
Abstract
Introduction
Immune-related hepatitis is an adverse effect following treatment with immune-checkpoint inhibitors, such as ipilimumab, nivolumab and pembrolizumab. International guidelines advise on the use of corticosteroids as first-line treatment, although guidance on how to treat cases resistant to corticosteroids is limited. We aimed to evaluate the presentation and management of patients with grade 3-4 immune-related hepatitis, following treatment with immune-checkpoint inhibitors for stage 4 or unresectable or stage 3 melanoma, with a particular focus on steroid-refractory cases.
Methods
A retrospective observational review of patients developing immune-related hepatitis whilst undergoing treatment with immune checkpoint inhibitors for advanced melanoma from July 2014 to February 2020 at a tertiary oncology centre.
Results
Forty-one patients developed immune-related hepatitis, of which 83% had been treated with the combination of ipilimumab and nivolumab. The median time to onset of IR-hepatitis was 47 days (range: 4–476), and the median time to peak alanine aminotransferase was 71 days (range: 4–478). Four patients had resolution of grade 3 immune-related hepatitis without the introduction of corticosteroids. A total of 37 patients were treated with corticosteroids. A total of 12 required oral treatment only and 13 were successfully managed as outpatients. Six patients had steroid-refractory immune-related hepatitis; and all received tacrolimus, with one also receiving mycophenolate mofetil and infliximab.
Conclusions
This study describes the largest UK series of immune-related hepatitis patients in the literature. We present two important deviations from current guidelines. Firstly, there is some evidence that withholding steroids is possible in grade 3-4 immune-related hepatitis. Secondly, tacrolimus can be used successfully to manage patients resistant to corticosteroids, with the early introduction most beneficial to reduce time on steroids.
Keywords
Introduction
The introduction of immune checkpoint inhibitors (ICIs) has improved survival in a wide range of tumour types, with a particularly significant impact on the management of advanced melanoma. 1
Ipilimumab, a cytotoxic T-lymphocyte-associated antigen 4 inhibitor, was the first ICI used in clinical practice to demonstrate improved survival in melanoma.2,3 Following this, the anti-programmed death-1 receptor (PD-1) inhibitors pembrolizumab and nivolumab, both showed superior outcomes when compared to single-agent ipilimumab.4,5 The Checkmate 067 trial demonstrated a three-year survival with single-agent nivolumab of 52%, 6 and follow-up data from the Keynote 006 trial revealed 50% of patients treated with pembrolizumab to still be alive at 33 months. 7 Outcomes for patients have been further enhanced by combining these different classes of ICI; long-term follow-up data of the Checkmate 067 trial demonstrated 6.5-year survival rates of 57% for patients who received the combination of nivolumab and ipilimumab compared to 43% of in the nivolumab alone group. 8
ICIs exert their anticancer effect by disrupting the negative interactions that occur between T-cells and tumour tissue, resulting in increased T-cell activity at the tumour site. 9 This removal of the negative homeostatic control of T-cell function can result in on-target off-tumour effects or immune-related adverse events (IRAEs). These are unique to immunotherapy and present a challenge in terms of clinical management. There is now a developing literature base on the management of these IRAEs.10,11
Immune-related hepatitis (IR-hepatitis) is clinically significant toxicity that can develop after treatment with ICIs, 12 with the incidence in key trials ranging from 2% to 4% with single agents, to 18% with combination treatment, (1–2% and 8% grade 3-4, respectively).4,5 Comparable rates have been reported in retrospective real-world studies, as well as meta-analyses of trial data.13–18 CTCAE version 5 criteria for IR-hepatitis are described in Table 1.
Common terminology criteria for adverse events (CTCAE), for hepatitis version 5. 19

AST: aspartame aminotransferase; ALT: alanine aminotransferase; ULN: upper limit of normal; T-bil: total bilirubin.
Management of IR-hepatitis is outlined by the American Society of Clinical Oncology (ASCO), 20 and European Society of Medical Oncology (ESMO) guidelines, 21 with corticosteroids being the mainstay of treatment; Table 2.
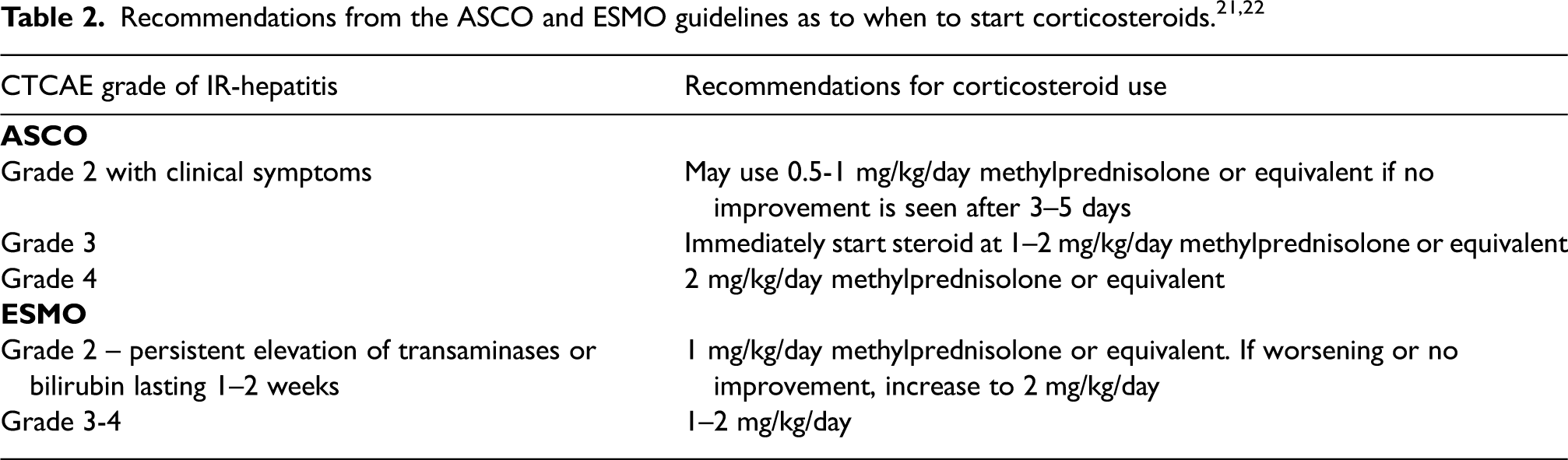
However, there are a number of unanswered questions surrounding the management of IR-hepatitis, including specific guidance on the use of alternative immunosuppression when patients are refractory to corticosteroid treatment.
The ESMO guideline proposes the use of the immunosuppressant mycophenolate mofetil as a second-line agent and suggests tacrolimus may be used the third line. 22 In comparison the ASCO guideline recommends the use of mycophenolate mofetil or azathioprine in patients with grade 3 IR-hepatitis that is steroid refractory. 21 Tacrolimus may be a more attractive option, given its faster onset of action and the fact it targets CD8 positive T-cells which have been implicated in the pathogenesis of IR-hepatitis. 22
In this study, we present our experience with a large cohort of advanced melanoma patients who developed grade 3-4 IR-hepatitis. We review and critically evaluate their pharmacological management, including the use of tacrolimus as the immunosuppressant of choice in steroid-refractory patients, and we review and discuss the current management guidelines for IR hepatitis, particularly in steroid-refractory cases.
Methods
An in-house Microsoft Access database was accessed to select patients for this retrospective observational analysis. Inclusion criteria included patients with a diagnosis of stage 4 or unresectable stage 3 metastatic melanoma who had received at least 1 cycle of ICI and were documented as developing subsequent grade 3-4 IR-hepatitis by CTCAE version 5, between July 2014 and February 2020. Electronic patient records and prescribing systems were accessed to collect relevant data, including baseline demographics, details of ICI exposure, and presentation of IR-hepatitis, as well as management and treatment pathways, with specific details on pharmacological management. The liver function tests collected included alanine transferase and bilirubin as the standard of care, and a diagnosis of grade 3-4 hepatitis was made using these results and CTCAE criteria version 5. In patients where grade 3-4 IR-hepatitis developed a wider panel including autoantibodies and a viral screen was also performed. This study was registered with the institution audit panel (CARMS-17197).
Results
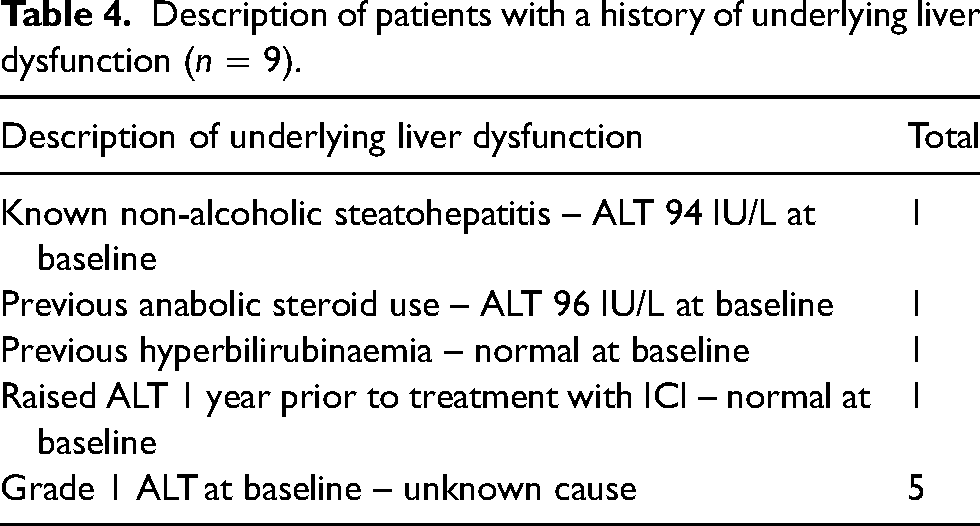
We found 41 patients who developed grade 3-4 IR-hepatitis after treatment with ICIs for advanced melanoma, between July 2014 and February 2020. A total of 56% of the study population were male, with the median age at the start of treatment 55 years (range: 32–81 years). Thirty-nine patients had stage 4 disease and two unresectable stage III. Nine patients (22%) had a history of liver dysfunction prior to ICI initiation; six had a history of raised ALT and one with raised bilirubin – all with unknown cause. In addition, one patient had a history of non-alcoholic steatohepatitis (NASH) and one of previous anabolic steroid use which was documented as a possible reason for raised ALT. Seven patients (12%) had a history of autoimmune disease which included ulcerative colitis, type 1 diabetes mellitus, hypothyroidism, myasthenia gravis, psoriasis, a previous episode of Guillian-Barre and PHEWS (persistent hypereosinophilia with Wells syndrome). A total of 83% of the patient received combination ICIs, and 17% received single agents. Baseline demographics are given in Tables 3 and 4, and treatment schedules are shown in Figure 1. Dosing for all the drugs was as per the Summary of Product Characteristics for these agents.23–25
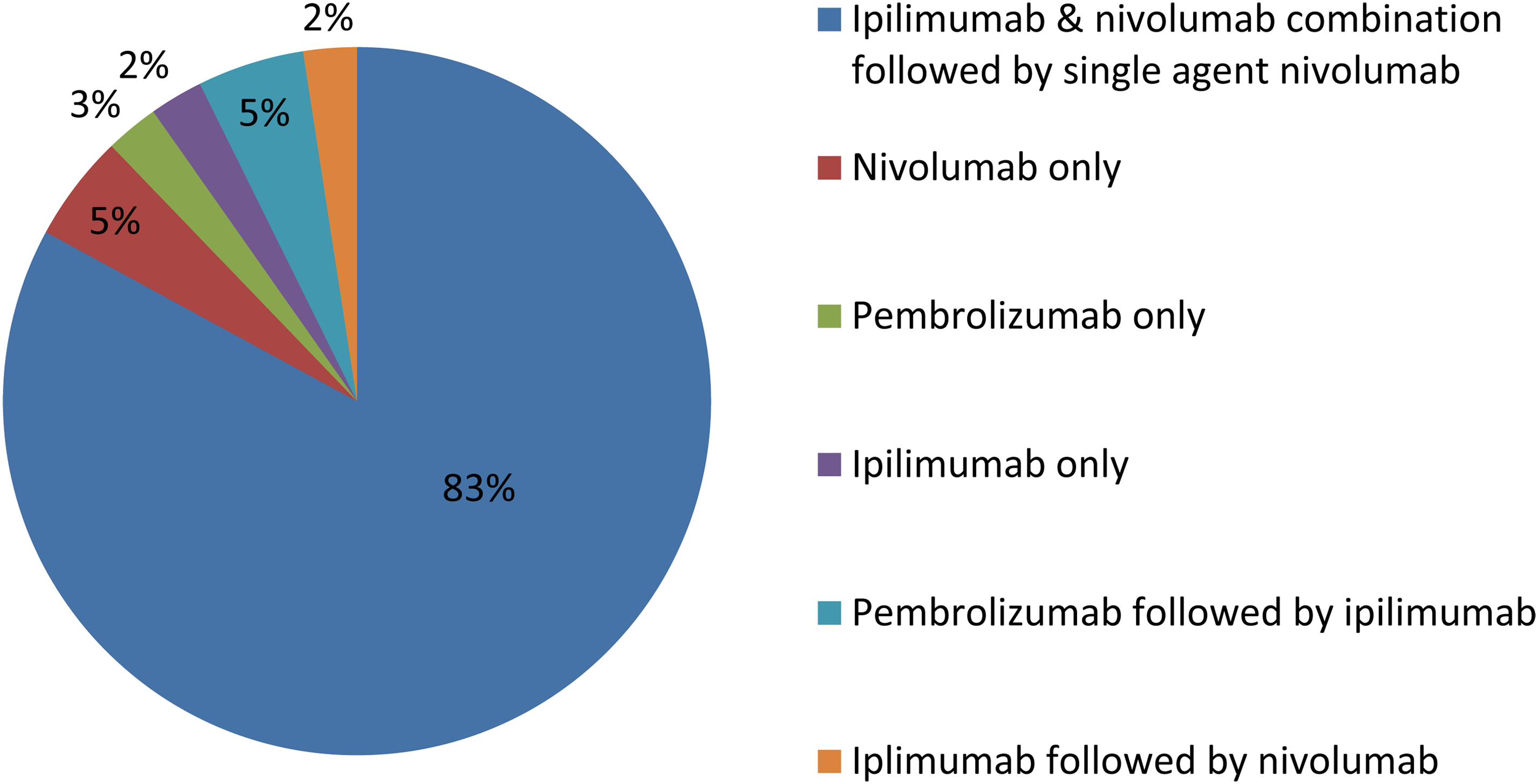
ICI regimens received by patients who developed subsequent grade 3-4 IR-hepatitis (n = 41).
Baseline demographics of all patients developing grade 3-4 IR hepatitis.
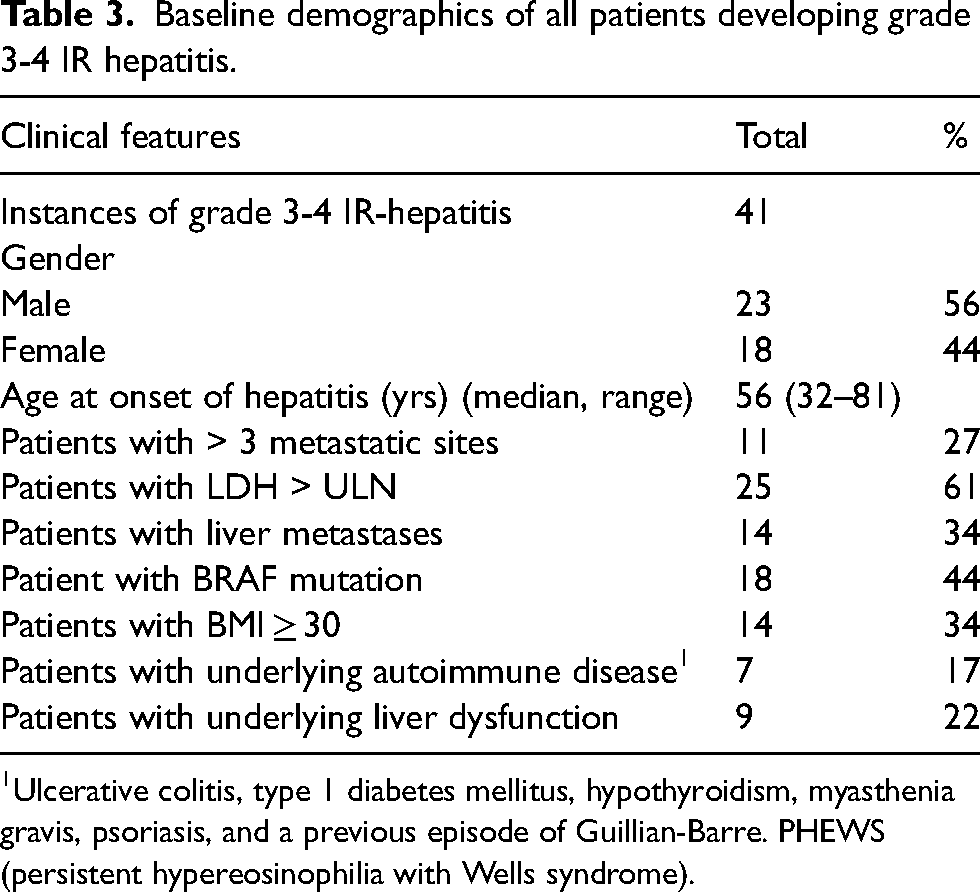
Ulcerative colitis, type 1 diabetes mellitus, hypothyroidism, myasthenia gravis, psoriasis, and a previous episode of Guillian-Barre. PHEWS (persistent hypereosinophilia with Wells syndrome).
Description of patients with a history of underlying liver dysfunction (n = 9).
Presentation of IR-hepatitis
The median time to onset of a rise in ALT of ≥ grade 1 after ICI was initiated was 47 days (range: 4–476), with a median time to peak ALT of 71 days (range: 4–478). A total of 28 (68%) patients were admitted to the hospital for management of IR-hepatitis, and 13 (32%) were managed as outpatients.
Management of IR-hepatitis
A total of 37 (37/41, 90%) were treated with corticosteroids, of which 25 (68%) required intravenous treatment, and 12 (32%) were managed with oral corticosteroids alone. Six patients (16%) required escalation to alternative immunosuppression. These six patients all received tacrolimus. One initially received mycophenolate mofetil and infliximab before being switched to tacrolimus. Treatment pathways are outlined in Figure 2, and details of the response to treatment and time to resolution for IR-hepatitis for different treatment modalities within this pathway are given in Table 5.
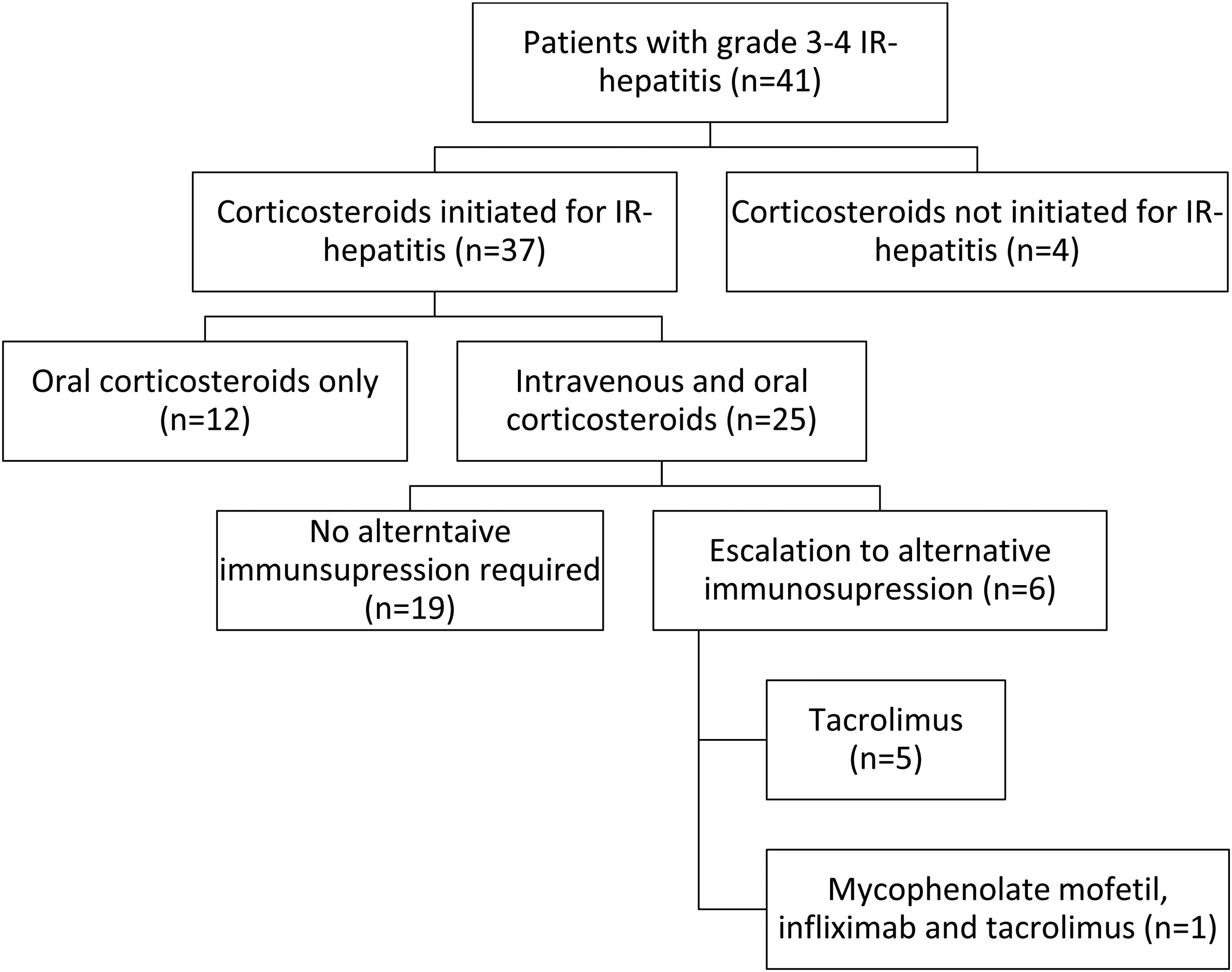
Use of systemic treatment to treat grade 3-4 immune-related hepatitis.
Response to treatment and time (in days) to resolution for IR-hepatitis for each treatment group.
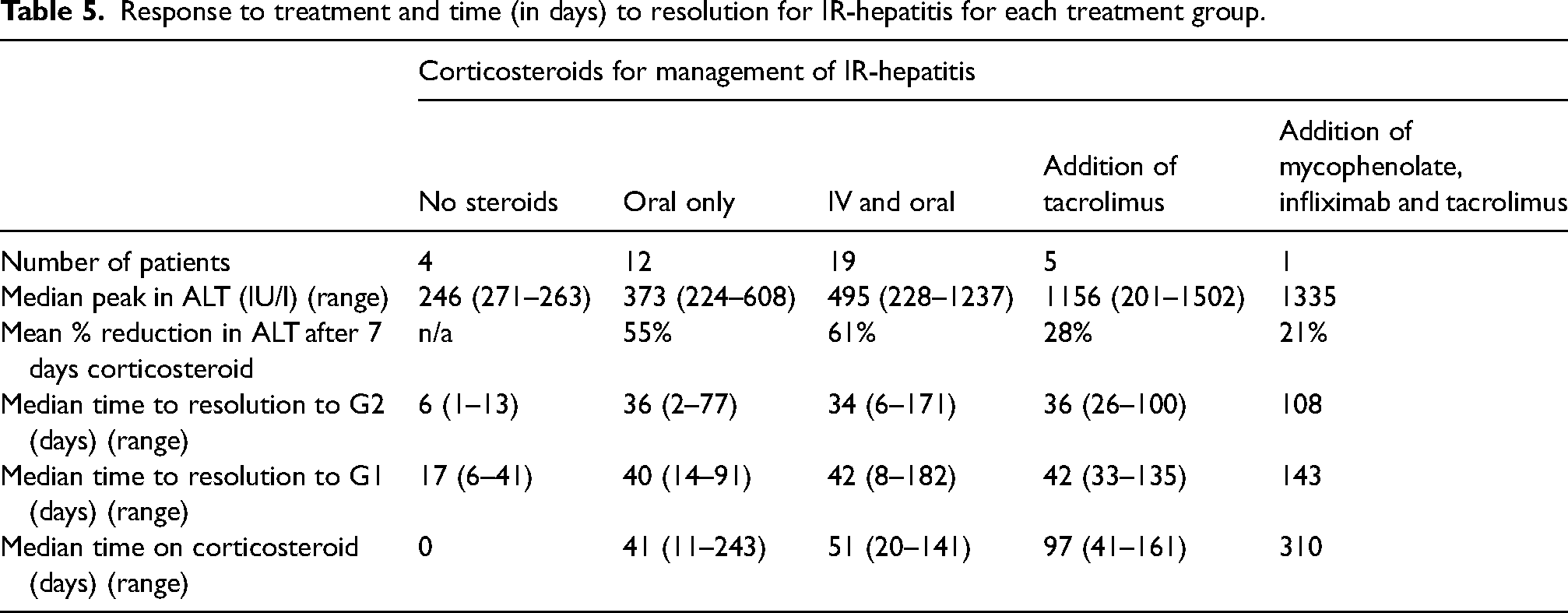
The median time to resolution to grade 2 ALT was 36 days (range: 2–171) and to grade 1 ALT was 41 days (range: 6–182).
Four patients had IR-hepatitis managed without corticosteroids. ALT returned to grade 1 for all four patients within 6 weeks. They had LFTs monitored twice weekly, and had no intervention aside from pausing ICI treatment.
A total of 37 patients were treated with corticosteroids with a median duration of corticosteroid treatment of 51 days (11–310). In these patients, methylprednisolone was used for the patients treated with IV corticosteroids, and prednisolone was used for the patients given oral corticosteroids.
Of the 12 patients who were managed with only oral prednisolone, 10 were started at 1 mg/kg/day, with two managed with a flat dose of 40 mg. All these patients responded well to treatment; they had a lower peak ALT to start with and responded to oral treatment alone. Ten of these patients returned to grade 2 ALT after seven days’ treatment, and although the other two were officially still grade 3 after 7 days, their ALT was under 300 IU/L and continued to fall. Given these patients had a good response, it follows that they had a shorter duration on corticosteroids. Ten patients were reduced to 10 mg of prednisolone or less over 6 weeks. Only two spent a prolonged time on steroids; one patient due to a persistent grade 1 ALT and one due to underlying NASH and it was felt a slow steroid wean was required to avoid recurrence of IR-hepatitis. None of these patients had a recurrence of IR-hepatitis after stopping treatment.
The 25 patients treated with IV methylprednisolone were started at 1 mg/kg/day. Three of these patients were escalated to 2 mg/kg/day. One of these had escalation within 2 days of treatment with 1 mg/kg day as ALT was >1000 IU/l, whereas the other two were escalated only after an unsuccessful switch to oral prednisolone. The fourth patient received a pulse dose of 500 mg IV methylprednisolone. These four patients also required the addition of alternative immunosuppression.
The median peak in ALT was higher for patients who were treated with IV steroids. However, the median time to resolution to grade 2 (34 days) and then grade 1 ALT (42 days) was comparable to the group of patients who received oral-only treatment, although the median total duration of steroids was longer.
Tacrolimus use in IR-hepatitis
There were six patients in total who were refractory to corticosteroids treatment and required the addition of alternative immunosuppression. Five of those were treated with tacrolimus and a sixth patient was treated with tacrolimus, mycophenolate and infliximab.
Patient TAC_1
Patient TAC_1 had an atypical IR-hepatitis in that the ALP was also elevated (a cholestatic picture of liver dysfunction) and the ALT persisted at grade 2 despite steroids. Liver biopsy supported IR-hepatitis as the underlying cause. Tacrolimus in combination with ursodeoxycholic acid resolved the elevated ALP and ALT and allowed steroids to be weaned.
Patient TAC_6
Patient TAC_6 had a life-threatening drug-induced liver injury. There was no response to 2 mg/kg of IV methylprednisolone and neutropenia occurred following the addition of mycophenolate mofetil, which then prompted treatment with infliximab and subsequently tacrolimus. This case has been reported in the literature as a severe case of IR-hepatitis that was refractory to steroids and was the first successful and safe use of infliximab as a rescue therapy. 26
Patients TAC_2, TAC_3, TAC_4 & TAC_5
Clinical data of the other four patients who received tacrolimus are given in Table 6. All these patients responded to tacrolimus allowing their corticosteroids to be weaned. However, examining these in more detail showed differences in patient management. Patient TAC_5 was treated with steroids for 45 days before the decision was made to escalate to tacrolimus. In contrast, the other three patients had tacrolimus initiated earlier at 9, 9 and 23 days, respectively. This delay in initiating tacrolimus may have been the reason TAC_5 remained on steroids for the longest out of this small group of patients. Tacrolimus in this small group of patients was initiated at a dose of 3–4 mg orally daily. As ALT normalised steroids where withdrawn prior to the withdrawal of tacrolimus.
Clinical data for four patients treated with tacrolimus.
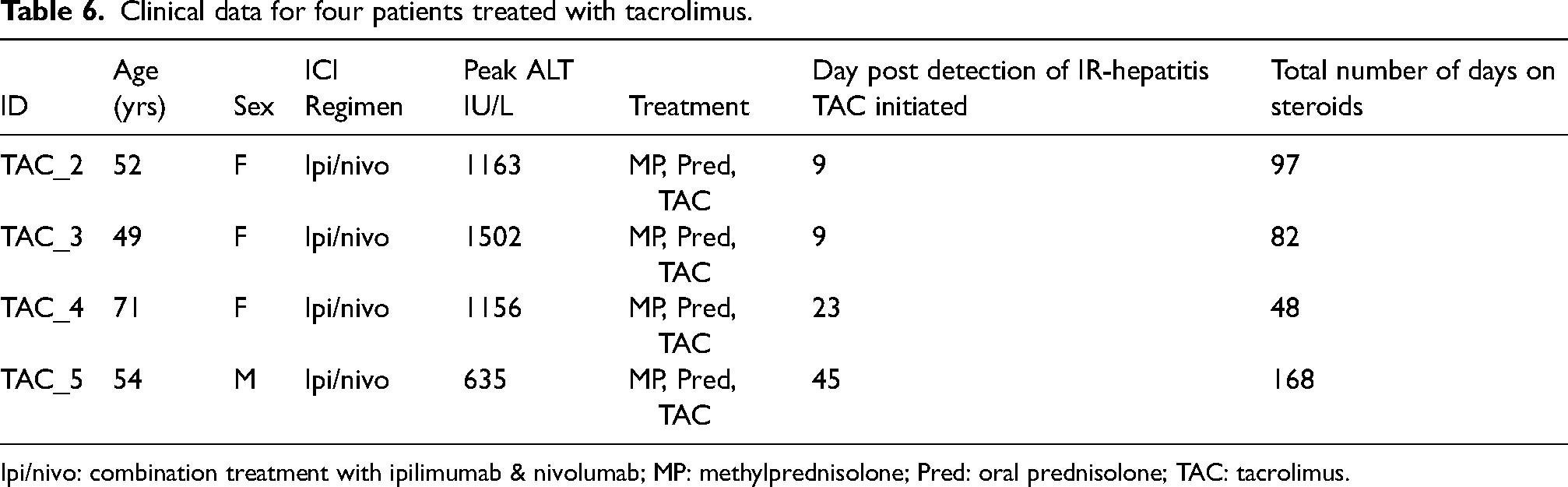
Ipi/nivo: combination treatment with ipilimumab & nivolumab; MP: methylprednisolone; Pred: oral prednisolone; TAC: tacrolimus.
Discussion
IR-hepatitis is a rare but clinically significant adverse event that can result following treatment with checkpoint inhibitors. 12 In this study, we describe the management of a series of patients who presented with grade 3-4 IR-hepatitis after treatment with ICIs for advanced melanoma.
The median time to onset of IR-hepatitis of 47 days coincides with cycles 3 to 4 of combination ICI treatment, although the wide range in the onset of four to 476 days, is a reminder that IRAEs can occur for many months to years after the initiation of treatment. 27 Peak ALT occurred at approximately 3 weeks after median onset. This suggests that particularly close monitoring of ALT is required in the 2–3 weeks after a rise in ALT is detected, and a pathway for this in clinical practice should be established.
A total of 13 patients were successfully managed as outpatients, despite needing high-dose steroids and frequent monitoring. This illustrates that safe, intensive monitoring and management does not require inpatient admission. Establishing outpatient management as a formal pathway is beneficial to patients’ quality of life and also preserves hospital inpatient resources.
Corticosteroids were the mainstay of treatment in this study. This is in line with ASCO and ESMO guidelines.
Duration of treatment and weaning schedules are not specified by ASCO or ESMO.21,22 Acknowledging the small sample size, this study suggests that patients who respond well to oral treatment should have their corticosteroid weaned to stop over 6 weeks.
The four patients who did not receive corticosteroids were clinically well and had a peak ALT at the lower end of grade 3. It was noteworthy that all had a return to grade 1 ALT within 6 weeks. If the ASCO guidelines had been followed, these four patients would have been treated with 1–2 mg/kg methylprednisolone or equivalent. 21 A management approach without the use of corticosteroids is attractive in advanced melanoma as it avoids exposure of patients to these high-risk medications. In addition, there has been concern that the use of corticosteroids has a detrimental effect on the efficacy of ICIs. 28
This small group of patients provides some evidence that “watch and wait” may be appropriate for patients with a grade 3 ALT rise at the lower end of the range. This approach is supported by both De Martin et al. 13 and Gauci et al., 29 and challenges the ASCO and ESMO guidelines in relation to the universal need for corticosteroids. De Martin et al. 13 report a benign course of ≥ grade 3 IR-hepatitis in 16 patients treated with ICIs, with six of them demonstrating a spontaneous improvement in liver function without receiving any corticosteroids, and this is corroborated by Gauci et al. 30 De Martin et al. propose an algorithm for delaying the introduction of corticosteroids through the use of close monitoring of LFTs, biopsy, and introducing steroids only if there is no improvement after 7 days. 30 It is acknowledged that none of the four patients in this study who were managed without steroids, proceeded to biopsy. This would obviously have implications for an outpatient approach.
In contrast to the four patients treated without steroids, six patients in our cohort had steroid-refractory IR-hepatitis and were treated with tacrolimus. Importantly, this is a group whose management is not well defined by current ASCO or ESMO guidelines.21,22
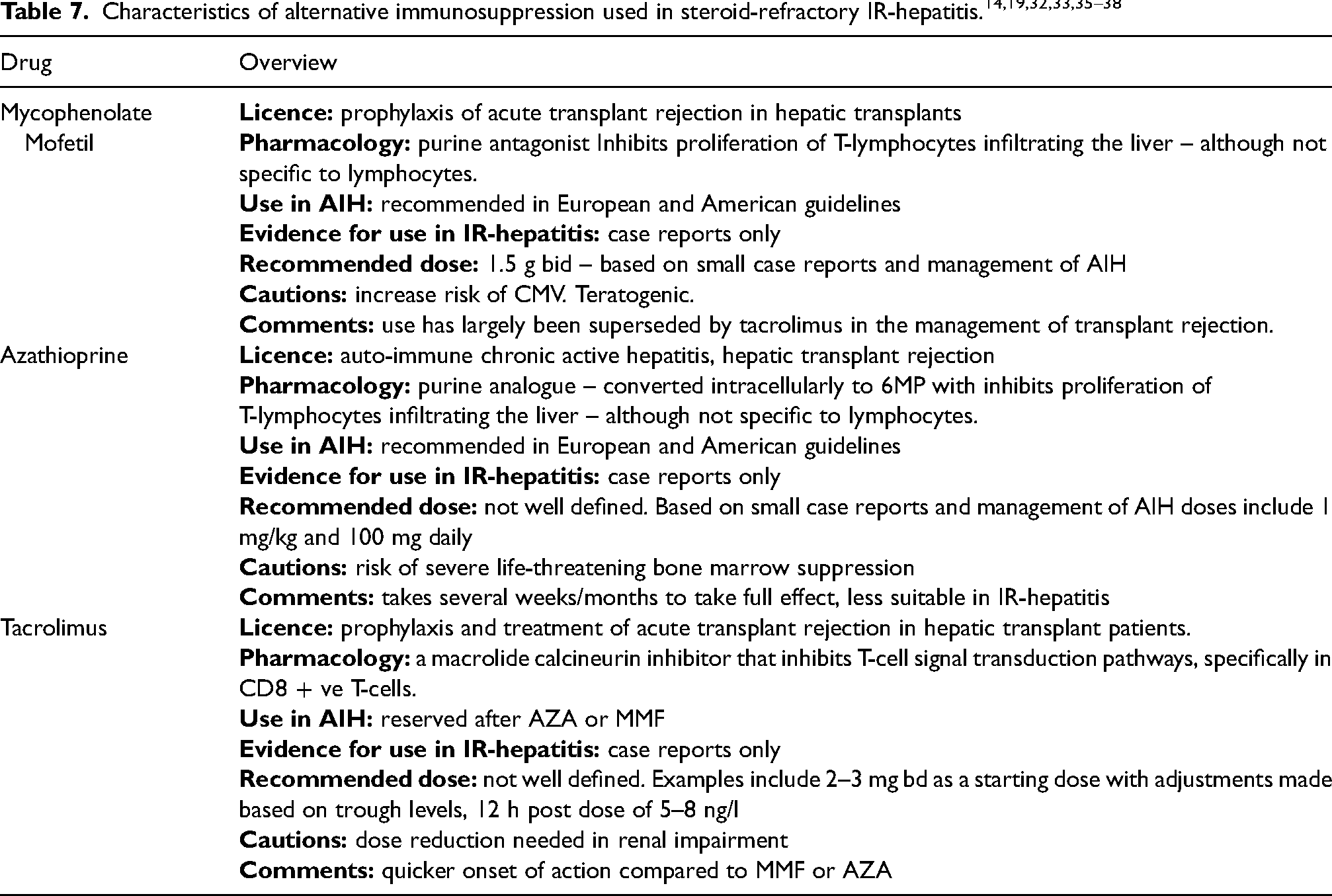
Parallels are commonly drawn to the management of autoimmune hepatitis (AIH), where mycophenolate mofetil and azathioprine are first-line agents.31,32 The limited evidence base for use of these agents in IR-hepatitis has been summarised by Ziogas et al. 33 and is more comprehensive for mycophenolate compared to azathioprine or tacrolimus. In the algorithm proposed by Ziogas et al., mycophenolate and azathioprine are suggested as treatment options prior to the introduction of tacrolimus. A recent multicentre study reported on the use of mycophenolate in all 37 patients who required an alternative immunosuppressant, whereas tacrolimus was only used in four patients as a second-line agent. 16 This is in contrast to our study where all patients requiring alternative immunosuppression received tacrolimus.
Tacrolimus is the newest of the three agents, and although the evidence base for its use is not wide, it does have the advantage of specifically targeting CD8 positive T-cells which have been implicated in the pathogenesis of IR-hepatitis. 23 In addition it appears to have a quicker onset of action and a more favourable side effect profile34–36 Table 7 outlines the common properties of each of these immunosuppressant agents.
Of the six patients treated with tacrolimus, the four patients in Table 6 were comparable; it was a lack of response to escalated corticosteroids that prompted the use of tacrolimus. In all four patients, tacrolimus resulted in a rapid reduction in ALT and allowed successful weaning of steroids. The experience of these four patients suggests early introduction of tacrolimus may be considered in steroid-refractory IR-hepatitis.
Our study has several limitations. It was a small retrospective review relying on the interpretation of clinical notes with an inherent reporting bias; there may have been eligible patients that weren’t included as the relevant fields weren’t identified in the database. It did not address the role of biopsy – something which is likely to be important if patients are to be managed without steroids.13,30 It is also acknowledged that management of IR-hepatitis is likely to have changed over the time period of this study, for example, it is likely tacrolimus was introduced for patients treated more recently as more experience has been gained in the use of this drug. Despite these limitations, the current international guidelines for IR-hepatitis although useful, also have shortcomings and this study has drawn some important conclusions that should help address outstanding areas of clinical uncertainty in this field.
Firstly, there may be some patients present with a grade 3 ALT who do not need to be exposed to corticosteroids and, as proposed by De Martin et al., 31 there is growing evidence that a ‘watch and wait’ approach is possible in clinically well patients.
Furthermore, if patients do require initiation of corticosteroids, we have demonstrated that this can be successfully undertaken on an outpatient basis, and we have also shown that weaning of steroids can be achieved over a six-week period if the initial response is obtained. It is acknowledged that further consideration for both of these approaches would be needed if a biopsy was to be considered.
Finally, for those patients who do not respond adequately to steroids, this study has described the successful use of tacrolimus in a number of patients. The use of alternative immunosuppression in IR-hepatitis is not well characterised and so this is a significant addition to this area of practice. This is a newer drug compared to mycophenolate and azathioprine and its quicker onset of action and improved side effect profile make it an attractive alternative in this setting, although more experience is required, especially with respect to optimum dosing.
Conclusions
We provide evidence for two important deviations from the current IR-hepatitis guidelines; firstly, to avoid steroids completely in select patients, and secondly to use tacrolimus for IR-hepatitis refractory to corticosteroids. Further data is required for the adoption of these strategies, as well as the use of biopsy, preferably within the context of randomised controlled trials.
Footnotes
Funding statement
No specific funding was used for this study.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.