
Abstract
Background
Pembrolizumab is a humanized monoclonal antibody that is used to treat a variety of cancers. It exerts its mechanism of action by blocking the programmed death receptor-1 (PD-1). Toxicity concerns include immune-related toxicities, including colitis, hepatitis, pneumonitis, nephritis, endocrine toxicities and more rarely, myocarditis and other organ system toxicities.
Objective
To review a real-world case involving immunotherapy induced myocarditis after a patient received pembrolizumab and discuss how the current pandemic created complexity in toxicity management.
Discussion
An 83 year old male with metastatic lung cancer developed fatal myocarditis after receiving 2 doses of pembrolizumab. Applying the Naranjo score, the likelihood of pembrolizumab causing the myocarditis is probable, with a score of 6. Severe cardiac toxicities are rare with pembrolizumab, but can still occur. It is vital to be aware of these toxicities, and educate patients on signs and symptoms. Complicating the situation even further was the global pandemic, which created fear and hesitation in the patient and the patient’s family to seek medical treatment out of fear of exposure. This pandemic adds another layer to the complexity of care for patients with cancer and management of toxicities. Pharmacists play a significant role in ensuring the safety and efficacy of medications, especially oncology agents.
Conclusion
Proper education of patients regarding symptoms and when to report are paramount to assisting in early detection and intervention for immunotherapy-related adverse events. New management and treatment strategies will need to be discussed and implemented considering the changing landscape around the SARS-CoV-2 pandemic.
Introduction: Pembrolizumab and immune-related toxicities
Pembrolizumab is an immune checkpoint inhibitor with a rapidly growing list of FDA-approved indications. This monoclonal antibody is directed against programmed cell death protein 1 (PD-1) and the binding of pembrolizumab to the PD-1 receptor prevents programmed cell death ligand 1 and 2 (PD-L1 and PD-L2) from interacting with PD-1. 1 PD-L1 is located on and often expressed by tumor cells. The interaction between PD-1 on immune cells and PD-L1 on cancer cells, results in an inhibition of our immune system and prevents T-cell function against cancer cells. This shift in balance allows for the environment to favor cancer cell growth. By blocking this interaction, pembrolizumab helps to restore the immune response as tumor cells are no longer able to inactivate T cells through this pathway. 1 , 2 With the approval of pembrolizumab in 2014, and now various other immune-checkpoint inhibitors, the treatment landscape for cancer has shifted and survival outcome improvements have been seen in many disease states, including lung cancer. 2 While pembrolizumab’s mechanism of action has shown to be highly effective, it brings with it risks of immune-related adverse events (irAEs). While most of these events are not severe or life threatening, there is still risk present for any patient taking pembrolizumab as the specific risks for patient susceptibility to irAEs is not well understood. To date, there are 3 Anti-PD-1 agents FDA approved for cancer indications, cemiplimab, nivolumab, and pembrolizumab. There are also 3 Anti-PD-L1 agents currently FDA approved: atezoliuzmab, avelumab, and durvalumab. Common irAEs associated with immune checkpoint inhibitors, such as pembrolizumab, include diarrhea/colitis, hepatotoxicity, hypo- and hyperthyroidism, and fatigue 1 Other less common irAEs include pneumonitis, myocarditis, and ocular neuritis and other toxicities. These irAEs have been reported to occur as early as after one dose of immunotherapy and as late as up to a year or more after therapy is completed. There has been an increasing number of cases that have been reported on immune checkpoint inhibitors (ICI) causing myocarditis. Here we report the findings of a patient who developed fatal myocarditis after receiving two doses of pembrolizumab.
Case overview and course of treatment
Informed consent was obtained from the patient’s family for use of this case in the literature
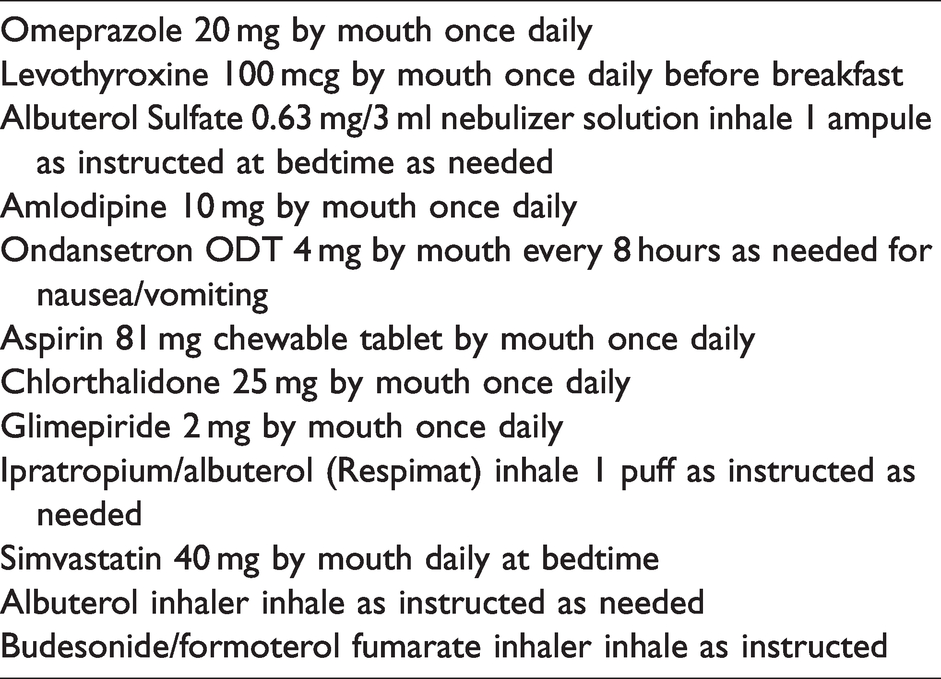
An 83 year old Caucasian male with extensive oncologic history reports to clinic in January 2020 for treatment of non-small cell lung cancer with pembrolizumab. Past medical history is significant for COPD, diabetes, hypertension, hypothyroidism, and history of prostate cancer (1990), and colorectal cancer (2018). Past surgical history is significant for partial nephrectomy, gallbladder removal, and laparoscopic hemicolectomy. Family history is significant for multiple cancer diagnoses including his father and his sister (types and age of onset are unknown). He is a former smoker and quit in 2009. His home medications include: Amlodipine 10 mg by mouth once daily, levothyroxine 100 mcg by mouth once daily before breakfast, simvastatin 40 mg by mouth daily at bedtime, glimepiride 2 mg by mouth once daily, chlorthalidone 25 mg by mouth once daily, aspirin 81 mg by mouth once daily, ondansetron 4 mg by mouth once every 8 hours as needed for nausea and vomiting, ipratropium and albuterol respimat 100 mcg puff as instructed as needed, omeprazole 20 mg by mouth at bedtime as needed, albuterol inhalation as instructed at bedtime as needed, and budesonide/formoterol inhalation as instructed (Table 1). Patient did not have any other use of complementary or alternative medications including herbal supplements that could have impacted metabolism of these agents. Upon review it was determined that there were no drug interactions between the patient’s prescription medications and pembrolizumab.
Patient’s home medication list.
Patient’s oncologic history includes multiple primary cancer diagnoses. He was diagnosed with early stage prostate cancer in the early 1990s and received radiation therapy as the only treatment intervention at that time. In 2012, the patient was diagnosed with early stage renal cell carcinoma and underwent partial left nephrectomy. In August 2018, the patient underwent a digital rectal exam by his urologist which revealed a low rectal tumor. This was followed by a colonoscopy in September 2018 which showed an ulcerated distal rectal mass. Biopsy results revealed invasive adenocarcinoma. The patient was offered surgical intervention with abdominal perineal resection, but the patient declined. The patient was diagnosed with Stage II rectal cancer and began treatment in October 2018 with 6 cycles of neoadjuvant FOLFOX. Patient received all cycles of treatment without issue. MRI at the end of January 2019 revealed significant decrease in size of the original rectal lesion. Again, patient refused to receive abdominal perineal resection and instead underwent transanal excision of rectal tumor in March 2019.
At this time the patient was discharged to surveillance and went for repeat CT scan in September 2019 which showed a new lobular mass consolidation in the right upper lung lobe. No abnormality in the rectum was noted. A follow-up colonoscopy was performed December 2019 which was negative for malignancy. Patient underwent right lobe biopsy of the lung mass on January 2020. Pathology was consistent with adenocarcinoma of lung origin. Repeat CT scan of chest in January 2020 revealed 2 large contiguous speculated masses in the right lung. Other scattered bilateral pulmonary nodules are found and suspicious for metastatic disease. At this time the patient was diagnosed with primary non-small cell lung cancer (as opposed to metastatic rectal cancer to the lung). MRI of the brain in January 2020 reveals no evidence of metastatic disease and no acute intracranial findings. A PET CT scan was ordered and performed at the end of January 2020 which showed no evidence of distant metastatic disease. Right upper and right middle lobe masses are compatible with primary lung malignant neoplasm. Full molecular profile of tumor performed, revealing PD-L1 positivity at 70% via immunohistochemistry. Patient was referred to medical oncology and began treatment with cycle 1 of pembrolizumab 200 mg IV every 3 weeks repeated every 21 days in February 2020. Baseline labs were all WNL with the exception serum creatinine and renal function as expected with patient’s history of renal insufficiency and past surgery (Table 2). Patient tolerated cycle 1 well with no complaints or adverse events reported. Patient received cycle 2 of pembrolizumab in early March 2020 and again tolerated therapy well with no issues reported.
Baseline labs from February 2020.
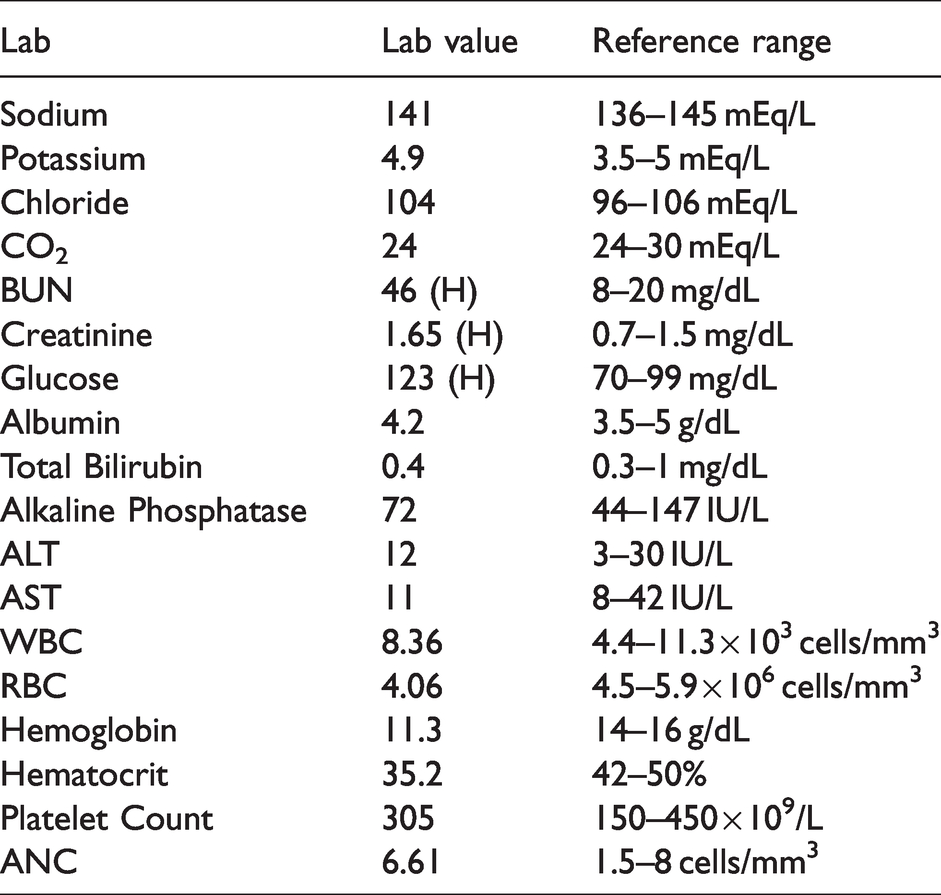
Cycle 3 of pembrolizumab was set to be received on March 30th 2020, but lab results prior to cycle 3 on March 27, 2020 reveal elevation in liver enzymes with ALT now at 107 U/L and AST now at 167 U/L (more than 3 times elevated from baseline original values of 12 U/L and 11 U/L respectively (Table 2). At this time it was determined to withhold cycle 3 treatment of pembrolizumab and delay for 1 week. Of note, patient complains at this time of more shortness of breath, but patient was saturating O2 at 97% in clinic and with underlying COPD patient was referred to see pulmonologist. Two days later on April 1st 2020, the patient was at home and reported “really bad shortness of breath”, 911 was called and was instructed to get oxygen at home. Patient reports heavy chest as well as pain in back of neck and back. Patient oxygen saturation at home was reported at 94% on room air. An EKG was done at his house and was not concerning for an acute coronary syndrome. EMS team recommended against transport to the ER due to the SARS-CoV-2 pandemic. CT of chest was ordered (without contrast due to underlying CKD) and patient was started on empiric prednisone 40 mg by mouth×3 days, followed by 20 mg by mouth for 3 days, and then 10 mg by mouth for 3 days as well as levofloxacin 500 mg daily by mouth×7 days.
The following day on April 2nd, 2020, the patient was able to have a virtual office visit with the pulmonologist for follow-up on suspected COPD exacerbation. Patient reports that his breathing had worsened over the last 5 days but states that the previous night it was “slightly better”. Pulmonologist felt that patient was stable and experiencing a COPD exacerbation. Risk of pulmonary embolism was present, but patient denied leg edema, so this was not suspected. Recommendations from pulmonologist included: continuing prednisone taper and levofloxacin, increasing use of ipratropium/albuterol and budesonide/formoterol, resting, and seeking medical attention at ER if symptoms worsen. The patient did not improve overnight and returned to clinic on April 3, 2020. He was seen by medical oncology and was notably much shorter of breath with dyspnea with conversation and no longer being able to walk more than a few feet without significant shortness of breath resulting in the need to use a wheelchair. On exam, lungs showed markedly diminished breath sounds diffusely with no adventitious sounds. Heart rate was 120 beats/min and regular. Extremities had no edema or evidence of DVT. Patient had already been instructed to go to the ER earlier that day, but patient declined. Oncology team reviewed with patient concerns of worsening symptoms if not addressed immediately. At this time patient was taken to the hospital and was admitted with primary complaints of shortness of breath. During his stay, the patient was diagnosed with complete heart block and a pacemaker was placed on April 6, 2020. On April 8th, patient had elevated troponins and endomyocardial biopsy was consistent with drug-induced myocarditis from the immunotherapy pembrolizumab (Table 3). During hospital admission, patient was on BiPAP and was unable to wean off. He was also intubated for respiratory fatigue. At that time, patient expressed his wish to be extubated to nasal cannula. He did not want any more procedures or treatment and made the decision for hospice care. The patient was discharged to hospice care on April 10, 2020 and ultimately died the following day.
Cardiac labs.
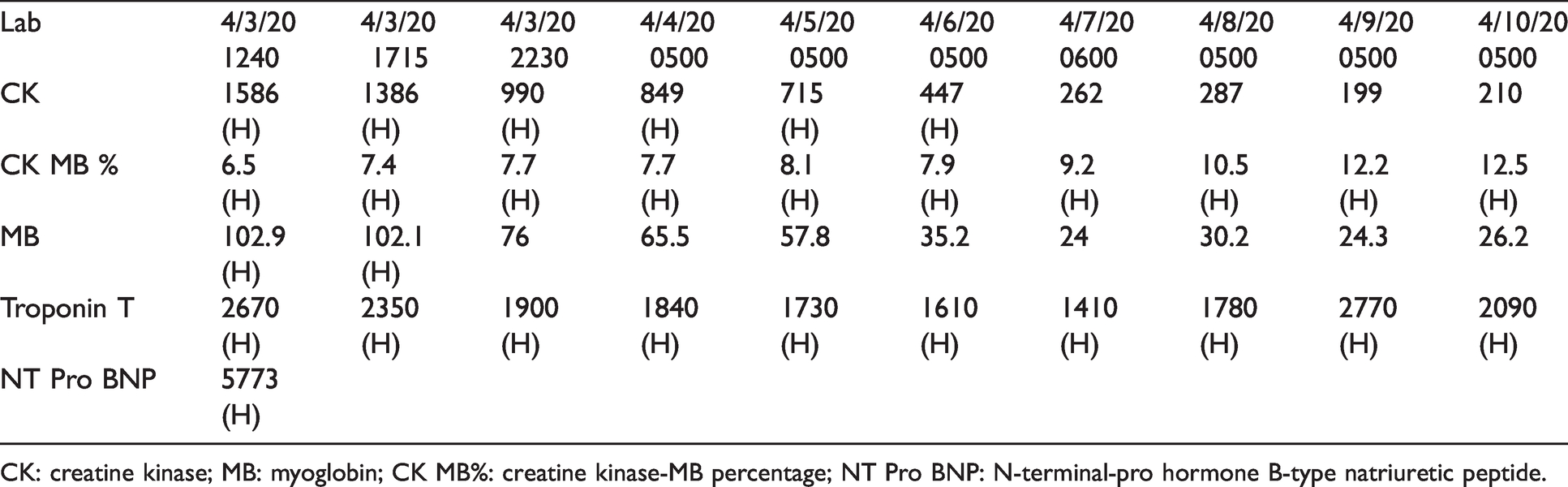
CK: creatine kinase; MB: myoglobin; CK MB%: creatine kinase-MB percentage; NT Pro BNP: N-terminal-pro hormone B-type natriuretic peptide.
Discussion
Myocarditis is defined as the inflammation of the myocardium which can lead to necrosis of the cardiac myocytes. 3 The most common cause of myocarditis is viral infections such as Coxsackie B virus, adenovirus, hepatitis C, cytomegalovirus, echovirus, influenza virus, Epstein-Barr virus, and the parvovirus B19. However, myocarditis can also be immune-mediated be T-cell activation. Immunotherapy-related myocarditis from pembrolizumab is rare, at <1% reported, but other cardiac toxicities such as arrhythmias have a higher incidence, around 11∼. 1 A study that was conducted on mice showed that PD-1 protects against inflammation and myocyte damage by limiting T-cell responses in the heart. 4 By administering pembrolizumab and blocking PD-1, there is potential for decreased protection against inflammation and myocyte damage. This can lead to increased risk for immune-related myocarditis, as seen in our patient. Immunotherapy-related adverse event incidence varies widely, ranging from 15–90%. 5 This is mostly due to inconsistencies in reporting leading many to believe that the incidence is often underestimated. A major focus of the last several years has involved the development of practice guidelines for the management of these immunotherapy-related adverse events (American Society of Clinical Oncology, European Society of Medical Oncology, National Comprehensive Cancer Network).5–7 The key to management for these toxicities involves early recognition and intervention with high-dose corticosteroids being utilized as the mainstay treatment for immunosuppression. Studies have shown that short-term treatment with immunosuppressive therapy, such as corticosteroids, does not impact efficacy or survival outcomes for patients receiving immune-checkpoint inhibitors. 5
The symptoms for myocarditis are often non-specific, with patients presenting with complaints of fatigue, shortness-of-breathe, or chest tightness. Immunotherapy-related myocarditis is more common with combination immunotherapy, such as nivolumab and ipilimumab. 5 In patients suspected of cardiotoxicity, an immediate work-up and cardiology consult is recommended along with laboratory monitoring and imaging. Cardiac biomarkers, electrocardiogram, and inflammatory biomarkers such as erythrocyte sedimentation rate, white blood cell count, and C-reactive protein should all be drawn and patients should undergo telemetry monitoring and a cardiac MRI (Magnetic Resonance Imaging), while also ruling out other potential causes (viral titers, pulmonary-work up if cardiac work-up negative). 5 Management of immunotherapy-related myocarditis follows the other immune-related toxicities in that for severe or life-threating myocarditis patients should be initiated on high doses corticosteroids and treated until cardiac function returns to baseline, followed by steroid taper over 4-6 weeks. Severe myocarditis can be classified by presence of arrhythmia, cardiac makers above the upper limit of normal, or cardiac findings on imaging. 5
Multiple reports regarding pembrolizumab-induced cardiotoxicity have been reported.8–11 Fuentes-Antras and colleagues reported on a fatal event of autoimmune storm that occurred after 1 dose of pembrolizumab in a patient with metastatic lung cancer. 8 This patient received pembrolizumab and prior to cycle 2 developed myocarditis, pneumonitis, hepatitis, thyroiditis, and myasthenia gravis. The patient initially received oral beta-blocker therapy for their symptoms, but then later was initiated on high-dose dexamethasone once immunotherapy-related toxicity was suspected. Another article discusses a patient with metastatic non-small cell lung cancer who developed second-degree atrioventricular block three weeks after receiving cycle 1 of pembrolizumab and required permanent pacemaker placement. 9 Imai and colleagues also report a case of myocarditis after a patient received 2 doses of pembrolizumab for metastatic lung cancer. 10 The patient improved after treatment with glucocorticoids and tacrolimus. Finally, another myocarditis case report by Martinez-Calle and colleagues evaluated possible underlying causes for the immune-related adverse events. 11 In this case, a patient with multiple myeloma undergoing clinical trial investigating pembrolizumab in combination with standard treatment for first-line multiple myeloma, developed myocarditis after a single dose of pembrolizumab. The patient died after maximal support and care including high dose corticosteroids and infliximab. The authors suggested some degree of underlying autoimmunity due to the early and severe onset of immunotherapy-related myocarditis, such as the patient's previous exposure to chest radiation for breast cancer treatment, a silent cardiomyopathy, or an undiagnosed previous episode of myocarditis. Based on our patient’s past medical history, underlying autoimmunity is unlikely, but remains an unknown possibility, as patient did receive radiation therapy for prostate cancer in 2018, for underlying cause of the pembrolizumab induced myocarditis after 2 doses of therapy.
Applying the Narajano adverse drug probability scale to this case, a score of 6 was obtained indicating probable likelihood the pembrolizumab is the cause of the myocarditis in this patient (Supplemental material). 12 Despite direct and timely intervention, the patient still ultimately succumbed to the cardiotoxicity and passed away. Complicating the situation even further was the global pandemic, which created fear and hesitation in the patient and the patient’s family to seek medical treatment out of fear of possible exposure. This pandemic adds another layer to the complexity of care for patients with cancer and management of toxicities. The likelihood of the outcome of this case changing if the pandemic had not been taking place is minimal but cannot be ruled out if potential earlier interventions were implemented. Also of note is the patient’s past medical history of chronic pulmonary disease and how that also played into the differential and may have led to some delays in seeking inpatient treatment. Pharmacists play a significant role in ensuring the safety and efficacy of medications. It is important for pharmacists to educate patients of the signs to be aware of to identify a serious immune-related toxicity. Counseling points that should be shared with the patient include signs and symptoms of myocarditis such as chest pain, rapid or abnormal heartbeat, shortness of breath, difficulty breathing, fluid retention, fatigue, and fever. 1 , 5 Although these symptoms may present as mild, it is important for patients to communicate with their physician or pharmacist as soon as possible so that early detection of serious adverse effects can be identified and treated appropriately. New management and treatment strategies will need to be discussed and implemented considering the changing landscape around the SARS-CoV-2 pandemic, including proper education of patients, triage support, and increased and expanded pharmacy services in the ambulatory and acute settings.
Conclusion
In conclusion, our patient suffered fatal immune-related myocarditis after receiving only 2 doses of pembrolizumab. Although rare, it is important to recognize that myocarditis, and other severe, life-threating immune-related adverse effects can occur early on in therapy or later after therapy discontinuation. Timeline of toxicity onset is variable and currently inconclusive. Pharmacists play a crucial role in monitoring patients and managing immune-related toxicities. Proper education of patients regarding symptoms and when to report are paramount to assisting the health care team in early detection and intervention for immunotherapy-related adverse events. More studies are needed to review possible timelines of various immune-related toxicities and underlying mechanisms and risk factors.
Supplemental Material
sj-pdf-1-opp-10.1177_10781552211012782 - Supplemental material for Immune-checkpoint inhibitor toxicity during a pandemic: Overcoming patient fears to provide care. A case report
Supplemental material, sj-pdf-1-opp-10.1177_10781552211012782 for Immune-checkpoint inhibitor toxicity during a pandemic: Overcoming patient fears to provide care. A case report by Christopher T Elder, Elizabeth C Davis, Stephanie Jaipal and Charles E Wight in Journal of Oncology Pharmacy Practice
Footnotes
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.