
Abstract
Introduction
HLX01 is the first rituximab biosimilar produced in China and the first monoclonal antibody biosimilar marketed in China. The purpose of this study was to comprehensively evaluate whether HLX01 is clinically consistent with the original drug based on real-world data to provide evidence for the clinical substitution of biosimilars in China.
Methods
A single-center retrospective study was conducted to select patients with diffuse large B-cell lymphoma who met the inclusion criteria and were treated with HLX01 or reference rituximab. Baseline characteristics, efficacy and safety results were recorded, and the corresponding statistical analysis was performed for various indicators.
Results
Thirty-three patients diagnosed with diffuse large B-cell lymphoma were included and divided into two groups that received HLX01 or reference rituximab. The results showed no significant difference in the overall response rate (86.7% vs. 88.9%; p = 1.000) or complete response rate (46.7% vs. 55.6%; p = 0.889) between the two groups. Kaplan–Meier survival curves also showed no significant difference in time-to-event variables between the two groups (log-rank = 0.244). Safety was also comparable in both groups.
Conclusions
HLX01 is a suitable replacement for reference rituximab in the treatment of diffuse large B-cell lymphoma and is relatively inexpensive, thereby reducing the economic burden of patients. Nevertheless, the conclusion of this study still needs to be further validated by large-sample real-world data and explored for HLX01 in other indications, such as follicular lymphoma.
Clinical trial registration
Not applicable.
Introduction
Non-Hodgkin's lymphoma (NHL), a heterogeneous tumor, has become the most common hematologic malignancy with an estimated 77,240 new cases in the United States in 2021. 1 As the most common type of NHL, diffuse large B-cell lymphoma (DLBCL) accounts for approximately 30% of all NHL cases.2,3 The advent of rituximab (MabThera®, F. Hoffmann-La Roche Ltd), which has shed light on patients with DLBCL, has significantly improved the prognosis of patients with DLBCL by specifically acting on the CD20 receptor on the surface of NHL cells.4–6 Nevertheless, the high cost and limited availability of rituximab preclude its use by many eligible patients, especially in developing countries, such as China.7,8
The advent of biosimilars has not only introduced alternatives with similar clinical effectiveness to that of the original drugs but also reduced the cost of medication for patients.9,10 HLX01 (Han-Li-Kang®) was developed by Shanghai Henlius Biotech and approved by the National Medical Products Administration (NMPA) on February 22, 2019, representing the first rituximab biosimilar produced in China. Several recent studies, including phase 3 clinical trials, have shown that HLX01 is bioequivalent, effective and safe compared to the reference rituximab.11–13
Nevertheless, the DLBCL patient population exhibits significant heterogeneity in biology and clinical practice; thus, further real-world data are needed to support the application of HLX01 in DLBCL. 14 Moreover, based on the fact that the development of biosimilars in China is only in the beginning stages, many ordinary people, and even doctors and pharmacists, do not have a complete understanding of the concept of biosimilars and even worry about their efficacy and safety. Thus, real-world research on biosimilars is encouraged in China to further improve the relevant systems of biosimilars. As the first monoclonal antibody biosimilar marketed in China, it is necessary to conduct a clinical comprehensive evaluation of whether HLX01 achieves clinical consistency with the original drug from a real-world perspective, providing an evidence-based basis for the clinical replacement of biosimilars in China.
Methods
Patients and materials
The medical records of patients with histologically confirmed DLBCL were retrospectively reviewed to identify patients who initiated treatment at The First Affiliated Hospital of Guangdong Pharmaceutical University, a tertiary Class A hospital, from February 2019 to March 2021. All included patients had received at least one cycle of the reference rituximab or HLX01 chemotherapy regimen. Patients with primary mediastinal B-cell lymphoma, posttransplant lymphoproliferative disorder, transformed lymphoma, human immunodeficiency virus-associated DLBCL, and pulmonary lymphomatoid granulomatosis were excluded to improve the homogeneity of the study population.
Data collected in the patient's medical records included clinical characteristics at diagnosis, including sex, age, presence of B symptoms, International Prognostic Index (IPI), Eastern Cooperative Oncology Group performance status (ECOG PS), disease stage, molecular subtype, number of extranodal sites involved, combination regimen, lactate dehydrogenase (LDH) and β2-microglobulin levels. Among them, molecular typing of cases was classified into germinal center B-cell (GCB) and non-GCB DLBCL subtypes by the Hans algorithm, whereas clinical staging was classified into stages I to IV using the Ann Arbor staging system. 15
The study was conducted in accordance with the Declaration of Helsinki. Each patient signed an informed consent form at the initiation of diagnosis, allowing for further clinical research using the clinical records, and this study was approved by the Ethics Committee of the First Affiliated Hospital of Guangdong Pharmaceutical University.
Treatment and response assessments
All patients received 375 mg/m2 MabThera or HLX01 on Day 1 of each 21-day cycle in combination with other chemotherapeutic agents. The number of treatment cycles and consolidation therapies varies according to the patient's disease stage, response to initial chemotherapy, and treatment tolerance of individual patients. Six cycles of chemotherapy were planned for most patients. In each treatment cycle, patients received oral acetaminophen, intravenous antihistamines, and hydrocortisone prior to treatment with either the MabThera or HLX01 and were routinely administered long-acting granulocyte-colony stimulating factor (GCSF) on Day 2 of each cycle to prevent febrile neutropenia (FN). For patients with stage I disease, at least four adjuvant chemotherapies were administered if no residual disease remained after surgical resection or biopsy resection.
Based on the International Working Group consensus response assessment criteria for lymphomas, patients were evaluated for response at the middle and end of chemotherapy, and related adverse events during treatment were recorded. 16 Adverse events were graded according to the Common Terminology Criteria for Adverse Events version 5.0.
Statistical analysis
The Shapiro–Wilk test was used to determine whether continuous variables were normally distributed, and continuous variables that met the normal distribution were described as the mean, standard deviation, median, and interquartile range. Differences between categorical variables were assessed using the chi-square test or Fisher's exact test, and differences between continuous variables were assessed using Student's t test or the Mann–Whitney U test. The overall response rate (ORR) was defined as the sum of complete response (CR) and partial response (PR) rates. In addition, subgroup analysis of efficacy parameters was performed according to molecular subtype (GCB vs. non-GCB DLBCL). PFS was defined as the time from the start of chemotherapy to disease progression, including any recurrence or death from any cause. Patients without documented disease progression or death at the time of the final analysis were censored at the date of the last follow-up, with a cutoff date of 1 March 2022. Time to event variables and HR values were assessed using Kaplan–Meier product limit and Cox proportional hazards models, and recurrence status was compared between the two groups using the log-rank test. The unadjusted model included only drug type to assess whether it was a factor influencing PFS, and the adjusted model was further established to correct for factors, such as age, molecular subtype, clinical stage, IPI, β2-microglobulin, LDH, number of extranodal invasions, and B symptoms, to observe the effect of drug type on PFS. All statistical analyses were performed using R Version 4.1.1 with p values < 0. 05 was considered statistically significant.
Results
Patient characteristics
A total of 68 patients were obtained from the hospital database. After excluding 29 patients who did not meet the inclusion criteria, 39 patients were screened. To improve the comparability of HLX01 to MabThera, 6 patients were excluded due to switching from HLX01 to MabThera or from MabThera to HLX01 during treatment. Finally, 33 patients with DLBCL were included in the retrospective analysis, including 15 patients treated with HLX01 and 18 patients treated with MabThera (Figure 1). The baseline demographic and disease characteristics of the patients are shown in Table 1. No significant differences in sex, age, molecular type, disease stage, B symptoms, ECOG PS, extranodal invasion or combination regimen were noted between the two groups (all P > 0.05). Nevertheless, significant differences in gender, IPI, LDH, and β2-microglobulin were noted between the two groups (all P < 0.05).
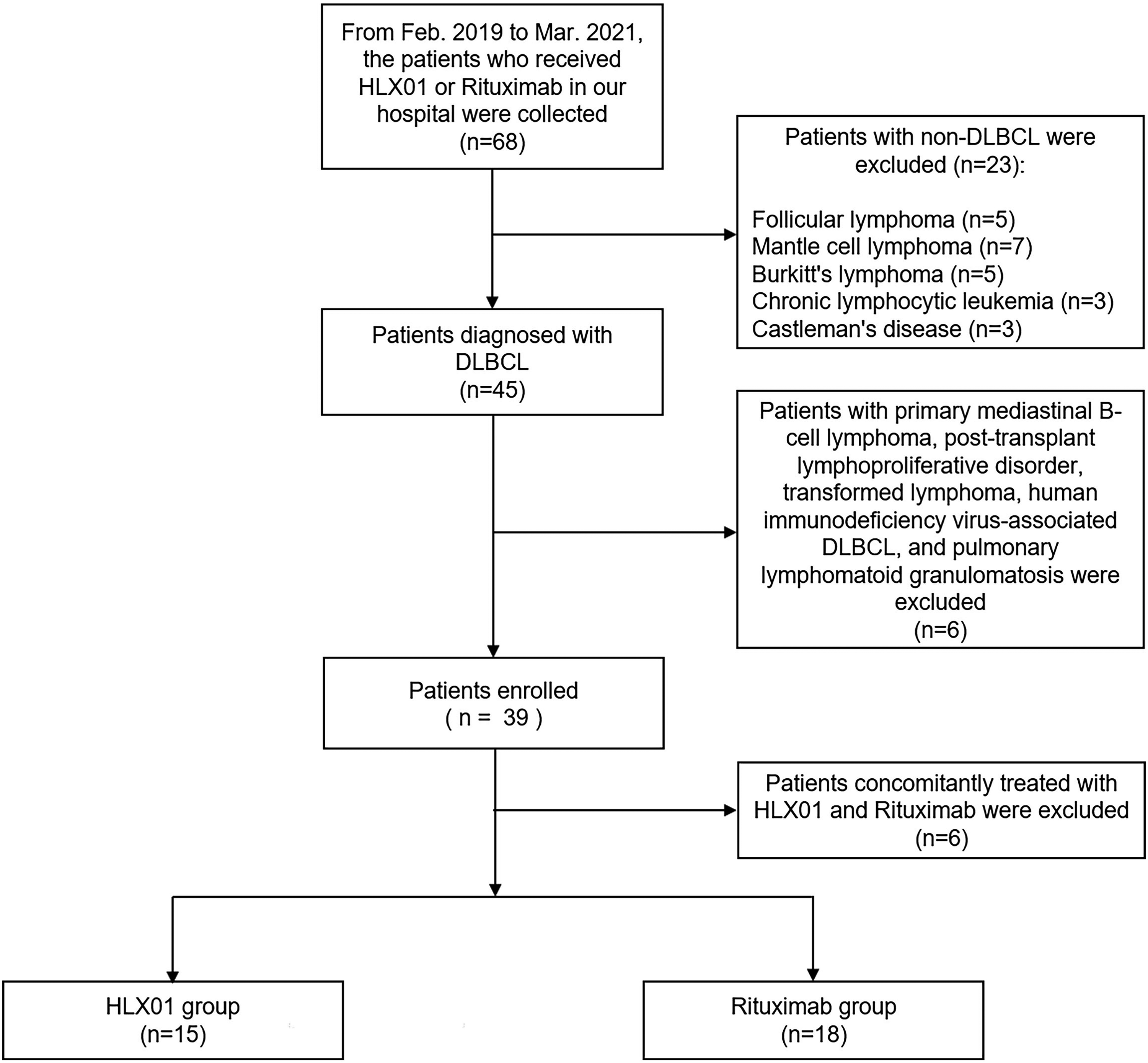
Screening patient flow chart.
Demographical characteristics and clinical data of the patients.
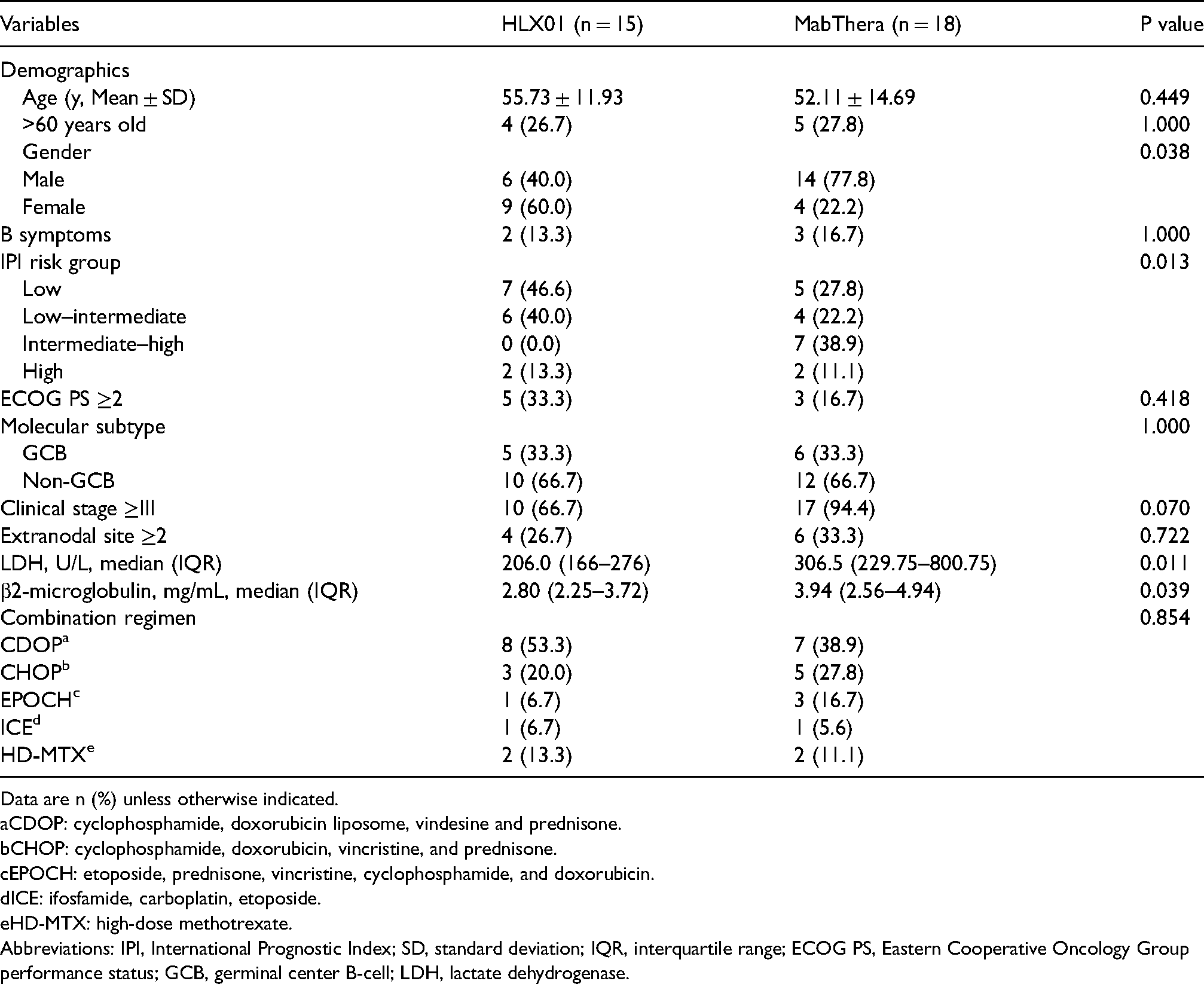
Data are n (%) unless otherwise indicated.
CDOP: cyclophosphamide, doxorubicin liposome, vindesine and prednisone.
CHOP: cyclophosphamide, doxorubicin, vincristine, and prednisone.
EPOCH: etoposide, prednisone, vincristine, cyclophosphamide, and doxorubicin.
ICE: ifosfamide, carboplatin, etoposide.
HD-MTX: high-dose methotrexate.
Abbreviations: IPI, International Prognostic Index; SD, standard deviation; IQR, interquartile range; ECOG PS, Eastern Cooperative Oncology Group performance status; GCB, germinal center B-cell; LDH, lactate dehydrogenase.
Efficacy results
Overall, a total of 29 (87.9%) patients completed the planned chemotherapy cycles, including 6 cycles of adjuvant chemotherapy in 1 case in the HLX01 group. In the entire patient population, 29 (87.9%) and 17 (51.5%) patients achieved an overall response and complete response (CR), respectively. Among them, 13 (87.9%) and 7 (46.7%) patients in the HLX01 group achieved an overall response and complete response, respectively, whereas 16 (88.9%) and 10 (55.6%) patients in the MabThera group achieved an overall response and complete response, respectively. No significant differences were noted between the overall response rate (P = 1.000) and complete response rate (P = 0.889) of patients in the two groups after receiving chemotherapy (Table 2). Subgroup analyses were also conducted for patients with GCB versus non-GCB disease to assess the efficacy outcomes of the two groups with different molecular subtypes, and the results showed no statistically significant difference in the efficacy outcomes between the two groups (all P > 0.05) (Table 3).
Efficacy outcomes of two groups.

Data are n (%).
Abbreviations: CR, complete response; PR, partial response; PD, progressive disease.
Efficacy outcomes of two groups according to molecular subtype.
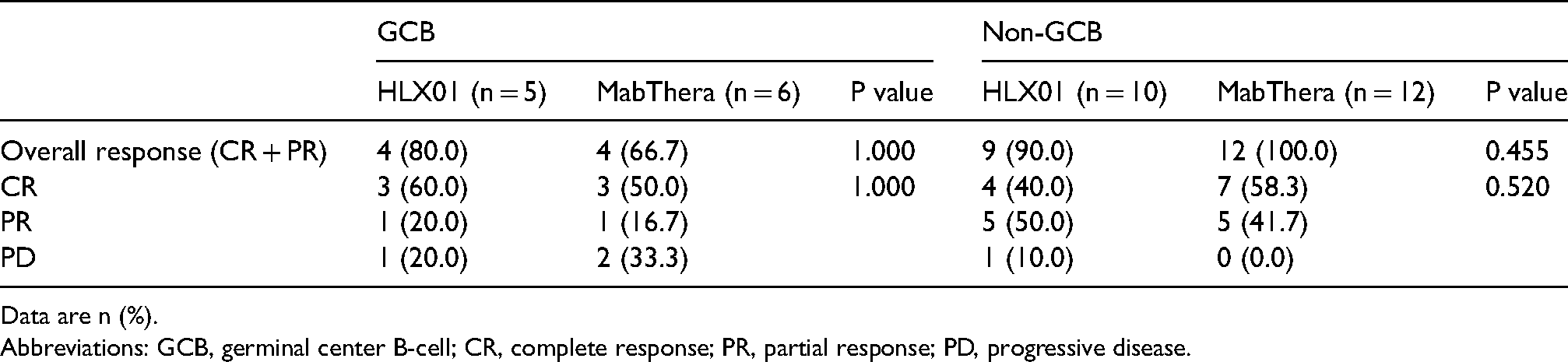
Data are n (%).
Abbreviations: GCB, germinal center B-cell; CR, complete response; PR, partial response; PD, progressive disease.
In the survival analysis, the median (range) follow-up time for the entire patient population was 9 (4–27) months. The median (range) follow-up times were 6.5 (4–20) and 11 (5–27) months in the HLX01 and MabThera groups, respectively. Thirty-three patients did not experience a death event within the planned chemotherapy cycle. Four patients were lost to follow-up after disease progression within the planned chemotherapy cycles (2 in the HLX01 group and 2 in the rituximab group). Given that no patient died during the entire treatment period or follow-up period, only PFS curves were plotted, and Kaplan–Meier estimation described the recurrence status between the two groups. The results of the log-rank test showed no significant difference in recurrence status between the two groups (P = 0.244), whereas the median PFS was not achieved in either group (Figure 2). Both unadjusted [HR: 0.479 (95% CI: 0.128, 1.792), P = 0.274] and adjusted [HR: 0.185 (95% CI: 0.022, 1.562), P = 0.121] Cox regression models showed no effect of drug type on PFS.
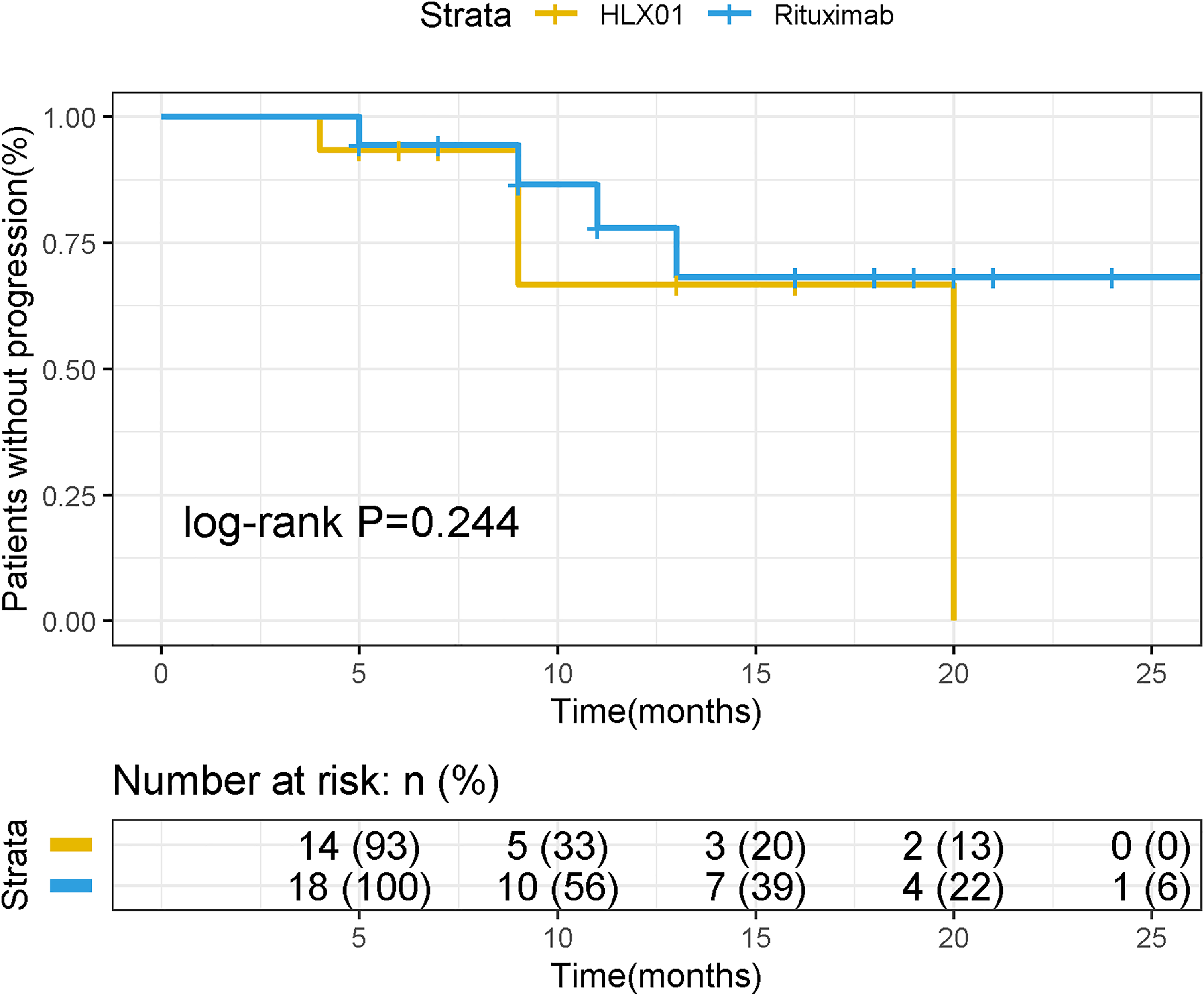
Kaplan–Meier survival curves for progression-free survival.
Safety results
All patients experienced adverse events even after conventional prophylactic medication before chemotherapy, including 7 patients with grade 3 or greater adverse events in the HLX01 group and 9 patients with grade 3 or greater adverse events in the MabThera group. Among the population with grade 3 or greater adverse events, 6 patients treated with HLX01 developed FN, whereas 8 patients in the MabThera group developed FN, 1 patient in the HLX01 group reported severe pneumonia, and 3 patients in the MabThera group reported severe anemia. In addition, both HLX01 group and Mabthera group reported 1 patient with sepsis due to severe infection. Overall, no significant difference was noted between the two groups in the population with grade 3 or greater adverse events (P = 0.387) (Table 4). Two patients in the MabThera group reported infusion-related reactions with symptoms including chills and shivering. In the early stage of chemotherapy (the first to the third cycle), the most common adverse reactions were myelosuppression, including leukopenia and neutropenia. Specifically, 10 patients treated with HLX01 had myelosuppression, whereas 13 patients in the MabThera group had myelosuppression. No significant difference was noted between the two groups (all P > 0.05) (Table 4).
Adverse events of two groups.
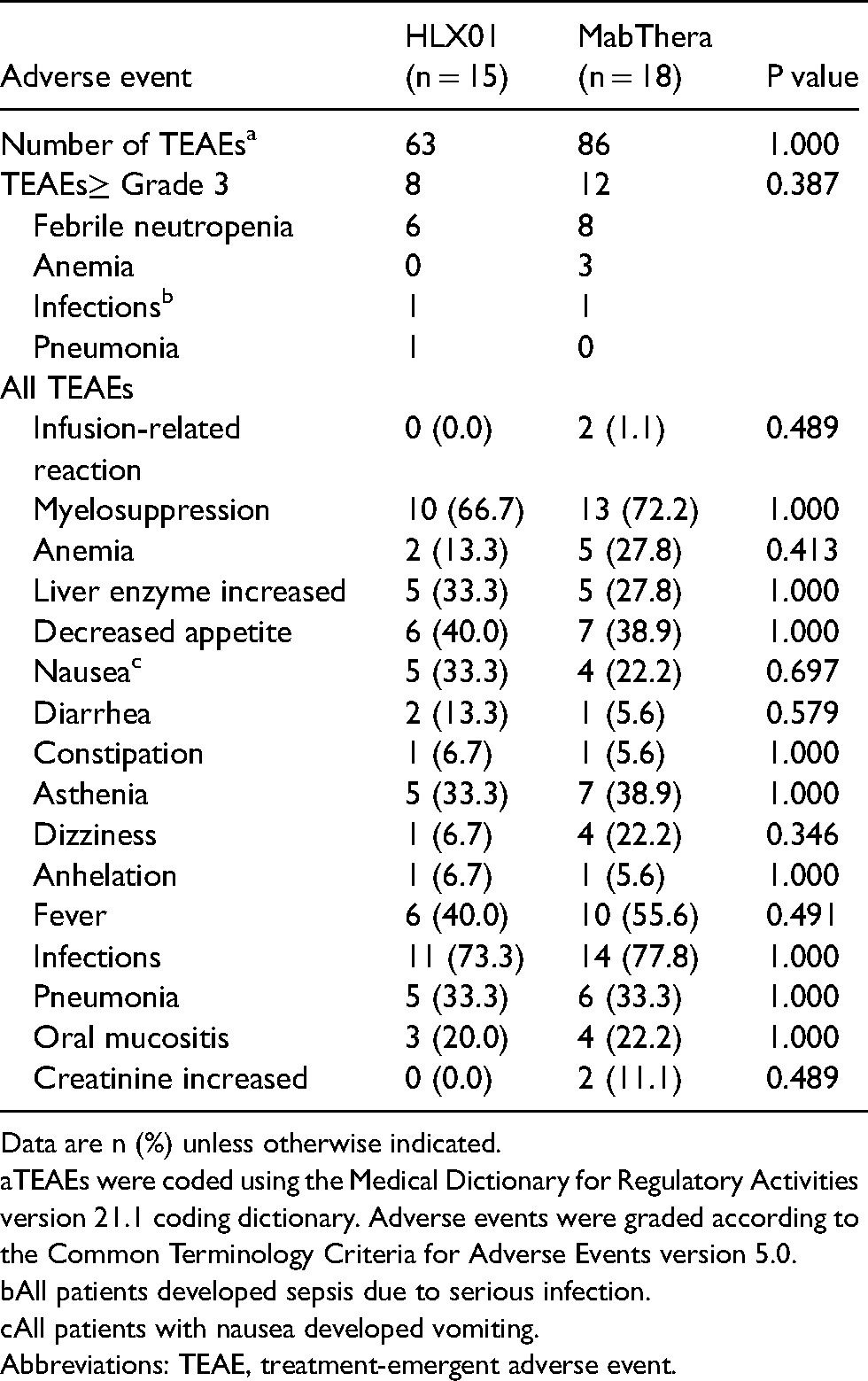
Data are n (%) unless otherwise indicated.
TEAEs were coded using the Medical Dictionary for Regulatory Activities version 21.1 coding dictionary. Adverse events were graded according to the Common Terminology Criteria for Adverse Events version 5.0.
All patients developed sepsis due to serious infection.
All patients with nausea developed vomiting.
Abbreviations: TEAE, treatment-emergent adverse event.
During the entire chemotherapy period, a total of 25 patients developed infection in the entire patient population, including 11 patients in the HLX01 group and 14 patients in the MabThera group, with no significant difference noted between the two groups (P = 1.000). In addition, renal impairment was reported in two patients in the MabThera group and none in the HLX01 group, but no statistically significant difference was observed between the two groups (P = 0.489). Overall, no significant differences in anemia, liver enzyme increased, decreased appetite, nausea, diarrhea, constipation, asthenia, dizziness, anhelation, fever, pneumonia, or oral mucositis were found between the two groups (all P > 0.05) (Table 4).
Discussion
Therapeutic monoclonal antibodies account for less than 5% of the biopharmaceutical market in China due to their high cost, which is much lower than the global average market share of 30%. The emergence of biosimilars has improved the burden capacity of patients and provided greater access to basic treatments for a wider range of patient populations, especially patients in developing countries, such as China. 11 However, given the relatively large molecular weight and complex structure of biosimilars, these agents are not completely consistent with the reference drug in terms of structure and function. In addition, the development of biosimilars in China is only in the beginning stages, and patients, doctors and pharmacists still have a half-doubtful attitude toward biosimilars. Thus, it is very important to use real-world data to analyze and evaluate newly marketed biosimilars and compare them with original drugs.
This study evaluated the efficacy and safety of HLX01 versus MabThera in the treatment of patients with DLBCL based on real-world clinical data. The results showed no significant differences in the efficacy, survival outcomes or adverse events between HLX01 and MabThera in the treatment of patients with DCLBCL, and HLX01 did not show any special adverse reactions compared with MabThera. Only 46.7% of patients in the HLX01 group achieved a CR compared with 55.6% in the MabThera group, but the ORR was similar between the two groups (86.7% in the HLX01 group and 88.9% in the MabThera group). This finding may be explained by the small sample size. To enhance the homogeneity of the two groups, we performed a subgroup analysis of molecular subtypes (GCB vs. Non-GCB DLBCL). The results showed no statistically significant difference in the CR rate between the two groups.
It is worth noting that, due to the complex clinical situation in the real world, 6 of the included patients were previously treated in other hospitals (3 in the HLX01 group and 3 in the MabThera group), and the specific chemotherapy regimen was unclear. In the treatment of DLBCL, rituximab in combination with other chemotherapy regimens is also common in real-world clinical practice relative to the traditional first-line combination regimen CHOP (cyclophosphamide, doxorubicin, vincristine, and prednisone). 17 Of the 33 patients included, the combination chemotherapy regimen used in 15 patients was CDOP (cyclophosphamide, doxorubicin liposome, vindesine and prednisone), which has been recommended for patients with poor cardiac function in China, and it has been shown that doxorubicin liposome instead of traditional doxorubicin is a safer treatment option for patients’ cardiac function. 18 The combination chemotherapy regimen used in the four patients was EPOCH (etoposide, prednisone, vincristine, cyclophosphamide, and doxorubicin), which was recommended for the treatment of advanced patients by the Chinese Guidelines for the Diagnosis and Treatment of Diffuse Large B-Cell Lymphoma Therapy, but also by the Chinese Society of Clinical Oncology (CSCO) Guidelines for the Diagnosis and Treatment of Malignant Lymphoma as Category II recommendations for the treatment of DLBCL.19,20 The combination chemotherapy regimen used in 2 patients was ICE (ifosfamide, carboplatin, etoposide), which is recommended by the Chinese Society of Clinical Oncology (CSCO) guidelines for the diagnosis and treatment of malignant lymphoma for patients with relapsed/refractory DLBCL. 19 The combination chemotherapy regimen used in 4 patients was HD-MTX (high-dose methotrexate), which is recommended for patients with primary central nervous system lymphoma (PCNSL) by the Chinese Guidelines for the Diagnosis and Treatment of Diffuse Large B-Cell Lymphoma, while studies have shown that this regimen can improve the survival prognosis of patients with PCNSL.21–23 Compared with R-CHOP regimen in phase III clinical trials conducted by Shi et al., this study included more types of chemotherapy regimens in combination with HLX01 or MabThera for the treatment of DLBCL, providing a reference basis for clinical rational drug use.
In the survival analysis, 4 patients experienced disease progression during treatment (2 in the HLX01 group and 2 in the MabThera group), and 5 patients had disease progression during follow-up after the end of treatment (3 in the HLX01 group and 2 in the MabThera group). Both median PFS values were not reached in either of the two groups. Regarding safety, no significant differences in adverse events were noted between the two groups, and this result was consistent with the phase III clinical trial conducted by Shi et al. 13 The current study showed that in clinical practice, HLX01 exhibits equivalent efficacy and safety to MabThera in the treatment of patients with DLBCL. Since the patent protection of rituximab originators expired in the European Union (MabThera®) and the United States (Rituxan®) in 2013 and 2018, respectively, a number of rituximab biosimilars have been developed. 24 To date, nine rituximab biosimilars have been marketed,25–31 and the results of a meta-analysis conducted by Lee et al. 32 showed that rituximab biosimilars were not significantly different from the original drug in terms of efficacy and safety.
As the first monoclonal antibody biosimilar manufactured in China and marketed for the first time in China, the emergence of HLX01 has opened the market for monoclonal antibody biosimilars in China. Although phase III clinical trials have demonstrated that HLX01 in combination with the CHOP regimen is comparable to MabThera in combination with the CHOP regimen in terms of efficacy and safety in the treatment of patients with DLBCL, 13 more postmarketing real-world data are needed to continue to evaluate the clinical equivalence of HLX01 and MabThera because the actual clinical situation is complex. In addition to the heterogeneity of patients’ conditions, different combination regimens are available that affect the efficacy and safety of the drug on the disease. In December 2019, Mabthera, the original drug of rituximab, was added for the treatment of two new indications related to follicular lymphoma (FL) and chronic lymphocytic leukemia (CLL) in China, whereas HXL01 was also approved for the treatment of the above two indications in July 2020. Furthermore, for indications not approved in China by Mabthera, such as rheumatoid arthritis, HLX01 was also licensed for the treatment of this indication on March 1, 2022. Therefore, long-term real-world studies are required to comprehensively evaluate the clinical equivalence of HLX01 and MabThera not only for DLBCL but also for other indications. This biosimilar has the potential to greatly reduce the economic burden under the premise of obtaining the same efficacy and safety as the original drug.
This study has some limitations, such as differences in gender, baseline IPI, LDH, and β2 microglobulin data between the two groups of patients. Given that this study is a single-center retrospective study, and since HLX01 is newly launched in China, the sample size of patients using the drug is small, so the differences cannot be avoided. However, we used Cox proportional hazards models to correct for these differential influencing factors, and the adjusted model showed that these influencing factors had no effect on the results of drug type acting on PFS. The comparison between drugs had some reliability because the results reflected the treatment situation using the same resources under the same conditions in the same institution. Furthermore, the results of this study were not significantly different from the phase III clinical trial conducted by Shi et al., 13 both demonstrating the clinical equivalence of HLX01 and Mabthera. Second, given the need to enhance the homogeneity of the study population, patients with histological variations were excluded from this study, and future studies should consider these variables. In addition, due to the limited information provided by medical records, some patients had adverse events recorded simply as myelosuppression without specific types of myelosuppression, and 18 patients were lost to follow-up less than one year after completing the planned follow-up period of chemotherapy cycles (10 in the HLX01 group and 8 in the Mabthera group). Thus, mature survival data were not available. In general, even if the statistical method is adjusted for in this study, due to the limitations of small sample size and lack of power, the conclusions of this study still need to be verified by a larger scale study with real-world data to further demonstrate the clinical similarity between HLX01 and Mabthera.
In conclusion, this study showed no significant difference in treatment response, survival results or adverse events between HLX01 and Mabthera in the treatment of patients with DLCBCL, further showing the clinical equivalence of HLX01 and Mabthera. Nevertheless, due to the limitations of small sample size in this study, more multicenter, real-sample, rigorously designed world data are needed to further evaluate the clinical equivalence of HLX01 and Mabthera in the future.
Footnotes
Acknowledgements
This study was supported by National Key Clinical Specialty Construction Project (Clinical Pharmacy) and High Level Clinical Key Specialty (Clinical Pharmacy) in Guangdong Province.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by the The Pharmaceutical Research Special Fund of Guangdong Provincial Hospital Association (Hengrui) Pharmaceutical Research Key Project, The Guangzhou Minsheng Science and Technology Research Program Project, The central finance subsidy fund for the improvement of medical services and guarantee capacity, (grant number 2021YXZD01, 201803010096, Z155080000004).