
Abstract
Introduction
Overuse of anti-cancer therapy near end of life is an important quality-of-care issue. An aggressive approach to treatment can have negative effects on the quality of life and cost of hospital-based resources. The objective of this study was to measure indicators of potential aggressiveness of end-of-life care in a cohort of adult patients with advanced solid tumor. The secondary objective was to analyze the association between clinicopathological variables and indicators of aggressiveness.
Methods
Retrospective data analysis was performed on adult patients with solid tumors who received palliative chemotherapy for advanced cancer and died in our hospital between 2017 and 2019. Indicators of aggressiveness of end of life care included chemotherapy use in the last days of life, emergency room visits and hospitalizations (including intensive care unit admissions) in this period, and referral to a palliative care unit before death. Univariate and multivariate analyses were conducted to identify the variables that independently predicted the use of palliative chemotherapy near end of life.
Results
Of the 571 patients included, 128 (22.4%) received chemotherapy within the last 2 weeks of life and 102 (17.8%) start a new chemotherapy regimen 30 days before death. During the last month of life, 168 patients (32.9%) visited emergency room more than once and 117 (20.5%) were hospitalized more than once. A total of 294 patients (51.5%) died in the acute care unit and 285 (49.9%) were referred to the palliative care unit. 24 of them (8.4%) died within 72h after referral.
Conclusions
The percentage of patients receiving chemotherapy near the end of life as well as the rate of emergency room visits and hospitalizations during this period are much higher than the value of the quality standard established in the literature. According to these indicators, cancer patient care at end of life can be considered overly aggressive. Optimization of palliative care at end of life is necessary.
Introduction
Despite recent advances in oncology therapy, cancer is still a leading cause of death in most countries. 1
With the development of immunological and targeted therapies, which have less side effects and higher expected efficacy, the use of chemotherapy (CT) in the final weeks of life has experienced a significant increase according to different studies2–4 and this has led to an increase in the cost of hospital-based resources [emergency room (ER) visits, hospitalizations, and admissions to the intensive care unit (ICU)] and a decrease in the use of palliative care services.
However, the appropriate use of CT near end of life (EoL) is still unclear. The goal of palliative CT for patients with incurable cancer is to prolong survival and improve or maintain quality of life (QoL). Prescription of palliative CT represents a very delicate equilibrium between toxicity and potential clinical benefit that is even more complex when treating patients with a short life expectancy. Although palliative CT can relieve symptoms and temporary disease control, it may cause harm in terms of side effects or complications from treatment which may impair QoL. In fact, several studies have explored the association between continuing EoL CT and unfavorable outcomes, including reduced survival and lower QoL.5,6
Both the American Society of Clinical Oncology (ASCO) and the European Society of Medical Oncology (ESMO) have made recommendations in clinical practice guidelines for the concurrent use of CT near EoL and early involvement of palliative care services for patients with advanced cancer.7,8 Discontinuing CT in the last 2 weeks of life is listed as a benchmark for improving clinical practice in the Quality Oncology Practice Initiative of ASCO and has been identified as one of the “top five” practices that could reduce medical costs and improve patients’ care. 9
Earle et al. identified aggressive care near the EoL as a sign of poor quality cancer services and proposed quality indicators of cancer care for external benchmarking. 10 Three major areas were evaluated: (1) overuse of CT very near death; (2) possible misuse of treatment resulting in high rates of ER visits, hospitalizations, or ICU stays for terminal patients; and (3) underuse of hospice services as measured both by lack of referral or very late referral to a palliative care unit (PCU).
The objective of this study was to measure indicators of potential aggressiveness of EoL care proposed by Earle et al. in a cohort of adult patients with advanced solid tumors. The secondary objective was to analyze the association between clinicopathological variables and indicators of aggressiveness.
Materials and methods
Study design and participants
This study used a retrospective observational design. Adults aged 18 years or older diagnosed with a non-curable locally advanced or metastatic cancer who died at the Spanish public university hospital from January 2017 to December 2019 were identified. Patients who received palliative CT were included in the study. Patients were excluded if the cancer diagnosis was a hematological malignancy, if they were not seen by the medical oncology service, or if they were treated with curative intent. Data were collected from the electronic medical record system and Farmis-Oncofarm® software. Approval for the study was obtained by an institutional review board.
Clinicopathological features collected included age at time of death, gender, cancer type, Eastern Cooperative Oncology Group (ECOG) at the time of last CT dose, number of lines of palliative CT received, last regimen received (with start and finish dates), and number of cycles (in case of oral anti-cancer treatments, one cycle was considered to have been taking them for 1 month).
The following classification was adopted in order to analyze the results according to tumor chemosensitivity 11 : highly sensitive tumors (breast, ovary, testis, and osteosarcoma), intermediately sensitive tumors (lung, colorectal, head and neck, stomach, esophagus, uterus, bladder, prostate, and unknown primary) and low chemosensitive/chemoresistant tumors (kidney, pancreas, hepatobiliary, central nervous system (CNS), melanoma, mesothelioma, soft tissue sarcomas, and thyroid).
Anti-cancer therapy was classified into five groups: (1) cytotoxic CT (intravenous or oral drugs, including combinations with drugs from other groups), (2) targeted therapy (monoclonal antibodies (mAbs), tyrosine kinase inhibitors (TKIs), and PARP inhibitors), (3) immunotherapy, (4) endocrine therapy, and (5) radiopharmaceutical. In this study, the term “chemotherapy” is used for all these groups.
Indicators of potential aggressiveness of treatment included the administration of CT in the last month and last 2 weeks of life; administration of palliative radiotherapy (RT) in the last 2 weeks of life; number of ER visits and hospital admissions for all causes, including to the ICU, in the last month of life; and referral to a PCU as well as length of stay.
Furthermore, data about the use of additional supportive care, such as colony-stimulating factors (CSFs), erythropoietins, intravenous Fe, or transfusions during the last line of CT also was collected, as well as the number of patients who required reduced dose or discontinue drugs from their last CT regimen.
Statistical analysis
Categorical variables were expressed as numbers and percentages, while continuous variables were presented using mean and SD for normally distributed variables and median and interquartile range (IQR) for non-normally distributed variables. The normally of the distribution was investigated using the Shapiro–Wilk test
Univariate analyses comparing characteristics of patients and aggressiveness criteria were carried out using Student’s t-test for continuous variables and chi-square test for categorical variables. A p-value < 0.05 was considered statistically significant.
Multivariate logistic regression analyses were performed to characterize factors associated with the indicators of aggressiveness. Adjusted odds ratios (ORs) were reported with their 95% confidence intervals (CIs).
All data were analyzed using R 3.6.2 software (R Core Team 2019).
Results
Between January 2017 and December 2019, a total of 975 patients diagnosed with a solid advanced cancer died in our hospital, 571 of which received palliative CT and were included in this retrospective analysis (404 patients were excluded because they received CT with curative intent or died without receiving CT).
Baseline characteristics are summarized in Table 1. The median age at death was 69 years (IQR: 60–77) with 65.3% male and 34.7% female. The most frequent diagnosis was lung cancer (24.2%), followed by colorectal (16.5%), urogenital (13.1%), and upper gastrointestinal (8.1%) cancer. About half of the patients treated (50.1%) had ECOG 0–1 (of note that 5.9% received their last CT with ECOG ≥3) and the majority of patients (66.9%) had intermediately chemosensitive tumors.
Clinical characteristics of patients receiving end-of-life (EoL) chemotherapy (CT).
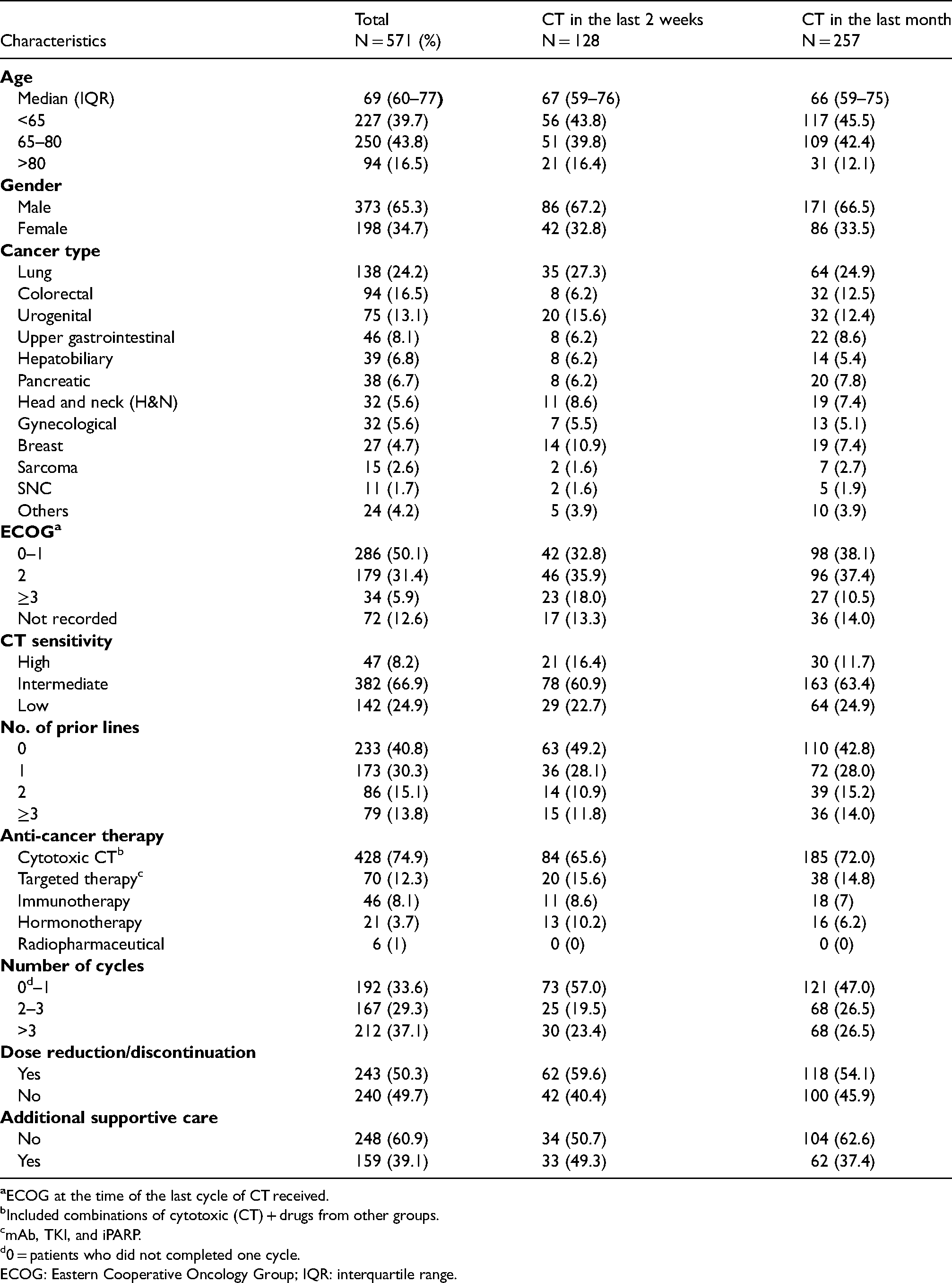
Included combinations of cytotoxic (CT) + drugs from other groups.
mAb, TKI, and iPARP.
0 = patients who did not completed one cycle.
ECOG: Eastern Cooperative Oncology Group; IQR: interquartile range.
Considering previous treatments, 233 patients (40.8%) were being treated with the first-line CT, 173 (30.3%) had received a single CT line, 86 (15.1%) had received 2 lines, and 79 patients (13.8%) had 3 or more previous lines of CT. The mean number of cycles that patients received of their last CT was 4.4 (SD = 6.2) but it is particularly noteworthy that 192 (33.6%) patients received only a single cycle or did not even complete it.
The median number of days between the start of the last CT treatment and patient death was 93 days (IQR: 47–183). This last regimen was mostly cytotoxic CT (74.9%) followed by targeted therapy (12.3%) and immunotherapy (8.1%).
Because of the study design all patients died in the hospital. Death occurred in an acute care unit for 294 patients (51.5%) while 277 (48.5%) died in the PCU. Because of the nature of the register, all the patients had at least 1 hospital admission in the last month of life.
Indicators of potential aggressiveness of treatment
Use of anti-cancer therapy near the EOL
Of the 571 patients, 128 (22.4%) received CT within the last 2 weeks of life and 257 (45%) during the last month of life. Of the 128 patients who received CT in the last 14 days, about half of them (49.2%) were being treated in the first line. The majority of these patients (68.7%) had ECOG ≤2, however, 23 patients (18%) received CT in their last 2 weeks with ECOG ≥ 3.
In terms of type of anti-cancer therapy, most of these patients (65.6%) received cytotoxic CT. The median number of days between the last dose of CT and patient death was 34 (IQR range 17–69). Of note that eight patients died on the same day or the day after CT administration.
A new CT regimen was started in the last month of life in 102 patients (17.8%). Fifty patients (49.0%) initiated the first line, 26 (25.5%) started the second line, 16 (15.7%) the third line, and 10 patients (9.8%) the fourth or more line. Almost three-quarters of patients, 75 (73.5%) started a regimen of cytotoxic CT, 14 patients (13.7%) targeted therapy, 11 (10.8%) immunotherapy, and 2 patients (1.9%) started a endocrine therapy.
Regarding the use of additional supportive care, more than one-third of patients (39.1%) required the use of supportive care during his last palliative CT line (including use of G-CSF, erythropoietin, IV Fe, or transfusions) and about half of patients (49.7%) required reduced doses or even discontinuation drugs from their CT regimen.
Finally, 31 patients (5.4%) received palliative RT within the last 14 days of life.
Variables found to have a statistically significant association with the administration of palliative CT within the last 2 weeks of life in the univariate analysis were ECOG, cancer type (breast cancer), and chemosensitivity of tumor (Table 2). With multivariate analysis using a logistic regression model, ECOG ≥3 (OR 12.4, 95% CI 5.15−31.4) and cancer type (breast cancer OR 8.61 compared with colorectal, 95% CI 1.23–65.8) remained significant predictors (Figure 1).
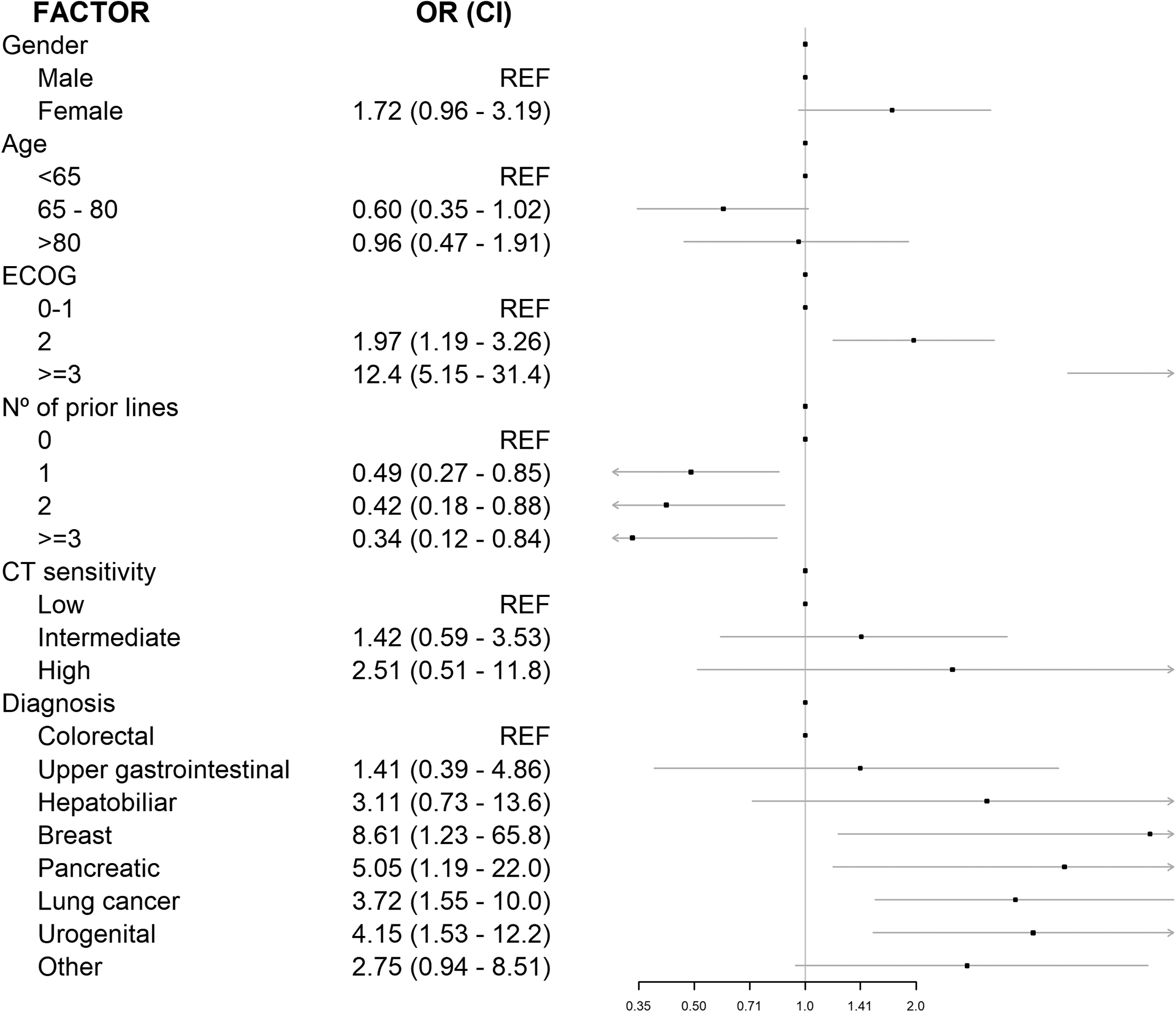
Factors associated with use of chemotherapy (CT) in the last 14 days of life: Multivariate analysis.
Factors associated with the use of chemotherapy (CT) in the last 14 days of life: Univariate analysis.
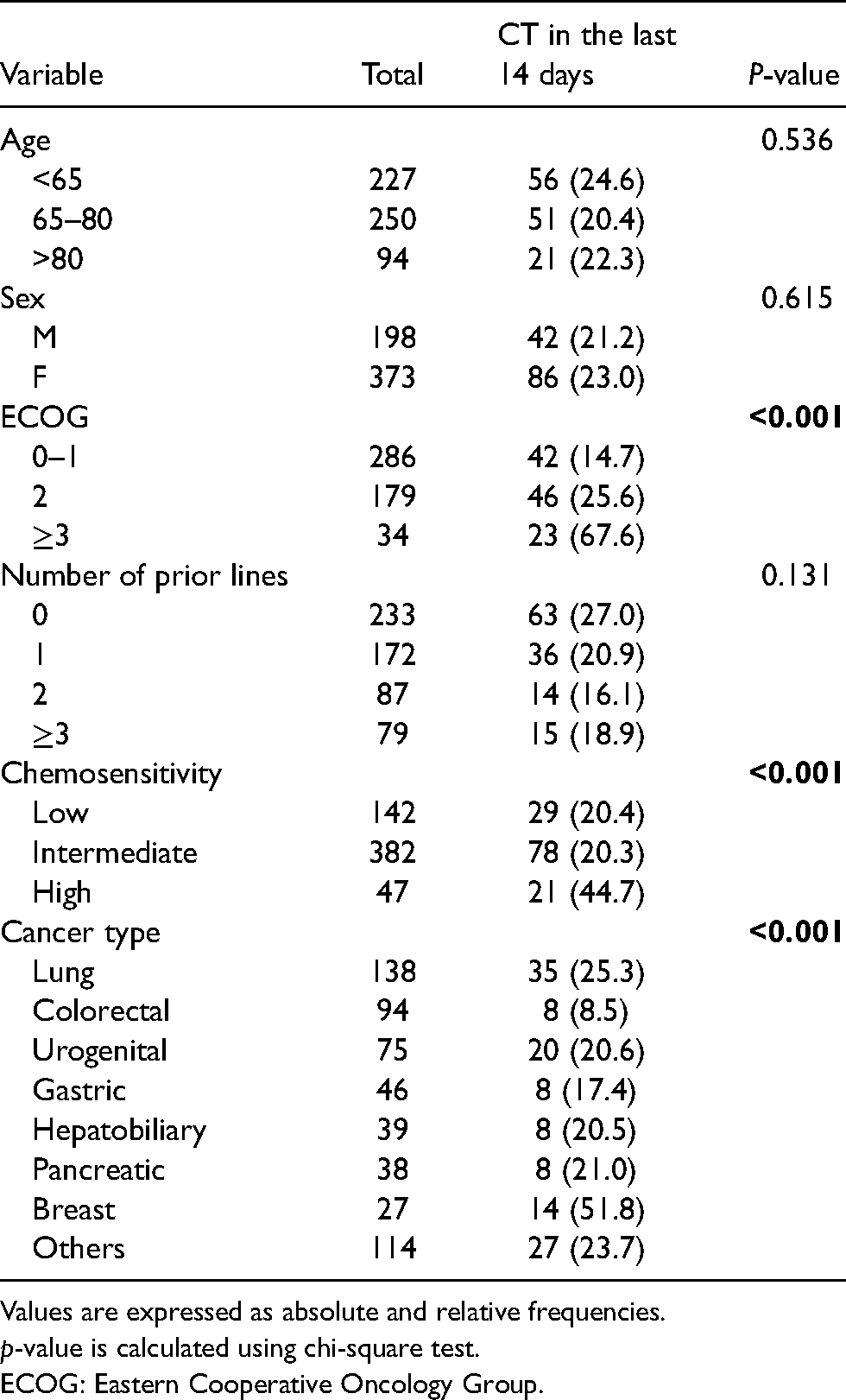
Values are expressed as absolute and relative frequencies.
p-value is calculated using chi-square test.
ECOG: Eastern Cooperative Oncology Group.
Use of health care services (ER visits and hospital admissions)
Of 510 patients (61 are excluded due to being hospitalized the last 30 days of life or starting his first-line CT during their last hospitalization), 420 patients (82.4%) had at least 1 ER visit in the last month of life and 168 (32.9%) visit ER more than once. The mean number of visits was 1.2 (SD = 0.8).
Because of the nature of the register, all the patients had at least 1 hospital admission in the last month of life and 117 patients (20.5%) were hospitalized more than once. The mean number of days spent in the hospital was 12.2 (SD = 9.3). Of note that 57 patients were hospitalized during the whole last month. On the other hand, only one of the 571 patients (0.2%) was admitted to the ICU in the last month of life.
Use of hospice care
A total of 285 patients (49.9%) were followed by the PCU before death (including admission to a hospital PCU, palliative consultations during admission in other acute departments, homecare support team services, and outpatient visits). Of these, 24 patients (8.4%) died within 72h to be referred to PCU.
Table 3 summarized the results for the aggressiveness criteria and the comparison with the objectives defined by Earle et al.
Aggressiveness indicators: Comparison between Earle et al. 10 and our results.
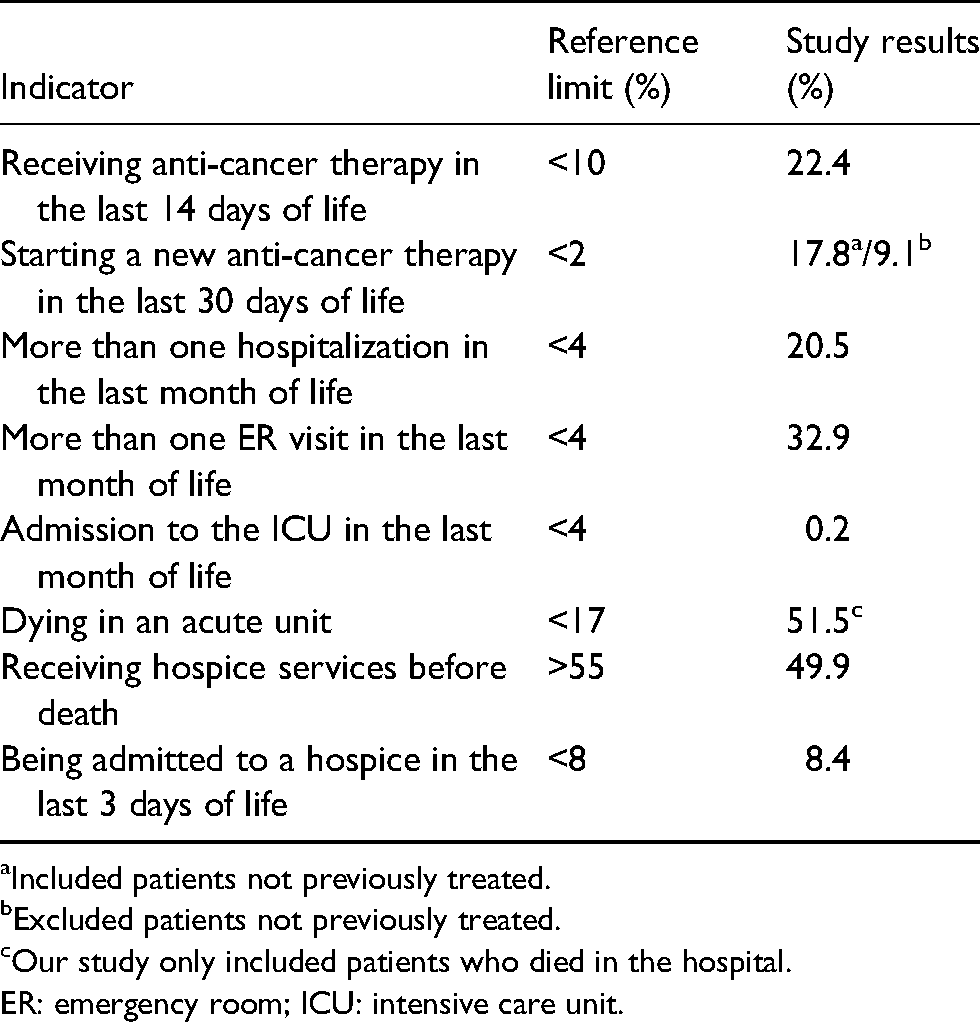
Included patients not previously treated.
Excluded patients not previously treated.
Our study only included patients who died in the hospital.
ER: emergency room; ICU: intensive care unit.
Discussion
Proposed standard benchmarks for “not overly aggressive cancer” care include <10% of patients receiving CT 14 days before death and <2% of patients starting a new CT regimen 30 days prior to death. 10 In the present study, 22.4% of patients received CT within the last 2 weeks of life and 17.8% started a new CT regimen 30 days before death, which is approximately 2 and 10 times higher, respectively, than the value of the quality standard proposed by Earle et al.
However, these findings are consistent with those reported previously by other Spanish groups. Martin et al. found that 27.5% of patients received CT in the last 2 weeks of life and 14% started a new IV CT regimen a month before death. 12 Similarly, Taberner Bonastre et al. reported a total of 21.7% patients receiving CT in the last 2 weeks of life. 13 More recently, Baena-Cañada et al. showed that 15.3% of patients received CT in the last 2 weeks, 14 while Sánchez-Cuervo et al. reported a total of 26.5% of onco-hematological patients receiving CT in the last 2 weeks and 20.8% starting a new CT in the last month. 15 Lastly, García-Martín et al. found that a lower percentage of patients, 12.9%, received anti-cancer treatment during their last 14 days of life and 9.1% started a new regimen in their last 30 days. 16 However, this study included all patients seen in the institution, and not just those who received palliative CT. This result demonstrates that in Spain, the excessive use of CT at the EoL is a generalized phenomenon. Table 4 shows summary of reports in the literature concerning the use of CT near EoL in Spain compared with our results.
Summary of reports in the literature concerning the use of chemotherapy (CT) near end of life (EOL) in Spain compared with our results.
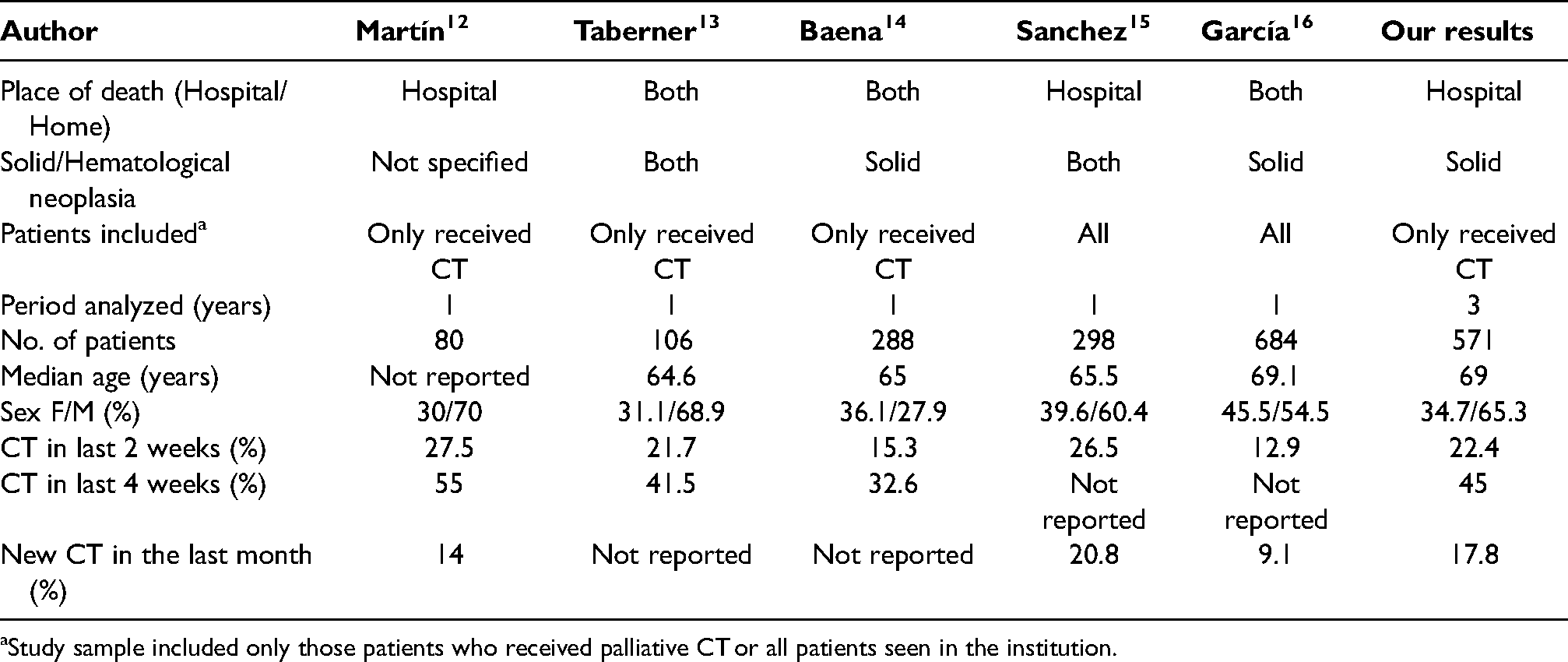
Study sample included only those patients who received palliative CT or all patients seen in the institution.
By contrast, studies performed in other European countries reported much lower rates of CT in the last 2 weeks of life: ranging from 5% in Norway, 17 7.2% in Finland, 18 7.6% in Swiss 19 to 11.3% in France. 20
This notable regional and national variation in the use of CT near EoL reflects not only cultural and religious differences but also differences in health care systems regarding cost reimbursement and availability of treatment options. Moreover, our findings may exceed those of other series because of a time bias defined by the increasing worldwide trend to administer CT near EoL in the era of therapeutics advances in precision oncology.
However, it should be kept in mind that reports about the use of CT near EoL are not necessarily comparable. Apart from having been conducted in different countries at different times, there are important methodological differences that must be acknowledged, as they can influence results and induce wrong conclusions when comparing data published on this topic. 21 For example, the number of patients considered to calculate the fraction of those undergoing treatment near EoL is variable, with some authors using the entire population of patients who died in a given period and others considering only the number of patients that received CT. Additionally, populations examined may include patients who died at home or not. The type of treatment considered as “chemotherapy” is also variable, with some studies excluding oral drugs or hormonal agents. Finally, criteria with respect to tumor (excluding or not hematological neoplasms) and patient’s characteristics are also potentially confounders making it very difficult to compare data from different institutions.
Despite the lack of evidence to support the practice, CT is widely used in cancer patients with poor PS and progression following an initial course of palliative CT.22,23 ASCO guidelines recommend against the use of CT in solid tumor patients who have not benefited from prior treatment and who have an ECOG of three or more. 9 In the present study, 34 patients (5.9%) received CT with an ECOG≥3 and 79 (13.8.%) had been treated with three or more previous lines of palliative treatment.
Furthermore, cytotoxic CT remained the most commonly used type of treatment despite the increasing use of immunotherapy and targeted therapies and despite its toxicity profile and low beneficial effect at this stage. In this study, the vast majority of patients (74.9%) received cytotoxic CT as their last regimen over targeted therapies (12.3%) or immunotherapy (8.1%). This could be explained mainly by the faster action of CT and its impact on symptom control in case of aggressive tumors.
It is particularly noteworthy that 40.8% of patients died during the first-line CT and 33.6% patients received only a single cycle or did not even complete it. These results are even higher in those patients who received CT in the last 2 weeks of life in which about half of them (49.2%) died during their first line of treatment and more than half (57%) even at their first cycle. It seems clear that the clinical evaluation criteria at the basis of the decision to prescribe CT might be brought into question.
During the last month of life, 82.4% of our patients had at least one ER visit and 32.9% visit ER more than once, which is more than eight times the value of the quality standard established by Earle et al. (<4%). Although it can be difficult to differentiate which of these visits are due to the disease itself and which are due to toxic adverse effects, the increased percentage of ER visits in our study may be related to the limited access to palliative care services and home health care for all patients which forces the patients to attend the ER if they have any symptoms.
Hospitalization near death is an essential indicator of aggressiveness of care; it is associated with poor QoL among dying patients 24 and increased health care costs. 25 Spain is one of the countries where the proportion of hospital as a place of death is higher,26,27 suggesting hospitalization near death is quite prevalent. In this study, 20.5% of patients had more than one hospitalization in the last month of life, above five times the threshold established by Earle et al. (<4%). The palliative intervention could be an option to improve this situation by reducing the cost and the length of hospital stay, as a prospective cohort study showed. 28
In addition to providing data on prevalence, we also investigated the factors associated with the use of CT near EoL. Previous studies have found that younger age is associated with higher rates of CT use at EoL while other variables such as chemosensivity, cancer type, ECOG, or gender show contradictory results. 29 In this study, only ECOG and type of tumor remained significant predictors in the multivariate analysis; patients with ECOG≥3 were those more likely to receive CT in the last 2 weeks of life, despite guidelines recommendations against it, which is a clear sign of overtreatment. Regarding type of tumor, breast cancer was the most likely to be positively associated with the use of CT at EoL, possibly due to the basis of treatment is endocrine therapy ± iPARPs, both oral drugs.
Taken together, our data seem to be in the higher range of the numbers reported in the literature and above the value of the quality standard proposed by Earle et al. The reasons for this overtreatment are many.
Prognostic difficulties: Physicians’ perceptions of prognosis may influence EoL CT use. Several studies have shown that oncologists generally tend to overestimate survival in end-stage cancer patients.30,31
Communication difficulties: Communicating about the EOL with patients has been reported as one of the most difficult and stressful parts of the work of oncologists. 32 Talking to patients and families about dying and supportive care is not easy. Even the clinicians who are well trained at giving bad news can find it painful, especially if they have a close relationship with the patient or if the patient is young. Telling the truth seems to take away their hope, so recommending a new course of CT to patients is often an easier option than discussing cessation of CT and transition to palliative care. A prospective study on palliative CT versus watchful waiting in advanced cancer patients showed that only 39% of patients reported discussing prognosis with the attending oncologist 33
Patient-related factors: However, even after the most honest communications regarding impending death, the patients may prefer to continue with active CT management rather than a symptom-based palliative approach, due to family or social pressures or their own unrealistic perception about disease status or benefits of CT. 34 In a study with cancer patients undergoing active treatment, one-third of them reported they did not believe that treatment was not curative despite they received such information. 35 Desperate patients and families may feel that doing something is better than doing nothing and may also associate “palliative care” or “hospice care” with abandonment. Previous studies have shown that many cancer patients are willing to undergo significant treatment-related toxicities despite little chance of benefit in survival. 36
Given that all these factors are often multifaceted, patients continue to receive CT very near the EoL, sometimes inappropriately. This inappropriate use of CT in the palliative care setting may have important negative consequences not only for patients but also for health care systems. CT and RT administrations are not the only procedures costly. It is necessary to take into account the percentage of different procedures, such as X-ray, scans, magnetic resonance imaging, as well as laboratory tests or additional supportive care products (e.g. blood products, CSFs, etc.) involved in using CT near EoL. In the present study, more than one-third of patients (39.1%) required the use of additional supportive care during their last line of palliative CT and about half of the patients (49.7%) required reduced doses or even discontinuation drugs from their CT regimen due to the toxic adverse effects derived from the treatment.
Integration of a palliative care services into standard outpatient oncology care is critical. According to the literature, the integration of specialized palliative care to standard oncology treatment significantly reduced aggressiveness of EoL care and improved patient QoL.37,38 Thus, hospice is commonly considered to be high-value, patient-centered care. In this study, 49.9% of patients were referred to specialized PCU before death, below the reference value established by Earle et al. (>55%). Furthermore, it was notable that 8.4% of patients referred to the PCU died within 72h after referral, above the 8% reference limit proposed by Earle et al., which means that patients are referred to palliative care very late in the course of the disease.
Our findings highlight the need to develop a model of early integration of palliative care services into standard outpatient oncology care since the incorporation of early specialized palliative care may reduce the risk of receiving CT during the final 2 weeks of life. 39 In 2016, ASCO recommended that patients with advanced cancer should receive dedicated palliative care services early in the disease course (within 8 weeks of diagnosis) concurrent with active treatment. 7 Despite these recommendations, patients are still referred to palliative care very near to EoL.
Limitations
The main limitation of this study is its retrospective design so confounding bias may exist.
Second, given the nature of the register, only patients who died in the hospital were included in the study. Patients who died at home or in nursing homes could not be included. Maybe if all deceased cancer patients had been included, the percentage in our study would be noticeably lower. However, it should be noted that in Spain around 65% of cancer patients die in hospitals.26,27
Third, we included only patients with solid tumors, hematologic malignancies were excluded. However, this is not necessarily a limitation because these patient groups could be approached very differently.
On the other hand, the study sample is just from one hospital site. Because patient’s characteristics, practice patterns, and resource availability may differ from other oncology settings, the generalization of the results is limited. For this reason, starting to systematically measure these indicators should be imperative because this evaluation would help us to compare health care centers and promote improvement strategies centered on patient care.
Despite the aforementioned limitations, one of the strengths of this study are that analyzes real-world clinical data of nonselected patients who are representative of the care offered to cancer patients at the EoL.
Conclusion
Prevalence of the use of CT near EoL in our cohort was higher than the value of the quality standard established by Earle et al. Similarly, the rate of ER visits and hospitalizations during the last month of life were also above these reference limits. According to the criteria by Earle et al., cancer patient care at EoL in our institution can be considered overly aggressive and this overtreatment could represent a generalized phenomenon.
Inappropriate use of CT in the palliative care setting may have important negative consequences both for patients and the health care system. The main consequence for the patients is the risk of being administered a useless, toxic, and potentially life-threatening treatment, actually resulting in a substantial worsening of the QoL. The major consequences for the health care system are the risk of wasting resources that might be efficiently assigned elsewhere.
Early integration of a palliative care services into standard outpatient oncology care is critical to reduce aggressiveness of EoL care and improve patient QoL.
Footnotes
Acknowledgments
The author would like to thank Andrés Blanco Hortas (Epidemiology Department, FIDIS, Hospital Lucus Augusti, Lugo, Spain) for his statistical assistance.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Ethics approval and consent to participate
The study was conducted in accordance with the ethical principles of the Declaration of Helsinki and consistent with Good Clinical Practice guidelines. The study protocol was approved by the Ethics Committee for investigation with medicinal products of Galicia (Ref 2021/048). Due to the retrospective nature of the study and that all patients were deceased, written informed consent was not required.
Data availability
Data of this study are available upon request to the corresponding author.