
Abstract
The analysis was conducted to assess the pharmacological costs of regorafenib and trifluridine/tipiracil in the treatment of refractory metastatic colorectal cancer (mCRC). Pivotal phase III randomized controlled trials (RCTs) of regorafenib and trifluridine/tipiracil in the treatment of refractory mCRC were considered. We have also considered the ReDOS trial, in order to verify if the dose-escalation strategy (practice changing for regorafenib) could influences the results. Differences in OS (expressed in months) between the different arms were calculated and compared with the pharmacological costs (at the Pharmacy of our Hospital and expressed in euros (€)) needed to get one month of OS. Trifluridine/tipiracil resulted the less expensive, with 1167.50 €per month OS-gained. The ReDOS trial further reduce costs with 510.41 €per month OS-gained in favour of regorafenib with the escalation-dose strategy. Both regorafenib and trifluridine/tipiracil can be considered economically sustainable treatments for refractory mCRC, apparently with a lower cost of trifluridine/tipiracil. The adoption of a dose-escalation strategy (ReDOS trial) could reverse the situation making regorafenib more cost-effective than trifluridine/tipiracil.
Recently, trifluridine/tipiracil, a new oral combination therapy, offered a therapeutic possibility beyond the second-line for patients affected by metastatic colorectal cancer (mCRC), with the improvement in clinical outcomes and prolonged survival. 1 This therapeutical option in refractory mCRC adds to regorafenib, a small-molecule multikinase inhibitor, that improved overall survival (OS) in the pivotal phase III RCTs (CORRECT trial 2 and CONCUR trial 3 ). More recently, the ReDOS trial, 4 a phase II randomized controlled trial (RCT), evaluated the safety and activity of two regorafenib dosing schedules: standard-dose strategy (62 patients, 160 mg/day orally for 21 days of a 28-day cycle) and escalation-dose strategy (54 patients, starting dose 80 mg/day orally with weekly escalation, per 40 mg increment, to 160 mg/day regorafenib). The primary endpoint (the proportion of evaluable patients initiating cycle 3) was met with 43% of patients in the dose-escalation group that initiated cycle 3 versus (vs.) 26% in the standard-dose group (p = 0.043). No head-to-head comparison of regorafenib vs. trifluridine/tipiracil in refractory mCRC were reported in literature. The introduction of these active new agents for the treatment of mCRC is associated with a relevant increase of costs and it is therefore important to make a balance between the costs of treatment and the added value represented by the improvement of the clinical parameters of interest such OS. The analysis was conducted to assess the pharmacological costs of regorafenib and trifluridine/tipiracil in the treatment of refractory mCRC.
Pivotal phase III RCTs of regorafenib and trifluridine/tipiracil in the treatment of refractory mCRC were considered. We have also considered the ReDOS trial, 4 in order to verify if the dose-escalation strategy (practice changing for regorafenib) could influences the results. Differences in OS (expressed in months) between the different arms were calculated and compared with the pharmacological costs needed to get one month of OS. The costs of drugs are at the Pharmacy of our Hospital and are expressed in euros (€), updated to January 2020. Calculations were based on an “ideal patient” (BSA 1.8 sqm; weight 70 Kg). The dosage of drugs were considered according to those reported in each RCT. We assumed the following costs: regorafenib= 23.09 €for each tablet (40 mg), trifluridine/tipiracil= 23.25 €for each tablet of 20 mg and 23.81 €for each tablet of 15 mg. We have subsequently applied the European Society for Medical Oncology Magnitude of Clinical Benefit Scale (ESMO-MCBS) to the above RCTs, 5 to derive a relative ranking (from grade 1 to grade 5) of the magnitude of clinically meaningful benefit that can be expected in this setting 6 ; adjustments (upgrade or down-grade) are planned based on quality of life (QoL) or grade 3-4 toxicities impacting daily well-being. 5 Three phase III RCTs and 1 phase II RCT, including 1880 patients, were considered. The main reported outcomes of the analyzed phase III RCTs are reported in Table 1. ESMO-MCBS (Table 1) reached grade 4 for ReDOS trial, 4 grade 3 for the CONCUR trial, 3 grade 2 for the RECOURSE trial 1 and grade 1 for the CORRECT trial. 2 Combining the costs of therapy with the measure of efficacy represented by the OS, we get the costs for obtaining the advantage in OS, for each arm of the analyzed trials. Trifluridine/tipiracil resulted the less expensive, with 1167.50 € per month OS-gained (Table 1). The ReDOS trial 4 further reduce costs with 510.41 €per month OS-gained in favour of regorafenib with the escalation-dose strategy.
Pharmacological costs and difference in OS with regorafenib and trifluridine/tipiracil in RCTs in refractory mCRC.
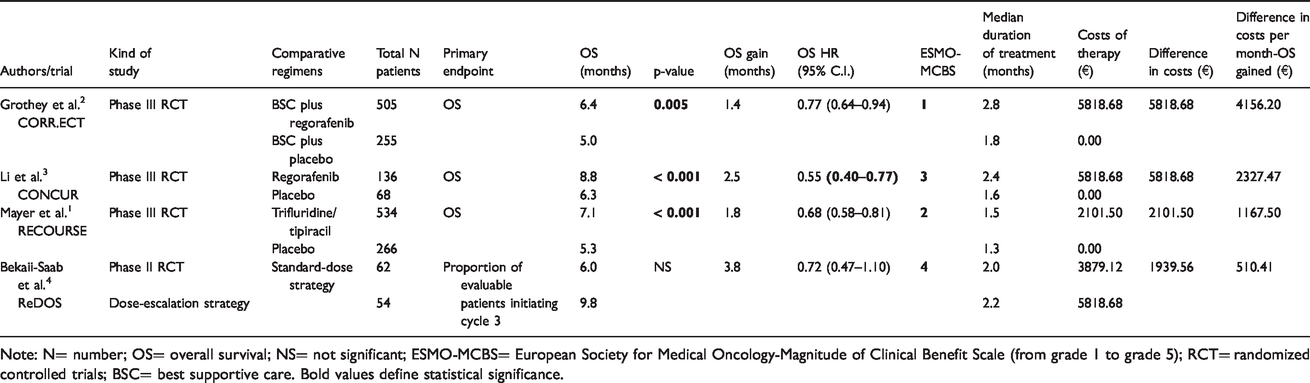
Note: N= number; OS= overall survival; NS= not significant; ESMO-MCBS= European Society for Medical Oncology-Magnitude of Clinical Benefit Scale (from grade 1 to grade 5); RCT= randomized controlled trials; BSC= best supportive care. Bold values define statistical significance.
From the data presented it is easy to see that the pharmacological costs were influenced by two main factors: the efficacy of the therapies (strictly associated with the patient's inclusions criteria) and the price of drugs used. Furthermore, we needed RCTs to allow comparison of efficacy between the arms of each trial. Despite this, our analysis has several limitations, such as cross-trial comparisons. Moreover, we have considered only the direct costs, but there are other important cost elements that are not considered here (e.g. outpatient/inpatient administration costs or treatment-related adverse event costs or health-related quality of life between different first-line treatments).7,8 In facts, the data we have reported are not a real cost-effectiveness analysis (that would imply not only direct medical costs, but also indirect medical costs), but an analysis of pharmacological costs; we also know the limits of completeness of this costs analysis, that not considered the toxicity of the different schemes were not considered, because it implies a different analysis. In particular, referring to pivotal phase III RCTs, grade 3 or higher treatment-related adverse events occurred in the 54% of patients treated with regorafenib2,3 and in the 69% of patients treated with trifluridine/tipiracil 1 (in particular, 38% had neutropenia of grade 3 or higher, 4% had febrile neutropenia, and 9% received granulocyte colony-stimulating factor) and this could affect cost management.
The introduction of regorafenib dose-escalation strategy in the ReDOS trial 4 could really practice-changing and it is also confirmed by cost-effectiveness profile with a low cost per month of OS-gain (510.41 €).
In addition, the annual cost of drugs treatment (14,010 €for trifluridine/tipiracil and from 27 929.64 € 3 to 49 874.40 € 2 for regorafenib) are in line with those reported in literature, that found a favored implementing intervention for thresholds of less than $61,500 (57,138 €) per life-year gained. 9 Concerning regorafenib, different results were obtained in the CONCUR trial 3 and in the CORRECT trial. 2 The limit is that the CONCUR trial 3 was done in a broder population of Asian patients with previously treated mCRC and we know that this is a different population than Caucasian patients, with a possible different response to therapy. These results are also more important in we consider ReDOS trial, 4 with annual cost of 6124.92 €(in line with literature 9 ).
The pharmacological costs are transferred to the Italian reality and, more generally, to Europe (free movement of patients and goods). The idea is to emphasize not only the cost topic, but also the method, which is to combine the pharmacological costs of drugs with the measures of efficacy (OS), in order to achieve a given objective as possible. This method incorporates a structured, rational and valid approach to data interpretation and analysis that can help clinicians to weigh the relative merits of competing relevant therapeutic options in situations in which there is no direct comparative data comparing the available therapeutic options. 5 To this must be added that the use of ESMO-MCBS to standardize a scientific validity has some criticism, such as the use of the lack of consideration of toxicities in the definition of the grade of magnitude of clinical benefit.
However, to our knowledge, this is the first time an analysis of the pharmacological costs of refractory mCRC treated with regorafenib or trifluridine/tipiracil is linked to OS, with the addition of drug dosage-strategy. 4
In light of the relevant expenses of these new drugs it might be also interesting to compare the costs of regorafenib and trifluridine/tipiracil for the treatment of refractory mCRC with the costs of immune check point inhibitors (ICIs, nivolumab, pembrolizumab and atezolizumab) registered in other tumors (eg. NSCLC, head and neck carcinoma, urological malignancies) and known as the most expensive new drugs in medical oncology10–15 and the costs of the reference elements in international markets, gold 18 karat (K) (currently listed on 45. 916 €per gram) and platinum (currently listed on 28.53 €per gram). ICIs are very expensive (already known), with pembrolizumab that has the highest cost (205 608.00 €per gram) towards nivolumab (107 500.00 €per gram) and atezolizumab (1726.03 €per gram), with a Δ toward gold 18 K and platinum per gram of 205 561.10 €and 205 586.55 €for pembrolizumab, respectively, of 107 453.10 €and 107 478.55 €for nivolumab, respectively and of 1680.87 €and 1697.50 €for atezolizumab, respectively. Both regorafenib and trifluridine/tipiracil have a highest cost per gram, with 577.25 €(regorafenib), 1.162.50 €(trifluridine/tipiracil, 20 mg tablets) and 1587.33 €(trifluridine/tipiracil, 15 mg tablets), with a Δ toward gold 18 K and platinum per gram of 532.09 €and 548.72 €for regorafenib, respectively and of 1117.34 €(20 mg tablets), 1542.17 €(15 mg tablets) and 1133.97 €(20 mg tablets), 1558.80 €(15 mg tablets) for trifluridine/tipiracil, respectively. So, a reduction in pharmacological costs is mandatory if we want to consider regorafenib and trifluridine/tipiracil even more advantageous in terms of cost-effectiveness.
Combining pharmacological costs of drugs with the measure of efficacy represented by the OS, both regorafenib and trifluridine/tipiracil they can be considered economically sustainable treatments for refractory mCRC, apparently with a lower cost of trifluridine/tipiracil. The adoption of a dose-escalation strategy (ReDOS trial 4 ) could reverse the situation making regorafenib more cost-effective than trifluridine/tipiracil. The price of newly registered oncologic drugs is continuously increasing posing a serious treat to the sustainability of the National Health Systems, especially in Countries in which the public control and oversight over the prices is limited. Medical Oncologists and the society as a whole are becoming more and more concerned with the issues of the costs of cancer treatments and are able to bring attention to the “just price” of new treatments that must reflect the reality of their true benefits and societal and personal costs.
Footnotes
Authors’ Contribution
All authors contributed equally to (1) conception and design, acquisition of data, or analysis and interpretation of data; (2) drafting the article and revising it critically for important intellectual content; and (3) final approval of the version to be published.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.