
Abstract
Introduction
Rituximab carries a boxed warning for severe or fatal infusion reactions; most occurring with the initial infusion. Prior studies established that if the initial rituximab infusion is tolerated, subsequent infusions can be given safely over 90 min. The University of Chicago Medicine (UCM) did not have a standardized method to document infusion reactions for outpatient chemotherapy patients, making it challenging for providers to know a patients’ eligibility for rapid infusion. This quality improvement project focused on a series of interventions to improve documentation and electronic ordering of rituximab.
Methods
A flowsheet for nurses to record patients’ tolerance of chemotherapy infusions was created within the electronic health record (EHR). Following results of flowsheet impact, a second intervention was implemented to modify ordering of rituximab. The primary endpoint was the incidence of guideline concordant rate ordering of rituximab. Secondary endpoints included the incidence of accurate chair time scheduling pre- and post-interventions and nursing compliance with flowsheet documentation.
Results
Prior to flowsheet implementation, 85% of patients were infused at the guideline concordant rate, compared to 79% post-implementation. Prior to modification of rituximab ordering in the EHR, 85% of patients were infused at the guideline concordant rate, compared to 87% after implementation. Complete nursing documentation was done 89% of the time when the flowsheet was utilized, compared to 11% pre-interventions.
Conclusion
No difference in primary or secondary endpoints was found following our interventions. However, the infusion documentation flowsheet, when used, provided more complete reaction data compared to when it was not used.
Introduction
Problem description
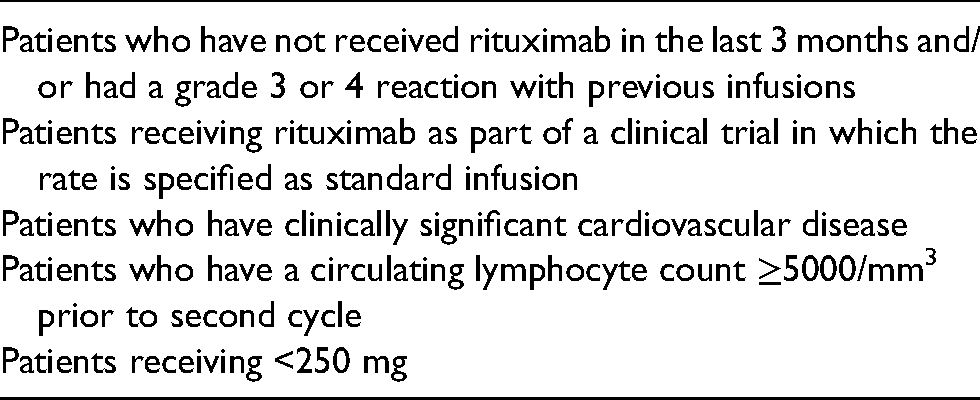
At The University of Chicago Medicine (UCM) outpatient chemotherapy infusion center, pharmacists and nurses can adjust, per protocol, the ordered rate of rituximab from standard titration to a rapid 90-min infusion for all eligible patients (see Table 1 for exclusion criteria). This however, is predicated on accurate and complete documentation of past infusion reactions. At the UCM outpatient chemotherapy infusion center there was not a standardized method for nurses to document infusion reactions. This resulted in time-consuming chart review to determine tolerance and ultimately lower than desired adoption of rapid rituximab infusions.
Exclusion criteria for rapid rituximab.
Available information
Rituximab is a chimeric human/mouse monoclonal antibody that binds to surface CD20 and is commonly used for the treatment of non-Hodgkin's lymphoma and chronic lymphocytic leukemia. 1 Rituximab, as with many biological agents, carries a risk of severe infusion reactions. Generally, reactions occur with the first infusion and are characterized as mild to moderate (Grade 1 or 2) with an incidence of ≥25%, while severe reactions (grade 3 or 4) occur less frequently with an incidence of approximately 10%. 2 Due to the risk of severe and fatal reactions with rituximab, the Food and Drug Administration issued a boxed warning for infusion-related reactions in the product labeling. While the exact mechanism of rituximab infusion reactions is unknown, the risk is highest during the first infusion and it is thought that rituximab cell-mediated lysis results in the release of inflammatory cytokines. The incidence and severity of reactions decreases significantly with each subsequent infusion. 2
Original labeling of rituximab recommended that each infusion be slowly titrated every 30 min over a total of 4–6 h to avoid infusion reactions. Per manufacturer recommendations, the initial infusion should be started at a rate of 50 mg/hr, then if tolerated, increased by 50 mg/hr every 30 min to a maximum rate of 400 mg/hr. Additionally, premedication with acetaminophen plus an antihistamine is recommended in the package insert. The slow and protocolized titration schedule is both labor and time-intensive for administering staff. Furthermore, Medicare reimbursement to institutions decreases substantially after the first hour of infusion, and long chair times constrain the number of appointments an institution can provide. 3 A shorter infusion time could reduce chair time, provide cost savings for the institution and increased patient satisfaction. According to a National Comprehensive Cancer Center infusion efficiency workgroup evaluation, data at one institution suggested infusion center chair is associated with $730 direct margin per hour. 4 Due to the challenges with long infusion times, several studies began looking at the safety of giving rituximab over a shorter period of time for patients meeting certain criteria.
The RATE trial (Rituximab Alternative Dosing Rate in Patients with Previously Untreated Diffuse Large B-Cell or Follicular Non-Hodgkin's Lymphoma) was a phase III, open-label trial that evaluated the safety of a rapid rituximab over 90 min. Investigators found that patients who had not previously experienced a grade 3 or 4 infusion reaction to their initial rituximab infusion could safely receive subsequent doses over 90 min. 5 The RATE study prompted the labeling of rituximab to include the 90-min administration time for patients without the presence of the following: grade 3 or 4 reaction to initial infusion, clinically significant cardiovascular disease, or circulating lymphocyte count ≥5000/mm4. Decreasing drug infusion times in an outpatient infusion clinic allows for significantly reduced appointment times from 6–8 h to 3 h.
Specific aim
The purpose of this quality improvement project was to complete a series of interventions to improve documentation of chemotherapy infusion tolerance, ordering, and administration rituximab. Refining these processes could impact patient safety, decrease cost, and increase patient satisfaction.
Methods
Study setting
This was a retrospective, single center, quasi-experimental quality improvement project. This project was formally determined to be quality improvement, not human subjects research, and was therefore not overseen by the Institutional Review Board, per institutional policy. Adult patients receiving rituximab intravenous infusions for an oncologic indication at UCM outpatient infusion center were included in the analysis. The infusion center located at the Hyde Park campus in Chicago, IL is equipped with 54 patient chairs and infused over 19,000 chemotherapy medications in 2019, as well as antibiotics, blood products, and intravenous fluids.
Intervention
We utilized the Plan-Do-Study-Act (PDSA) methodology which is a four step cycle that allows teams to implement a change, solve problems, and continuously improve processes. Its cyclical nature allows it to be utilized in a continuous manner for ongoing improvement. The primary outcome assessed after each PDSA cycle was the incidence of appropriate administration time of rituximab infusions pre- and post-intervention. The secondary outcomes assessed after each intervention were the incidence of accurate chair time scheduling and nursing compliance with flowsheet documentation. Encounters were identified by using a medication utilization report for patients receiving rituximab. Results were analyzed with descriptive statistics only (n, %).
PDSA 1: improving documentation of tolerance to infused rituximab
The first improvement focused on addressing reliability of infusion reaction documentation which was noted to be a barrier to assessing eligibility for a rapid infusion. To address this, a documentation flowsheet was built into the EHR for chemotherapy infusion center nurses to document after each visit (Figure 1) to improve communication between clinicians in regards to the patients’ tolerance of the infusion. If the nurse answered “yes,” to the initial question of “did the patient have a reaction,” additional questions regarding the reaction populated.
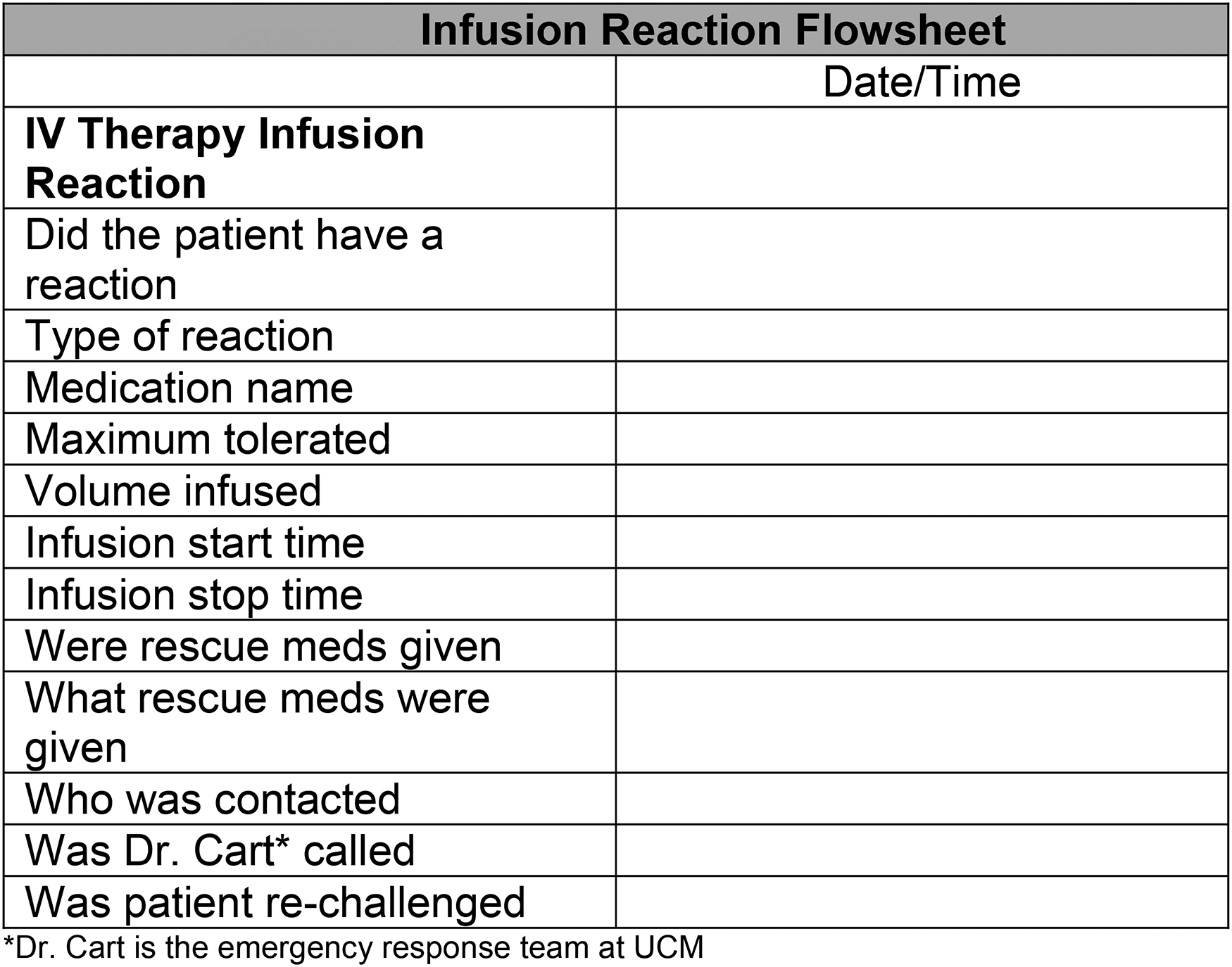
Infusion reaction flowsheet.
Plan
As part of the planning process, we reviewed the current documentation practice done by nursing in the infusion center and had a series of meetings with nursing leadership to identify opportunities for standardized work. Our group decided to move forward with incorporating a flowsheet documentation tool into the EHR.
Do
We then worked with a member of the medical informatics team to develop the infusion reaction documentation flowsheet. Infusion center nurses were sent education on how to access the flowsheet and what to document after the flowsheet was live in the EHR beginning June 2019.
Study
Data for Intervention 1 was collected between January 2019 and October 2019 to assess outcomes pre- and post-implementation. This ten-month collection period allowed for baseline data to be collected and analyzed five months prior to and five months after the flowsheet was implemented. Data collected included: chemotherapy regimen, indication, chemotherapy cycle, rituximab use within the past 3 months, patients’ eligibility for rapid infusion, if the infusion was ordered/administered at the guideline concordant rate, nursing utilization of the flowsheet documentation, and accurateness of chair time scheduling.
Act
Data analysis was then completed and a second process improvement was identified.
PDSA 2: identifying eligible patients at time of order entry
Plan
After analyzing results from Intervention 1, we found that the majority of patients eligible for rapid infusion that did not receive a rapid infusion were patients with relapsed disease who had restarted a rituximab-containing regimen within 3 months (n = 42). These patients would have been eligible for rapid infusion, however, since the new treatment was considered “Cycle 1 Day 1,” the standard infusion was administered per the rapid rituximab exclusion criteria. Also, patients were being excluded for cardiovascular disease that was not part of the exclusion criteria from the RATE study (IE: hypertension, atrial fibrillation, etc). We held meetings with the lymphoma providers to go over the results from PDSA 1 and presented our recommendations to change the order questions in the EHR, to which the group approved.
Do
To more reliably comply with the literature and exclusion criteria determined from prior studies, the order questions embedded in the rituximab electronic record were revised. The purpose of the order questions is to guide the provider to order the guideline concordant infusion rate; either standard or rapid. However, the original order questions did not address if the patient had received rituximab in the past 3 months, the severity of cardiac disease, or other specifics needed for exclusion as previously outlined in the literature. Order questions were updated and live in the EHR beginning September 2020 (Figure 2), with the goal to increase appropriate infusion rate ordering.
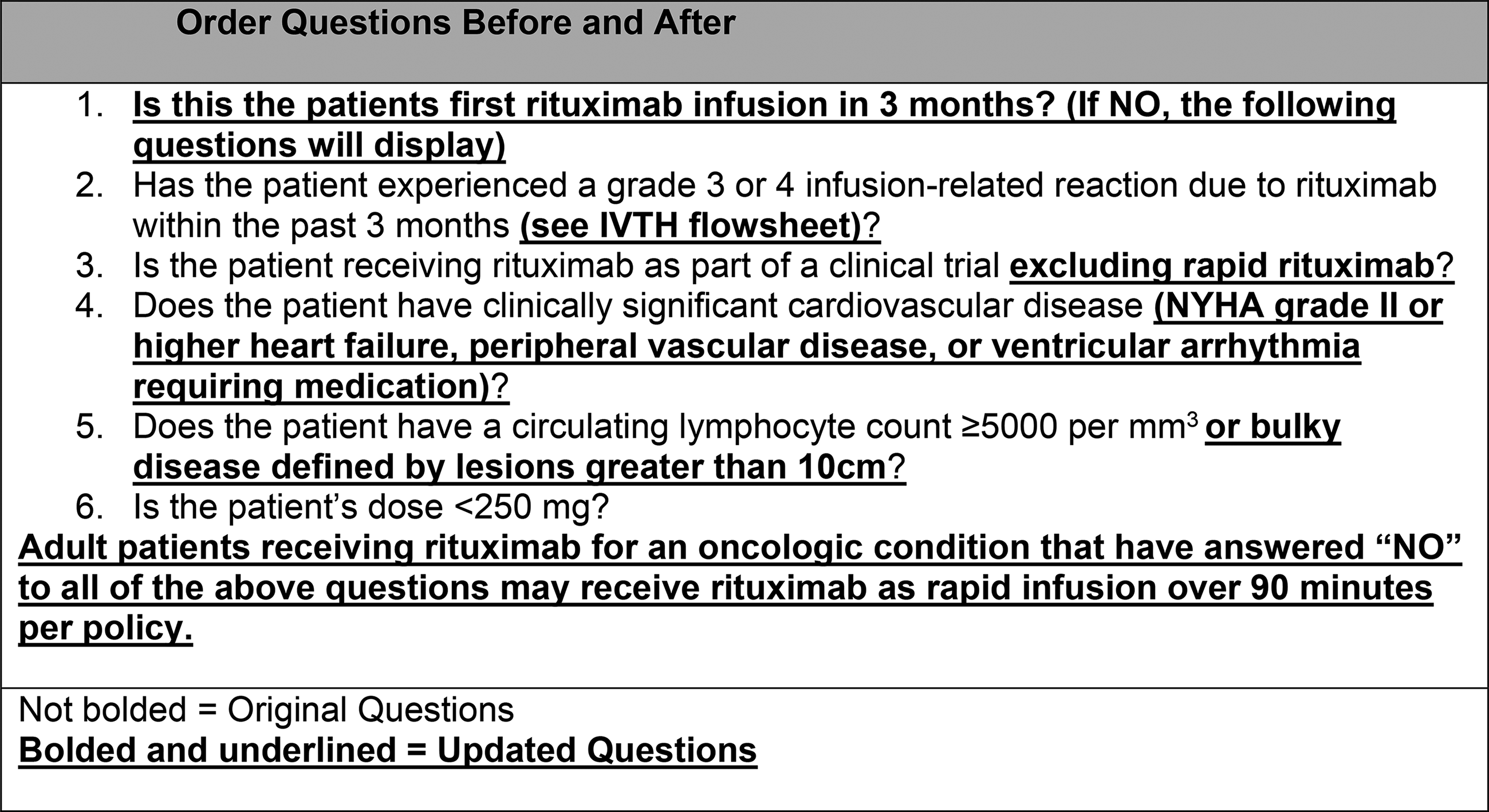
Order questions before and after.
Study
Data for Intervention 2 was collected from August 2020 through October 2020 and included: chemotherapy regimen, indication, chemotherapy cycle, rituximab use within the past 3 months, patients’ eligibility for rapid infusion, if the infusion was ordered and administered at the appropriate rate, nursing adherence to flowsheet documentation, and accurateness of chair time scheduling. A convenience sample, data from one month before, the month of, and one month after the intervention was implemented, was determined to be sufficient based on the number of rituximab orders administered. We determined the amount of data collected from this study period allowed enough time for us to understand how the order questions were being used by the ordering providers.
Act
After analyzing the data, we made rounds in the infusion center and provided nursing education on the interventions and updates made to the rituximab orders and policy.
Results
A total of 411 rituximab infusions were analyzed, which were associated with 149 unique patients. The majority of patients received rituximab for NHL (91%) with the remainder being treated for an oncologic condition other than NHL. A variety of rituximab-containing regimens were observed, with rituximab monotherapy being the most common. Patient characteristics are outlined in Table 2.
Patient characteristics.
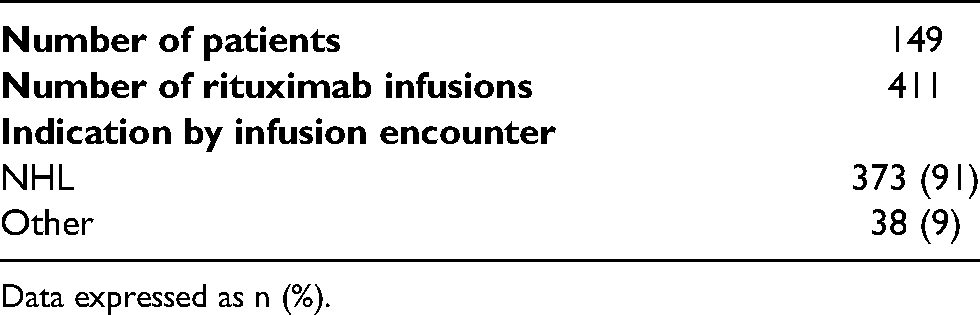
Data expressed as n (%).
Flowsheet documentation
The implementation of the infusion reaction documentation flowsheet did not affect our primary and secondary outcomes as we predicted (Table 3). Pre-implementation, 85% of rituximab infusions were infused at the guideline concordant rate, compared to 79% post-intervention. Pre-implementation chair time was scheduled appropriately 38% of the time, and 41% post-implementation. After the flowsheet went live, nurses appropriately documented infusion tolerance for 48% of rituximab infusion encounters. We found that the majority of patients that were eligible for rapid infusion but did not receive as rapid infusion were those with relapsed disease and restarted on another rituximab-containing regimen within 3 months (n = 42). Since new treatment was considered “Cycle 1 Day 1” in the patients’ treatment plan, the standard infusion was administered per our rituximab order questions guidance and infusion policy, which states that Cycle 1 should be given per standard titration and not as rapid. This finding prompted the second intervention of updating the eligibility criteria within the rituximab electronic order.
Results: intervention 1.
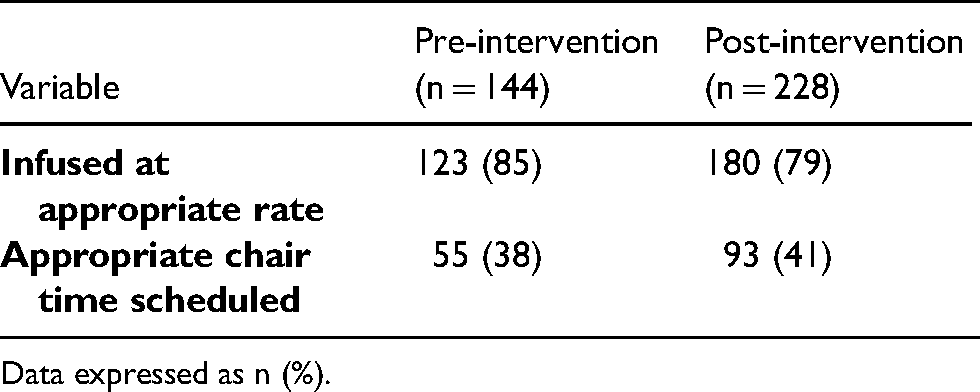
Data expressed as n (%).
Identifying eligible patients at time of order entry
The updated order questions in the rituximab electronic did not increase the incidence of our primary or secondary outcomes (Table 4). Pre-implementation, 85% of rituximab infusions were infused at the guideline concordant rate, compared to 87% post-intervention. Pre-implementation chair time was scheduled appropriately 49% of the time, and 36% post-implementation.
Results: intervention 2.
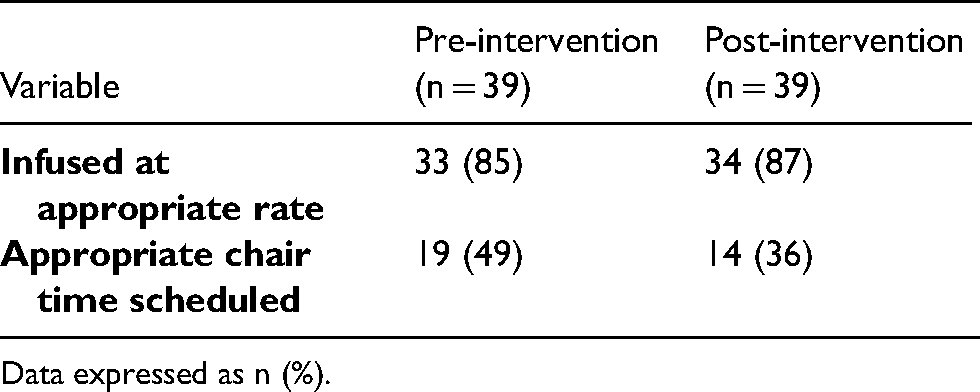
Data expressed as n (%).
Reaction documentation
A total of 27 reactions were observed over the course of the study period. Complete documentation of the reaction was defined by: reaction that occurred, dose that was administered at the time of the reaction, total volume infused, infusion start and stop time, rescue medications given, and if the patient was re-challenged was done 89% of the time when the flowsheet was utilized, compared to 11% when the flowsheet was not used and nurses only documented in the patient encounter notes.
Discussion
Summary
This was a quality improvement project which sought to first improve and standardize nursing documentation of patient tolerance to infused chemotherapy agents in an outpatient infusion center to determine if more reliable documentation would increase guideline concordant rate ordering of rituximab. Based on the findings from the first intervention, we updated the questions within the rituximab electronic order to better guide the practitioners towards the guideline concordant rate at the time of order entry. We found that the addition of the flowsheet template into the EHR (Intervention 1) did not increase the guideline concordant rate ordering as expected; appropriate chair time scheduling increased modestly. After the order questions were updated (Intervention 2), we found the guideline concordant rate ordering increased slightly, whereas appropriate chair time scheduling decreased. The minimal changes found pre- and post-interventions were likely due to factors other than the interventions themselves. Additional staff training to identify and address practice gaps should be considered.
Comparison with available literature
Several studies have explored and demonstrated the safety of maintenance rituximab infusions given as a rapid 90-min infusion for patients at low risk of developing severe reactions.3,4,6 Previous publications have focused on pharmacy-driven protocols to convert eligible patients to rapid rituximab infusions and have shown that this is safe and is an opportunity to be financially beneficial for the institution.7,8 Our project aimed to focus on the implementation of electronic interventions to provide oncology physicians, nurses, and pharmacists with the most reliable and accurate information regarding the patients’ tolerance to infused chemotherapy with the additional goal of increasing guideline concordant rate ordering of rituximab. To our knowledge, this is the first quality improvement project to describe such a process of utilizing functions within the EHR.
Limitations
Limitations to our project include, lack of control of accurate documentation, inability to correlate cost-savings with chair time, and inability to make flowsheet completion by nursing mandatory before closing the patients visit encounter.
Conclusion
Additional nursing, physician, and pharmacist education is needed to increase compliance of ordering the most appropriate rituximab infusion rate and scheduling of chair time. Despite the absence of notable improvement in guideline concordant ordering or rituximab infusion rates and appropriate scheduling of chair time, the infusion documentation flowsheet did result in more complete documentation of patient infusion reactions and outcomes, which is valuable information for pharmacists and ordering providers.
Footnotes
Ethical approval
This project was formally determined to be quality improvement, not human subjects research by The University of Chicago Medicine.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.