
Abstract
Introduction
Fludarabine, a purine analog, is getting more attention with the increasing use of reduced intensive conditioning regimens in allogeneic hematopoietic stem cell transplantation (allo-HSCT). The side effect of bradycardia was observed in only a few cases reported in the literature. In clinical practice, bradycardia can be asymptomatic or cause syncope and cardiac arrest. This study aimed to evaluate the bradycardia side effect of fludarabine used in the conditioning regimen in allo-HSCT recipients and to increase awareness of this issue.
Methods
This retrospective study included 73 patients who received fludarabine in the allo-HSCT conditioning regimen between January 2015 and January 2021. Patients with and without bradycardia were compared regarding demographic data, allo-HSCT characteristics, electrolyte values, fludarabine administration dose and duration, and survival. Univariate and multivariate analyzes were performed to evaluate independent predictors for fludarabine-induced bradycardia.
Results
Fludarabine administration doses and days were higher in the bradycardia group, but no statistically significant difference was observed. In the multivariate analysis, age was the only independent predictor of fludarabine-induced bradycardia (odds ratio (OR) 0.93, 95% confidence interval (CI): 0.89–0.98, p = 0.007). The median age in the group with bradycardia was 19 years younger than those without bradycardia (34 (19–49) vs 53 (19–69), p = 0.005). In 11 (84.6%) of the patients who had bradycardia, bradycardia improved with the discontinuation of fludarabine alone, but atropine was administered in 2 (15.4%) patients.
Conclusion
Age was the only independent predictor of fludarabine-induced bradycardia; therefore, close heart rate monitoring is recommended during fludarabine administration, especially in younger patients.
Introduction
Fludarabine is a chemoimmunotherapeutic agent, a synthetic nucleoside analog used in many hematological diseases. 1 It has multiple mechanisms of action that can result in DNA strand breaks, phosphorylated p53 accumulation in the cell, and apoptosis, and also inhibits DNA repair.2,3 The frequency of fludarabine use is increasing, as it can be better tolerated with the increasing use of reduced intensive conditioning in allogeneic hematopoietic stem cell transplantation (allo-HSCT) in recent years.4,5
The most common side effects of fludarabine are infections and myelosuppression, such as anemia and thrombocytopenia. However, fludarabine-related cardiovascular side effects are not frequent, but congestive heart failure and left ventricular failure have been reported.6–8 Fludarabine-induced bradycardia was reported with only a few cases.9,10 While bradycardia can be asymptomatic, it presents with a wide range of symptoms, from general symptoms such as fatigue and dizziness to neurological symptoms such as syncope and even cardiac arrest. 11
In the present study, we aimed to examine the bradycardia side effect of fludarabine used in the conditioning regimen, which can be ignored and may lead to significant results in our allo-HSCT patients. The primary aim is to examine the characteristics of patients who develop bradycardia due to fludarabine. The secondary aim is to examine whether patients who develop bradycardia affect allo-HSCT results and survival.
Methods
Patients and study design
Patients who underwent allo-HSCT between January 2015 and January 2021 in the Bone Marrow Transplantation Unit of Erciyes University Şahinur Dedeman Hospital, which has Joint Accreditation Committee of ISCT and EBMT (JACIE) accreditation (ID number: 649, CIC number: 627), were included in this retrospective study. A total of 73 patients who used fludarabine in the conditioning regimen were included in the study. The patients were compared in two groups: developing (n = 13) and nondeveloping (n = 60) bradycardia after fludarabine. These two groups were compared in terms of age, gender, primary diagnosis, and transplant characteristics followed by the day and number of fludarabine infusions, total dose, electrolyte values, and electrocardiographic (ECG) characteristics.
All patients signed a written informed consent. All ethical procedures and standards were carried out in accordance with the 1975 Helsinki Declaration. The study was approved by the Erciyes University Clinical Research Ethics Committee (approval number: 2021/700).
Evaluation of bradycardia
Sinus bradycardia is a heart rate that generates from the sinus node and has a rate of <60 bpm. 11 Chemotherapy-induced bradycardia occurs during or 24 h after drug administration. 12 Therefore, we defined fludarabine-induced bradycardia as a heart rate above 60 beats per minute (bpm) before fludarabine administration and a decrease below 60 bpm within the first 24 h during or after fludarabine administration. Fludarabine administration time was 30 or 60 min depending on the conditioning regimen. During this time, all patients were monitored as continiously, but were then intermittently monitored. Echocardiography and 12-leads ECG were performed in all our patients before allo-HSCT. A cardiologist performed a cardiological evaluation, and consent was obtained. The Naranjo Adverse Drug Reaction Probability Score Scale was used to assess whether there is a causal relationship between fludarabine and bradycardia. 13
Statistical analysis
The Kolmogorov–Smirnov test was used to assess the distribution of continuous variables. The Mann–Whitney U test was used to compare nonparametric data; Student's t-test was used to compare parametric data. Parametric variables were expressed as mean ± standard deviation, and nonparametric variables were expressed as median (range). Chi-square or Fisher's exact test was used to compare categorical data.
Overall survival (OS) was measured as the time from allo-HSCT to death regardless of any cause. Progression-free survival (PFS) was defined as the time from allo-HSCT to relapse. Univariate analyses were performed to assess for independent predictors for fludarabine-induced bradycardia. All variables with differing significance were included in multivariate analyses and deleted step wisely. The data were analyzed using the Statistical Package for the Social Sciences (SPSS) for Windows (release 25.0; SPSS Inc., Chicago, IL, USA). A two-tailed p-value of <0.05 was considered statistically significant in all tests.
Results
The median age of the patients in the fludarabine with bradycardia group was 34 (19–49) years, albeit the patients in the fludarabine without bradycardia group were 53 (19–69) years (p = 0.005). While 54% (n = 7) of the patients in the bradycardia group were female, 43% (n = 26) of the patients in the other group were female (p = 0.45). The most common primary diagnosis in both groups was acute myeloid leukemia. The essential characteristics of patients and transplantation are described in Table 1.
The essential characteristics of patients and transplantation.
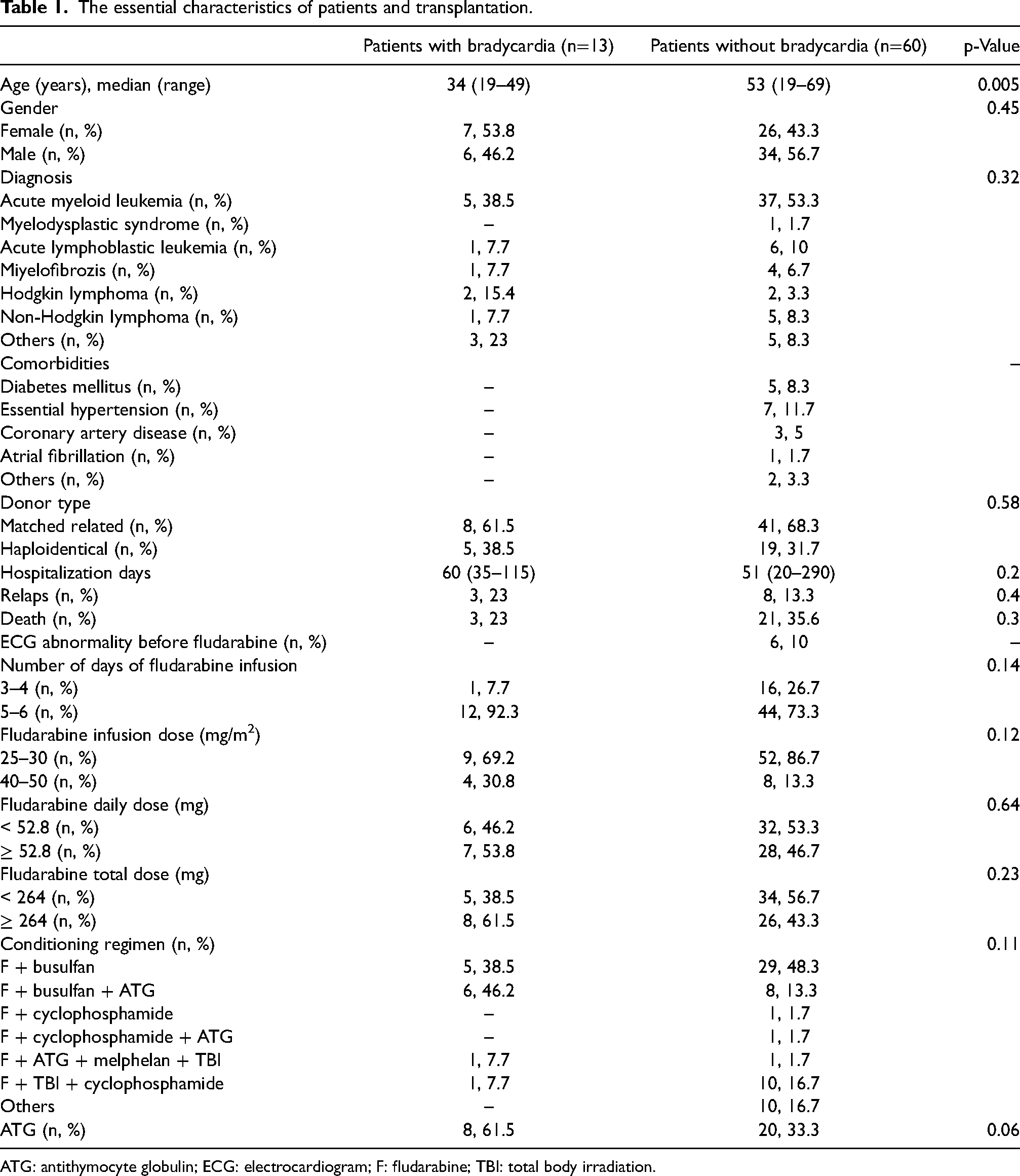
ATG: antithymocyte globulin; ECG: electrocardiogram; F: fludarabine; TBI: total body irradiation.
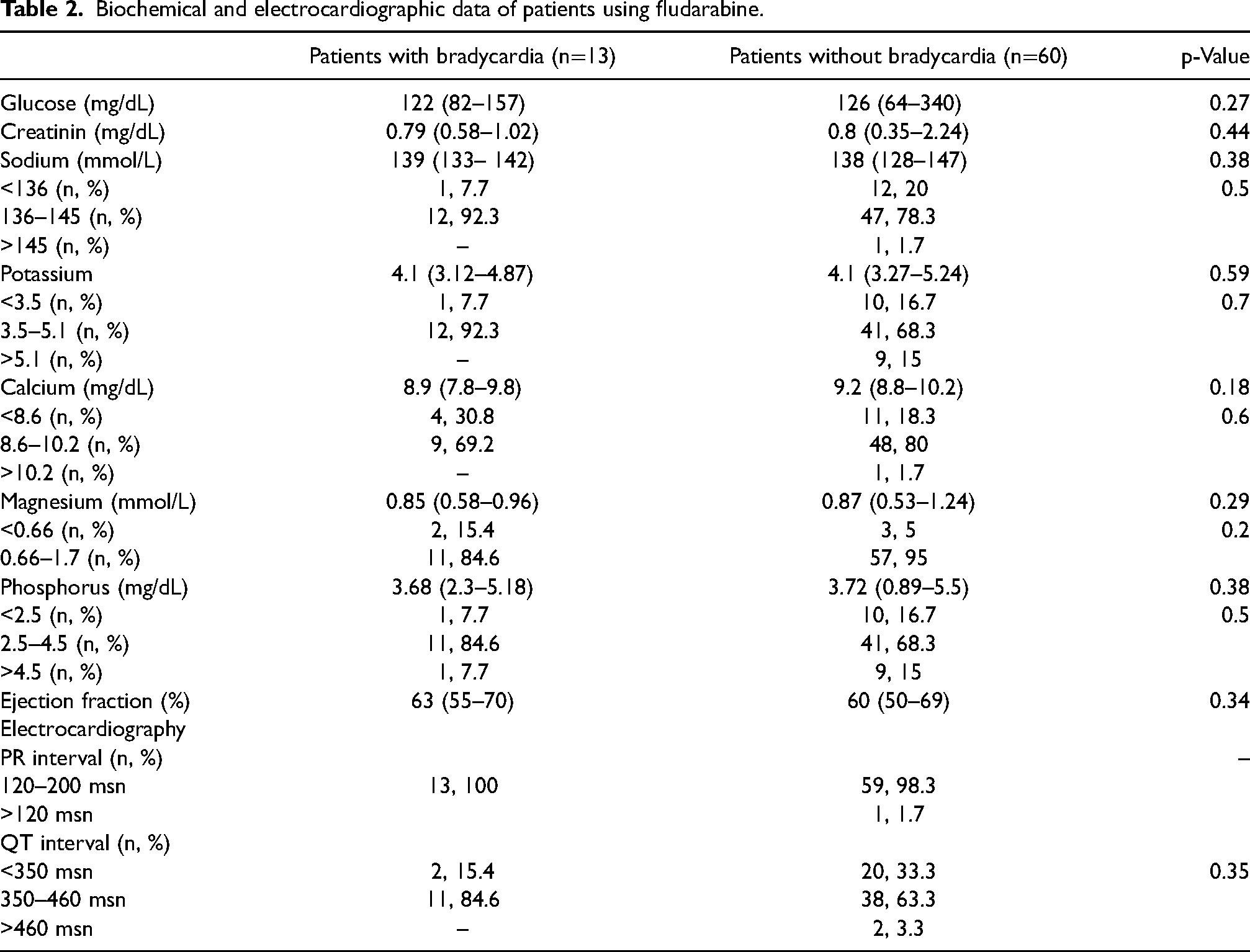
The median daily dose of fludarabine was 52.8 (30–97.6) mg. In the bradycardia group, there were 7 (54%) patients who received fludarabine above 52.8 mg daily, while 28 (47%) patients were in the other group (p = 0.64). The median fludarabine total dose was 264 (135–488) mg. Those who received more than the median fludarabine total dose were more in the bradycardia group, but no statistically significant difference was observed (62% (n = 8) vs. 43% (n = 26), p = 0.23). Fludarabine infusion days and doses are detailed in Table 1. Electrolyte and other biochemical values are described in Table 2 (p < 0.05 in all).
Biochemical and electrocardiographic data of patients using fludarabine.
Bradycardia was observed in 17.8% (n = 13) of patients who used fludarabine in the conditioning regimen. The median Naranjo Adverse Drug Reaction Probability Score was 7 (6–9), indicating the probable reaction. The median time to develop bradycardia after fludarabine administration was 25 (17–40) minutes. No pathological findings other than sinus bradycardia were observed in the ECG, and all patients had normal fever, blood pressure, partial oxygen saturation, and respiratory rate. Three patients also used other drugs that could cause bradycardia side effects. Of these drugs, one patient used metoclopramide and fentanyl, another used voriconazole, and the other patient used amlodipine. However, these drugs were also used in the days before bradycardia developed. Bradycardia improved in 11 (84.6%) patients after fludarabine administration was terminated. Bradycardia requiring treatment indication was observed in 2 (15.8%) patients. One of the patients was male, and the other was female. The male patient, 29 years old and diagnosed with acute lymphoblastic leukemia, underwent haploidentical allo-HSCT. The female patient, 24 years old, was diagnosed with Hodgkin lymphoma and underwent allo-HSCT from a matched sibling donor. In these two patients, bradycardia improved with atropine administration.
In the univariate regression analysis evaluating the factors that may affect fludarabine-induced bradycardia, antithymocte globulin, fludarabine total dose, and age were observed as independent factors (odds ratio (OR) 3.45, 95% confidence interval (CI): 0.99–11.9, p = 0.05; OR 1.01, 95% CI: 1.0 −1.02, p = 0.03; and OR 0.94, 95% CI: 0.90–0.98, p = 0.008, respectively). However, in the multivariate analysis, age was the only independent predictor of fludarabine-induced bradycardia (OR 0.93, 95% CI: 0.89–0.98, p = 0.007) (Table 3).
Univariate and multivariate regression analysis of factors affecting fludarabine-induced bradycardia.
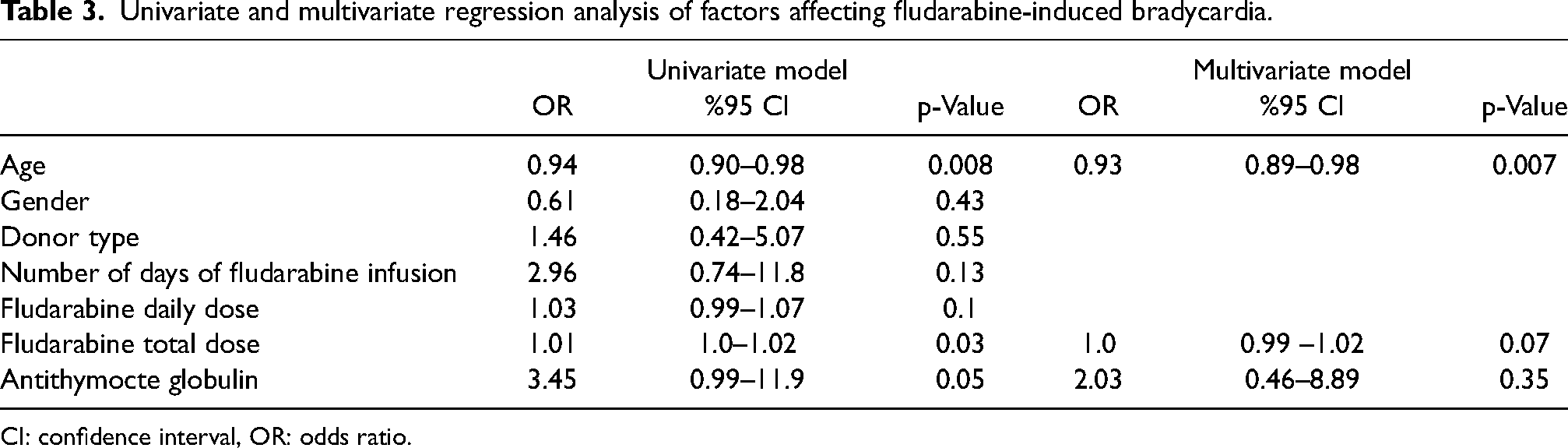
CI: confidence interval, OR: odds ratio.
The median follow-up time after allo-HSCT was 20.8 months (3.4–66.6), and the mean OS was 43.4 ± 3.5 months (95% CI: 36.6–59.7). The mean OS was 47.03 ± 6.46 (95% CI: 34.37–59.70) months in the bradycardia group and 42.7 ± 3.82 (95% CI: 35.22–50.19) months in the other group (p = 0.38, log-rank test) (Figure 1). While OS at 1, 2, and 5 years was 100%, 87.5%, and 54.7%, respectively, in the bradycardia group, it was 87.3%, 64.1%, and 41.8%, respectively, in the group without bradycardia. The mean PFS was 56.88 ± 3.4 (95% CI: 50.21–63.56) months in the group without bradycardia and 46.33 ± 7 (95% CI: 32.61–60.05) months in the bradycardia group (p = 0.39, log-rank test) (Figure 2).
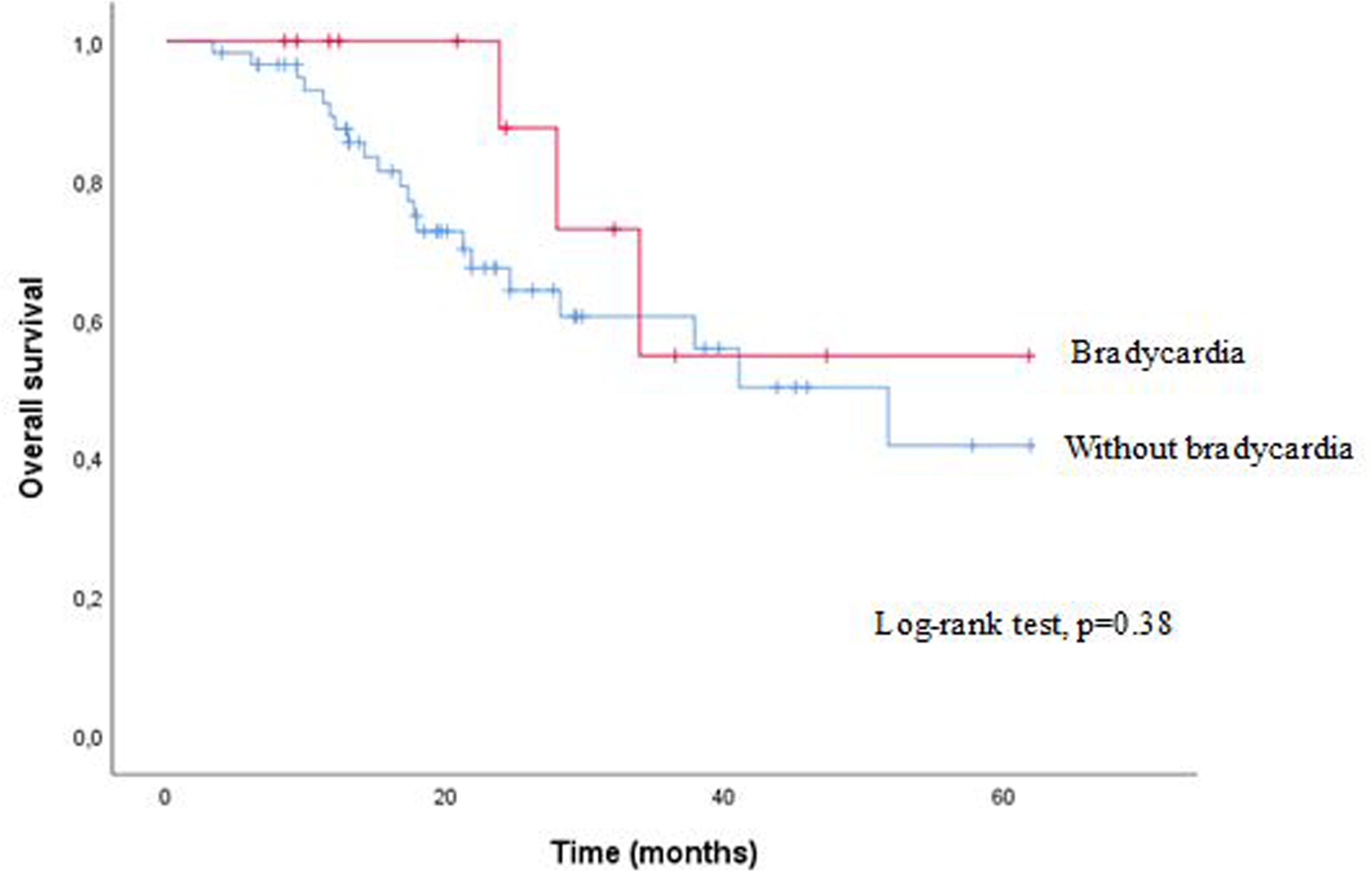
Overall survival in patients using fludarabine with and without bradycardia.
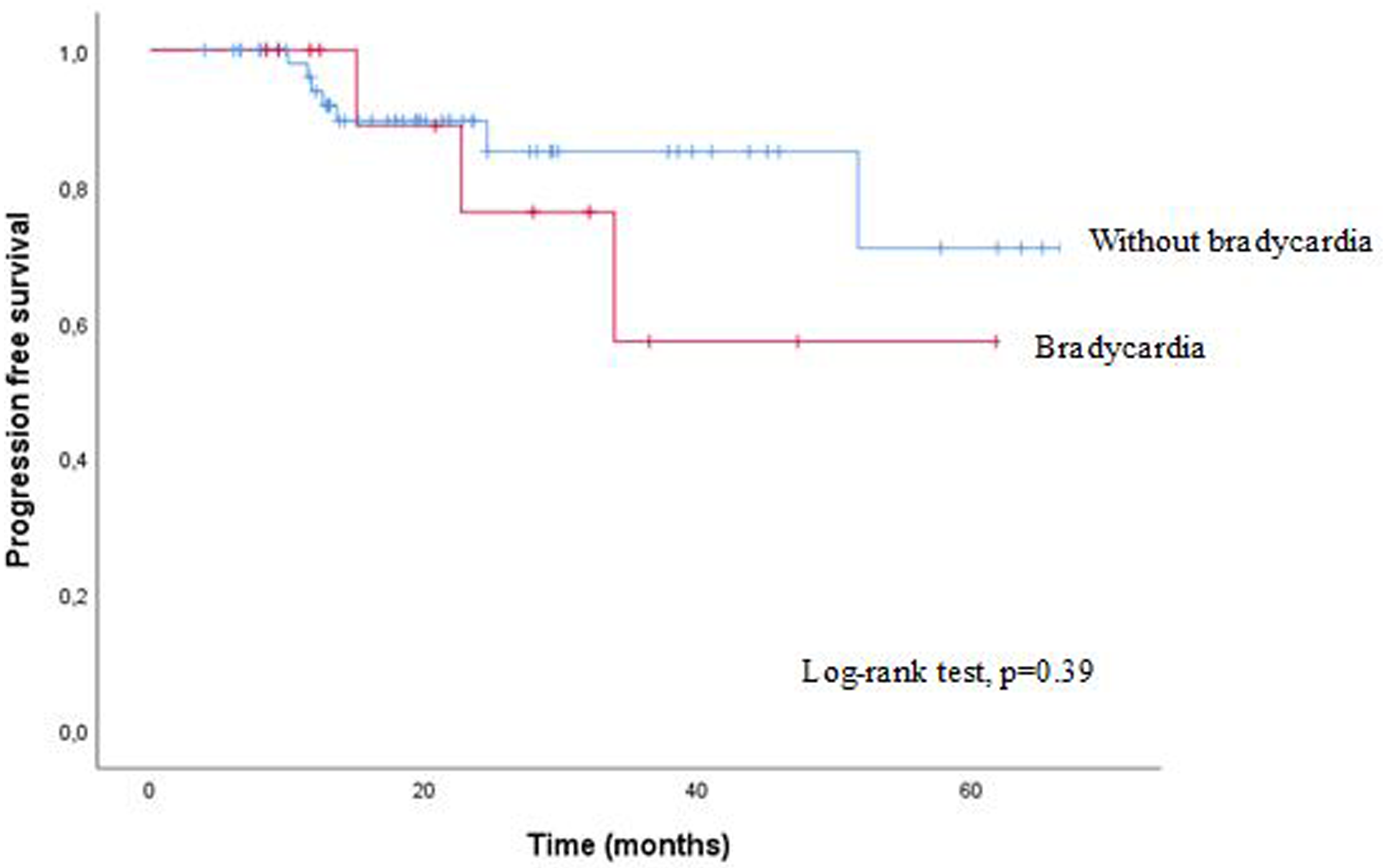
Progression-free survival in patients using fludarabine with and without bradycardia.
Discussion
Chemotherapy-induced bradycardia may occur by several damage mechanisms. 12 Stimulation of the parasympathetic system, desensitization of adrenergic receptors, release of vasoactive molecules during chemotherapy administration, electrolyte disturbances, transient myocardial ischemia due to coronary vasospasm, the effect of abnormal intracellular calcium on the sinoatrial node (SAN), and the direct effect of chemotherapy itself or its metabolite on SAN cells are among these mechanisms.14–17 Fludarabine is a nucleoside prodrug and has an intermediate called fluoroadenosine. Fluoroadenosine might have electrophysiological effects similar to those of adenosine. 10 Adenosine is a signaling molecule and activates the acetylcholine-gated potassium current that slows SAN pacemaker rate, inhibits I(f), and reduces the rate of spontaneous depolarization of SAN cells, indirectly preventing the increase of I(Ca,L) adenylyl cyclase activity and intracellular cyclic adenosine monophosphate (cAMP) levels and reduces norepinephrine release by activating presynaptic purinergic receptors located in sympathetic nerve endings.17–19
Fludarabine-induced bradycardia was previously reported in a patient with refractory leukemia. 9 Subsequently, Philip et al. 10 evaluated 10 patients’ ECG data using fludarabine in the conditioning regimen. In this case series, a mean heart rate reduction of 18.9 bpm was observed after fludarabine administration in allo-HSCT recipients. Bradycardia developed in 6 (60%) of the patients; this rate was 17.8% in our study.
The development of chemotherapy-induced bradycardia is multifactorial, but the risk factors are still unclear as it is rarely observed. 14 In our study, the mean age of patients who developed bradycardia was 19 years younger than those who did not. Bradycardia is observed more frequently in elderly patients. 20 The age of the patient with refractory leukemia who developed bradycardia after fludarabine was 22 years old. 9 In our study, the ages of patients who developed bradycardia requiring atropine administration were 24 and 29 years. Severe distress may alter autonomic nervous system control in patients with malignancy. 14 Young patients have more stress during the allo-HSCT period than the elderly, which may explain why fludarabine and its intermediate fluoroadenosine cause more bradycardia in younger patients. 21
Chemotherapy-induced bradycardia usually develops independently of the dose. 11 In our study, the fludarabine dose was higher in the bradycardia group, but no statistically significant difference was observed. Rackley et al. observed the development of bradycardia in eight allo-HSCT recipients and improved bradycardia after immunosuppressive therapy. 22 These results stated that bradycardia was associated with cardiac graft versus host disease (GVHD). Since bradycardia was evaluated in our study's conditioning regimen administration time, there was no development of GVHD. However, no statistically significant difference was observed between the two groups, regarding the allo-HSCT results. There is only one study in the literature that contradicts our results. This study conducted 24h ECG Holter monitoring for patients who underwent HSCT. 23 Administration of fludarabine was an independent risk factor for increased heart rate in 24h ECG Holter monitoring. However, in this study, 24h ECG Holter monitoring was performed not during fludarabine administration but after the conditioning regimen and HSCT administration. Therefore, heart rate assessment was performed at different time points.
The strength of our study is that fludarabine, which is increasingly used in the conditioning regimen, is the first to highlight bradycardia. This side effect is that can be overlooked and may have significant consequences for susceptible allo-HSCT recipients. There are some limitations in our study. Firstly, it was fluoroadenosine, an intermediate of fludarabine, which we attributed to bradycardia caused by fludarabine. Therefore, measuring serum drug levels of fludarabine and fluoroadenosine would be more appropriate to support our hypothesis. Another limitation is that vital measurements are performed intermittently in our patients. Evaluation of 24h ECG Holter monitoring will be more helpful in these patients. Another limitation is that although cardiologists consented to allo-HSCT by cardiac examination for each patient, most of our patients had previously used several cardiotoxic drugs. The last limitation is that our study was retrospective and was a single-center experience.
Conclusion
Bradycardia was observed in 17.8% of our patients who used fludarabine in the conditioning regimen. Age was the only independent predictor of the development of fludarabine-induced bradycardia. For this reason, it is recommended to monitor the heart rate more frequently and be careful regarding bradycardia development during fludarabine administration, especially in young patients. Although our results are promising, further studies evaluating the fludarabine intermediate fluoroadenosine are needed to support our results.
Footnotes
Author contribution
SÇ designed the study and wrote the manuscript. SÇ and ZTG performed the statistical analysis. AA and ŞET did the data managements. ŞET provided the clinical pharmacy information. MK and AÜ reviewed and all authors approved the final version of the manuscript.
Data availability statement
The data that support the findings of this study are available on request from the corresponding author. The data are not publicly available due to privacy or ethical restrictions.
Conflict of interest disclosure
The authors declare no competing interests.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Ethics approval statement
All patients signed written informed consent. All ethical procedures and standards were carried out following the 1975 Helsinki Declaration. The study was approved by Erciyes University Clinical Research Ethics Committee (approval number: 2021/700).
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.