
Abstract
Introduction
Chemotherapy-induced nausea and vomiting is a serious complication of cancer treatment that compromises patients’ quality of life and treatment adherence, which necessitates regular assessment. Therefore, there is a need to assess patient-reported nausea and vomiting using a validated scale among Arabic speaking cancer patient population. The objective of this study was to translate and validate the Functional Living Index-Emesis (FLIE) instrument in Arabic, a patient-reported outcome measure designed to assess the influence of chemotherapy-induced nausea and vomiting on patients’ quality of life.
Methods
Linguistic validation of an Arabic-language version was performed. The instrument was administered to cancer patients undergoing chemotherapy in a tertiary hospital's cancer center in Saudi Arabia.
Results
One-hundred cancer patients who received chemotherapy were enrolled. The participants’ mean age was 53.3 ± 14.9 years, and 50% were female. Half of the participants had a history of nausea and vomiting with previous chemotherapy. The Cronbach coefficient alpha for the FLIE was 0.9606 and 0.9736 for nausea and vomiting domains, respectively, which indicated an excellent reliability for the Arabic FLIE. The mean FLIE score was 110.9 ± 23.5, indicating no or minimal impact on daily life (NIDL).
Conclusions
The Arabic FLIE is a valid and reliable tool among the Arabic-speaking cancer population. Thus, the Arabic version of the FLIE will be a useful tool to assess the quality of life among Arabic speaking patients receiving chemotherapy. Additionally, the translated instrument will be a useful tool for future research studies to explore new antiemetic treatments among cancer patients.
Introduction
Chemotherapy-induced nausea and vomiting (CINV) is a preventable complication of cancer therapy that can negatively impact the patients’ quality of life and performance status. Thus, compromising the treatment outcomes.1,2 Despite significant improvement in CINV prophylaxis practices, the incidence of nausea and/or vomiting following chemotherapy still exists in approximately 40% of cancer patients. 3
There are seven self-assessment tools for CINV. 4 The Functional Living Index-Emesis (FLIE) instrument is a patient-reported outcome measure designed and validated by Lindley et al, to assess the influence of CINV on daily functioning, particularly patients’ quality of life. 5 The FLIE instrument has been used in several clinical trials of marketed antiemetics. The FLIE has 18 questions and is examine two domains: nausea (questions 1–9) and vomiting (questions 10–18), and focus on functional impact. The first item in each domain asked the patient to rate how much nausea and vomiting they had experienced. The remaining eight items covered different sections influencing the patient’s quality of daily life (i.e., “recreation or leisure activities,” “make meals/do tasks”, “ability to enjoy meals”, “enjoy drinking fluids”, “see family/friends”, “daily functioning”, “personal hardship”, and “hardship on others”). The minimum domain score is 9, and the maximum domain score is 63. Higher scores indicate less impairment in daily life due to nausea or vomiting, and scores ≤108 were defined as “interference with daily functioning”.5,6 Patient-reported outcome use in cancer patients has been positively associated with symptom control, supportive care responses, patient satisfaction, and well-being. 7
The FLIE instrument was translated into more than 20 languages 8 and has been a beneficial tool for many researchers exploring new antiemetic options in cancer patients worldwide. However, the instrument was not translated into Arabic, the official language of Saudi Arabia and over 20 other countries and one of the six official languages of the United Nations. 9 The study aims to translate, culturally adapt, and validate the FLIE instrument in Arabic.
Methods
Study design and setting
A prospective cohort study was conducted at the cancer center of King Khalid University Hospital, King Saud University Medical City, a teaching hospital with 1200 beds, located in Riyadh, Saudi Arabia. The study was approved by the Institutional Review Boards of King Saud University Medical City.
Selection of participants
The participants of this study were recruited between May 2018 and May 2019 among patients admitted to the cancer center. The convenience sampling method was used. Arabic speaking patients above or equal to 18 years-old, who are actively receiving chemotherapy were included in the study. Written and signed informed consent was obtained from all prospective participants before study entry. Patients’ electronic medical records were reviewed to verify that they did receive the medications. Patients who were not on active chemotherapy sessions were excluded. Patients’ identification numbers were encrypted to maintain the data confidentiality and stored in password-protected and limited-access computers.
Data source
Mapi Research Trust granted permission for validating and using the Functional Living Index –Emesis (FLIE) instrument. 5 The FLIE contact information and permission to use: Mapi Research Trust, Lyon, France. Internet: https://eprovide.mapi-trust.org. The process of the Mapi language services business unit linguistic validation of a clinical outcome assessment consists of four steps: (1) forward translation, (2) backward translation, (3) cognitive interviews (patient testing), and (4) proofreading.
Step 1: Forward translation: first, two local professional translators were recruited. Both were native Arabic speakers as well as good English speakers and have an experience with medical scales validation. Each of the translators produced an independent forward translation of the original instrument, including patient instructions and instrument questions. As a result, two forward translations were produced. A local coordinator was involved. Both translators and the local coordinator reviewed the translations. Some differences were identified and discussed. These difference include the following: (1) rewording the following parts of the instrument: “you are asked to rate”, “quality of life”, “daily functioning”, and “imposed a hardship”; (2) rephrasing the following parts: “if you are unsure of your answer or do not understand the question, read the question again carefully”, “at any point along the line”, and “usual recreation or leisure activities”. After a discussion, sentences that were equivalent to the original instrument and easy to understand by the target population were chosen. Finally, both translators and the local coordinator agreed on a reconciled pooled version (version 1). No interpretation problems of the original instrument were found.
Step 2: Backward translation: a local professional translator was recruited. A backward English version was produced after the translators translated the first version of the instrument into Arabic in step 1. The translator had no access to the original version of the instrument. After that, a local coordinator completed a comparison of the backward version with the source language. Some mistranslations in the first version of the instrument were identified. Accordingly, changes were made to the first version, resulting in the second version.
Step 3: Cognitive interviews (patient testing): the instrument was sent to clinical pharmacist practicing in the oncology center and an oncologist to review and ensure the content are relevant to what we are intended to examine. The instrument was then reviewed by all investigators to check subjectively the relevance of the instrument to ensure face validity. Thereafter, the translated scale was pilot tested among fifteen cancer patients to check the comprehensibility of the scale’s items. All were native Arabic speakers. The comprehension test was performed through individual interviews. During the interviews, the local coordinator inquired whether the participants had any difficulty understanding the instrument and checked the participants’ interpretation of all items. Generally, the translated instrument was well understood by the patients, with no significant difficulties. One patient had an issue understanding the part that explained the correct answering method; it was changed accordingly to an alternative proposed by the interviewer. The other patients had no issues. As a result, a third version of the instrument was produced.
Step 4: Proofreading: was done to eliminate any typing, spelling, or grammatical mistakes remaining in the most recent target-language version. An English linguist whose native language is Arabic proofread the third version of the instrument. The proofreading identified some grammar and spelling mistakes, which were adjusted accordingly. Thereafter, the final Arabic version of FLIE (Arabic-FLIE) was reviewed, and after all comments were addressed, approved by all members of the research team. The study adhered to the methodological guidelines for translation, adaptation, and validation of self-reported screening instruments. 10
Data collection
Several baseline demographic and clinical data were gathered upon hospital admission. These include age, gender, chemotherapy agents and cycle, if a patient has risk factors for nausea and/or vomiting including alcohol consumption, a history of smoking, a history of motion sickness, pregnancy, and history of nausea and/or vomiting with previous chemotherapy, or if rescue therapy of antiemetic was used during the first 5 days after. 11 Information about multiday chemotherapy agent use and antiemetic use was collected from the patients’ electronic medical records.
A pharmacy intern and a pharmacy resident interviewed subjects to gather socioeconomic characteristics of the patient population. The interviews took place in private rooms to ensure the privacy of the participants. Family members helped Illiterate patients. Health literacy was assessed using the Arabic version of the Single Item Literacy Screener (SILS). This tool consists of a single question that assesses the respondent’s ability to read and comprehend educational information and instructions about different medical conditions and medications without anyone’s help.12,13 The Multinational Association of Supportive Care in Cancer Antiemesis Tool (MAT) was used to record nausea and vomiting on day 1 (acute phase), the 24-h period after the initiation of chemotherapy, and days 2–5 (delayed phase), the 24-to-120-h period after initiation of chemotherapy 14 The FLIE-item score was assessed on the morning of day 6 post-chemotherapy. 15
Statistical analysis
For patients’ confidentiality, all data were coded, and no patient identifiers were collected. Frequencies and percentages were used to describe the categorical variables. Means and standard deviations, or median and interquartile range (IQR), were used to describe continuous variables. Bartlett’s test for sphericity was used to assess the sufficiency of the correlations between the questions to run factor analysis. 16 The Kaiser–Meyer–Olkin test (KMO) was used to assess sampling adequacy. 17 The internal consistency, i.e. reliability, of the Arabic-FLIE questionnaire, was examined using Cronbach’s alpha method. 18 Principle components factor analysis was performed to explore the structure of the Arabic-FLIE. The number of factors was identified by Eigenvalues greater than 1. In addition, we created a scree plot and rotated it using varimax rotation with orthogonal transformation for easier interpretation and smaller structure. 19 Statistical significance was defined by p < 0.05. All analyses were conducted using the STAT 14 (StatCorp 2015, Stata Statistical Software: Release 14. College Station, TX: StataCorp LP).
Results
Study population
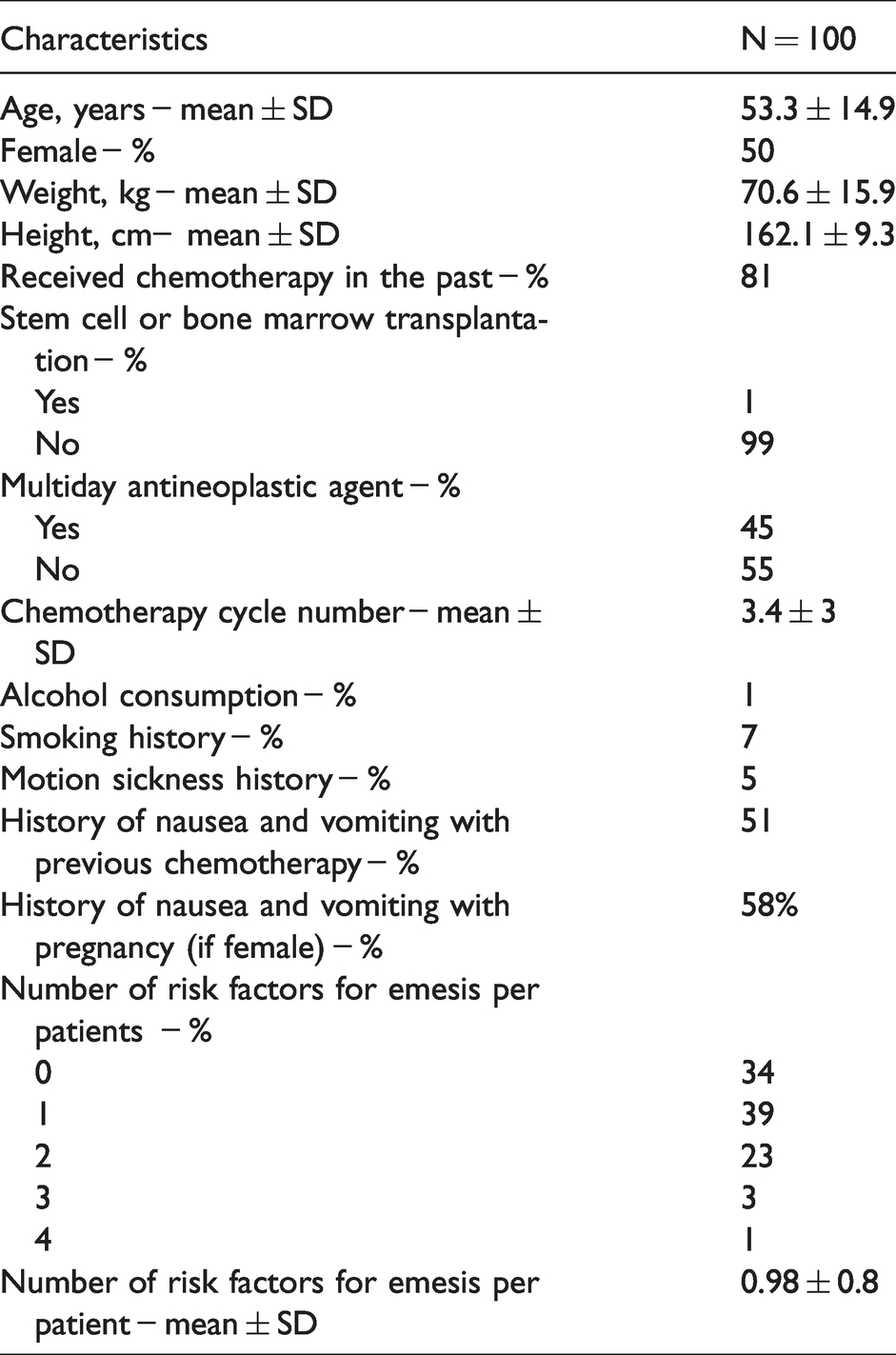
A total of 100 patients consented to participate in this study and were interviewed. The baseline characteristics of the patients are shown in Table 1. The mean age of the participants was 53.3 ± 14.9 years, and 50% of the participants were female. There were 45% of the patients who received a multiday antineoplastic(s) regimen. Eighty one percent of the patients had previous chemotherapy experience and around half of the patients (51%) had a history of nausea and vomiting with previous chemotherapy, where 66% of the patients had at least one risk factor for nausea and vomiting. According to the American Society of Clinical Oncology (ASCO) classification of the chemotherapy level of emetogenecity, 11 there were 45% and 27% of the patients who received moderate and severe emetogenic chemotherapy agents, respectively. Nausea and vomiting episodes in the acute phase occurred in 40% and 8% of the patients, respectively. Only 56% of the patients had a complete response, and 71% had no or minimal impact on daily life. The overall FLIE score for the cohort was 110.9 ± 23.5 (Table 2). The FLIE score for patients with complete response was 120.3 ± 1.8 versus 99 ± 4.2 for patients with no complete response, p value ≤0.001.
Baseline characteristics of patients on chemotherapy (N = 100).
Characteristics of chemotherapy agents used by the patients (N = 100).
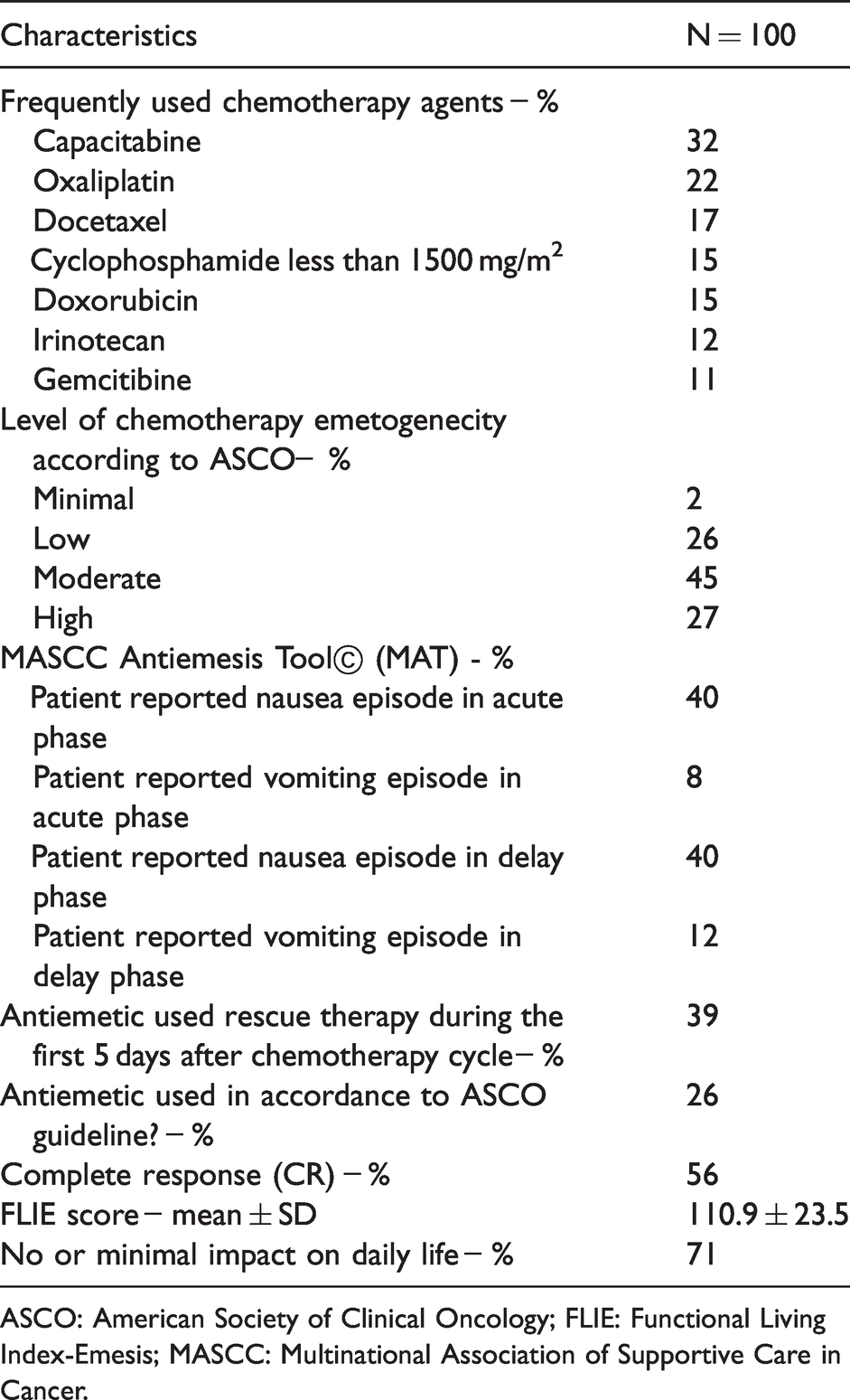
ASCO: American Society of Clinical Oncology; FLIE: Functional Living Index-Emesis; MASCC: Multinational Association of Supportive Care in Cancer.
Instrument validation
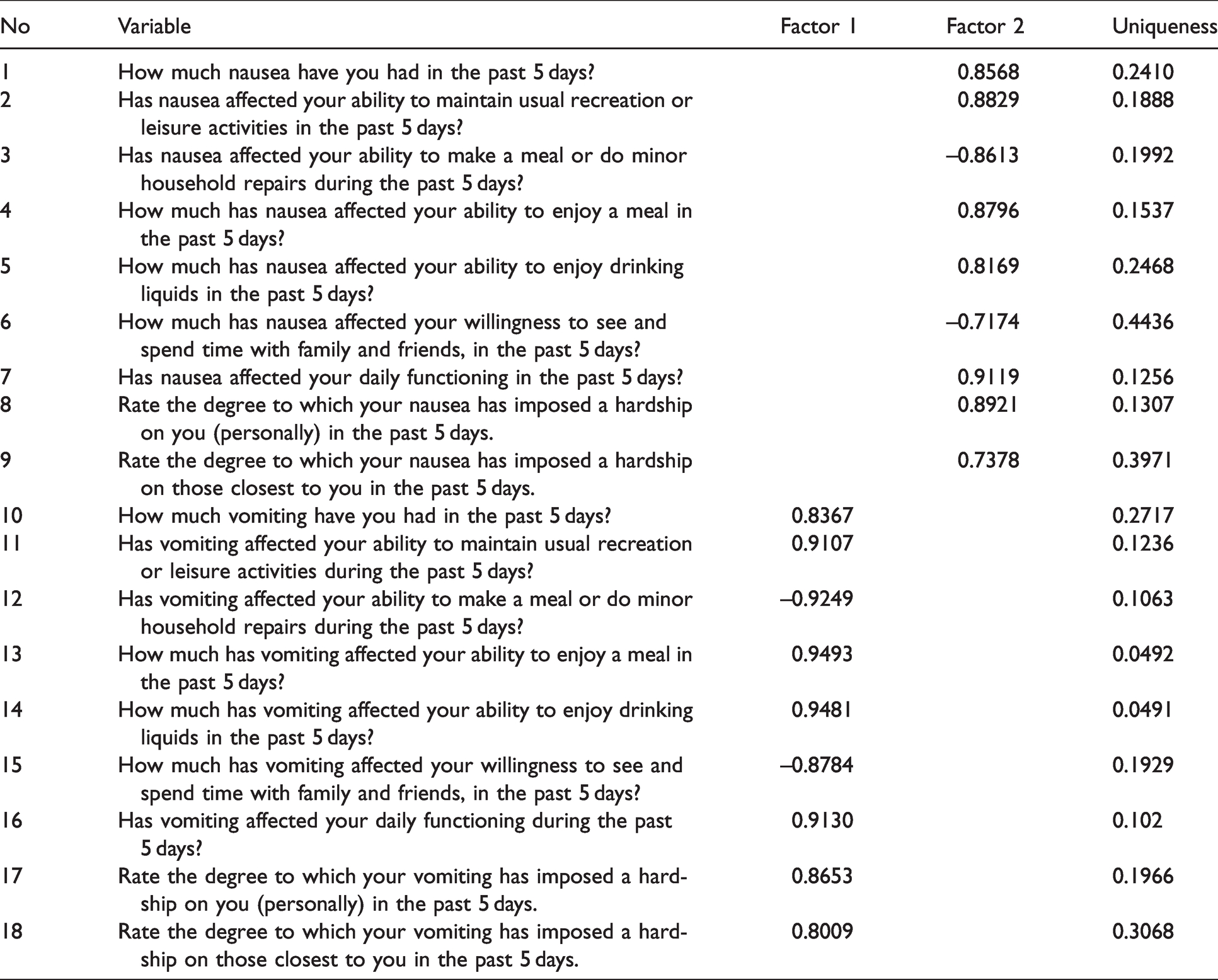
The Arabic-language versions of the FLIE instrument are shown in Supplementary Appendix 1. The organization of the questions and possible answers are the same in both versions of the instrument. The Bartlett’s test for sphericity was significant (P < 0.001) indicate sufficient intercorrelation between the items to run the principal components factor analysis. In addition, the Kaiser–Meyer–Olkin (KMO) test of 0.867 indicates that the sample size was adequate to conduct this type of evaluation. The internal consistency, measured by the Cronbach alpha coefficient, for both sets of questions for the nausea and vomiting domains was 0.9606 and 0.9736, respectively. The participants did not report problems with answering the questions included in the form. Two factors were extracted from the Arabic version of the FLIE using an Eigenvalue cutoff point of ≥1, as shown in Figure 1. Factor 1 was congruent with the domain for nausea, while factor 2 was consistent with the vomiting domain. The loading of each item of the Arabic-FLIE is presented in Table 3.
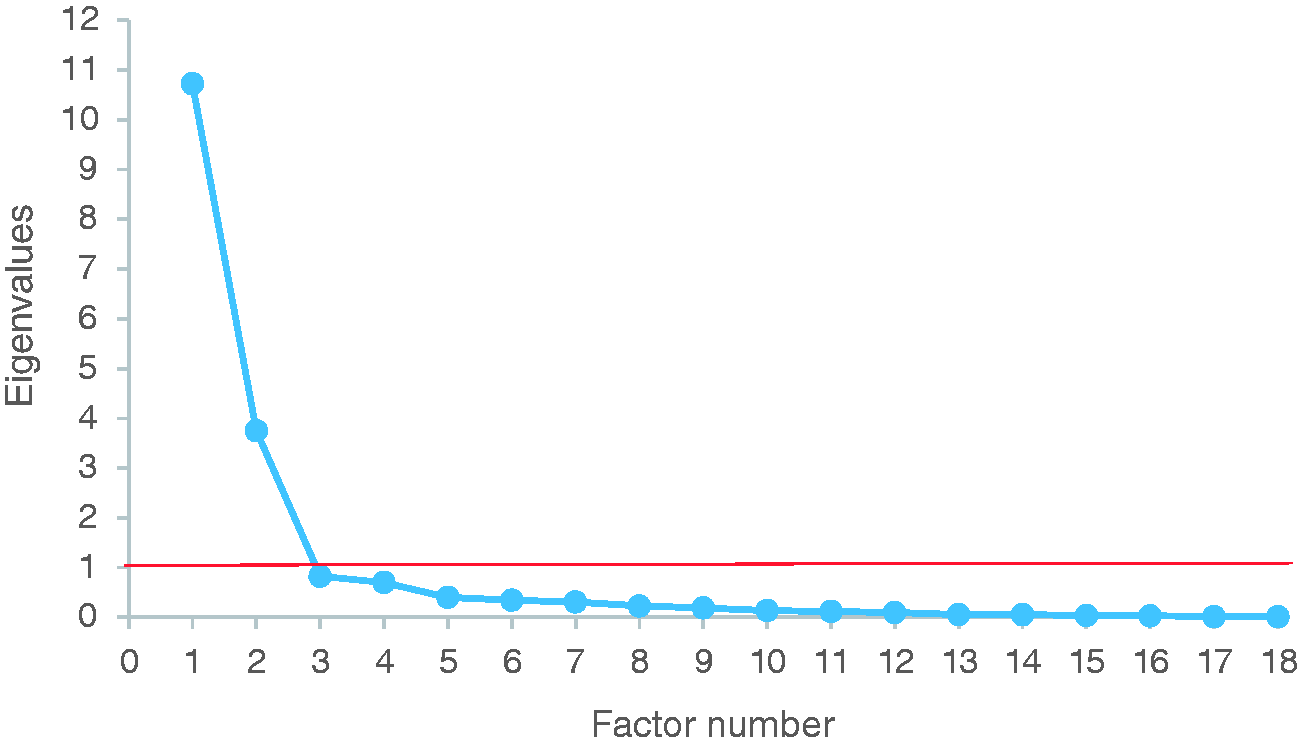
Numbers of factors that can be extracted from the Arabic version of Functional Living Index-Emesis and their eigenvalues.
Extracted factors from the Arabic version of Functional Living Index –Emesis (FLIE) questionnaire on chemotherapy (N = 100).
Discussions
This study led to the first translation and cultural validation of the Arabic-FLIE. It is a validated instrument to assess the impact of CINV on patients’ ability to maintain their daily life activities. 15 The Arabic-FLIE demonstrated a high level of internal consistency, as indicated by Cronbach’s alpha coefficients. The internal consistency was adequate and indicated a degree of coherence among items on the FLIE instrument. An alpha value of > 0.95 implies higher reliability of the Arabic version. The original three-day version’s reported internal consistency was > 0.9 5 while the internal consistency of the modified five-day version had excellent internal consistency (alpha value of 0.79). 15
Although CINV guidelines are routinely published and updated, several studies have shown that antiemetic guideline implementation is suboptimal. This could negatively impact treatment related outcomes. Severe CINV may require emergency care or hospitalization, yielding additional economic burdens for cancer care. 20 In Europe, the estimated cost for hospitalization per patient due to CINV was around $460 to $1310. 21 Two local retrospective chart reviews of around 300 oncology patients reported lack of conformity to ASCO guidelines for antiemetic management. Finding of these studies were confirmatory to our results. However, the incidence of acute and that of delayed nausea were higher in our population. Neither studies reported the impact of CINV on patients quality of life.22,23
Arabic is the sixth most frequently used language and is estimated to be the native tongue of 420 million people worldwide. With the projection of a 1.8-fold increase in cancer incidence in the Arab world by 2030, 24 it is imperative to utilize self-assessment instruments such as FLIE as part of the care in patients actively receiving chemotherapy. In Saudi Arabia, more than nine major national cancer centers provide cancer care for all patient populations. 25 In 2016, 16,859 new cases of cancer were registered. By 2030, the annual cancer incidence is projected to increase to around 40,000 and around 19,000 cancer deaths.26,27 Local societies, such as the Saudi Oncology Society, its subdivision—the Saudi Oncology Pharmacy Assembly—and others in the Arab world can work as advocates for disseminating and implementing this validated Arabic FLIE instrument across oncology centers for clinical and research purposes. This can be of added value to improving the quality of care for Arabic-speaking cancer patients undergoing chemotherapy. Utilizing the FLIE is also essential for assessing the effectiveness of prescribed medications.
Our study’s strengths include being the first to assess the validity and reliability of the Arabic FLIE as an assessment tool for Arabic-speaking cancer patients. This translation process considered the local cultural and linguistic context. Also, we have evaluated this survey in patients with different chemotherapy regimens and emetogenic risks. This might support the generalizability of our findings.
While this is the first study to translate the FLIE to Arabic, our main limitation was that we only covered a small number of patients in a single oncology center. Thus, assessing the external validity in a larger sample of Arabic speaking cancer patients across different healthcare systems would be necessary. Moreover, while nurses can be the primary personnel to introduce this instrument to the Arabic-speaking cancer patients, many institutions still lack adequate native Arabic-speaking nursing staff, limiting the external validity to other healthcare professionals.
Conclusions
We developed a valid and reliable version of the FLIE in Arabic that can be used to assess the impact of CINV on cancer patients’ quality of life. Additionally, the translated version will be a vital tool for future research that explores new antiemetic options for cancer patients.
Footnotes
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Supplemental material
Supplemental material for this article is available online.