
Abstract
Radiations dissipated are high energy waves used mostly as treatment intervention in controlling the unwanted multiplication of cell. About 60%–65% of cancer treatment requires radiation therapy and 40%–80% of radiation therapy causes RINV which are true troublemakers. Radiation therapy (RT) is targeted therapy mostly used to treat early stages of tumour and prevent their reoccurrence. They mainly destroy the genetic material (DNA) of cancerous cells to avoid their unwanted growth and division. The RINV affects the management and quality of life of patients which further reduces the patient outcome. RINV depends on RT related factors (dose, fractionation, irradiation volume, RT techniques) and patient related factors like (gender, health conditions, age, concurrent chemotherapy, psychological state, and tumour stage). RT is an active area of research and there is only limited progress in tackling the RINV crisis. Advanced technological methods are adopted that led to better understanding of total lethal doses. Radiation therapy also affects the immunity system that leads to radiation induced immune responses and inflammation. Radio sensitizers are used to sensitize the tumour cells to radiations that further prevent the normal cell damage from radiation exposure. There is a need for future studies and researches to re-evaluate the data available from previous trials in RINV to make better effective antiemetic regimen. The article focuses on radiation therapy induced nausea and vomiting along with their mechanism of action and treatment strategies in order to have a remarkable patient care.
Keywords
Introduction to radiation therapy
The radiation therapy (RT) also called radiotherapy is a physical agent or external beam used to destroy cancer cells and in lower doses used in X-rays for imaging purposes. The radiation used in radio-oncology are called ionising radiations as they form ions and deposit energy in cells of the tissues which can kill malignant cells leading to cancer cell death. The high energy radiations can be transmitted in a controlled release pattern that specifically target the cancer cells and prevent the DNA from division and proliferation. Radiation therapies are often given as a treatment modality or for palliative care that aims in reducing the symptoms rather than curing the disease. Radiation therapy can be either used alone or along with chemotherapy, immunotherapy or surgery for treatment of cancer. They can be initiated before surgery (neoadjuvant) for easy targeting of the tumour, shrinking the size of tumour and to avoid complications, or during surgery (intra-operative) to target the exact tumour cells and to avoid harm to normal cells. It can be given as an adjuvant therapy after the surgical procedure to destroy any remaining cancer cells. Daily divided doses of radiation therapy are beneficial as they produce less tissue damage compared to large single doses. 1 Radiation induced nausea and vomiting (RINV) is the primary problem encountered by radiation therapy in cancer treatments. 2 80% of the nausea and vomiting symptoms are associated with RT that eventually has to be diminished as they may lead to major problems like dehydration and electrolyte imbalance. 3 The antiemetics are usually administered 1–2 h before the radiation therapy until the treatment with radiations are over. Side effects must be monitored especially in RT doses given for paediatric, geriatric, hepatic and renal impairment cases. 4 The total body irradiations (TBI) are most likely to cause RINV hence fractionated dose delivery is important here. 2 The total body irradiation (TBI) and half body irradiation (HBI) mostly affects the enteric system which contains emetic receptors to a greater extent and patients receiving such radiations are widely treated with serotonin receptor antagonists. 5 RT may take weeks or months for the DNA of the cancer cells to shrink in size or die off. Certain types of cancers when treated with the RT in early stages can get a higher level of cure rate. One of the major concerns of RT is that the cancer cells existing outside the radiation field are not destroyed with radiations. Hence clear imaging of the cancer cells is essential in proving this treatment modality a success.
Types of radiation therapy
This era is still in the process of understanding the remarkable advancements in the treatment modalities of radiotherapy in carcinogenesis. The most commonly used type are external beam radiation therapy (EBRT) or teletherapy and internal beam radiation therapy (IBRT) or brachytherapy. 6 The external beam radiations involve radiations transmitted from an external source such as a machine to specific body parts on the patient. This provides only a limited deposition of radiation on deeper tissues hence maximum dose accumulation occurs on the superficial area of the targeted area. The course of treatment of external beam RT can be 5 days in a week with concurrent time for normal cells to repair. External beam radiation therapy does not make the patient radioactive. Intra-operative EBRT are used during surgeries to target the localised tumours. EBRT are commonly performed in lung, hand and neck, prostate, breast, uterus, GI tract, brain cancers. 7
Brachytherapy (BRT) or internal beam radiation therapy involves the placing of a radioactive material inside a well protected catheter or needles and leaving them into the body. This can be a temporary method that involves the withdrawal of radioactive material after some time or can be permanent leaving them inside the body for several weeks. There can be small amount of radiations present on the body of such patients hence a distancing is preferred. The temporary set up of implants are kept for a specified period of time by patient in hospitalised days and removed before discharge. BRT are commonly used in prostate, breast, endometrial and cervical cancers. 7
There is an another method called systemic RT that involves the usage of radionuclide substance like radioactive I131 for thyroid cancer treatments, radio-labelled monoclonal antibodies injected to the blood that travels systemically to kill the cancer cells. They are capable of transferring low dose rate (LDR) of radiations by fractionated RT methods that prevents the normal cells from hypoxic conditions and immune suppressions. 8 However the minimisation of bystander effect and abscopal effect suggest systemic RT promising in the future. 9
Challenges and concerns related to radiation induced nausea and vomiting
There is always a need to control the emesis associated with RINV and CINV (chemotherapy induced nausea and vomiting) as they interfere with the potential results of therapy. Therefore RINV and CINV should never be underestimated as they adversely affect the life of a patient. There can be variations in the treatment schedule proposed to individual patients according to their emesis risk level and patient related characteristics. Individual patient mental status, anxiety levels can also be considered to prevent potential RINV. 5 To have an efficient outcome it is important to personalize the RT strategies by combining both patient related biological aspects and physical aspects of radiations. 6 The early stage identification of DNA damage of the non targeted regions is important as they help to reduce the complications of secondary malignant neoplasm. Minimisation of their occurrence is an important factor to achieve success in treatment plan. 10 Concerns related to CINV and RINV in geriatrics involve a high score in the frailty index which helps to identify the co morbid conditions if prevailing in geriatric patient that may interfere with the radiation treatments. This helps to increase the potency and efficiency of treatment strategies. Dose adjusted to hypo fractionated radiation therapy finds a better way for treatment implementation. 11 The tumour lethal doses may vary for different cancers 7 and people with variation in 5HT3B genome responds differently to 5-hydroxytryptamine 3 receptor antagonist (5-HTRA) therefore genomics must be considered for dosing . 12 However the major goal of RT remains to protect the normal tissues from radiation exposure, preserve quality of life (QOL) of patient, maximise cure rates and minimise the side effects related to therapy. 13
Possible mechanisms of radiation induced nausea and vomiting
The mechanism of action of RINV is not fully developed but to an extent is similar to CINV as they both share the same pathways and similar neurotransmitters. But although the similarity exists nausea are predominant than vomiting in case of radiation therapy. On initiating the radiation therapy the neurotransmitters are stimulated that causes an emetogenic reflux system activation that sends messages to brain which ultimately produces the nauseous and vomiting sensation. The neurotransmitters responsible for these signal transmissions are 5-hydroxytryptamine 3(serotonin), dopamine, neurokinin-1(NK-1). 14 The 80% of serotonins are released during the initial phase of radiation therapy due to the destruction of enterochromaffin cells of gastrointestinal tract. 15 There are larger presence of 5 Hydroxyindole acetic acid (5HIAA) metabolite in urinary output during chemotherapy that directly symbolizes the increased release of serotonin . The substance P released from neurokinin receptors are also responsible for emesis and is mostly concentrated on GIT. On the acute phase of emesis 5-hydroxytryptamine3 receptor antagonists (5-HT3 RAs) are given and during the delayed phase a substance P is released that binds to NK receptors hence neurokinin-1 receptor antagonists (NK-1 RAs) are preferred. However the cause of nausea is unknown but is apparently treated with antiemetic. There are immunoreactive compounds that react to the chemical ionizing radiations during the RT .The levels of arginine vasopressors and peptide YY are high during emesis but they are just the anticipatory indicators of fluid loss not associated with RINV.14,16
There are four parts responsible for the nausea and vomiting stimulation which include chemoreceptor trigger zone (CTZ), area prostema, the cerebral cortex and limbic system that shows response to smell, taste, pain and tensions. 17 The pathophysiology of RINV involves the chemoreceptor trigger zone (CTZ) called vomiting centre at the area prostrema region. They have the ability to alter the release patterns of neurotransmitters like serotonin by the triggers of chemical agents of chemotherapy. 18 Vomiting centre (VC) present at the medulla oblongata and CTZ present at the area prostrema. The CTZ and vagal afferent neurons send impulses to VC that activates the abdominal, salivary and respiratory centres that indeed cause vomiting. The three phases of vomiting include pre ejection, retching and ejection phase.18,19 Acute nausea and vomiting occurs within 24 h of chemo radiotherapy induced emesis. Delayed nausea and vomiting occurs after 24–96 h of radiation therapy. Breakthrough nausea and vomiting are most dangerous as they happen in between the therapy and renders it ineffective. Anticipatory nausea and vomiting occur due to the vomiting fear from the previous episodes of radiotherapy, mainly controls psychological thoughts. 16 Emesis can occur as a result of concurrent medications or complications related to radiations. 18
The major biological mechanism of radiation therapy involves breaking the DNA to single stranded forms present inside the cell thus prevents the malignant cells from further growth and proliferations. The radio sensitivity of the cancer cells towards radiation is an important factor to protect the normal tissue tolerance. 7
Nausea need not cause vomiting always but emesis is always triggered by nauseous stimuli hence their mechanism must be evolved in RINV. The cause of intractable nausea in the delayed phase must also be an area of radiation research. Genetic testing might be needed as alteration in 5HT3B receptors can change the binding to antiemetic agents. 13 The GI cancers including oesophagus, pancreas and liver are more prone to RINV. There are studies that states 5HT3RA are safe for gastro intestinal CINV which are useful treatment strategic norms for RINV as well. 20
Factors affecting radiation induced nausea and vomiting
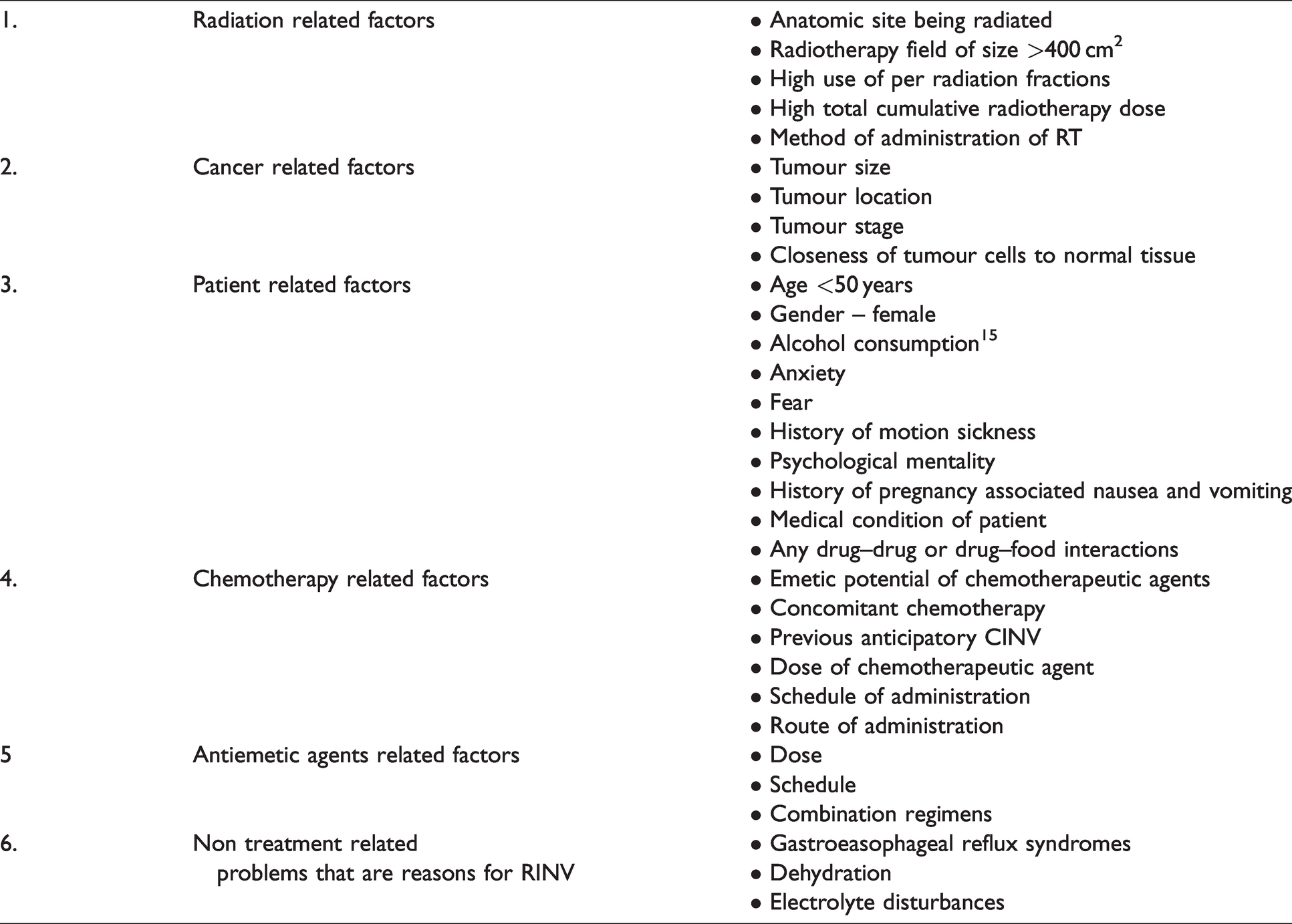
The antiemetic agents efficiency in RINV is not fully developed hence the following factors are considered prior to implementing radiation therapy (Table 1).2,5,14,15,18
Factors considered for RINV.2,5,14,15,18
Comparison of current guidelines for radiation induced nausea and vomiting
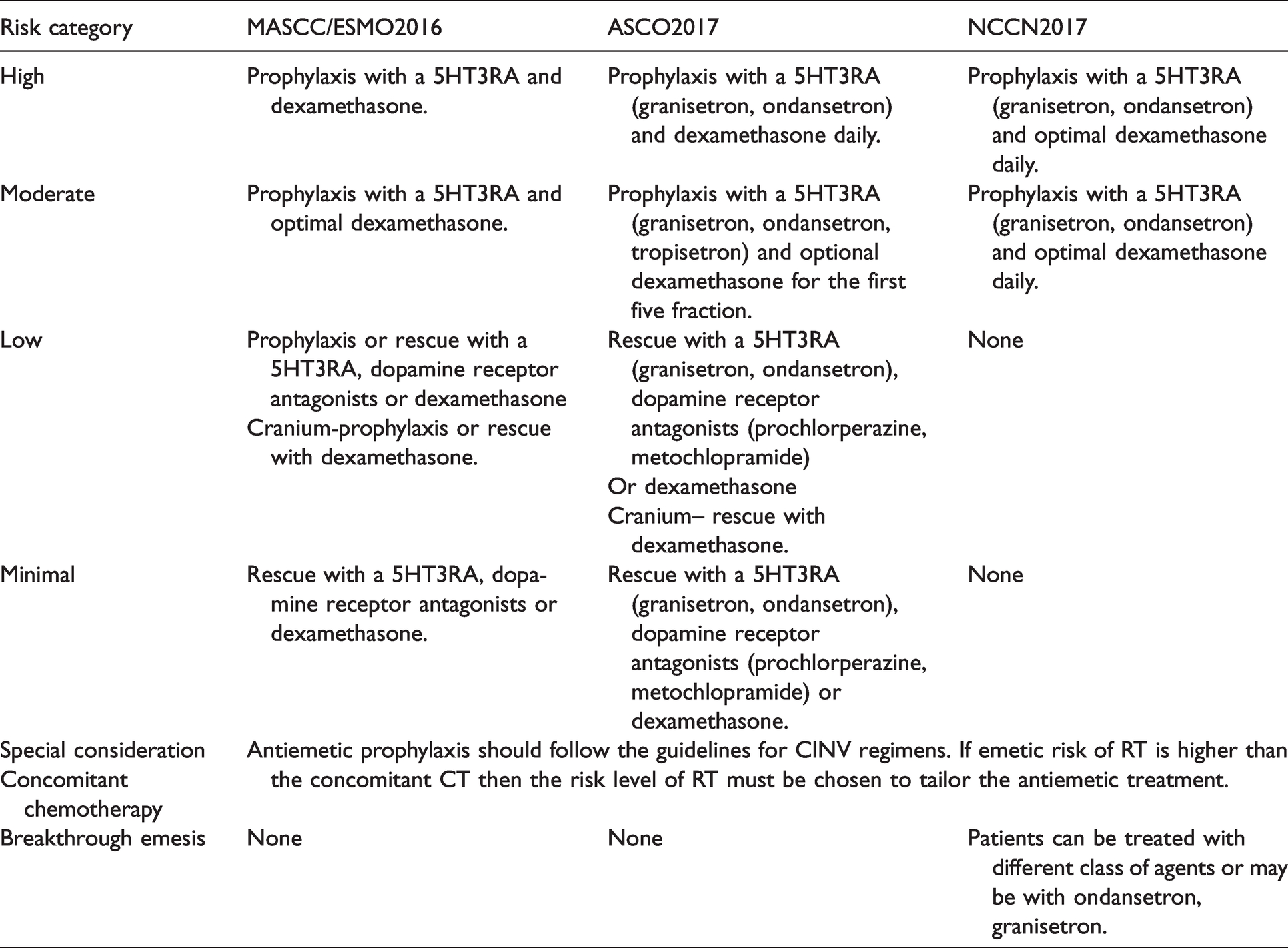
As RINV is a common and frequent event we need protocol and guidelines to treat it. The guidelines are prepared by reviewing the previous cases in clinics and their efficacy to cure diseases hence variations in the guideline can be brought to bring better clinical results. Following the guidelines can provide better patient outcome and adherence to antiemetic guidelines can bring higher results in RINV.3,4,21 Therefore clinical guidelines for antiemetic activity of RINV focuses on the emetogenic severity in an individual patient. 2 These include the American society of clinical oncology (ASCO), Multinational association of supportive care in cancer (MASCC) and National comprehensive cancer network (NCCN). Management of the symptoms related to a disease condition helps in improving the compliance and adherence to therapy which eventually improves the therapeutic outcome hence guidelines and their latest versions help the practitioners to rapidly recommend the treatment for quicker results. These guidelines are beneficial when put into practice that may further collaborate for improvement in adjusting the antiemetic and radiation doses (Table 2). 16
Latest comparison of RINV guideline.3,4,16,21
Therapeutic approaches in RINV including newer drugs and perspectives 11
Primary treatment involves the identification and implementation of measures to modify the risk factors. Secondary measures take up the antiemetic therapy. RINV is common phenomenon in cancer patients undertaking radiation therapy. The clinical manifestations of RINV can occur at any phase of treatment. As this makes a deter in the successful treatment plan they must be taken care of with appropriate antiemetic therapy. 14
5-Hydroxytryptamine receptor antagonists (5-HTRA)
The first generation include ondanstron, granisetron and dolasetron while second generation include palonosetron.14,22 The drugs namely ondansetron and granisetron are 5-HTRA that blocks serotonin release by binding to serotonin receptors. Studies show that the buccal film administration route of ondansetron is of greater importance in patients with the history of nausea and vomiting. Granisetron are having high selectivity towards the 5-HT3Rs hence used in chemotherapy and post surgery procedures. 5-HT3RA like ondansetron and granesetron are useful in case of total body irradiations. Palonosetron have a half life of 40 h greater than ondansetron and granisetron. They also have improved characteristics of delayed RINV and higher efficacy in high and moderate risk chemotherapy.3,17 They showed better results in combination with other antiemetic in CINV. 14 There can be toxic effects for the antiemetogenic agents that must be taken into considerations. The use of ondansetron in rectal cancer enhances the constipative effect. The cardiac adverse effects must be monitored in ondansetron and dolasetron. 21 5HT3RA are the mostly used antiemetic in chemotherapy for prophylactic prevention of emesis and has an effect that lasts for 24–48 h hence are good for acute phases of CINV. They can be provided to the patient until the radiotherapy begins and stops once the treatment begins. The granisetron and tropisetron bind irreversibly to the 5HT receptors and shows effects up to 48 h whereas the ondansetron binds reversibly to the serotonin receptors hence their effects can be ceased once displacement by serotonin neurotransmitters during the dose administration. 5HT3RA with or without dexamethasone are most widely used since the last two decades for RINV. Studies show that palonosetron along with prednisone and NK-1RA was useful in pregnant woman to prevent emesis for up to five cycles. 23 The uses of serotonin antagonists are used in analgesics, CINV, RINV, anaesthesia induced nausea and vomiting, post operative nausea and vomiting. Alcohol induces the dopamine and serotonin release hence 5HT3RA reduces the alcohol addiction symptoms to a small range. 24 The delayed and protracted effects of radiation therapy are not treated with 5HT3RA. They can be given orally, intravenously and subcutaneously with adequate check on their adverse effects. 16
Neurokinin 1-receptor antagonists (NK-1RA)
Aprepitant: They are used in delayed phases of RINV to prevent the release of substance P that stimulates nausea and vomiting. They are mainly used in combinations with 5-HT3RA or corticosteroids for higher efficacy. 14 There are studies proving the efficacy of combinations of dexamethasone, ondansetron, and aprepitants.12,17 Aprepitant are metabolised by CYTP3A4 hence caution required in hepatic impaired patients. Fosaprepitant are prodrug of aprepitant given mainly via IV. There are studies proving the efficacy of ondansetron, dexamethasone and fosaprepitant. There are certain drug interactions concerned with concomitant use of aprepitant and dexamethasone that increases the dexamethasone concentration hence dose reduction are recommended. Aprepitant with benzodiazepines also cause metabolisation of BZD hence higher doses of BZD given for effective results.17,19
Dopamine receptor antagonists
They include metochlopromide, prochlorperazine and haloperidol that prevent the release of dopamine responsible for the RINV. Of this the highly recommended and usually dispensed are metochlopromide. 14 There are evidences stating metochlopromide antiemetic as first line agent in advanced cancer states. Meanwhile metochlopromide can show neurological effects. 21 Metochlopromide is D2 receptor antagonists that act on CTZ, GI tract. Metopimazone they are phenothiazines that are antidopaminergic and antiemetic at CTZ. They are used in combination with ondansetron for CINV at high risk. 17
Corticosteroids
Dexamethasone: They are glucocorticoids that are used mostly in combination with 5HT3RA and NK-1RA to reduce the high degree of emetogenic effects related to radiation therapy. 14 The use of corticosteroids dexamethasone and 5HT3RA are useful in early stages of radiation induced vomiting for a period of 1–5 days. 23 The corticosteroids are mostly used as they are cost effective and mostly available. 4
Combined agents
Most of the antiemetic agents when given in combination show accelerated results. The combination of 5HT3RA and NK-1RA with ondansetron or granisetron, or a triple treatment regimen of 5-HTRA, corticosteroids and aprepitant, or a dexamethasone and NK-1RA also shows high range of blockage for emesis. Netupitant a combination of palonosetron and NK-1RA along with dexamathasone has a higher half lives hence reduces the dosing frequency. 14 There are beneficial results for suggesting the use of 5HT3RA and dexamethasone for upper abdomen and pelvic region radiation therapy. 15 The development of a single antiemetic is a challenge to overcome the RINV. There can be toxicities associated with the combination therapies. One such approach is the olanzepine in combination with 5-HT3RA, NK-1RA, dexamethasone and aprepitant shows greater results in cisplatin based chemotherapies as they have the ability to block multiple receptors of serotonin, dopamine, adrenergic, histamine and muscarinic. 21 The medications can be delivered in convenient forms like rapidly dissolving films for ondansetron that provided wide protection and higher control rates in acute phases itself. The granisetron transdermal delivery system that contain the same oral doses act as an adhesive and prolong the effect for seven continuous days that contain multiple fractionated chemotherapy. There is a controlled sustained release pattern that has higher control, higher response rates. These advancements as proven clinically effective in CINV and can be reproduced in RINV as they share the similar mechanisms. 22 Hence combination therapy proves beneficial. 12
Other treatments
Olanzapine: These are basically antipsychotic medications with an antiemetic characteristic property. They can be used in combination with 5-HT3RA in a dose of 10 mg daily for 3 days. As they have adverse effects of sedation hence must be cautiously used in elderly patients. 14 The combination of olanzapine with palonosetron, dexamethasone and aprepitant in a randomised double blinded placebo control study of patients undergoing high levels of emetogenic chemotherapy and not previously undergone chemotherapy has shown positive results in early and long term benefits in emesis. They have the potential to target multireceptors to prevent emesis with no serious adverse effects that caused anticipation for the patients25,26 hence proves to be a better antiemetic option.
Complementary therapies
The use of adjuvant non pharmacological methods like acupuncture and acupressure are used as complementary in case of RINV but the nauseous feelings are diminished to a smaller extend only. The Zingiber officinale ginger components are found effective as they exhibit the properties of 5-HT3RA and NK-1RA. There are studies demonstrating the usefulness of ginger capsules with reduced patient oriented side effects in CINV. 14 Herbs like peppermint called MENTHE X PIPERITA LAMIACEAE are calcium channel blockers that cause intestinal smooth muscle relaxation spasmolytic agents and for PONV. 17
The use of cannabinoids is exploited for antiemetic purposes. Cannabinoids (CB) has synthetic class of nabilone and levonantradol. They consist of CB1 receptors present on peripheral neurons, brain and spinal cord and CB2 receptors present on peripheral tissues. Mostly the CB1 receptors agonists are useful to prevent the emesis stimuli whereas CB2 receptors utility is under investigations. Studies also show that the cannabinoid receptor antagonist reduces the frequency of antiemetic agents. There can be a dose independent lethargic side effects of cannabinoid agonists hence prior concerns must be taken to avoid works that require concentration. 27
Antihistamines like diphenhydramine and hydroxyzine are given for palliative care and as adjuvants for dystonic reaction and antiemetics. Benzodiazepines like lorazepam have the properties of anti-anxiety, decrease anticipatory nausea and antiemetic. There are midazolams that are used for post operative nausea and refractory emesis.17,28
Emetogenic risk classification
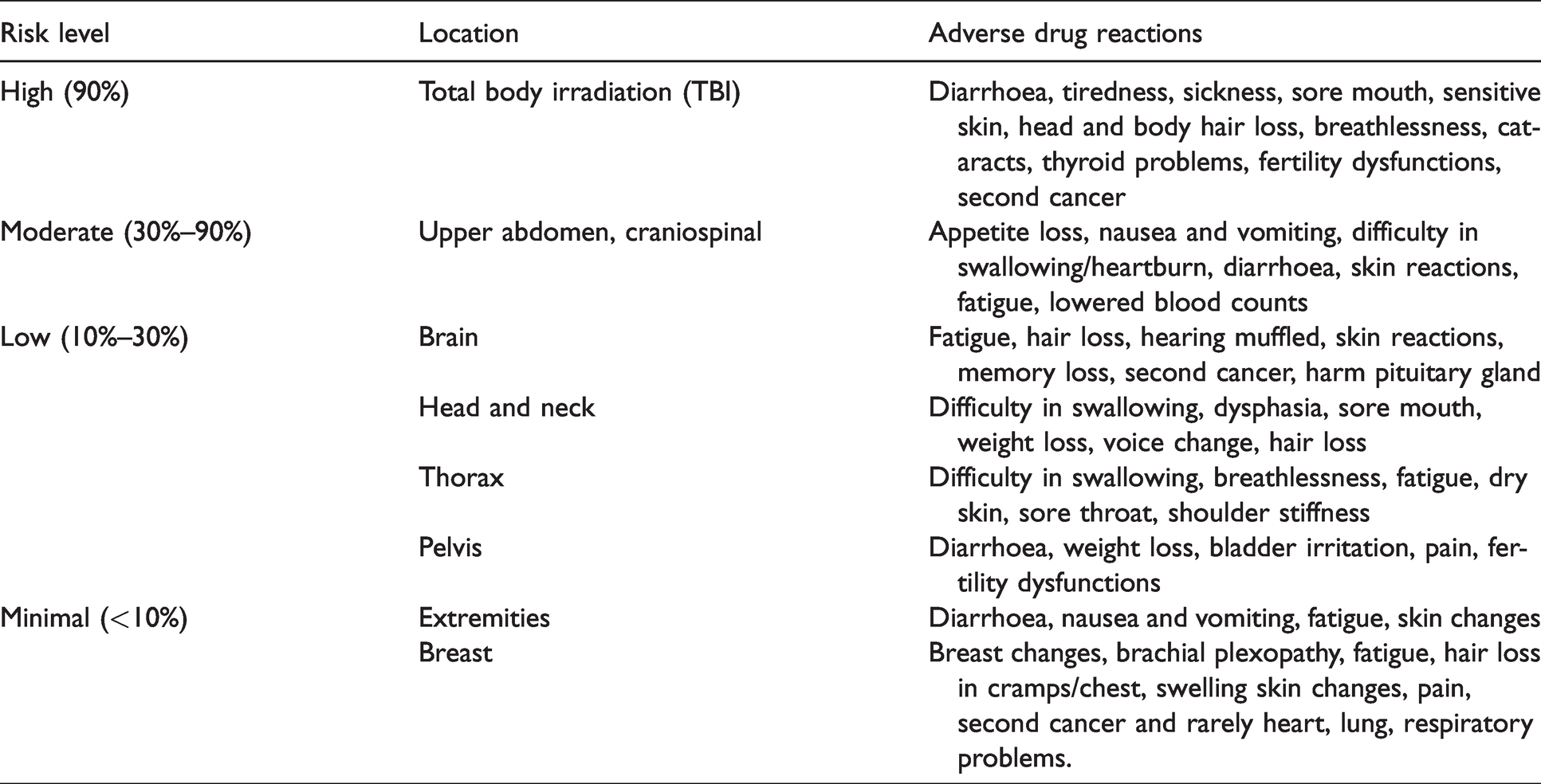
The emetic risk is categorised into high, moderate, low and minimal according to the site of radiation. Identifying the extent to which radiation process enter and exert their effect in individual patients helps to identify the risk. Individual patient mental status, anxiety levels, can also effect the severity of risk experienced during RT. Usually antiemetic are effective in the first week but prolonging effects of fractionated radiotherapy can be controlled if continued accordingly. 21 The major high level risk of nausea and vomiting are found in case of total body irradiations therefore it requires a greater patient care surveillance.13,23 Hence risk categorisation helps in individualisation of therapy as most of the radiations target total body or upper body that has high or moderate risk (Table 3). 13
Levels of emetogenic risk for radiotherapy. 13
RINV: Major adverse effects of antiemetic medications
Radiation therapy is a curative modality for cancer treatment hence it is important to identify the toxicities of radiation therapy and resolve them. 6 An estimate of three out of five has cancer and hence RT induced late serious side effects must be considered important as they might even develop to secondary malignant stages that are lethal. 29 Antiemetic can change the eating patterns hence small meals, with less spicy and eat before feeling hungry as they can trigger nausea. Vomiting and diarrhoea can also cause electrolyte imbalance and hence result in malnutrition. 30 The patients can be taken care with proper dietary requirements using liquid feeds for at least 3 months to avoid malnutrition. A well balanced diet improves the quality of life. Dietary individualization, patient counselling, education and management help to provide maximum results.
The experience of each patient with RT is different hence there must be an individual side effect evaluation in each patient. There can be side effects due to polypharmacy and drug–drug interactions. Elderly people are mostly having concomitant disease therefore there can be chances of antiemetic interacting with other medications. The renal and hepatic impairment in some may again decrease the efficacy of treatment. The RT usually causes diarrhoea which is balanced by the constipative symptoms of 5HT3RA that reduces the bowel dysfunctions. All the 5HT3RA are metabolised to a great extend by CYP 450 enzymes. This means induction or inhibition of the enzymes lead to the efficacy of drug administered. Ultra metabolizers metabolize drug rapidly hence the efficacy of drug is lost (Table 4). 31

Technological advancements in radiation therapy
The exact position of the tumour is identified with the help of CT and MRI imaging. This provides a greater level of exposure to the radiations for the practioners. One of the treatment technique involves three dimensional conformational radiotherapy (3D-CRT) that includes the radiations passed to most sensitive parts of the body including spine, lungs, bladder, prostate with a 3D imaging of the organ taken and treatment planning is done on beam arrangements and dose calculations to get specific results. 7 Intensity modified radiation therapy (IMRT) are useful in targeting the critically complex shaped organs at risk(OAR) structure of the body. They use a technique called inverse planning system that uses dose adjustment algorithms that initially radiate the dose as per the prescriptions and then modify the beam to achieve size and shape that is closest to the tumour to protect the normal cells. They can be followed by tapering the dose concomitantly and preserve the QOL.33,34 Image guided radiation therapy (IGRT) are advanced form of 3D-CRT techniques. They have certain advantages over the other methods that helps to decrease the dose uncertainties in volume, cause decreased side effects like xerostomia and reduced acute and delayed problems. They are more target specific as multiple images are constructed from advanced 3D and CT views. 32 Therefore IGRT helps in identifying the borders for RT and scan the surface for radiation therapy prior for knowing the size, spread of cancer. 10 Stereotactic radiation therapy mainly renders radiations in fractionated forms and have proven efficacy in lung cancer, HCC, spinal and prostate cancers. 35 Stereotactic radiosurgery (gamma knife) helps to concentrate multiple beams to focus on a small tumour with precision. The latest advancements of robotic surgery/cyber knife also help to deliver medications painlessly by a computer controlled robot technology. 7 There are latest advances including Adaptive radiation therapy (ART) which include treatment strategies modified according to the changes in the anatomy of the patient. They check the previous tumour treatment responses; identify hypoxic and respiratory problems, volume of tumour shrinkages and areas of radiation resistance. 33 These technological advancements in radiation therapy helps for more precise radiotherapy targeting that leads to reduction in radiation induced side effects. However as the clock ticks there is a need to bring advancements in every field that are affordable and equally accessible to all. 7
Significance of radio sensitizers and radioprotectives in radiation therapy
RT modalities have a relation between the radiation therapy and the immune system. The anticancer treatment modalities usually trigger the immune system and promote immunosuppression hence dose and delivery of radiation therapy must be fractionated. 36 As tumour cells also consist of immune cells antitumor- immune responses are seen in local tumour radiations. RT causes inflammatory reactions as immune system is affected and long lasting of this scenario causes cognitive dysfunctions. 37 Radiation therapy causes production of free radicals that cause oxygen stress in cells leading to cell death. The antioxidants present in the endogenous system helps to reduce the radiation damage to cells. Hypoxia causes a cell to be radiation resistant hence substances called radiosensitizers are necessary to improve the sensitivity to radiations. 38 Radiosensitizers sensitize the tumour cells and produce less harm to the normal cells. Substances like carbogen, mitomycin-c, nicotinamide, metronidazole, hyperbaric oxygen, irinotecan are radio sensitizers. These are of great concern as there should be protection criteria for normal cells rather than dose reduction as that can reduce the therapeutic efficacy. 10 The advanced method of targeted radiotherapy involves the use of metal nanoparticles to target the cancer cells by photoelectric effect. The controlled release pattern, high loading capacity, enhanced permeability and retention (EPR) effects of nanoparticles (NPs) contributes to the better drug targeting. The vitro studies performed by MTT assay on MGC-803 gastric cancer cells and human gastric mucosal epithelial GES-1 cells using chitosan modified gold nanoparticles (CS-GNPs) as radio sensitizers confirmed a nonlinear relationship between the radiation dose enhancement and CS-GNPs concentration. Similarly the use of bovine serum albumin (BSA) capped silver microspheres composed of silver (Ag) nanoparticles as radio sensitizers in MTT assay against gastric cancer cell radiotherapy provided enhanced biocompatibility and reduced cytotoxicity. 39 The radiotherapeutic effects demonstrated by the palladium nanosheets under X-ray irradiation on MCF-7 cells enhanced the formation of reactive oxygen species (ROS) along with DNA double stranded breaks that facilitated targeted therapy leaving normal cells unaffected. 40 The in vitro experimental studies of PSMA-expressing prostate cancer cells treated with Au-Gd(III) PSMA NPs as radio sensitizers enhanced the tumour cell killing and sensitisation enhancement ratios with reduced off-targeting. 41 The use of melatonin in various cancers with radiotherapy increases the cytotoxic effect of radiations and reduce the DNA repair capacity of tumour cells. 42 Mostly tumour cells with hypoxia, low oxygen and nutritional states are resistant to radiotherapy hence radio sensitizers provide an additive effects and prevent the radiation resistance of tumour cells. 43 This field of nanotechnology used as radio sensitizers enhances the selective sensitivity of tumour cells and sets the normal cells free of damage. 44 Therefore the ultimate success of radiotherapy is the localisation of radiation dose within the tumour cells and decrease tissue injury to normal cells.45,46
Similarly radio protective agents are used for protection against the lethality’s of radiotherapy. There are many agents useful in this scenario including sulphur containing compounds like cysteine, amifostine (WR2721), 47 cell growth factors, granulocyte colony stimulating factors, granulocyte colony macrophage stimulating factor, antioxidants, enzymes, nitroxides, growth factors, vitamins, immunomodulators, xanthine and adenosine derivatives. They repair the DNA damage, normal tissue damage and protect the normal cells. 48 An increased production of keratinocyte growth factor (KGF) is an indicative of epithelial damages via radiation therapy that needs repair. Superoxide dismutase reduces the oxidative stress and normal cell injury. They are antioxidants and scavenge the free radicals hence protects the DNA. 49 Therefore radio protectors and radiosensitizers are gaining attention and may pave greater therapeutic benefits in the future.
Patient care approach for radiation induced nausea and vomiting: In general50–54
Patients experience a whole plethora of queries in their minds regarding their diagnosis, treatment, follow-ups, survival, changes in life that may affect their quality of life hence there is a major need in making the patients understand the pros and cons of radiation therapy. The patient educator provides individual support, encouragement and confidence to cope up with the treatment strategy. Thereby patient counselling put forward precautions to reduce the degree of adverse effects regarding RT.In case of nausea
Eat small snacks throughout the day instead of large meals. Do not skip meals as they might worsen the nausea. Take an anti-nausea medicine before treatment in case of first signs of nausea to prevent vomiting. Eat and drink sufficiently to avoid dehydration. Take small sips slowly throughout the day but do not administer anything just before the treatment. Avoid or remove foods with strong or unpleasant smells. There must be measures undertaken to guide the pain levels and skin rashes that are minor in RINV. A patient diary maintained for emesis is essential for improved assessments of vomiting frequencies. While treating elderly with RINV consider factors like co morbidities and cognitive behavioural management.
Hence it is worth to note down the adverse issues in RT receiving patients as it would greatly improve their healthcare outcomes and quality of life.
Conclusion
As the endpoint or a permanent cure was not reached each time new antiemetic is tried. Evidence lacks whether to continue antiemetic beyond first week. In future consider the prognosis of patient factors, genes coding the receptors, pharmacogenomics and control delayed RINV for betterment of treatment strategy. There must be a balance between the safety and toxicity profile of a drug regimen. Future-PET scan and markers can identify the capacity of receptors and how long they can carry the drug. There is a need for future observational prospective data for future determination of nauseous sensation tackling. There is a lack in data for benzodiazepines, antihistamines and anticholinergics that can be used for RINV to smaller extend. There is a need for guideline updating as only 50% follow guidelines that make the scenario less resolved. Hence there is a need for larger randomised controlled antiemetic trials. The use of olanzapine targets multireceptors that are responsible for emesis with no serious side effects. Further researches in this area may pave the way for discovery of a better antiemetic. As there are constant advancements in finding drugs to cancer newer antiemetic with decreased side effects will also evolve in next 10 years. The promising use of radiosensitizers in radiotherapy need to be exploited for better therapeutic outcomes. Antiemetic is a cornerstone hence critical assessment of the usage of newer antiemetic for RINV with proper reproducible data based on properly designed randomised controlled trial is essential. RT induces slow growth of tumour cells and eases the cancer symptoms. RINV has become a case of anxiety and distress in patients. Individualisation of therapy with proper full assessment of condition is required to determine the medical condition. Nausea being an unpleasant feeling and a prodromal phase of vomiting needs to be differently identified and treated to provide the best patient outcomes. If RINV are not managed properly they may cause the RT to be inefficient and a period of extension in treatment days is visible.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.