
Abstract
Keywords
Introduction
Oral therapies are increasingly used in the primary treatment of cancer. In 2018 alone, nearly 90 oral anticancer medications were approved by the U.S. Federal Drug Administration.1–3 Given ongoing approvals for new medications and new indications among previously approved medications, this upward trend is expected to continue.4,5 Although treatment self-administration affords new conveniences for oncology patients, adherence to oral anticancer therapy is complex and presents additional challenges for patients, caregivers, and clinicians.6,7
Surprisingly little is known about how the oncology field, which has long been dominated by infused therapies, should best pivot to support patients prescribed oral anticancer therapy. 8 At first glance, shortfalls are apparent in current practice. Studies have documented high variability in patients’ adherence to oral anticancer therapy, with some estimating adherence as low as 46%. 9 This is particularly alarming as anticancer therapy non-adherence has been linked to disease progression, lower quality of life, and premature death.10,11 While the reasons for medication non-adherence are multidimensional12,13 the importance and centrality of patient-provider communication to supporting adherence has been demonstrated repeatedly.14–16 As such, the shift to oral anti-cancer therapy is thought to require that oncology clinicians explain how medications are to be taken, routinely assess patients’ medication adherence, identify barriers to adherence, provide self-management support, and foster patient engagement and problem solving. 17
Although studies have addressed how oncology clinicians communicate with and support medication adherence among patients with cancer, to our knowledge the literature has not been summarized for emerging evidence. Yet, those delivering care need to understand how best to assess and support patients’ adherence to oral anti-cancer therapy. Likewise, those conducting related research need to understand gaps in existing evidence to better formulate studies that can effectively contribute to supporting oncology patients in adherence to prescribed oral anticancer therapy. To this end, we conducted a systematic review to (1) determine the approaches to patient-provider communication, education, and counselling that have been tested to improve oral anticancer therapy adherence, (2) identify the behavioural, communication, implementation science or other frameworks, models or theories that have been used to guide the development of these approaches, (3) describe how therapy adherence has been evaluated as an outcome in the context of oral anticancer therapy communication-, education-, and counselling-based interventions, and (4) summarize evidence regarding the effectiveness of such interventions to support patient adherence to oral anticancer therapy.
Methods
This systematic review was designed and reported in accordance with the Preferred Reporting Items for Systematic Reviews and Meta-Analysis (PRISMA) guidelines. 18 We included both quasi-experimental and experimental studies that quantitatively assessed the relationship between a structured measure of an interpersonal communication-, education-, or counselling-based intervention and adherence to oral anticancer therapy among patients diagnosed with a malignancy. We included full-text, English language studies that focused on a patient-clinician communication-, education- or counselling-based intervention, in comparison to an alternative. Comparators included usual care, a different intervention strategy, or historical controls. Studies that did not use a structured measure of medication adherence or focused solely on the use of extended adjuvant therapy (i.e. tamoxifen among breast cancer patients) and not the primary treatment of cancer were excluded. We also excluded studies that evaluated the use of a technology-based or other type of prompt or reminder in absence of a counselling or educational component. The study protocol was published on the PROSPERO register of systematic reviews. 19 The institutional research board (IRB) at our organization determined the study to be exempt.
Search methods for study identification
We electronically searched Medline/Pubmed, EMBASE, PsycINFO, and CINAHL for full-text, original research articles that were published in English prior to March 13, 2020. Key search terms included MeSH terms aligned with cancer, oral anticancer therapy (including the names of specific medications), medication adherence, and interpersonal communication-, education- and counselling (see online Appendix). We manually scanned reference lists of relevant reviews, systematic reviews, and meta-analyses to identify additional relevant citations.
Study selection and review
Two members of the research team independently screened the titles and abstracts of all identified articles for study eligibility using Covidence. 20 Any article identified by either team member as potentially eligible was retained for full text review. Articles that were retained for full text review were similarly independently reviewed by two members of the research team to determine appropriateness for study inclusion. When needed, a third member of the research team was used to resolve conflicting opinions.
Data extraction
For each included article, two authors independently extracted study information into a structured charting form. Discrepancies in extracted information were discussed during team meetings and, if needed, a third author served as a tiebreaker. Characteristics extracted included: 1) study design, 2) study population characteristics (including sample size, age, and cancer diagnosis); 3) adherence measure(s) and data source(s); 4) clinician(s) delivering the intervention (e.g. physicians, nurses, pharmacists, or a combination of these) and 5) communication mode (e.g. face-to-face, telephone, and/or text). We also identified core components of the interventions. The list of intervention components extracted was based on recommendations provided in the American Society of Clinical Oncology and Oncology Nursing Society. 17 In addition to these recommendations, we also used published intervention descriptions to identify other key programme components as identified by authors. This process resulted in us extracting eight programme components, including the provision of (1) general educational material (printed and/or electronic), (2) storage and handling information, (3) concomitant medication counselling and management, (4) information regarding possible drug/drug or drug/food interactions, (5) planning regarding missed doses, (6) counselling and management of adverse events, (7) financial assistance (including insurance authorization and drug copay assistance), and (8) referrals to other supportive programming. Finally, we extracted information on the conceptual framework or theoretical model used for study and/or intervention design if one was reported.
Risk of bias assessment
Two authors independently assessed risk of study bias for each included article. For experimental studies, we used the Cochrane RoB 2 tool approach to assess the risk of bias. 21 Bias grades consisted of low risk, some concerns, and high risk. For quasi-experimental studies, we used the Cochrane ROBINS-I tool to assess risk of bias. 22 For the latter, risk of bias is considered as low, moderate, serious, and critical. Disagreements were discussed with a third investigator until consensus was reached.
Results
Study characteristics
We identified a total of 5887 papers that met the criteria for title and abstract screening. Among those,127 were selected for full text review, with 24 meeting the study inclusion criteria (Figure 1). Among the 24 included studies, 13 were based in North America (all in the United States),6,23–34 6 in Europe,35–40 4 in Asia,41–44 and one in Africa 45 (Table 1). Among the 22 studies that reported the type of malignancies studied, nine included patients with solid tumours only,24,26,36,37,39,40,43–45 five included patients with hematological malignancies only (all chronic myeloid leukemia [CML]),27,32,35,41,42 and eight included patients with either a solid or hematological malignancy.6,23,28–31,34,38 While the sample size of these studies ranged from 33 to 928, the majority (n = 15) included less than 100 people.23,25,27–30,33,35,37,39,41,43–45
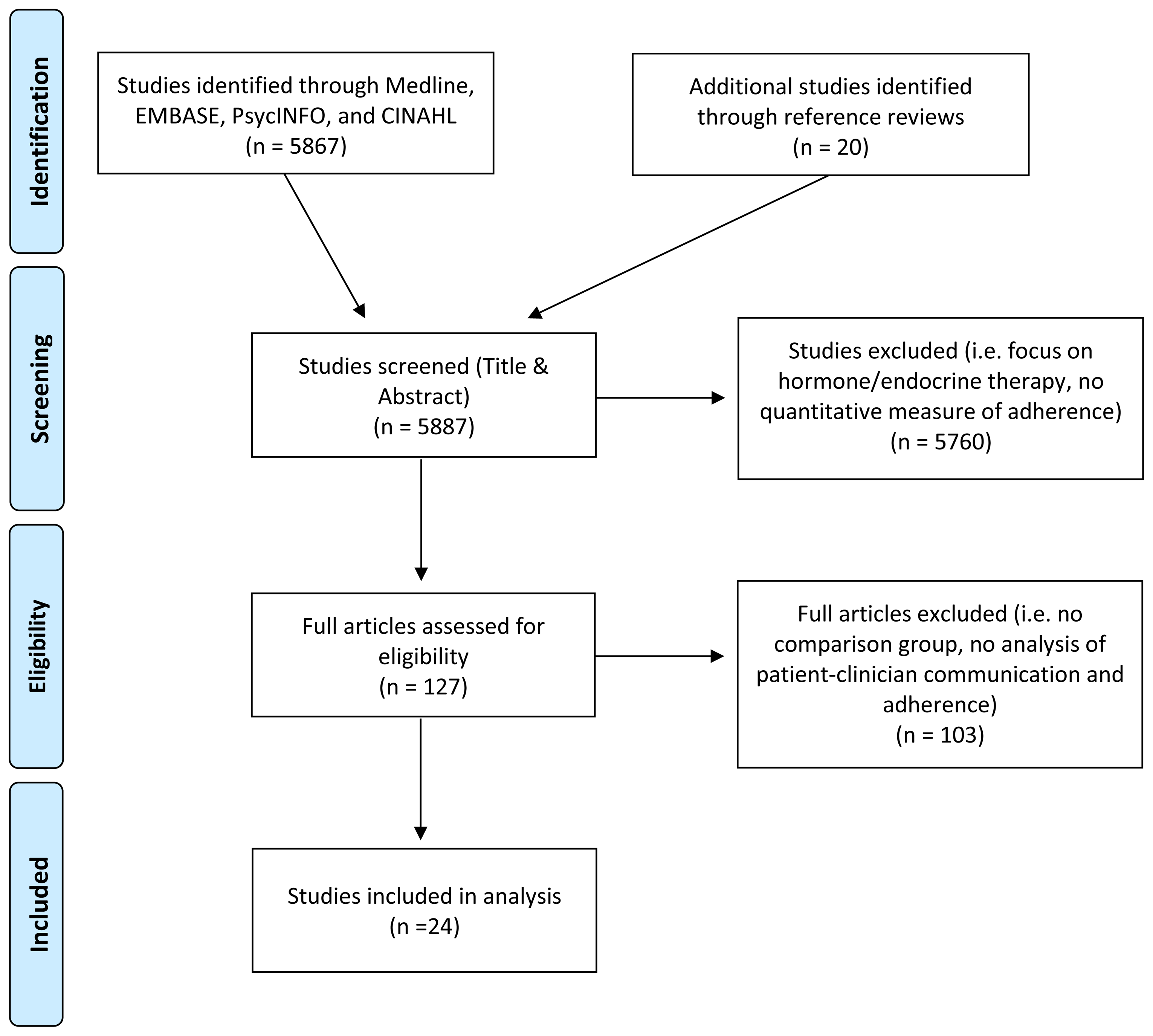
Study identification.
Characteristics of included studies.
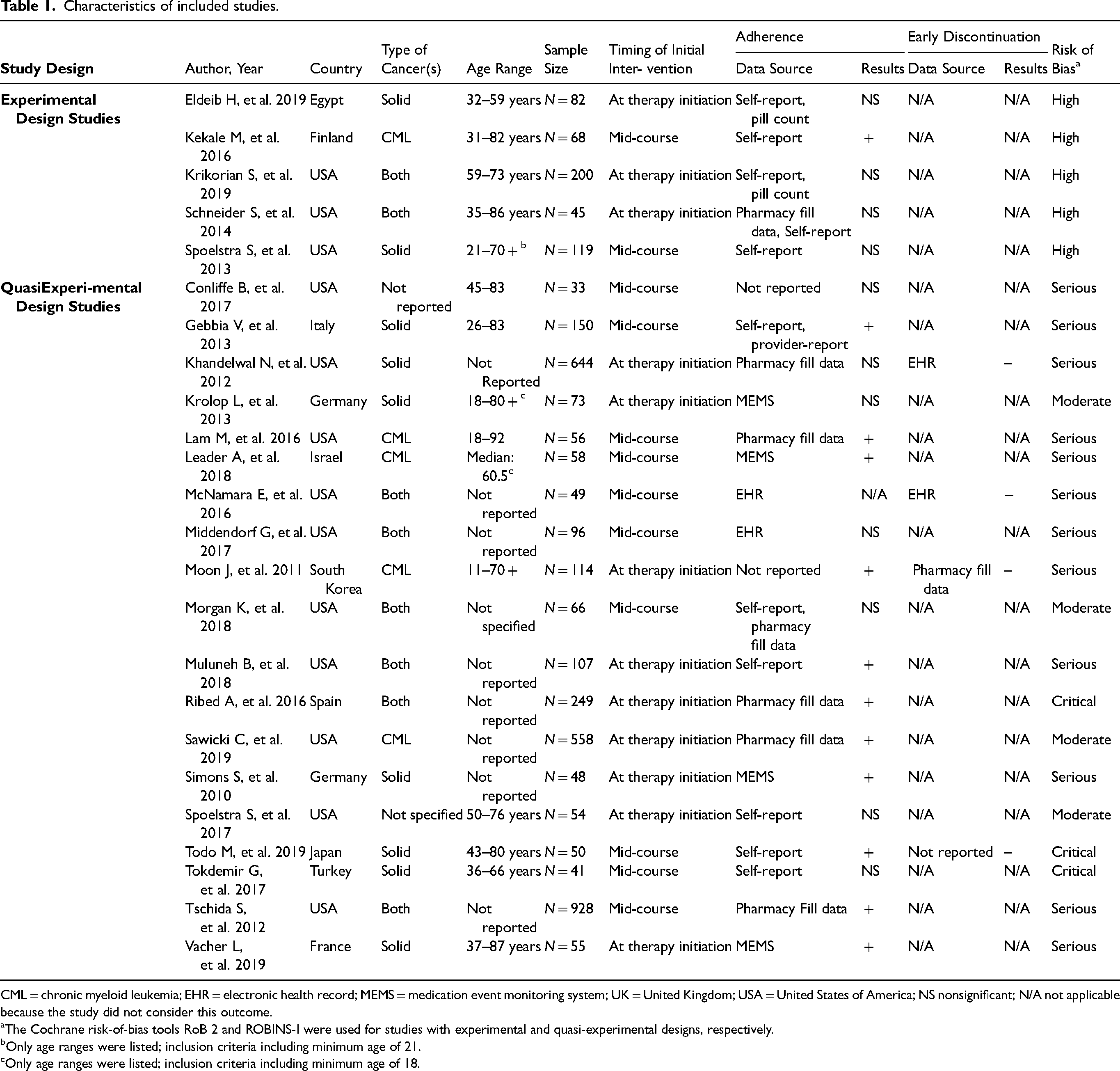
CML = chronic myeloid leukemia; EHR = electronic health record; MEMS = medication event monitoring system; UK = United Kingdom; USA = United States of America; NS nonsignificant; N/A not applicable because the study did not consider this outcome.
The Cochrane risk-of-bias tools RoB 2 and ROBINS-I were used for studies with experimental and quasi-experimental designs, respectively.
Only age ranges were listed; inclusion criteria including minimum age of 21.
Only age ranges were listed; inclusion criteria including minimum age of 18.
Measurement of medication adherence
All studies assessed patients’ medication use between two defined time points (i.e. therapy implementation adherence). For half of the studies, this observation began at the time of therapy initiation. Regardless of when the measurement observation was initiated, the specific length of time over which medication use was observed was highly variable, ranging from 60 days to over one year. As indicated in Table 1, patients’ medication taking between these two time points was measured using various data sources, including patient self-reports (n = 6),24,31,33,35,43,44 pharmacy fill records (n = 5),26,27,32,34,38 and electronic pill caps (n = 4).37,39–41 Other studies relied solely on information obtained from electronic health records (n = 2).28,29 Some studies used a combination of data sources, such as self-reports combined with pharmacy fill records (n = 2)23,30 or pill counts (n = 2),6,45 or a combination of patient self-reports and provider reports. 36
In addition to considering a patient's medication taking behaviour between two defined points in time, four studies also evaluated the duration over which patients took their medications. These four studies focused on patients’ early discontinuation of therapy or a patient having stopped treatment without instruction from a clinician.26,28,42,43 Among the three of these studies that reported the data source used for the measure of early discontinuation, two reported using the EHR26,28 and the other reported using pharmacy fill data. 42
Theories, models and frameworks used for study/intervention design
Only two studies reported using an established theory or model to guide intervention design.33,45 These studies used the Health Belief Model 45 and Social Cognitive Theory. 33 Other studies25,38,44 reported using published clinical standards, such as those developed by the American Society of Clinical Oncology and Oncology Nursing Society, 17 to guide intervention design.
Intervention structure and content
Fourteen of the papers6,23,25,27,29–32,34,38–40,43,45detailed some sort of pharmacist-based programme, five a nurse-based programme,24,33,35,42,44 and one that used a combination of nurses and pharmacists. 26 (Table 2) All papers described the intervention as addressing the management of side effects. Beyond the provision of side effect event management, papers described a range of educational and counselling components. More than half of the programme descriptions referenced providing written educational materials,6,23–26,28,30,31,34–40,42,44 and medication storage and handling information.6,29–33,38–44 Less commonly reported was guidance regarding concomitant medication management,25,31,37,38,41,44 possible drug/drug or drug/food interactions,6,25,27,31,37,38,41,44 and plans for missed doses.6,27,30,37,40,44,45 The provision of referrals to other supportive programming23,27,34 or guidance regarding financial assistance28–30,34 was infrequently noted as being provided.
Intervention structure and content.
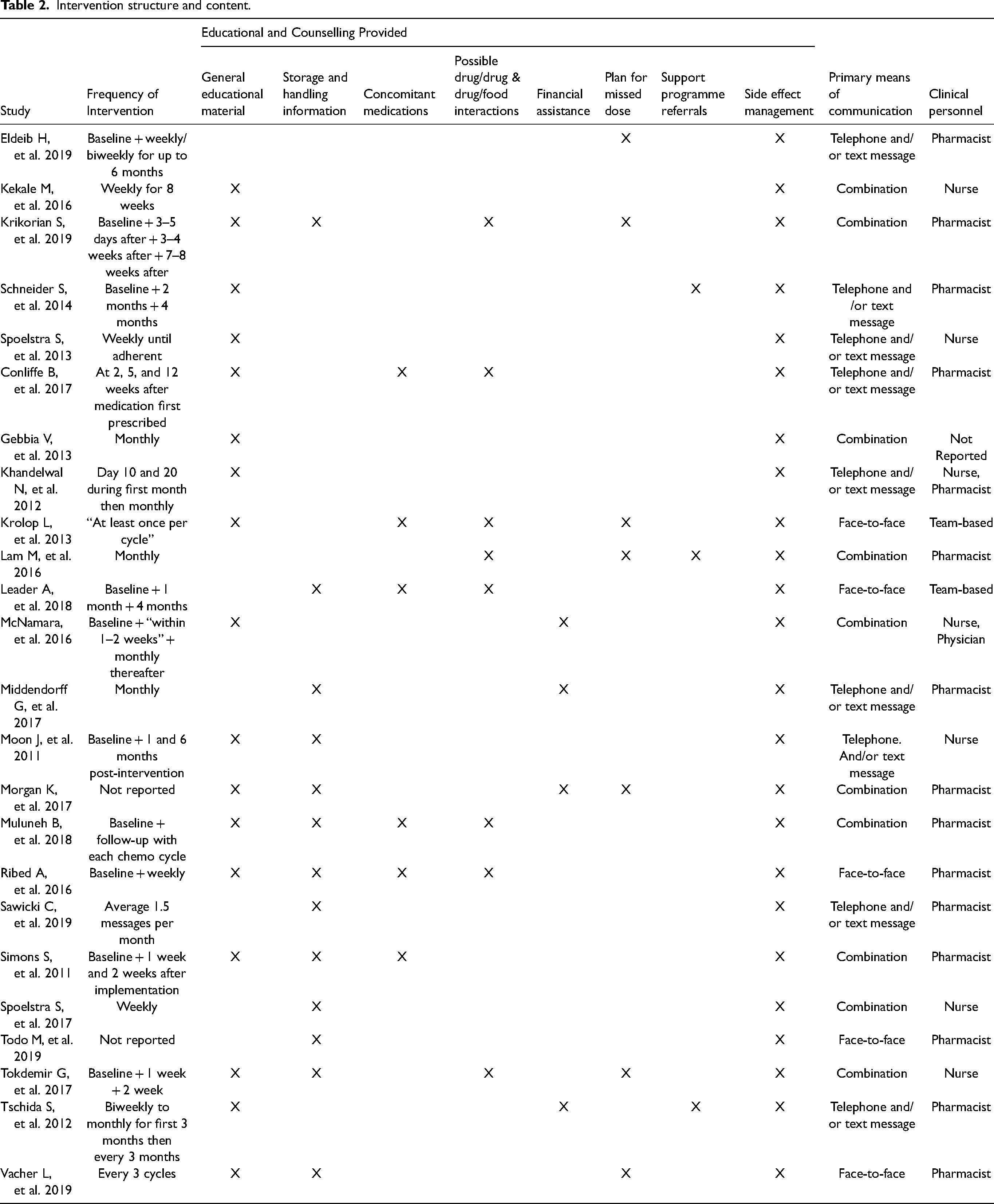
Only five programmes were described as being delivered via only in-person encounters,37,38,40,41,43 while nine programmes were described as being delivered via a combination of telephone- and text message-communications.23–26,29,32,34,42,45 Most programmes were delivered via a combination of these communication channels.6,27,28,30,31,33,35,36,39,44 There was little, if any, consistency in the frequency with which programme staff initiated outreach to patients (Table 2).
Study findings
Exactly half of the studies reported finding a statistically significant and positive relationship between programme receipt and medication adherence between two defined time points.27,31,32,34–36,38–43 We did not discern any patterns regarding either the structure or content of programmes reporting a statistically significant relationship between programme receipt and medication adherence in comparison to those that did not find a statistically significant relationship. For example, studies that reported a statistically significant relationship between program receipt and medication adherence included programmes targeting patients with CML, solid tumours or both, with a similar distribution among those not reporting significant findings. Likewise, programmes that were and were not effective at improving adherence targeted patients at the time of at therapy initiation and midcourse, and measured adherence via self-report or otherwise. Notably, however, all five studies targeting patients with CML alone found a statistically significant and positive relationship between the tested intervention and medication adherence. Nor did the content of successful programmes as described by study authors differ from those among studies with nonsignificant findings. For example, while most of the successful programmes provided general educational material, so did most other programmes. Nor did we note differences between the frequency of scheduled interventions or the licensure of the staff between programmes that did and did not positively affect medication adherence, although programmes that included at least some face-to-face contact seemed to perform better than those relying on telephone and/or text communications alone. All four studies that assessed the relationship between programme receipt and early discontinuation of therapy reported a statistically significant and negative association with programme receipt, albeit with a similar lack of consistency across programme structure and content.26,28,42,43
Risk of bias
Among the five randomized trials, each study had a high risk of bias.6,23,24,35,45 Non-randomized studies had a similar high/critical risk of bias, with four exceptions,30,32,33,37 each of which faced moderate risk. The most common reasons introducing a risk of bias among the 24 studies were their small sample sizes and/or a lack of controlling for confounders. For example, despite strong evidence,12,13,46 studies rarely considered patients’ health literacy, depressive symptoms or the complex role that race and ethnicity often play in the context of medication adherence.
Discussion
We identified two dozen studies, all of which have been published since 2010, that quantitatively assessed the relationship between an interpersonal communication-, education- or counselling-based intervention and adherence to oral anticancer therapy. Collectively, this literature illustrates a continued void in scholastic attention regarding how best to optimize medication adherence among patients prescribed oral anticancer therapy as well as the diversity of educational and counselling approaches used to support patients prescribed oral anticancer therapy. Exactly half of the studies identified reported statistically significant improvements in therapy adherence in relation to the intervention tested. However, we found little consistency in terms of type of education / counselling content, frequency of outreach, channel used for communication, or type of clinician delivering the content and no apparent associations between these and improved adherence outcomes. Furthermore, virtually all studies faced substantial risk of bias. Despite these shortcomings, programmes targeting patients with CML and those offering at least some counselling / educational sessions in person appeared to hold the most promise.
While our findings are consistent with those from two recent reviews,8,47 our focus on the specific educational and counselling content along with the communication channel and training of the person delivering the intervention offer additional insights. Notably, while we found many of the interventional studies provided counselling content consistent with clinical guidelines, and thus current practice recommendations, only two appeared to be grounded within an established theory or framework. Although this finding likely reflects that such studies are currently being conducted by clinicians—often as part of institutional quality improvement initiatives—it also highlights an opportunity as there are advantages to using behavioural models when studying and promoting medication adherence, including the ability to identify and address causal mechanisms underlying medication nonadherence. 48 For example, systematic reviews focusing on medication adherence, regardless of disease context, consistently have identified factors such as medication beliefs, self-efficacy, and social support as factors important to medication adherence.49–51 Furthermore, a recent review specifically focused on the psychosocial motivators and barriers to oral anticancer medication adherence among breast cancer patients has highlighted the importance of these same factors (i.e. medication beliefs, self-efficacy, and social support) to therapy adherence. 52
In addition to considering behavioural theories, an abundance of literature now illustrates the importance of a combination of patient, condition, socioeconomic, provider/system, and therapy factors affecting medication adherence.50,53 Particularly relevant in the context of oral chemotherapy is reimbursement policy and associated costs, which have consistently been found to serve as barriers to medication access.54–56 Of note are recent studies highlighting gaps in coverage due to underinsurance. 57 Given the known racial disparities in medication adherence58–60 identifying and targeting such structural barriers would seem prudent to ensuring that equity is considered in programme design. As only four of the studies identified by this review explicitly described offering guidance regarding financial assistance, considering how counselling-based interventions can best assess and address financial barriers throughout the course of therapy may be likewise important.
As evidenced by this review, little detail is known not only about what educational content and counselling is needed, but also about how often counselling should occur and how best to individualize communication to meet the diverse needs of cancer patients. The reality is that what is needed by way of intervention may likely differ across the continuum of therapy from initiation to discontinuation as well as by whether therapy is curative in intent or otherwise, and a multitude of other patient, therapy, and other more structural factors. Although our review focused on interpersonal communication-, education-, and counselling-based interventions to improve adherence, many clinicians may not even be aware of their patients’ medication taking behaviours. A cross-sectional study of 254 healthcare providers found that 44% of physicians and 50% of nurse practitioners did not know the level of adherence of their patients to oral chemotherapy despite 78% and 87%, respectively, reportedly knowing the consequences of non-adherence. 61 This suggests that adherence assessment and monitoring may not be a high priority in clinical practice due to a variety of reasons, including voids in knowing how best to go about doing so.
Results from this review should be interpreted considering important limitations. First and foremost is the small number and poor quality of available studies. In addition, among included studies, we found variability in both the populations targeted and measurement of medication adherence as well as in intervention content, frequency, and communication channel.
Conclusion
As former US Surgeon General C. Evertt Koop stated over 20 years ago “Drugs don’t work in people who don’t take them.” 62 In addition to the morbidity and mortality costs to patients and their loved ones, non-adherence comes at an economic cost 63 and can lead to avoidable medical consequences for patients if a physician, unaware of their patient's medication adherence status, interprets the progression of disease to treatment failure and unnecessarily intensifies a treatment regimen instead of offering interventions to improve adherence. Our review highlights how the evidence base regarding how best to support oncology patients in their adherence to prescribed oral anticancer therapy remains in its infancy—greatly in need of rigorous and large-scale studies that can advance patient-targeted educational and counselling practices and the scientific approaches to studying medication adherence within oncology care.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by the University of North Carolina at Chapel Hill