
Abstract
Introduction
The efficacy of immune checkpoint inhibitors (ICIs) against malignant melanoma and numerously solid tumors has been demonstrated in several clinical studies. The incidence of immune-related adverse effects (irAEs) has increased after the rapidly expanding indications and clinical applications of ICIs. We present a case of nivolumab and ipilimumab-induced encephalitis with rapidly worsening consciousness and full recovery following ICIs suspension and high-dose steroid coupled with intravenous immunoglobulin (IVIG).
Case Report
A 67-year-old woman was diagnosed with stage 4 BRAF wild malignant melanoma with metastasis to the axillary and mediastinal lymph nodes. Beyond progression with dacarbazine, ipilimumab and nivolumab combination were administered at the second-line treatment of metastatic setting. A week after the first cycle patient was reported to have a fever of more than 38°C. Subacute cognitive impairment including mild changes in behavior was reported on the third day of fever. She suddenly developed confusion, dysarthria, and motor dysfunction a few days later. Due to the altered mental status accompanied by fever, lumbar puncture was performed with a pre-diagnosis of encephalitis, meningitis, and leptomeningeal carcinomatosis.
Management & Outcome
After excluding viral and autoimmune encephalitis, high-dose methylprednisolone was administered in addition to IVIG for 5 days with the diagnosis of immunotherapy-related encephalitis according to the recommendations for the management of irAEs. On the second day of the treatment patient's neurological status improved gradually.
Discussion
Being aware of symptoms of serious neurological irAEs associated with ICIs can prevent complications and improve survival.
Introduction
Immune checkpoint inhibitors (ICIs) have been widely used to treat various advanced malignancies.1–3 However, they can cause numerous immune-related adverse effects (irAEs) induced by T-cell activation. 4 The overall incidence of neurological complications has been reported in 6% with PD-1 inhibitors, 3.8% for CTLA-4 inhibitors, and 12% for combination therapy. 5 ICIs-induced encephalitis occurs in 0.1% to 0.2% of patients within weeks after ICIs initiation and has non-specific changes on imaging. We present a case of nivolumab and ipilimumab-induced encephalitis with rapidly worsening consciousness and full recovery following ICIs suspension and high-dose steroid coupled with intravenous immunoglobulin (IVIG).
Case report
A 67-year-old woman was diagnosed with stage 4 BRAF wild left forearm localized cutaneous malignant melanoma with metastasis to the axillary and mediastinal lymph nodes. Beyond progression with dacarbazine as first-line therapy, ipilimumab (3 mg/kg every 3 weeks) and nivolumab (1 mg/kg every 3 weeks) combination were administered at the second-line treatment in the metastatic setting. A week after the first cycle of the nivolumab + ipilimumab combination patient was reported to have a fever of more than 38°C. Since the patient did not have a source of infection at the first assessment, she was hospitalized for the examination of fever etiology. Laboratory examination on the day of hospitalization showed that the C-reactive protein level was increased but procalcitonin was within the normal range. Empirical antibiotic treatment was initiated because of continuous fever. Bacterial growth was not detected in blood and urine cultures. Echocardiography did not suggest infective endocarditis. Computed tomography of the chest, abdomen, and pelvis showed no source of infection.
Subacute cognitive impairment including mild changes in behavior was reported on the third day of hospitalization. A few days later she suddenly developed confusion, dysarthria, and motor dysfunction. One day after the onset of confusion she had no response to verbal stimulus and only eye-opening and flexor response to pain (Glasgow Coma Scale (GCS) 6). She was electively intubated. Brain metastases and acute vascular lesions were excluded with brain magnetic resonance imaging (Figure 1). Due to the altered mental status accompanied by fever, lumbar puncture was performed with the pre-diagnosis of encephalitis, meningitis, and leptomeningeal carcinomatosis. Cerebrospinal fluid (CSF) opening pressure was normal. CSF revealed low glucose, elevated protein, lymphocyte levels, and no malignant cells. Laboratory parameters of the patient are given in Table 1. Acyclovir was administered until polymerase chain reaction (PCR) results were obtained for viral meningitis. There was no bacterial growth in the CSF culture, and cytomegalovirus and herpes simplex virus PCR tests were also negative. The autoimmune encephalitis panel was negative. The electroencephalogram showed no evidence of seizure activity. After excluding viral and autoimmune encephalitis, high-dose intravenous methylprednisolone (2 mg/kg per day) was administered in addition to IVIG 0.4 g/kg per day for 5 days with the diagnosis of immunotherapy-related encephalitis according to the recommendations for the management of irAE. 6 On the second day of the treatment patient's neurological status improved gradually (GCS:15) and she was extubated. State of consciousness and cognitive functions improved. Following five days of high-dose steroid, it was continued for one more month, with a dose reduction plan. She was discharged with a normal neurological examination. Fifteen days after discharge, she had no neurological symptoms in the outpatient clinic control. Immunotherapy was completely discontinued and single-agent paclitaxel was planned for the patient as a third-line treatment.
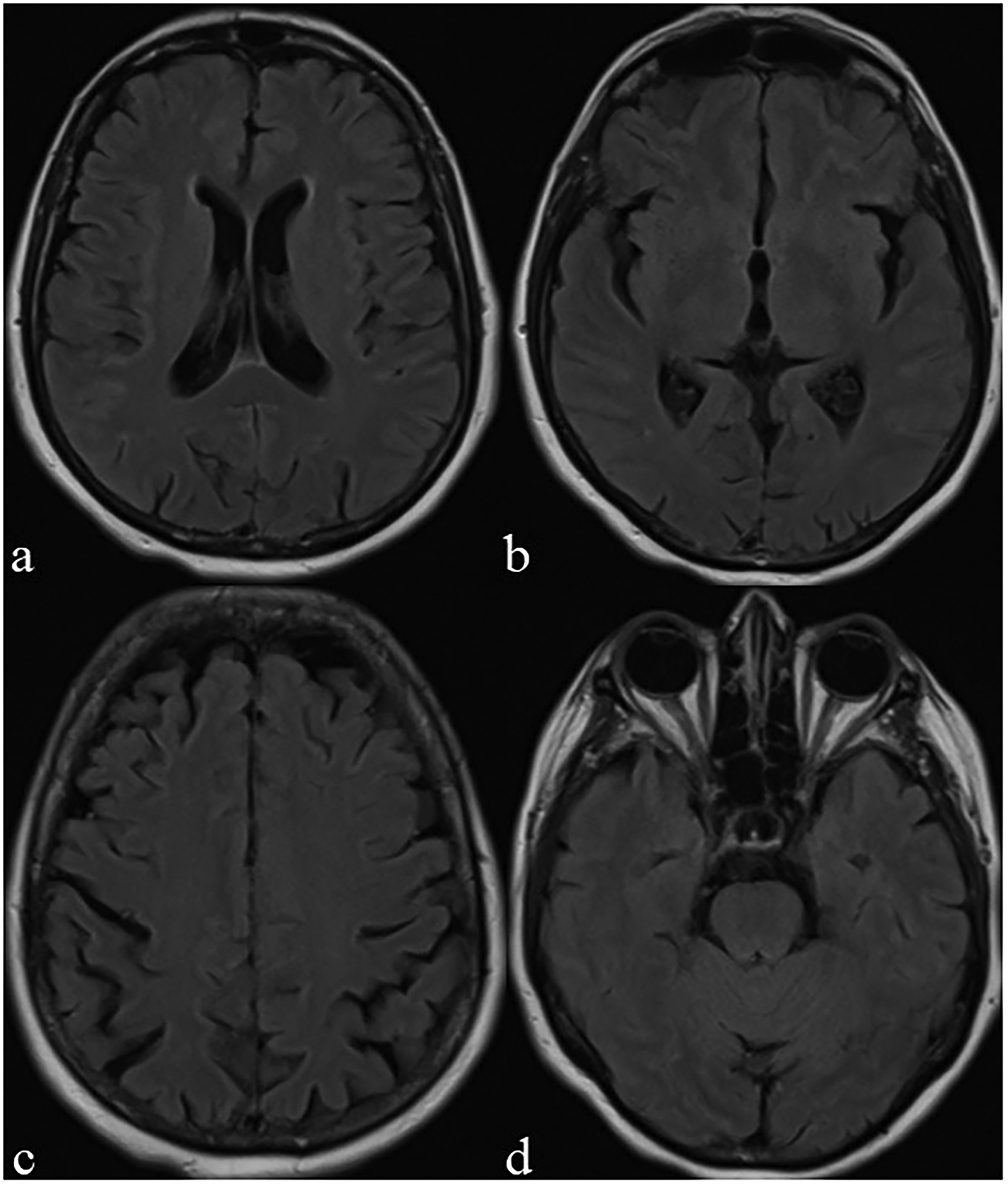
Axial T2-FLAIR magnetic resonance images showing no evidence of intra or extra parenchymal lesions.
Laboratory parameters of the patient.
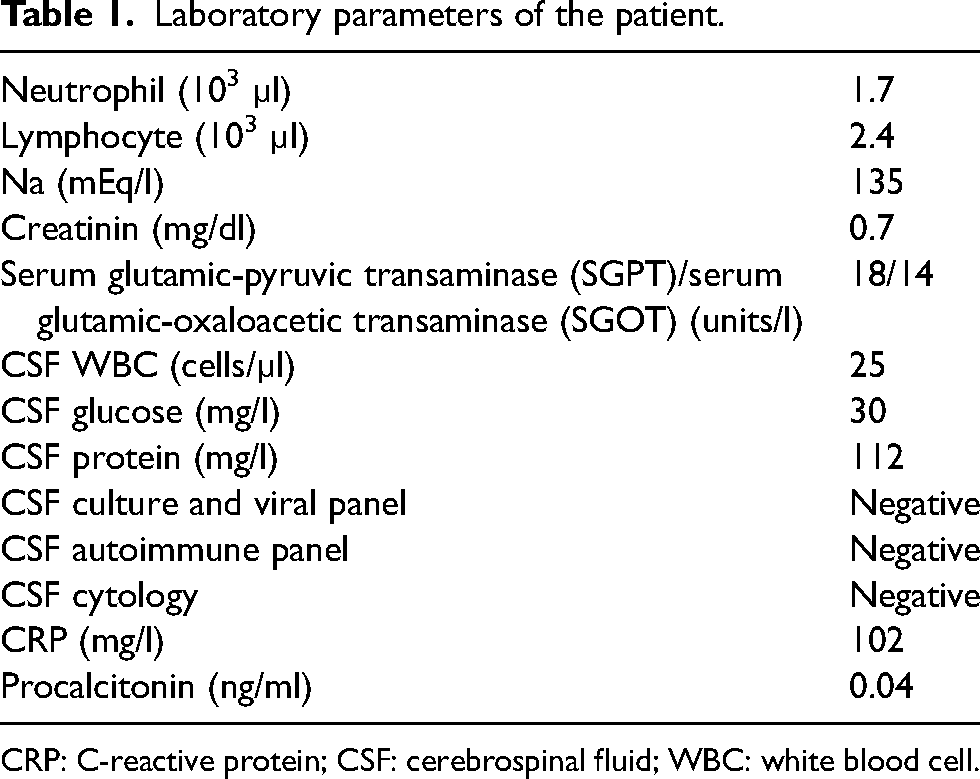
CRP: C-reactive protein; CSF: cerebrospinal fluid; WBC: white blood cell.
Management and outcome
We described a case of seronegative encephalitis following treatment with nivolumab and ipilimumab in a patient with metastatic malignant melanoma. In our case report, the interval between administration of ICIs and neurological symptoms was <5 weeks, it was consistent with similar reports. Due to severe symptoms leading to intubation, our patient was administered not only high-dose methylprednisolone but also IVIG in the first-line treatment. In previous case reports, IVIG was added to pulse steroids in cases that do not respond to high-dose steroids. In our patient, rapid response to treatment was shorter than in the previous case reports because we administered both treatment options at the same time, not sequentially. If our patient did not respond to steroid and IVIG, plasmapheresis or rituximab treatment would have been administered as the next line treatment. In the literature, rapid recovery was reported with rituximab in cases of encephalitis that do not have neurological improvement with high-dose steroids and IVIG. 7 In conclusion, prompt recognition of neurological irEAs can prevent fatal complications and mortality.
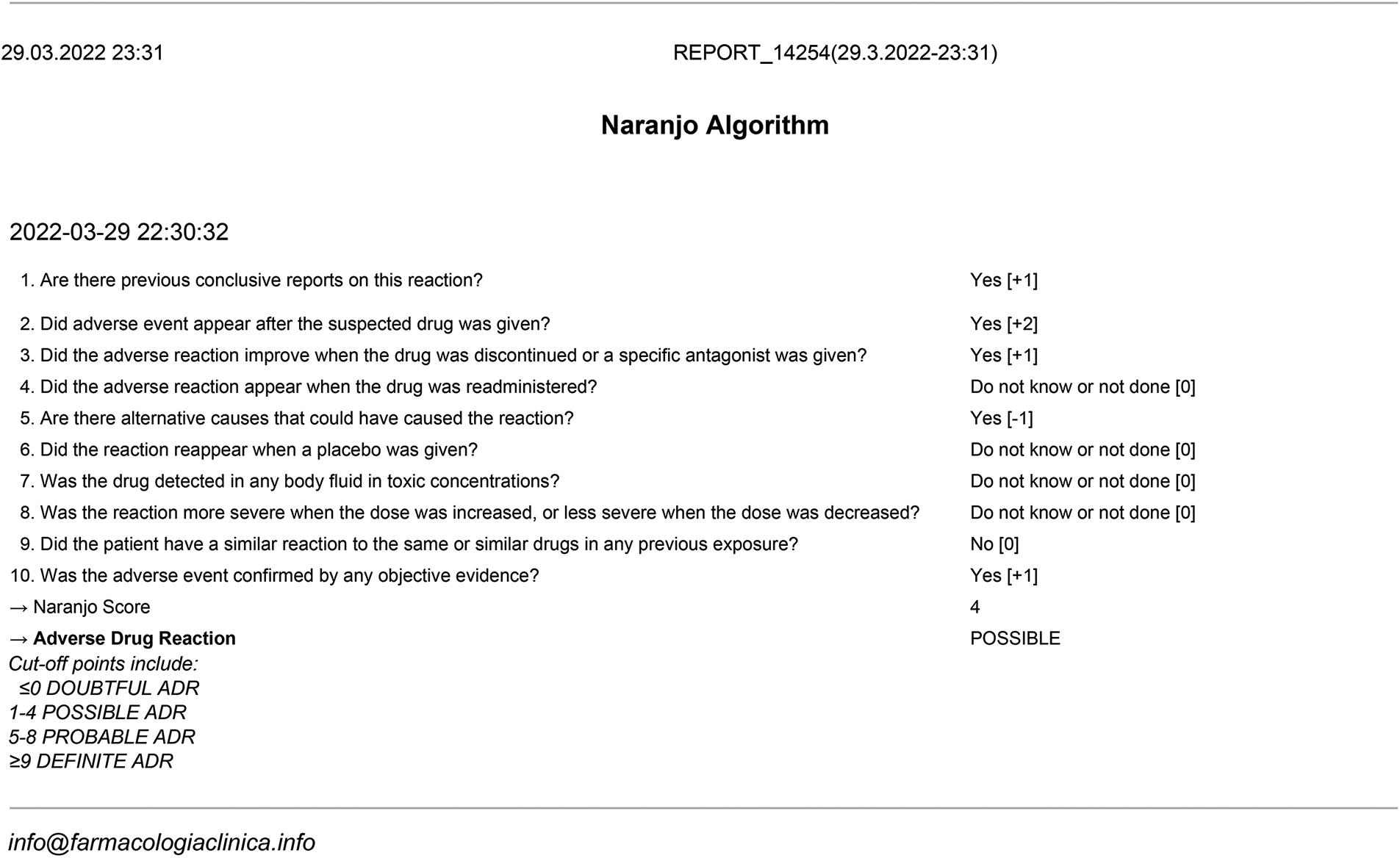
Final Naranjo score: 4 (see Naranjo Algorithm).
Discussion
The efficacy of ICIs against malignant melanoma and numerously solid tumors has been demonstrated in several clinical studies. The incidence of irAEs has increased after the rapidly expanding indications and clinical applications of ICIs. Nivolumab–ipilimumab combination therapy leads to more neurological complications than ICIs monotherapy. Most irAEs occur early in the first few cycles of treatment. Multiple alternative etiologies must be ruled out such as viral or bacterial meningitis and encephalitis, paraneoplastic syndromes, leptomeningeal carcinomatosis, cranial metastases, and cerebrovascular events. Delays in treatment may occur due to the difficulties in establishing an accurate diagnosis. The mechanism of ICIs related neurological adverse effects was not clear but several hypotheses are being suggested. Due to the cross-reactivity between tumor cells and normal cells, activated T-cells attack healthy tissues. One of the hypothesis is that ICIs can increase the level of preexisting autoantibodies accordingly ICIs lead to relapse of autoimmune diseases. 8 The clinical presentation of the encephalitis is quite heterogeneous and non-specific. Memory problems, disorientation, impaired attention, headache, confusional state, and seizures can occur. With most symptoms of nivolumab-induced encephalitis being non-specific, one of the remarkable risk factor is the short term between symptom initiation and administration of ICIs therapy. Neurological side effects associated with ICIs are diagnosed by excluding metastases, infections, paraneoplastic syndromes, and metabolic conditions.
Management guidelines of ICIs related adverse effects are based on the severity of symptoms. 6 The symptom severity of ICIs related adverse effects has a wide range from grade 1 to grade 4. While grade 1 represents mild symptoms, grade 4 represents severe symptoms such as confusion. For grade 1, continue ICIs but if symptoms worsen treat as grades 2 to 4. For grade 2, withhold dose, confer to a neurologist. For grades 3 to 4, permanently discontinue immunotherapy. Initial treatment of ICIs related encephalitis was high dose methylprednisolone. If severe or progressive symptoms present, pulse corticosteroids (methylprednisolone 1g daily for 3 or 5 days) plus IVIG 2 g/kg for 5 days can be administered.
Footnotes
Authors’ contributions
All authors meet the ICMJE authorship criteria. All authors have seen and approved the final version of the manuscript and contributed significantly to the work. Material preparation, data collection, and analysis were performed by KBY, OS, AU, and OY. The first draft of the manuscript was written by KBY and OS, and all authors commented on previous versions of the manuscript. All authors read and approved the final manuscript.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Informed consent
Written informed consent for patient information was obtained.