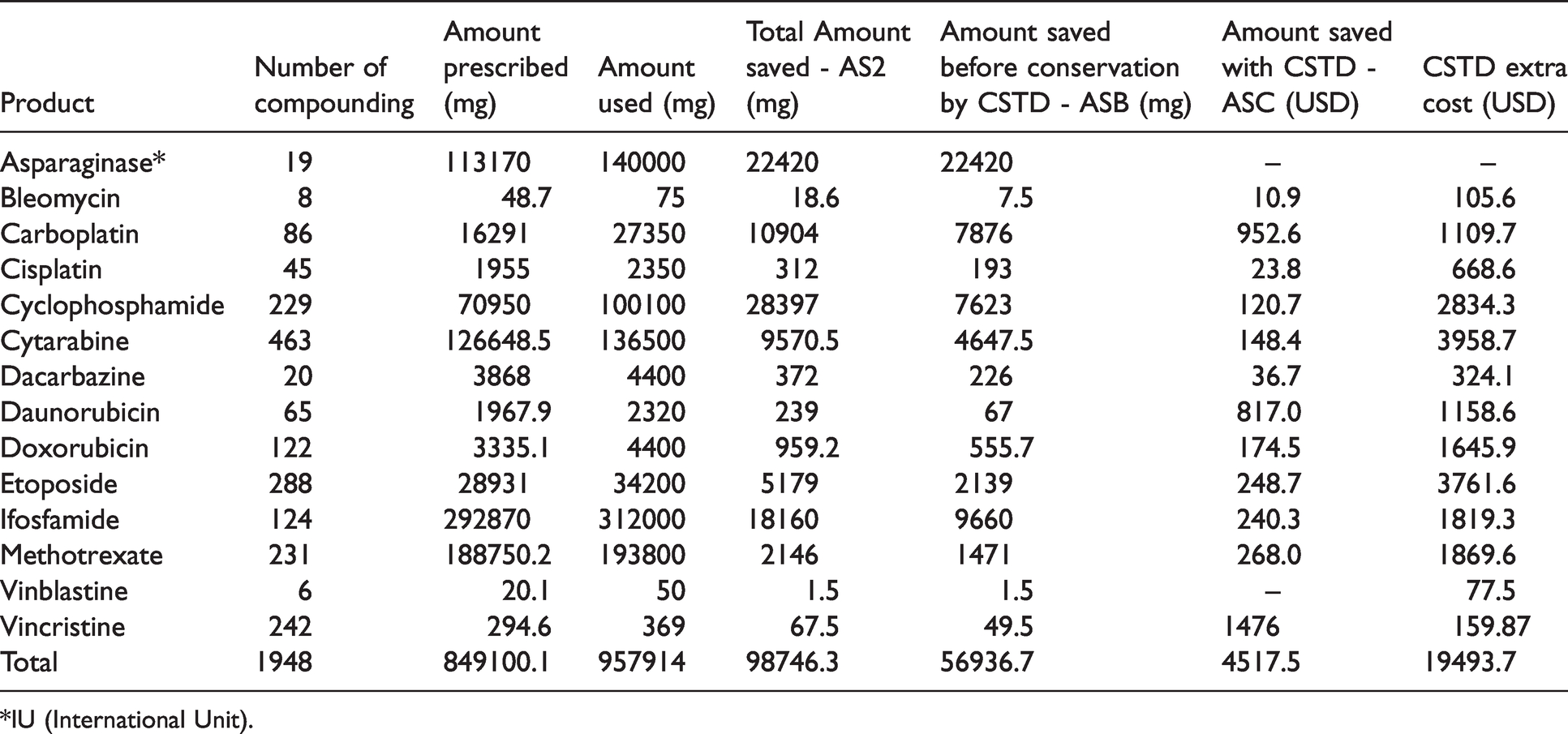
*IU (International Unit).
Waste minimization is estimated at an average of 72.5% ± 24.4%. This relative difference ranged from Methotrexate (18.9%) to Etoposide (97.1%) (Figure 3).
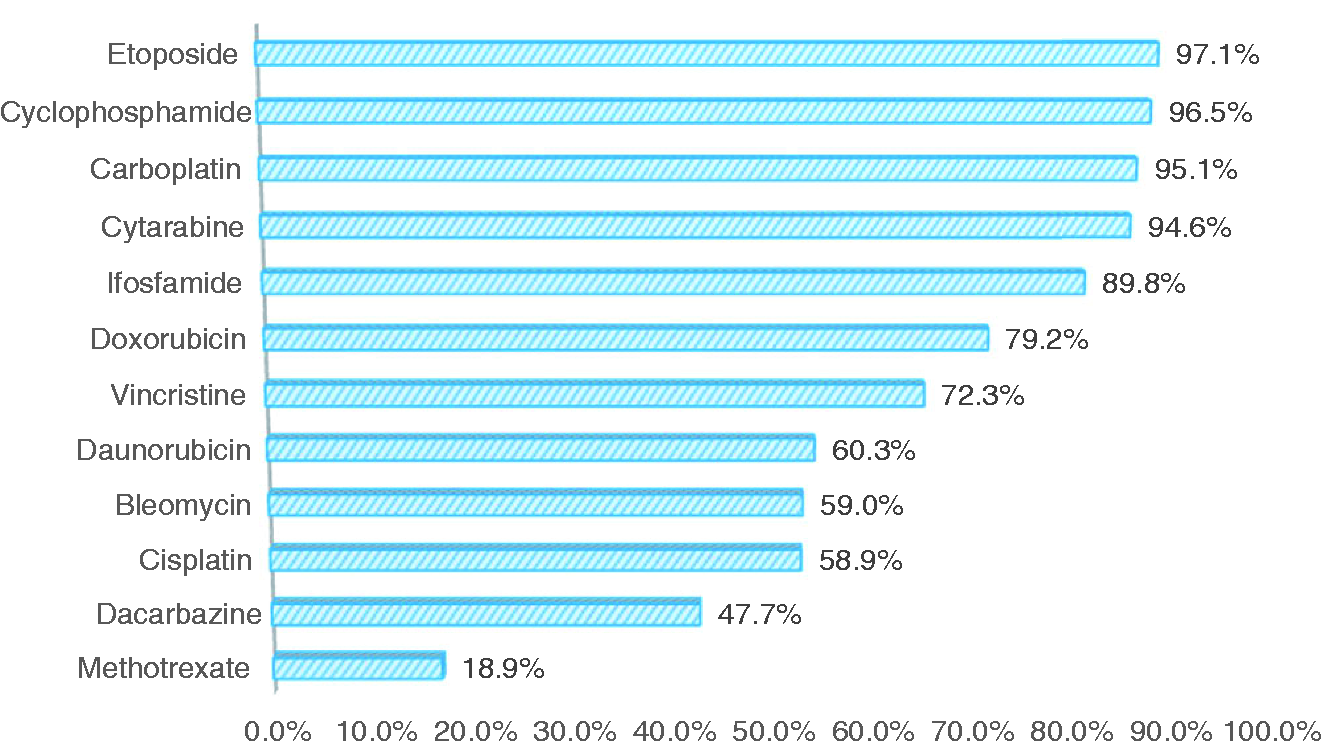
Drug waste minimization analysis based on CSTD utilization in period two.
During both study periods, the most frequently administered drug was Cytarabine (22.16%), followed by Vincristine (15.11%), Etoposide (13.85%) and Methotrexate (12.43%).
Discussion
The present study found a cost savings of 13,684.5 USD with the CSTD (period 2) and 8,602.7 USD without the CSTD (period 1). This represented considerable savings for the hospital in the same way as the other CCPUs in the hospital center sharing the same anticancer budget. Taking into account the acquisition cost of the CSTD and the savings of drugs made by the CSTD alone, the savings of its use was a deficit compared to the conventional system of compounding with syringes. We also estimated the waste minimization at an average of 72.5% of potential waste. Comparing the results of the two study periods, drug wastage was reduced from 18.7% to 6.4%. These results showed that the use of CSTD could reduce wastes due to microbiological instability by extending the BUD without offering an economic advantage over the conventional system. Akos et al conducted two similar studies in two periods in two different sized hospitals (240 beds versus 38) and found reductions in wastage between the two periods of 8.47% to 1.22% and 9.54% to 1.46%. In this study, the waste minimizations found of 64.14% and 83.58% of potential wastes bordered the 72.5% waste minimization in our study. However, we generated more waste. According to the authors, drug wastage can be inversely proportional to the size of the clinical department or the number of patients on therapy. 22
In this study, the limited availability of certain drugs, primarily asparaginase, cytarabine and etoposide, forced the adoption of a patient grouping approach. Thus, etoposide had the highest waste minimization rate (Figure 3). Other waste minimization strategies, such as selecting optimal dosages, dose rounding, and with satisfactory results, can be associated with CSTD use.17,23–25
Taking into account the proportion of drugs saved in the second study period, 15.2% in milligrams and 9% in USD, this savings in drug costs covered the additional CSTD-related costs for preparation and administration. Chan et al. found a similar proportion of 10.5% drug savings in USD that did not compensate for the costs of using PhaSeal® CSTD. The authors cited the widespread use of low-cost generic drugs in Malaysia as a likely cause of this finding. Considering that our study was conducted with generic drugs, a high acquisition cost of CSTD may also be the cause. Indeed, the acquisition cost of the CSTD can vary greatly depending on the location. 26
Other studies had shown that a cost saving was achievable by extending the BUD of open vials. Compared to the results of Edwards et al. based on similar types of anticancer drugs as in our study, the use of PhaSeal® CSTD was able to recover more leftover, 29% of the amount of drug used but generated more waste, 29.29%. 27 However, the amount of drug deployed may depend not only on patient-specific factors influencing the prescribed dose but also on the available drug dosages.
In this study, we estimated the proportion of drug savings achieved by the CSTD by dissociating it from that offered by the grouping of preparations in a centralized unit (scenario 1). This showed the value of introducing CSTD in antineoplastic drug compounding and can be used as a model for decisions in low-income countries. Rowe et al. demonstrated that if the BUD was extended from 6 hours to 2,43,648 or 72 hours using PhaSeal® CSTD, the respective percentages of waste calculated over two months in relation to total drug used would be 2.5%, 1.8%, 1.6% and 1.1%. The methodology of calculation in our study may be similar to this approach of estimating recovered residuals as a function of time. The proportions of wastes recovered were very small in this study even if, it was a simulation of real conditions in CCPU.16,28
The cost savings of the CSTD could not be limited to the savings resulting from the management of leftovers. Indeed, the CSTD reduces surface contamination and exposure of health care workers to cytotoxics.29,30 This is in favor of strict regulations on waste management and prevention of occupational exposure to antineoplastic drugs that would require use of safe means of compounding for manipulators. Similarly, the first period of this study showed a cost savings of 51,616.2 USD over one year due to centralized compounding and pharmaceutical management. This savings covered expenses related to the integration of a pharmacist that did not exceed 8,000 USD. However, the benefits of centralization should not be limited to the management of leftovers, as they also include the reduction of antibiotic consumption by ensuring sterile products. In addition, the value of the work of the pharmacist integrated into the team cannot be calculated solely based on the management of leftovers. Indeed, in CCPU, the pharmacist's tasks can also have clinical and organizational interests that can be valued and affect the entire chemotherapy circuit: supply, administration and therapeutic monitoring.31,32
This study included details of CSTD acquisition costs as well as taking into account the cost of the conventional system. This could help with decisions making. For example, eliminating the delivery tubing from the CSTD to make benefits would not be cost saving. In addition, it is a complementary system designed to protect stakeholders from preparation to administration and waste disposal. This study had typical limitations of a pharmacoeconomic study, as several factors were cited that could influence the calculation of costs. However, the proportions in quantity of drugs saved and wasted remain strong parameters for comparison. The economic analysis did not include indirect costs generated by the CSTD, for example for waste management. However, these costs can be considered unavoidable even in the absence of the CSTD (in a centralized system or not). In addition, this was a specific population and the study did not include monoclonal antibodies like rituximab that are rarely used in pediatric cancer patients. Another limitation of this study is that it did not include the risk of contamination of vials during conservation; this would assess the risk for patient safety.
Conclusion
The use of CSTD combined with the extension of the BUD for chemotherapy compounding resulted in a considerable reduction in drug wastage. This practice was not cost saving considering the savings generated by CSTD alone versus centralization and compounding with conventional means (syringes and needles). The results of this study provide an economic assessment model applicable to CCPUs in low- and middle-income countries, using mainly generic drugs and wishing to apply CSTD. Research on the economic evaluation of CSTD and its applications in oncology pharmacy remains desired.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.