
Abstract
Introduction
Patients whose solid tumors (ST) show leptomeningeal metastasis (LM) have very poor prognosis and short overall survival. The aim of this study was to evaluate the efficacy of first-line programed death-1(PD-1) monoclonal antibody (mAb) treatment in these patients.
Methods
We retrospectively evaluated patients diagnosed with LM from ST who were treated with first-line PD-1 mAb at our hospital between April 1 and November 30, 2019. We analyzed their clinicopathological characteristics and response to the treatment.
Results
We collected and analyzed data from 6 patients with different primary ST. 5 patients received PD-1 mAb combined with chemotherapy and/or anti-angiogenic drugs, while one received only PD-1 mAb. The median (range) number of treatment cycles was 5.5 (1-21). PD-1 mAb treatment did not cause neurotoxicity. The time period of first assessment varied from 21 to 65 days after treatment. Among 5 patients who got obvious symptoms relief, 4 patients persisted for > 3 months and even showed a reduction in the number of tumor cells in cerebrosprinal fluid. Ventriculoperitoneal (VP) shunt was used to treat hydrocephalus observed beneficial in 3 patients: 2 before and 1 after PD-1 mAb treatment. The median (range) follow-up time was 214 (57-460) days. 4 patients died. The overall survival ranged from 57 days to at least 460 days. 1 of the two alive patients continued to show no worsening of symptoms after 457 days.
Conclusions
Patients with LM from ST can benefit from first-line PD-1 mAb combined treatment without additional neurotoxicity. Further research is required to validate the safety and efficacy.
Introduction
Leptomeningeal metastasis (LM) is defined as the spread of cancer cells within the leptomeningeal and the subarachnoid spaces. LM is reported to showed in 8% of patients with solid tumors by autopisies, appearing in some cases as the first presentation of their cancer. 1 Disease prognosis is extremely poor, and LM patients are reported to have a median overall survival (OS) time of 3 months. 2 Multidisciplinary therapies such as targeted therapy, chemotherapy, radiotherapy, and surgical procedures can control extracranial metastasis and thereby prolong survival. However, clinicians have observed further LM during the extended survival period. For example, breast cancer patients experienced an increased risk of LM after undergoing stereotactic radiosurgery for the treatment of brain parenchymal metastasis. 3 Therefore, it is critical to identify effective treatments for LM.
Programed death-1 (PD-1) monoclonal antibodies (mAbs), such as nivolumab and toripalimab, were among the first immune checkpoint inhibitors to be approved for the treatment of extracranial recurrence and metastasis of solid tumors, such as lung, urothelial, and melanoma.4–6 PD-1 mAbs monotherapy or combination treatment have showed efficacy. Nivolumab has been demonstrated as an effective treatment for advanced squamous non-small-cell lung cancer (NSCLC) : patients showed an objective response rate of 19%, median progression-free survival (PFS) of 4.9 months, and median OS of 5.8 months. 7 Another study reported that a combination of pembrolizumab and chemotherapy can prolong OS to 19.2 months in nonsquamous NSCLC patients with brain parenchymal metastasis (BPM). 8
However, LM has been strictly limited or even excluded from most clinical trials in the past. 9 The data from real-world cases need to be supplemented. Therefore, we retrospectively analyzed the efficacy and safety of the PD-1 mAb to treat patients diagnosed with LM from solid tumors.
Methods
This study was approved by the Ethics Committee of “Blinded for peer review”.
Patients
We analyzed a consecutive patients with LM from solid tumors who had undergone first-line PD-1 mAb treatment at the Department of Oncology in “Blinded for peer review”between April 1 and November 30, 2019. We included patients who had positive cytology in the cerebrospinal fluid (CSF) with or without leptomeningeal enhancement (LE) in magnetic resonance imaging (MRI). We collected individual patient data on cancer history, diagnosis of LM, response to LM treatment, and clinical outcomes.
Patient assessments
There is no standard response assessment for LM since it manifests as non-measurable lesions. Based on previous studies,10–12 we evaluated the response to PD-1 mAb treatment based on three outcomes: CSF cytology, MRI, and central nervous system (CNS) symptoms.
Based on the European Association of Neuro-Oncology Clinical Practice Guidelines, 13 positive cytology in the CSF was used as the main diagnostic criterion to classify patients as type I LM, corresponding to confirmed LM. In our study, after centrifugation and precipitation using the Saky method, 14 two independent experts examined CSF cells under a 40x objective: the presence of typical tumor cells indicated a positive result. After confirming positive cytology, we evaluated tumor burden based on the percentage of tumor cells in all nucleated cells: ≥ 10% indicated large quantities; 1–10%, small quantities; and < 1%, minute quantities. Next-generation sequencing (NGS) was performed to detect cell-free DNA in the supernatant or pellet of CSF samples 15 and primary tumor tissue in some patients, exploring the molecular markers that may be related to the prediction of efficacy such as tumor mutation burden(TMB) and/or microsatellite instability (MSI).
We performed MRI of the brain and the entire spinal cord for each patient, and focused on the presence of abnormal LE, ventricular enlargement (VE), and BPM. MRI was conducted with contrast enhancement at least 1.5 T field strength, 13 and all images were scanned at a thickness of ≤ 5 mm.
Before and after receiving the first PD-1 mAb treatment, we evaluated the physical status of patients based on the Eastern Cooperative Oncology Group (ECOG) Performance Status. CNS symptoms, such as headache, vomiting and dizziness, etc, were recorded. We also recorded the total number of PD-1 mAb treatment cycles after the diagnosis of LM.
Treatments
In our study, PD-1 mAbs included nivolumab and toripalimab. Nivolumab from Bristol-Myers Squibb was administered by intravenously 3 mg/kg once every 2 weeks (q2w). Toripalimab from Junshi Biosciences was administered by intravenously 240 mg once every 3 weeks (q3w). The main combination with PD-1 mAbs were chemotherapy such as cisplatin + nab-paclitaxel or cisplatin + capecitabine. Anti-angiogenesis drugs used in this study included bevacizumab and anlotinib, the former combined with chemotherapy and PD-1 mAbs, but the later combined only PD-1 mAbs. During PD-1 mAbs treatment, we use other drugs instead of hormones as much as possible to relieve intracranial hypertension symptoms.
Follow-up
The first follow-up was all carried in patients to evaluate the response to PD-1 mAb treatment within 3 months including CNS symptoms, MRI and CSF. If there was aggravation of CNS symptoms, the follow-up was assessed at any time. The final follow-up was conducted on December 30, 2020. Follow-up time was defined relative to the first PD-1 mAb treatment. OS was defined as the time from the diagnosis of LM until death due to any cause.
Results
Patient characteristics
We collected clinicopathological data from six patients (four men) who were diagnosed with LM from solids tumors and underwent first-line PD-1 mAb treatment at our hospital. They ranged in age from 45 to 63 years (Table 1). These patients suffered from a range of cancers including lung cancer, bladder cancer, gastric cancer, cholangiocarcinoma and unknown primary tumor, a majority (66.7%) experienced simultaneous extracranial metastasis and a minority (33.3%) experienced previous occurrence of BPM.
Clinicopathological characteristics of six patients diagnosed with leptomeningeal metastasis from solid tumors who received first-line programed death-1 monoclonal antibody treatment.
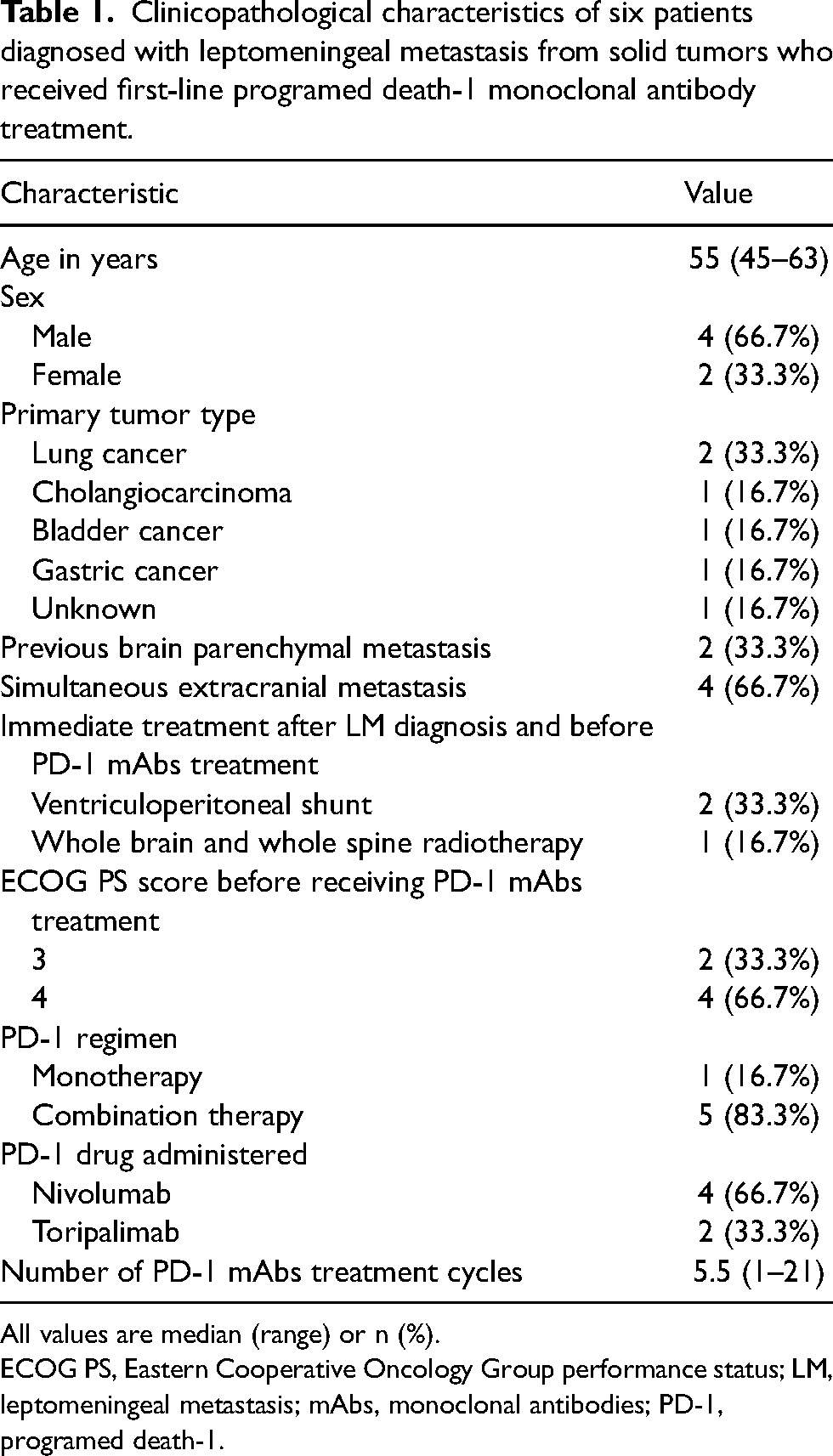
All values are median (range) or n (%).
ECOG PS, Eastern Cooperative Oncology Group performance status; LM, leptomeningeal metastasis; mAbs, monoclonal antibodies; PD-1, programed death-1.
Treatments
The median (range) number of PD-1 mAbs treatment cycles was 5.5 (1-21). In response to the LM diagnosis, all six patients accepted PD-1 mAbs as a first-line systemic pharmacotherapy. One patient received only PD-1 monotherapy due to myelosuppression after whole brain and whole spinal cord radiotherapy, while the other five received a combination of PD-1 mAbs therapy along with chemotherapy and/or anti-angiogenesis drugs. Ventriculoperitoneal (VP) shunt was used to treat hydrocephalus observed in 3 patients: this was beneficial for 2 patients who underwent before PD-1 mAb combination therapy and 1 patient who underwent after that. A detailed outline of the response to PD-1 mAb combination therapy and the outcomes of all six patients are provided in Table 2.
Individual patient response to first-line programed death-1 monoclonal antibody treatment.
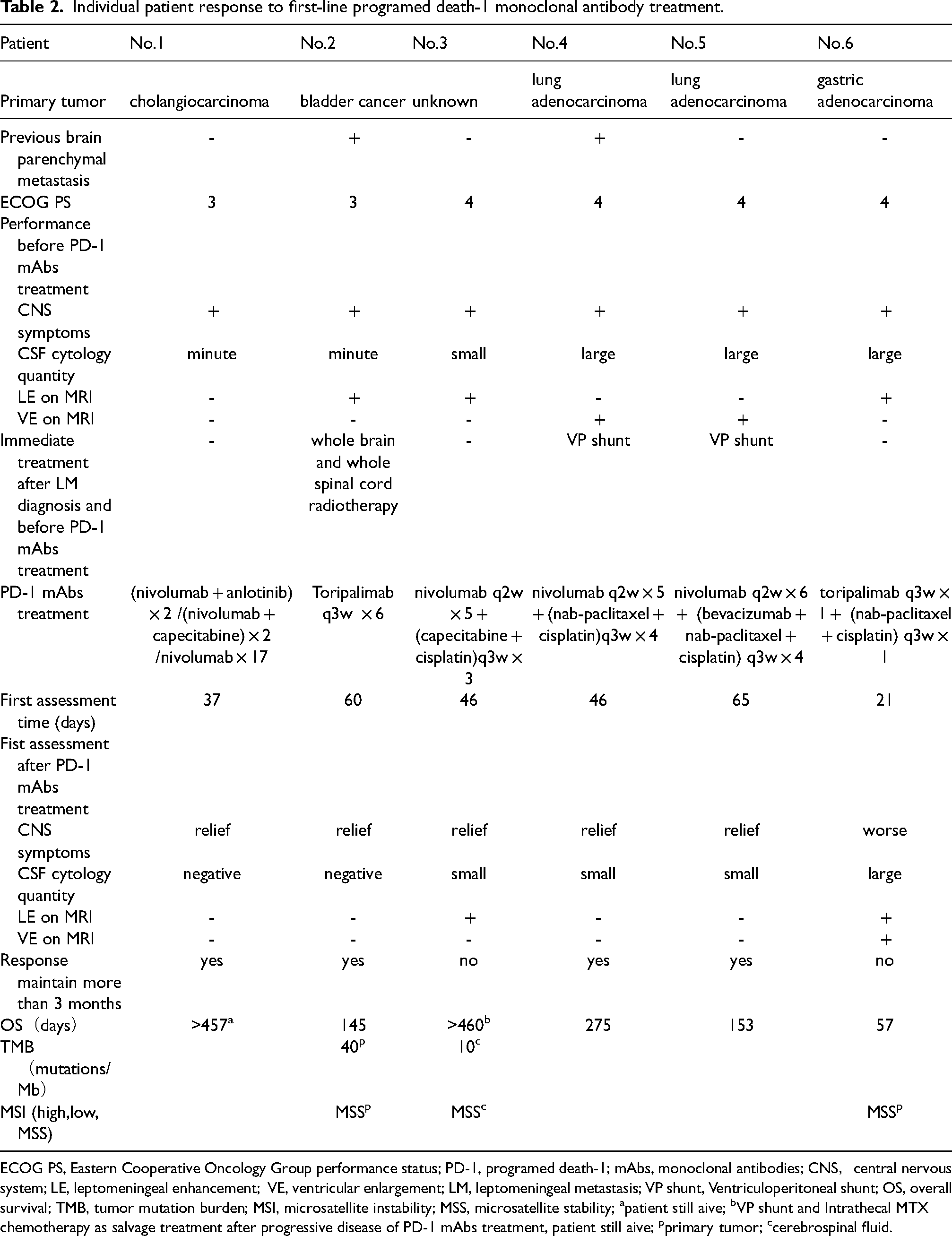
ECOG PS, Eastern Cooperative Oncology Group performance status; PD-1, programed death-1; mAbs, monoclonal antibodies; CNS,central nervous system; LE, leptomeningeal enhancement; VE, ventricular enlargement; LM, leptomeningeal metastasis; VP shunt, Ventriculoperitoneal shunt; OS, overall survival; TMB, tumor mutation burden; MSI, microsatellite instability; MSS, microsatellite stability; apatient still aive; bVP shunt and Intrathecal MTX chemotherapy as salvage treatment after progressive disease of PD-1 mAbs treatment, patient still aive; pprimary tumor; ccerebrospinal fluid.
Patient medical history and response to treatment
Patient no. 1 had undergone radical resection of a cholangiocarcinoma in 2003, about 16 years prior to this study; the tumor was originally discovered when the patient complained of feeling dizzy and walking unsteadily. Before receiving PD-1 mAb combination therapy, the patient had minute quantities of tumor cells in the CSF, no abnormalities on MRI, and an ECOG PS score of 3. The first-line treatment received by this patient was administered in two cycles and included a combination of nivolumab and anlotinib (12 mg d1-14 q3w). We conducted an assessment 37 days after treatment and found that the patient's symptoms got obvious relief and showed negative CSF cytology. Due to the occurrence of thrombocytopenia, second-line treatment included nivolumab and capecitabine (1 g/m2 d1-14 q3w), which were administered in two cycles, followed by 17 cycles of nivolumab administered as a maintenance treatment until the final follow-up. Patient no. 1 was still alive at last follow-up on December 30, 2020.
Patient no. 2 had undergone radical resection of bladder cancer in 2012, which was followed by extracranial metastasis in 2016 and an isolated BPM with total resection in 2017. About 5 months later in 2018, the patient had suffered headach and been diagnosed with new multiple BPM and LM. The patient had minute quantities of tumor cells in the CSF and LE on MRI an ECOG PS score of 3. The patient underwent whole brain and whole spinal cord radiotherapy, which leading to myelosuppression, and so that the patient had only PD-1 mAb monotherapy, receiving six cycles of first-line toripalimab. The first assessment, conducted 60 days after treatment, showed that the patient had no CNS symptoms and a negative CSF cytology; MRI scans showed no leptomeningeal abnormalities, and partial response (PR) of BPM. The OS of patient no. 2 was 145 days.
Patient no. 3 was admitted to our hospital with dizziness, and was found to have an unknown primary tumor. Before receiving PD-1 mAb combination therapy, the patient had small quantities of tumor cells in the CSF, LE on MRI, and an ECOG PS score of 4. No extracranial lesions were found in PET-CT scans, or during gastroscopy or colonoscopy. First-line treatment included 5 cycles of nivolumab and 3 cycles of capecitabine (1 g/m2 d1-14 q3w) + cisplatin (75 mg/m2 d1 q3w). The first assessment, conducted 46 days after treatment, showed that the patient's dizziness got partial relief, but there was no improvement in CSF cytology or LE on MRI. About 70 days after the diagnosis of LM, the patients experience aggravated dizziness and vomiting; MRI showed VE indicative of hydrocephalus. The patient was immediately treated and rescued with the help of VP shunt. The patient received monthly MTX (10 mg) injections intrathecally until the final follow-up on December 30, 2020. Patient no. 3 is still alive.
Patient no. 4 was diagnosed in 2016 with extracranial metastasis of a lung adenocarcinoma with exon 19 deletion mutation in the gene of epidermal growth factor receptor (EGFR); this was successively treated with six months of pemetrexed and cisplatin chemotherapy, and nine months of gefitinib. However, the patient continued to suffer from extracranial progressive disease (PD) and BPM. In 2018, EGFR T790 M mutation was detected in the extracranial tumor tissue; the patient received 10 months of osimertinib treatment with intracranial complete response (CR), followed by extracranial PD. After six months of receiving gefitinib and osimertinib, the patient began experiencing headache and vomiting and was diagnosed with LM. Before receiving PD-1 mAb combination therapy, the patient had large quantities of tumor cells with EGFR exon 19 deletion mutation in the CSF, as well as an ECOG PS score of 4. MRI showed VE indicative of hydrocephalus, but no leptomeningeal abnormality. After receiving a VP shunt, the patient underwent five cycles of nivolumab and four cycles of nab-paclitaxel (200 mg/m2 q3w) + cisplatin (60 mg/m2 q3w). The first assessment, conducted 46 days after treatment, showed that the patient got CNS symptoms obvious relief, the CSF had only small quantities of tumor cells, and MRI showed no abnormalities. The OS of patient no. 4 was 275 days.
Patient no. 5 was diagnosed in 2012 with extracranial metastasis of lung adenocarcinoma and successively received two years of pemetrexed with or without cisplatin chemotherapy as well as 8 months of icotinib, 14 months of osimertinib, and 3 months of AZD3759 treatment. The patient then experienced frequent headaches and vomiting. Before receiving PD-1 mAb combination therapy, the patient showed large quantities of tumor cells that with EGFR exon 19 deletion mutation in the CSF, an ECOG PS score of 4 and no leptomeningeal abnormalities on MRI. The patient received a VP shunt to treat hydrocephalus, which was identified based on VE observed on MRI. First-line treatment involved six cycles of nivolumab and four cycles of bevacizumab (15 mg/kg q3w) + nab-paclitaxel (260 mg/m2 q3w) + cisplatin (75 mg/m2 d1 q3w). The first assessment, conducted 65 days after treatment, showed that the patient got symptoms obvious relief, the MRI scans showed no signs of VE, and the CSF showed a reduction in the number of tumor cells. The OS of patient no. 5 was 153 days.
Patient no. 6 had undergone gastric adenocarcinoma resection in 2018, 18 months later with complaints of headache, dizziness, and seizure. Before receiving PD-1 mAb combination therapy, the patient had large quantities of tumor cells in the CSF and an ECOG PS score of 4. MRI scans showed LE. We observed no extracranial metastasis. First-line treatment included toripalimab, nab-paclitaxel (260 mg/m2 q3w) and cisplatin (75 mg/m2 q3w) administered together in one cycle. The first assessment, conducted 21 days later, showed that the headache and dizziness symptoms had worsened. Hydrocephalus was detected on MRI, but the patient rejected the VP shunt. The OS of patient no. 6 was 57 days.
Follow-up
The median (range) follow-up time across all six patients was 214 (57-460) days. No CNS related side effects were observed. During follow-up, two patients stopped receiving PD-1 mAbs treatment: patient no. 2 had to stop treatment due to the COVID-19 pandemic, while patient no. 4 had to stop because of the occurrence of arrhythmias.
By the final follow-up on December 30, 2020, one patient showed no worsening of CNS symptoms, 2 patients were still alive, and the cause of death in the other 4 patients was associated with LM.
Discussion
This study aimed to evaluate the efficacy and safety of using first-line PD-1 mAbs combination therapy for the treatment of patients with LM from solid tumors. After treatment, we found that most of the patients analyzed in our study response to PD-1 mAbs combination therapy and keep more than 3 months with the longest OS >460 days without neurotoxicity. Brastianos, PK et al. 16 has reported that pembrolizumab monotherapy is safe and displays the 3.6 months of median OS in heavily pre-treated patients with LM mostly from breast cancer. Our results show that PD-1 mAbs first-line combination therapy can also benefit patients with LM without causing additional neurotoxicity.
The gold standard for the diagnosis of LM is the presence of tumor cells in the CSF. Before receiving PD-1 treatment, all six patients included in this study had varying quantities of tumor cells in their CSF and had experienced different CNS symptoms. However, MRI showed that only 3 patients had LE, while the other 2 patients suffered from hydrocephalus due to VE without LE and the other 1 patient without abnormalities found on MRI. Therefore, the occurrence of LE on MRI lacks the sensitivity to diagnose LM. Similarly, we found no significant association between changes in LE and changes in CNS symptoms among patients who received PD-1 mAb combination therapy.
In this study, we evaluated the response to PD-1 mAb treatment based on the status of CNS symptoms, performance in MRI scans, and tumor quantities in the CSF. During the first assessments, which were conducted between 21 and 90 days after treatment according to both CNS symptoms change and the regimen, we found that it was easier to assess changes in CNS symptoms due to high intracranial pressure and meningeal irritation. Of the six patients, five got CNS symptoms obvious relief 42–90 days after PD-1 treatment. However, patient no. 6 experienced worsening CNS symptoms and the new onset of hydrocephalus 21 days after PD-1 treatment; this could be due to the high number of tumor cells observed in the CSF at the time of LM diagnosis. Our results also show that the occurrence or disappearance of VE (i.e. hydrocephalus) on MRI can act as an indirect indicator of LM progression or regression. Further, we found an inverse association between the quantity of tumor cells in the CSF and CNS symptoms: four of the five patients who got CNS symptoms obvious relief after PD-1 mAb treatment showed a clear reduction in tumor cell quantity.
CSF cytology results were also associated with disease prognosis after treatment. Among the patients included in this study, we found that patients nos. 1-3 had minute or small quantities of tumor cells in the CSF (i.e. small tumor burden), while patients nos. 4-6 had large quantities of tumor cells in the CSF (i.e. large tumor burden). This suggests that tumor quantities identified during CSF cytology can act as a surrogate marker of disease burden. Future studies should examine whether quantifying tumor cells in CSF can further refine the prediction of prognosis.17,18
One study involving NSCLC reported that the number of tumor cells in the CSF positively correlated with risk of death. 18 Large quantities of tumor cells in the CSF often caused leptomeningeal adhesions, which may help explain the hydrocephalus at the time of LM diagnosis in patients nos. 4 and 5, as well as the potential hydrocephalus observed in patient no. 6 about 3 weeks after diagnosis. Hydrocephalus in LM predicts poor prognosis: one study showed much worse median OS when hydrocephalus was not surgically treated (1.7 vs. 5.7 months). 19
Previous studies have reported that VP shunt can rapidly improve survival in 90.3% of patients with hydrocephalus caused by LM.20,21 In our study, VP shunt surgery was recommended to patients who developed hydrocephalus. Shunt before PD-1 mAb combination therapy may help explain the relatively long OS of patients no. 4 (153 days) and no. 5 (275 days), and shunt after PD-1 mAb combination therapy may have improved the survival of patient no. 3 (> 460 days). Patient no. 6, in contrast, did not accept the VP shunt and survived only 57 days. Future studies should examine the potential therapeutic benefits of combining the VP shunt and PD-1 mAb combination therapy.
In the case of patient No. 2, PD-1 mAb treatment was administered after whole-brain and whole-spinal cord radiotherapy. Although short-term benefits were obvious, there was no long-term benefit since the patient did not survive more than 145 days. Similar outcomes have been reported in patients with LM from solid tumors; the response rate of whole brain and whole spinal cord radiotherapy combined with intrathecal chemotherapy was 86.4% and the median OS was only 6.5 months. 22 Further work should explore whether PD-1 mAb can be more effective when combined with radiotherapy.
We believe that combining PD-1 mAbs with other drugs can have promising long-term benefits for patients with LM. The choice of drugs used is often determined by the primary tumor type. For example, there are no effective targeted therapies at present for bladder and gastric cancer, and lung adenocarcinomas resistant to targeted drugs for driving gene. Therefore, PD-1 mAb treatment was administered in combination with chemotherapy, after verifying that the selected drugs could easily pass through the blood-brain barrier relatively (e.g. capecitabine, platinum, taxanes). Anti-angiogenesis drugs such as bevacizumab 23 and anlotinib 24 has been reported beneficial for patients with LM, and can be considered in combination with the PD-1 treatment. Several patients in our study showed sustained efficacy (> 3 months) after receiving both PD-1 mAb and anti-angiogenesis drugs; for example, patient no. 1 survived for more than 414 days.
Patients no. 2 and no. 4 in our study had experienced BPM before LM. One might think it for granted that the damage from multiple attacks on the blood-brain barrier would facilitate the intracranial entry of drugs, but these two patients did not show clearly different outcomes from patients without BPM. The concentration of nivolumab in CSF: plasma ratios were 1:110 when given intravenously 3 mg/Kg every 2 weeks to NSCLC patients with LM. 25 Jana Portnow et al. 26 have reported that the concentrations of pembrolizumab given intravenously 200 mg every 3 weeks in CSF were approximately and steadly 1% of that in serum and those were sufficient for blocking PD-1 on T cells in the CSF of 10 patients with high-grade gliomas. The effects of PD-1 mAb can be due to a dual mechanism which are different from traditional chemetherapy drugs: the antibodies themselves can arrive the CSF and inhibit the T cells being already in CSF and they can bind T cells in peripheral blood which can subsequently go into CSF.
Additionally, we attempted to identify predictive molecular markers for the treatment of LM. NGS of patient samples detected the presence of microsatellite stable (MSS) cells in two sets of primary tumor tissues and one CSF sample. There were two cases of high tumor mutation burden (TMB): patient no. 2 with a TMB of 40 mutations/Mb in bladder cancer tissue, and patient no. 3 with a TMB of 10 mutations/Mb in the CSF. We found that patient no. 2 had a positive response to PD-1 monotherapy after radiotherapy, and the benefits lasted longer than 3 months; while patient no. 2, who received PD-1 mAbs and chemotherapy, showed a response that lasted shorter than 3 months. Future studies should examine whether NGS can help predict and explain how long treatment benefits last.
Our findings show that PD-1 mAbs can have a positive effect on the treatment of patients with LM. The combination of PD-1 mAbs with chemotheray and /or anti-angiogenesis drugs appears to be safe and well-tolerated. Therefore, PD-1 mAbs can be used as a first-line treatment for patients with LM from solid tumors. The salvage effect of the VP shunt on hydrocephalus may facilitate multiple cycles of PD-1 mAb treatment and prolong survival.
The results of our analysis must be interpreted carefully given some key limitations. Firstly, this is a retrospective study full of heterogeneity in primary tumors and combined treatment methods. Secondly, no control group such as traditional radiotherapy or intrathecal chemotherapy can be compared. Finally, there are too few cases. We fully know the shortcomings of this study. However, we still believe that this retrospective analysis of rare cases with very poor prognosis is still valuable. Inspired by this study, we will prospectively explore the efficacy of combination regimen with PD-1 mAbs for lung cancer LM patients without hydrocephalus and with small CSF tumor burden.
Footnotes
Acknowledgements
The authors thank Dr Xiaohua Liang, Xinli Zhou,Mengxi Ge, Rongrong Yao and Xiaoyu Ji for some help of treating the patient in this study. The authors thank Dr Kun Chen for the help of detection of tumor cells in cerebrospinal fluid in this study.
Funding
This study is funded by CSCO-hengrui Cancer Research Fund (Y-HR2018-026).
Conflict of interest
Zhaohui Chu declares that she has no conflict of interest Hao Lin declares that he has no conflict of interest Qiong Zhan declares that she has no conflict of interest Tao Liu declares that he has no conflict of interest Yu Wang declares that she has no conflict of interest
Author contributions
Zhaohui Chu contributed to the study conception and design. Material preparation, data collection and analysis were performed by Hao Lin, Qiong Zhan, Tao Liu and Yu Wang. The first draft of the manuscript was written by Zhaohui Chu and all authors commented on previous versions of the manuscript. All authors read and approved the final manuscript.
Ethical approval
All procedures performed in studies involving human participants were in accordance with the ethical standards of the institutional and/or national research committee and with the 1964 Helsinki declaration and its later amendments or comparable ethical standards.
Informed consent
Informed consent was obtained from all individual participants included in the study.
Data availability
All data generated or analyzed during this study are included in this article.
Conflict of interest statement
The authors have no conflicts of interest to disclose.
Ethics statement
This study was approved by the Ethics Committee of Huashan Hospital. All patients have signed informed consent.