
Abstract
Objective
We conducted a systematic review and meta-analysis aiming to assess the efficacy and safety of Nivolumab treatment in patients with newly diagnosed and recurrent glioblastoma multiforme (GBM).
Data sources
Our study followed the guidelines outlined in the preferred reporting items for systematic reviews and meta-analyses (PRISMA) recommendations. The protocol for this review can be found in the International Prospective Register of Systematic Reviews Database (CRD42022340071). We performed searches on the Medline, PubMed, Embase, Scopus, and Web of Science databases.
Data summary
A total of 545 studies were identified through our comprehensive search across the five databases (PubMed: 78, Embase: 82, Medline: 173, Scopus: 138, Web of Science: 74). After conducting a thorough analysis, our meta-analysis indicated that treatment with Nivolumab led to improved overall survival (OS) outcomes in newly diagnosed glioblastoma patients, as evidenced by a prolonged median OS based on trial data. However, there was no significant beneficial effect observed in terms of median progression-free survival (PFS), as well as OS at 6, 12, and 24 months. Furthermore, our results demonstrated no efficacy of Nivolumab in the treatment of recurrent GBM patients.
Conclusions
In conclusion, Nivolumab demonstrated promising results that warrant further investigation for its use in newly diagnosed glioblastoma patients. However, its effectiveness was not observed in the context of recurrent GBM.
Introduction
Gliomas are the most common type of brain tumors that originate from glial cells, including astrocytes, ependymal cells, and oligodendrocytes. Among gliomas, the most prevalent and aggressive type is glioblastoma multiforme (GBM), which is classified as a grade IV glioma according to the World Health Organization (WHO) classification of central nervous system (CNS) tumors. 1 GBM has a relatively high incidence, estimated at 2 to 3 cases per 100,000 individuals, although it has low rates of metastasis and affects approximately 0.4% to 0.5% of all patients. 2 The incidence of GBM tends to increase with age, with studies reporting the highest occurrence in the age group of 75 to 84 years old. Other risk factors, such as gender and race, also contribute to an increased risk for glioblastoma, with a higher prevalence observed in men and Caucasians. 3
The standard treatment for GBM initially involves surgery to remove as much of the tumor as possible. Following resection, radiotherapy sessions are conducted, typically consisting of 30 fractions (60 Gy), along with concurrent and adjuvant chemotherapy using temozolomide. 4 Despite significant advancements in treatment, the prognosis remains poor, with a median survival of approximately 12.1–14.6 months for newly diagnosed cases. Recurrent glioblastoma carries a prognosis of 14 to 16 months, with an overall 5-year survival rate of less than 10%. 5
GBM presents several challenges and barriers to treatment, including high infiltration, intertumor and intratumor heterogeneity, the blood–brain barrier (BBB), and an immunosuppressive microenvironment. In some cases, tumors are characterized by a lack of T cell infiltration, absence of tumor antigens, defects in antigen presentation, and a high accumulation of immunosuppressive cells. These factors can result in tumor resistance to immune checkpoint inhibitors and other treatments.6,7
Considering the immunosuppressive nature of glioblastoma, studies have shown that checkpoint inhibitors could potentially improve survival. Nivolumab, a human immunoglobulin G4 monoclonal antibody, specifically targets and inhibits programmed death-1 (PD-1).8,9 This anti-PD-1 therapy has been successfully used with significant effects in melanoma, renal cancer, hepatocellular carcinoma, and other tumors. However, the use of checkpoint inhibitors is associated with various adverse events, which can impact treatment adherence and safety.10–12
In light of the above information, we conducted a systematic review and meta-analysis to assess the efficacy and safety of Nivolumab treatment in patients with newly diagnosed and recurrent GBM.
Method
Search strategy
This systematic review with meta-analysis was conducted in accordance with the preferred reporting items for systematic reviews and meta-analyses (PRISMA) recommendations. 13 The purpose of this study was to evaluate the efficacy and safety of Nivolumab in the treatment of newly diagnosed and recurrent glioblastoma. To guide our search process, we formulated research questions using the PICO strategy. The research questions were as follows: “What is the efficacy of Nivolumab in the treatment of newly diagnosed and recurrent glioblastoma?” and “What is the safety profile of Nivolumab in the treatment of newly diagnosed and recurrent glioblastoma?” We conducted comprehensive searches in several databases including Medline, PubMed, Embase, Scopus, and Web of Science. The search strategy involved the use of the following keywords and their combinations: “high-grade glioma,” “glioblastoma,” “astrocytoma,” “GBM,” “Checkpoint Inhibitors,” “immunotherap*,” “nivolumab,” “PD-1,” and “anti-PD-1.” These keywords were combined using Boolean connectors such as “And,” “Or,” and “And Not” to refine the search results. The searches were conducted from May to June 2022, without any restrictions on language, publication date, or geographical location.
The protocol for this systematic review is registered in the International Prospective Register of Systematic Reviews Database (CRD42022340071).
Inclusion criteria
Randomized clinical trials studies, multi or single, center who used Nivolumab for the newly or recurrent GBM treatment, were selected. Furthermore, selected studies that complied all the criteria: (1) patients with newly or recurrent glioblastoma; (2) treatment with nivolumab alone plus some specific cytotoxic treatments; (3) two or more arms in cohort study; (4) reported outcomes of interest (overall survival [OS], progression-free survival [PFS], adverse events, and 6-month and 1-year OS); (5) ≥18 years old.
Data extraction
Titles and abstracts of potentially relevant studies were investigated by two investigators. When there were discrepancies between reviewers, a third investigator was consulted. We extracted the following data: author, study design, country, median age, sex, interventions, sample size and outcomes of interest. The outcomes of interest used were OS, PFS, and adverse events. When possible, the outcomes 6-month, 1-year and 2-year OS were extracted. To assess quality of studies in our systematic review and meta-analysis, the evaluation instrument (GRADE), was also used to provide support for rating the strength of recommendations. Criteria for this assessment will be study design, risk of bias and inconsistency. The quality of evidence will be characterized as high, moderate, low or very low, as recommended by Cochrane guidelines for randomized clinical trials (http://gradepro.org).
Statistical analysis
We analyzed all patients who started Nivolumab alone or plus some cytotoxic treatment, and were compared with Temozolomide, Bevacizumab or other cytotoxic treatment. The OS, PFS and adverse events of GBM patients were compared between the groups. We used Review Manager (version 5.3) software for statistical analysis, where for each study was established by Z test (p < 0.05) with 95% confidence intervals (CIs). The intensity of relationship between groups was presented in mean difference (MD) for continuous outcomes and relative risk (RR) for dichotomous outcomes. In order to visualize these results, we performed the Forest plot. To calculate the heterogeneity was used I2 statistic and Cochran’s Q test (Higgins & Thompson, 2002). A statistical test with a p-value less than 0.05 was considered significant. We calculated the pooled MD or RR using fixed-effects model (when P heterogeneity > 0.05 or I2 < 50%) and random-effects model (when P heterogeneity < 0.05 or I2 > 50%). Egger’s test and ROB2 was used to calculate and to detect bias in comparisons, using the metafor package and robvis package, respectively, in the R studio version 4.2.0. In addition, funnel plot graphs were generated, performing a qualitative assessment of which asymmetries suggest the presence of publication bias.
Results
Search results
During the initial search in the five databases (PubMed: 78, Embase: 82, Medline: 173, Scopus: 138, Web of Science: 74), a total of 545 studies were identified. After analyzing the titles and abstracts of these studies, 522 articles were determined to be ineligible and were subsequently excluded. Additionally, 10 duplicate studies were removed, leaving a total of 13 potentially eligible studies.
After conducting a thorough review of the methodologies employed in these 13 studies, 7 of them were found to not meet the inclusion criteria and were therefore excluded. Following this process, a final selection of 6 studies was included in this review and subsequent meta-analysis. The included studies are as follows: Duerinck et al. (2021), Omuro et al. (2018), Omuro et al. (2022), Reardon et al. (2020), Sampson et al. (2016), and Weller et al. (2021). For a visual representation of the study selection process, please refer to Figure 1.

Process of selecting studies for meta-analysis.
All of the included studies in this review and meta-analysis were randomized controlled trials (RCTs). Among them, only one study utilized a single-blind design, while the remaining studies were open-label, meaning that both the researchers and participants were aware of the treatment being administered. The studies were conducted in different countries, including the United States, Belgium, and Italy. Notably, five of the studies were multi-center trials, involving participants from multiple countries. Please refer to Table 1 for further details on the geographic locations of the studies and the participating centers. To assess the risk of bias in the included studies, the ROB2 (revised cochrane risk-of-bias tool for randomized trials) tool was employed. Based on this assessment, two studies were classified as having a low risk of bias, indicating that their design and execution minimized the potential for bias. The remaining four studies were classified as having some concerns, indicating that there may be certain aspects of the study design or execution that could introduce bias. For a visual representation of the risk of bias assessment, please refer to Figure 2. It is important to consider the potential impact of the risk of bias on the interpretation of the results and the overall reliability of the findings presented in the included studies.
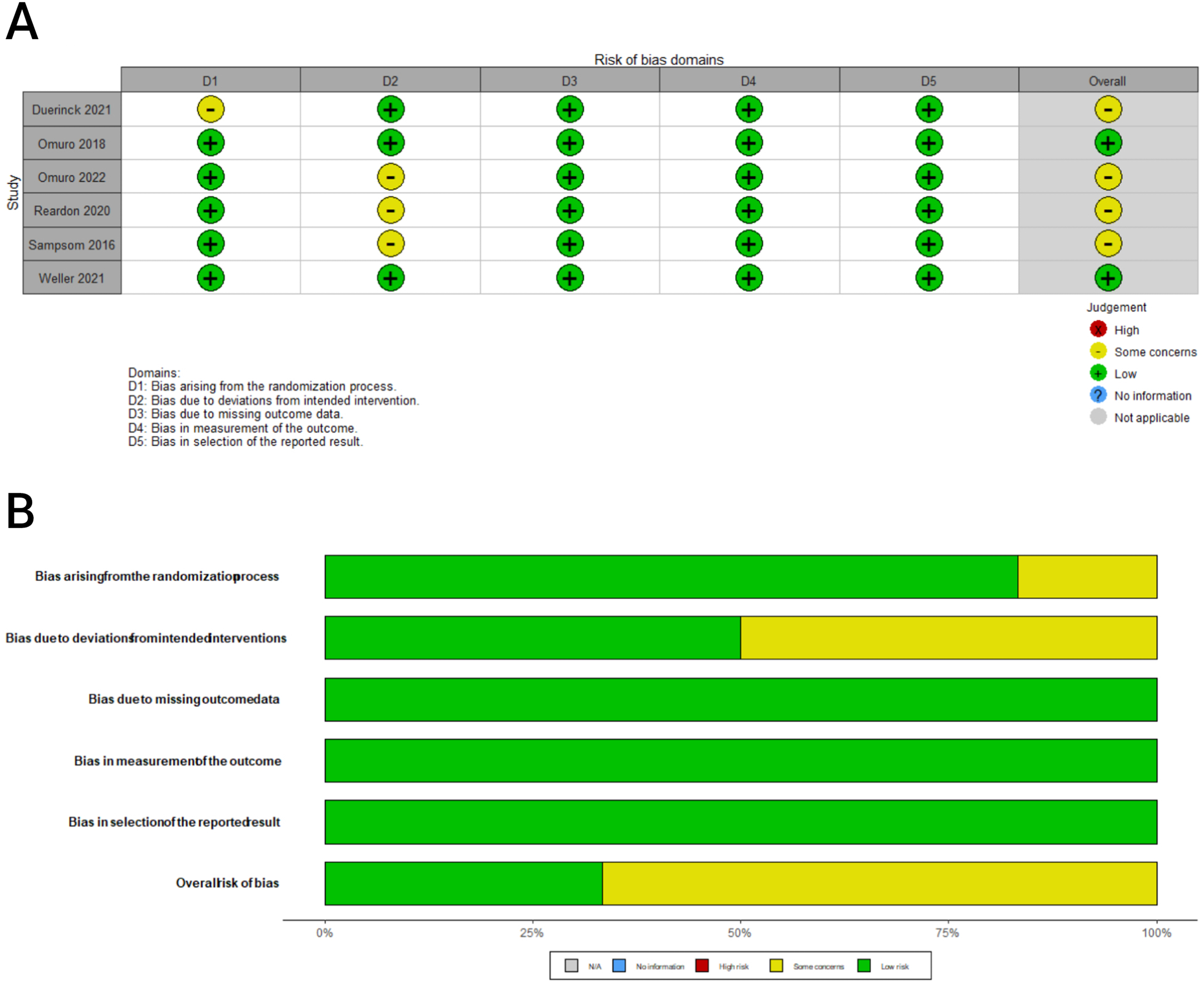
Risk of bias of included studies.
Characteristics of the studies included in the meta-analyses.
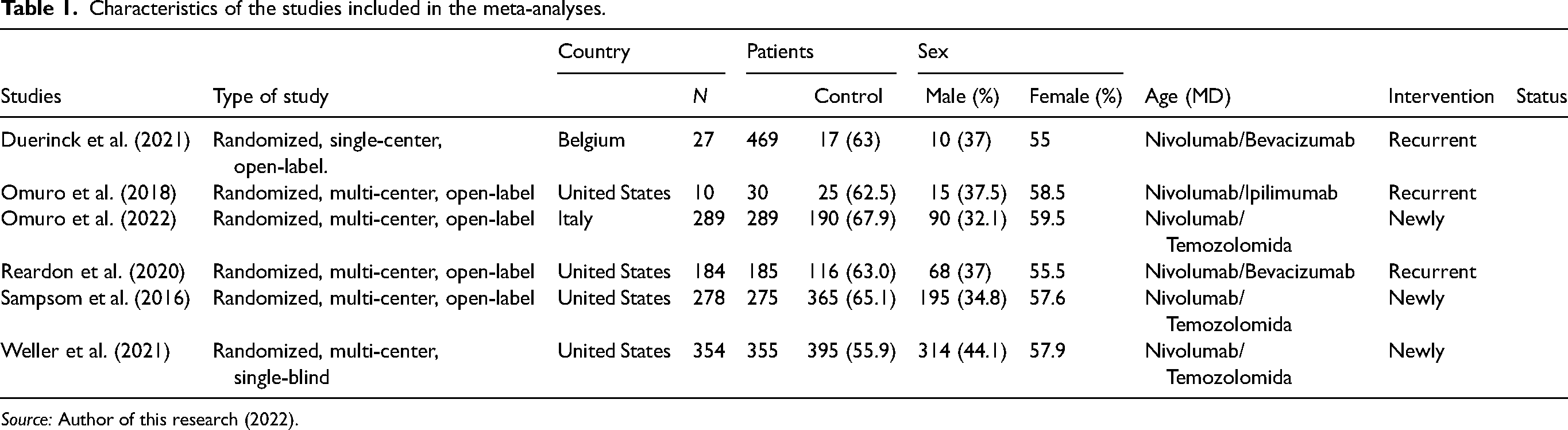
Source: Author of this research (2022).
The meta-analysis included a total of 2745 participants from the selected studies. Among these participants, 1142 individuals were treated with Nivolumab, while 1603 individuals received other specific cytotoxic treatments that served as controls for comparison purposes. Across all included studies, the male sex was more prevalent among the patients, accounting for 61.5% of the total participants. The mean age of the patients included in this meta-analysis was 57.3 years. The treatments utilized in the studies involved Nivolumab, as well as other specific cytotoxic treatments such as Ipilimumab, Temozolomide, and Bevacizumab. For further details on the specific treatments used in each study, please refer to Table 1. These demographic and treatment characteristics are important considerations for understanding the composition of the study population and the interventions evaluated in the meta-analysis.
The study data were divided into two subgroups based on patient characteristics. The first subgroup focused on newly diagnosed glioblastoma and included the studies conducted by Omuro et al. (2022), Sampson et al. (2016), and Weller et al. (2021). In this subgroup, a total of 921 patients were treated with Nivolumab, while 919 patients served as the control group for comparison. The second subgroup focused on recurrent glioblastoma and comprised the studies conducted by Duerinck et al. (2021), Omuro et al. (2018), and Reardon et al. (2020). In this subgroup, a total of 221 patients received Nivolumab, while 684 patients were included in the control group for comparisons. For a comprehensive overview of the data pertaining to each subgroup, please refer to Table 1 and Figure 3.
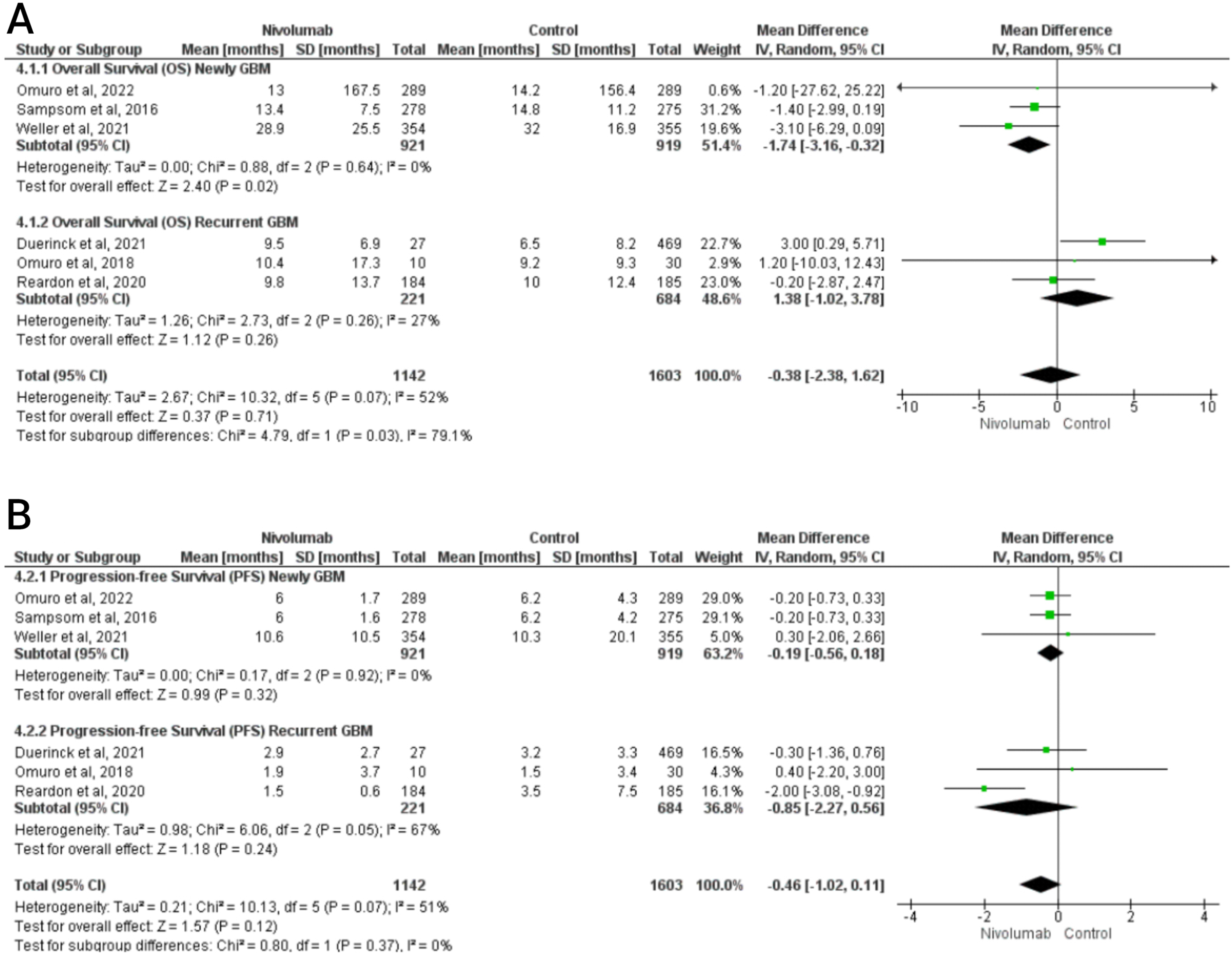
The forest plot showing the combinations between groups for overall survival and progression-free survival.
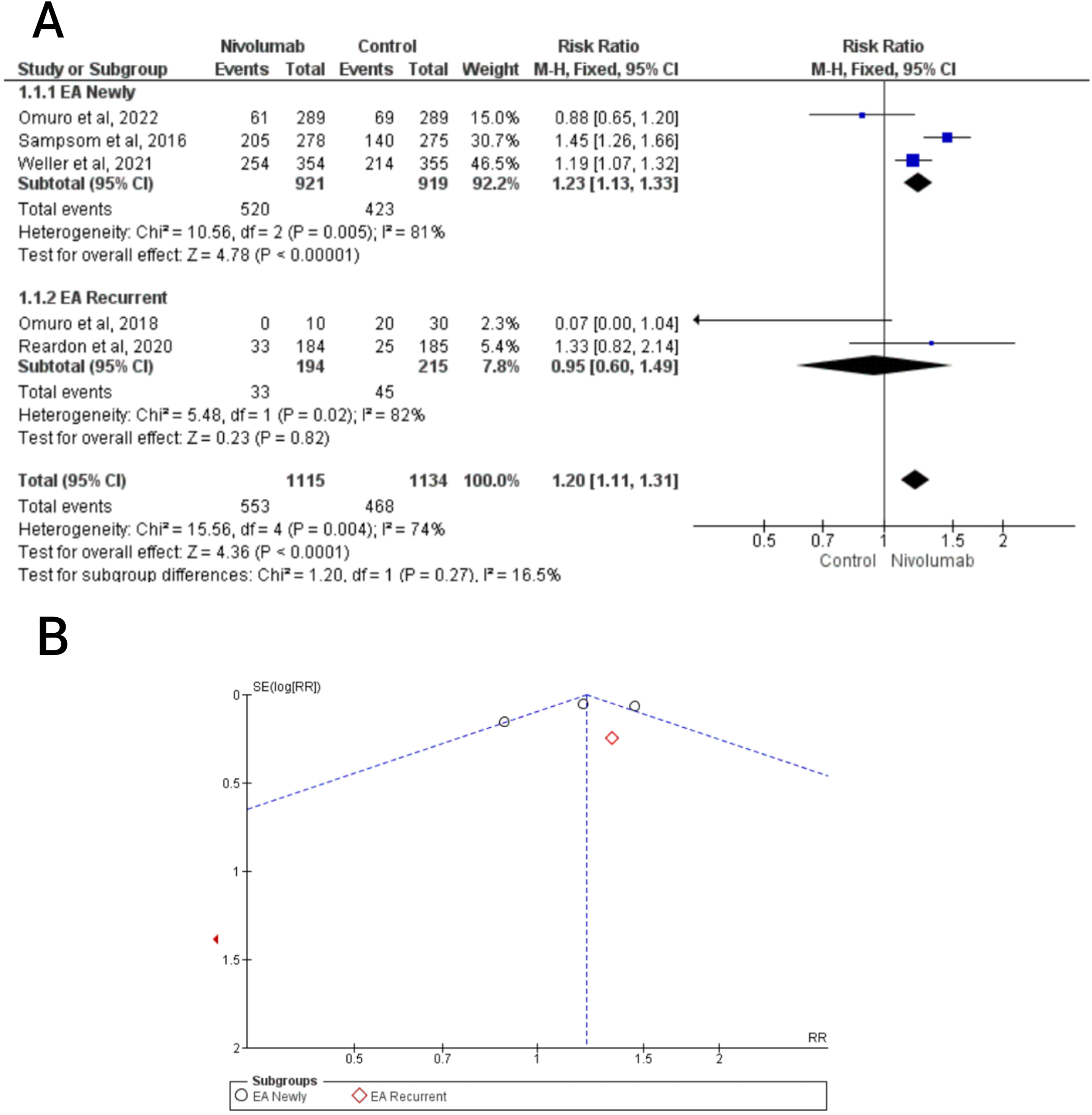
The forest and funnel plot showing the combinations between groups for adverse events in newly and recurrent glioblastoma.
Pooled incidence of primary outcomes
Associations for newly diagnosed GBM
In the subgroup analysis for newly diagnosed glioblastoma, the MD in OS indicated a positive effect for patients treated with Nivolumab compared to the control group. The analysis included 921 participants treated with Nivolumab and 919 participants in the control group. The median OS was increased in the Nivolumab group, with a MD of −1.74 (95% CI: −3.16, −0.32, Z = 2.40, p = 0.02). The heterogeneity for this outcome was low, with an I2 value of 0% (Chi² = 0.88, p = 0.64). The Egger's test showed no indication of publication bias between the studies, with a Z-value of 0.7232 and p = 0.4695. The funnel plot in Figure 5 also supports the absence of publication bias. The GRADE classification for this outcome was determined to be moderate (Table 2 and Figure 3).
Forest plot of association between Nivolumab and control group for OS.
Meta-analysis of association between Nivolumab and glioblastoma multiforme.
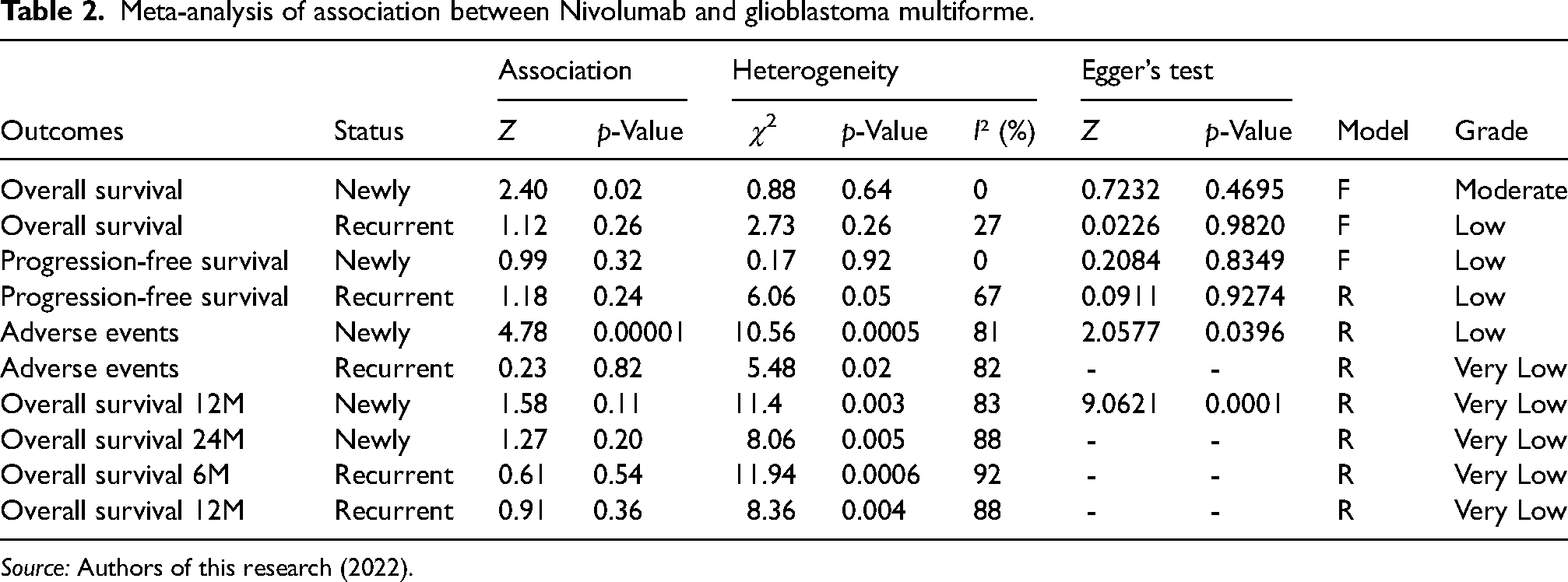
Source: Authors of this research (2022).
Regarding the median PFS, the results did not show a significant statistical difference between the Nivolumab and control groups. The analysis included data from the same subgroup of newly diagnosed glioblastoma patients, with an MD of −0.19 (95% CI: −0.56, 0.18, Z = 0.99, p = 0.32). The heterogeneity between the studies was null, with a Chi2 value of 0.17 and p = 0.92, resulting in an I2 value of 0%. The Egger’s test also indicated no publication bias, with a Z-value of 0.2084 and p = 0.8349. The GRADE classification for this outcome was determined to be low (Table 2 and Figure 3).
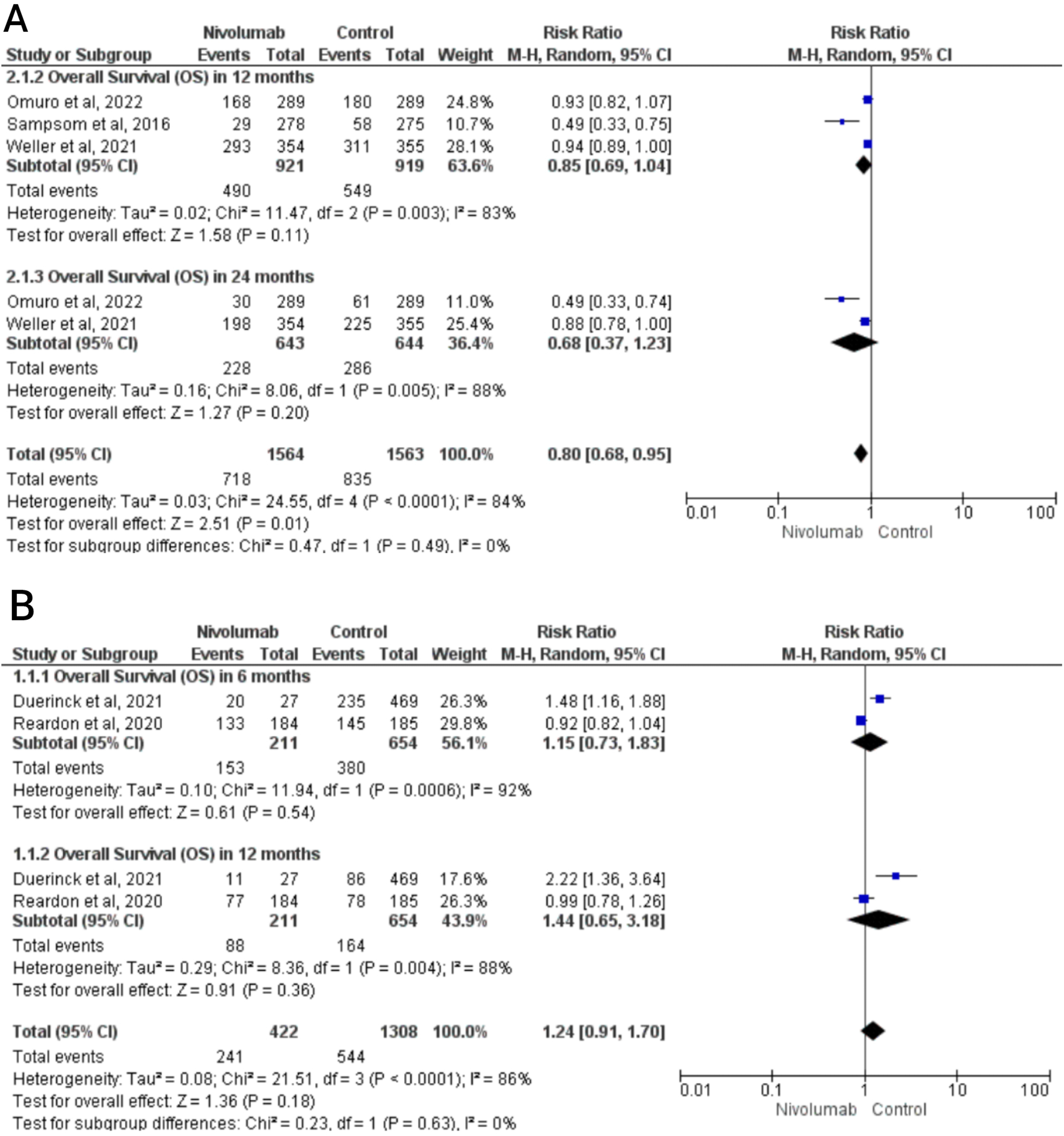
In the analysis of safety for the treatment with Nivolumab in newly diagnosed glioblastoma patients, a combination of relative risk (RR) was performed to assess the occurrence of adverse events between the compared groups. The results indicated that the RR was higher and significantly associated with patients treated with Nivolumab, with an RR of 1.23 (95% CI: 1.13, 1.33, Z = 4.78, p < 0.00001). However, it is important to note that there was a high heterogeneity in this outcome, with a Chi² value of 10.56 and p = 0.005, resulting in an I2 value of 81%. The presence of publication bias was detected through the Egger’s test, with a Z-value of −2.0577 and p = 0.0396. In terms of OS at 12 and 24 months, the analysis did not find a significant association between the Nivolumab group and the control group. The Z-values were 1.58 (p = 0.11) and 1.27 (p = 0.20) for OS at 12 and 24 months, respectively. However, it is important to consider the high heterogeneity in these outcomes, with Chi² values of 11.47 (p = 0.003) and 8.06 (p = 0.005), resulting in I2 values of 83% and 88%, respectively. Additionally, the GRADE recommendation for these results was very low (Table 2,Figure 5, and Figure 6).
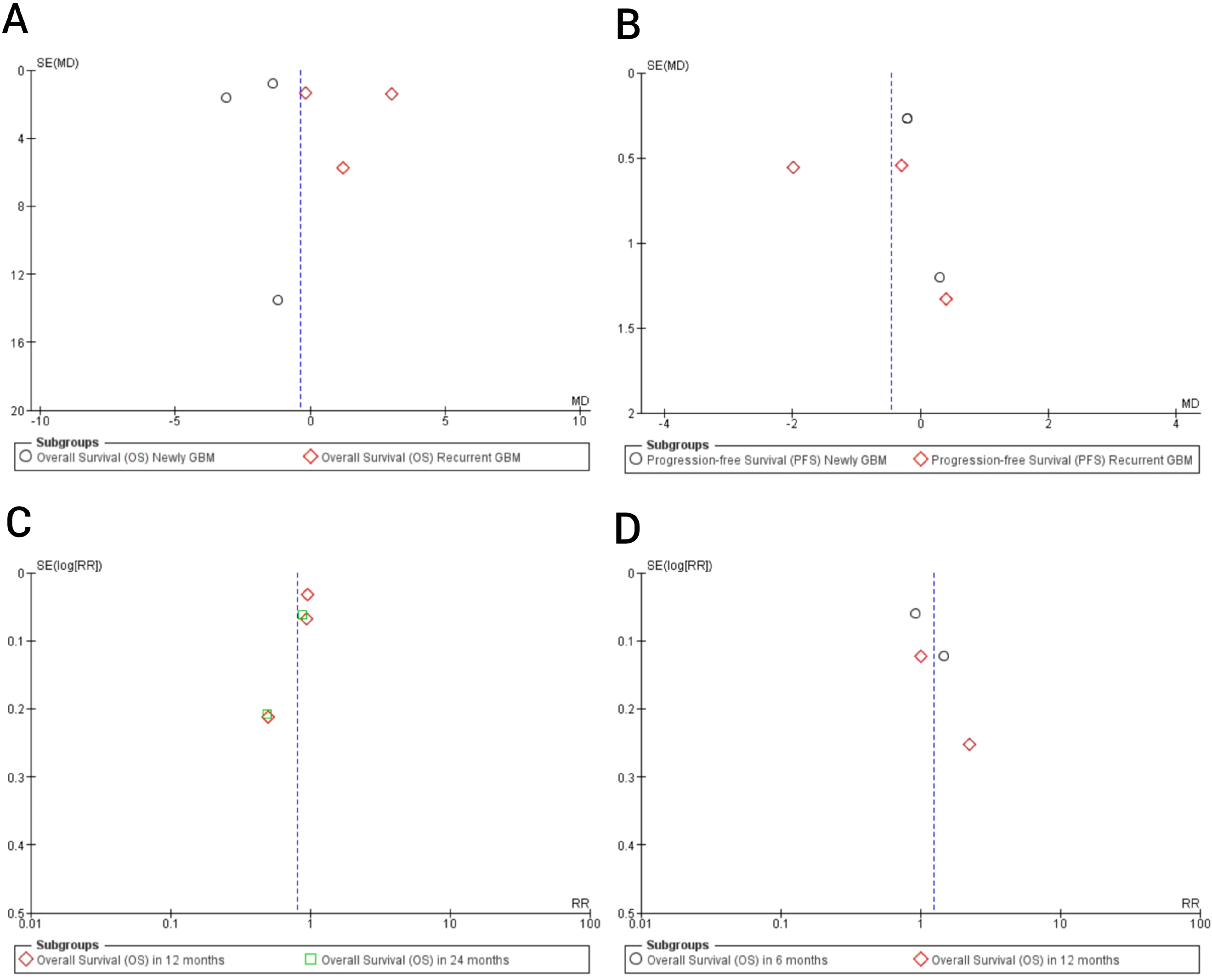
Funnel plots of association between Nivolumab and control group for OS and PFS.
It is crucial to interpret these findings in light of the limitations associated with the high heterogeneity, potential publication bias, and the very low GRADE recommendation. These factors may affect the reliability and generalizability of the results related to safety and OS in newly diagnosed glioblastoma patients treated with Nivolumab. Further research and larger studies are needed to provide more conclusive evidence in this regard.
Associations for recurrent GBM
In the analysis of median OS for recurrent glioblastoma in the studies by Duerinck et al. (2021), Omuro et al. (2018), and Reardon et al. (2020), the results did not show a significant statistical difference between the Nivolumab group (221 participants) and the control group (684 participants). The MD was 1.38 (95% CI: −1.02 to 3.78, Z = 1.12, p = 0.26). The heterogeneity for this outcome was moderate, with an I2 value of 27% (Chi² = 2.73, p = 0.26). To investigate the source of heterogeneity, an analysis was conducted and it was found that the trial by Duerinck et al. (2021) had a significant influence. After removing this trial, the remaining trials showed no heterogeneity (I2 = 0), but the statistical association remained insignificant (Z = 0.09, p = 0.92). The Egger’s test indicated no publication bias between the studies, with a Z-value of 0.0226 and p = 0.9820 (Table 2 and Figure 3).
For the recurrent glioblastoma subgroup, the MD in PFS showed no significant positive effects for patients treated with Nivolumab compared to the control group. The MD was −0.85 (95% CI: −2.27 to 0.56, Z = 1.18, p = 0.24). There was a moderate heterogeneity for this outcome, with a Chi² value of 6.06 and p = 0.05, resulting in an I2 value of 67%. Even after performing the source analysis, where studies with very different sample sizes between groups were removed, the heterogeneity remained. The Egger's test indicated no publication bias between the studies, with a Z-value of −0.0911 and p = 0.9274. The funnel plot in Figure 5 also supports the absence of publication bias. The GRADE recommendation for this outcome was low (Table 2 and Figure 3).
It is important to consider the limitations associated with the moderate heterogeneity and the lack of significant findings in the analysis of OS and PFS for recurrent glioblastoma. These factors may impact the interpretation and generalizability of the results. Further research and larger studies are needed to provide more conclusive evidence in this specific subgroup.
Due to the moderate heterogeneity (I2 = 67%), a sensitivity analysis was performed and the result revealed that a remarkable cut down on heterogeneity when the trial of Reardon et al. was deleted (Figure 4B). When we mentioned the outcome of the median OS with patients treated with bevacizumab (n = 433) compared with control (n = 401), the results showed that the bevacizumab group did not prolong median OS from the data of five trials (MD, −0.19 months; 95% CI: −1.37 to –0.99 months, p = 0.75) (Figure 5).
Figure 4 showed the RR for the occurrence of adverse events between the compared groups. For recurrent glioblastoma the RR no was significantly associated with patients treated with Nivolumab (RR, 0.95; 95% CI: 0.60–1.49, Z = 0.23, p = 0.82). However, for this outcome, a significant level of heterogeneity was observed (Chi² = 5.48, p = 0.02; I2 = 82%). According to the Recommendation Classification (GRADE), the quality of evidence for this outcome was assessed as low (Table 2 and Figure 4).
Discussion
Given the current scenario of high mortality and high recurrence rates, glioblastoma represents a significant health challenge. It is the most common primary malignant brain tumor in adults and is associated with a poor prognosis. In light of this problem, there is a need to explore new secure alternatives that can complement or replace existing treatment options such as surgical intervention and chemoradiotherapy.
In this study, we aimed to directly evaluate the effects of Nivolumab in both newly diagnosed and recurrent cases of glioblastoma. Our meta-analysis indicated that the Nivolumab group showed improved OS outcomes for newly diagnosed glioblastoma patients, with a prolonged median OS compared to control groups based on data from trials. However, there was no significant beneficial effect on median PFS, OS at 6, 12, and 24 months. Furthermore, no efficacy was observed in the treatment of recurrent glioblastoma patients.
For OS and PFS outcomes in newly diagnosed patients, as well as OS in recurrent glioblastoma, no significant heterogeneity was observed, and Egger's test did not identify the presence of publication bias. However, high heterogeneities were identified for other outcomes. Sensitivity analyses were performed due to the moderate to high heterogeneities, and the odds still reached statistical significance.
These findings summarize the results obtained from the studies included in our meta-analysis. Among the three studies that analyzed the efficacy of Nivolumab in newly diagnosed glioblastoma (Omuro et al., 2022; Sampson et al., 2016; Weller et al., 2021), the control group treated with Temozolomide showed better effects, prolonging both OS and PFS in patients. Our data diverge from these primary studies by demonstrating a favorable increase in OS for the Nivolumab group compared to the control group. The larger sample size in our analysis, which included all patients from the three studies, may have contributed to this change in statistical significance. Since there was no heterogeneity between studies, the evidence was classified as moderate.
In a phase 3 randomized clinical trial by Reardon et al. (2020), no statistical difference in the risk of death was observed between the Nivolumab and bevacizumab groups. The median OS was similar between the Nivolumab group (9.8 months; 95% CI, 8.2–11.8 months) and the bevacizumab group (10.0 months; 95% CI, 9.0–11.8 months). However, the control group had a more favorable median PFS outcome. Another published clinical trial by Duerinck et al. (2021) showed that the control group (Bevacizumab) was associated with higher OS compared to the Nivolumab group. However, when compared with a subgroup of control group patients who did not require corticosteroid treatment, Nivolumab showed significantly better OS. Additionally, Omuro et al. (2018) demonstrated limited efficacy of Nivolumab treatment when compared to Nivolumab plus Ipilimumab in their clinical trial.
Several factors must be considered when analyzing the efficacy of Nivolumab treatment for glioblastoma. One such factor is the methylation status of the MGMT promoter. Methylation of the MGMT promoter region leads to gene silencing, making neoplastic cells more susceptible to the effects of alkylating agents used in chemotherapy, such as Temozolomide, resulting in a better treatment response and prognosis. However, evidence regarding the efficacy of Nivolumab in relation to MGMT methylation needs further investigation. Studies by Weller et al. (2016) and Omuro et al. (2022), with patients having methylated and unmethylated MGMT promoters, respectively, showed no improvement in OS compared to the control group (TMZ). On the other hand, Reardon et al. (2020) found a difference in OS between patients with and without methylated MGMT promoter tumors, indicating that patients with methylated MGMT promoter and no baseline corticosteroid dependence are more likely to benefit from immune checkpoint inhibition.
The dependence on corticosteroids may have influenced the response to treatment, as evidence suggests that patients requiring corticosteroids to manage symptomatic cerebral edema may experience more rapid disease progression. Moreover, corticosteroids directly affect T-cell function, impairing immune system activation and priming.9,14,15
Another important factor to consider is PD-L1 expression. PD-L1 expression within the tumor microenvironment plays a role in T-cell accumulation. However, no association between clinical activity and tumor PD-L1 expression was observed in the studies by Omuro et al. (2022), Duerinck et al. (2021), and Omuro et al. (2018). Further investigation is necessary to determine the predictive value of PD-L1 expression.
To assess the safety of Nivolumab treatment, the presence of grade 3/4 treatment-related adverse events (TRAEs) was investigated. The Nivolumab group experienced more frequent events such as lymphopenia, seizure, fatigue, diarrhea, increased alanine aminotransferase, rash, headache, increased lipase, and nausea compared to control groups treated with Temozolomide or Bevacizumab. Additionally, Nivolumab-treated patients experienced more serious adverse events, including deaths related to vasogenic cerebral edema, sudden death, and respiratory failure, as compared to the control groups. The combination of ipilimumab and nivolumab was associated with an unacceptable high incidence of serious adverse events and low antitumoral activity. Locally administered Nivolumab in the brain tissue lining the glioblastoma resection cavity may result in a lower incidence of adverse events compared to intravenous administration.
Other factors that can be explored include low tumor mutational burden, recruitment of other immune checkpoints, decreased T-cell responsiveness, inhibitory cytokine production, interactions between the CNS microenvironment and microglia, predominance of myeloid cells, and a paucity of lymphocytes in the tumor microenvironment.16,17
The limitations of our study include the presence of publication bias in some analyses, detection of heterogeneity among the studies included in the meta-analysis, small sample sizes in some studies, and lack of detailed information on patients in the included studies.
Conclusion
In conclusion, our meta-analysis indicates that Nivolumab shows effectiveness in prolonging OS in patients newly diagnosed with GBM, but caution should be exercised regarding the lack of positive results for PFS and the occurrence of adverse events. Moreover, Nivolumab did not demonstrate efficacy in the treatment of recurrent glioblastoma. Based on these findings, we do not recommend replacing chemotherapy with Temozolomide (TMZ) with Nivolumab as a standard treatment for GBM. Further studies are necessary to explore the potential of checkpoint inhibitors and to gain a better understanding of the mechanisms underlying immune evasion in GBM. It is crucial to improve the efficacy of immunotherapies by investigating other biomarkers such as mutational burden and neoantigen landscapes. These studies can provide valuable insights into identifying patient subgroups that may benefit from immunotherapy and developing more targeted and personalized treatment approaches for GBM.
Supplemental Material
sj-docx-1-opp-10.1177_10781552231190104 - Supplemental material for Nivolumab for newly and recurrent glioblastoma multiforme treatment: A systematic review and meta-analysis
Supplemental material, sj-docx-1-opp-10.1177_10781552231190104 for Nivolumab for newly and recurrent glioblastoma multiforme treatment: A systematic review and meta-analysis by Alexandre Wendell Araujo Moura, Sirlene da Silva Rodrigues, Taciana Freire de Oliveira, Beatriz Marques Lobato, Natalia Neto Pereira Cerize and Patricia Léo in Journal of Oncology Pharmacy Practice
Supplemental Material
sj-docx-2-opp-10.1177_10781552231190104 - Supplemental material for Nivolumab for newly and recurrent glioblastoma multiforme treatment: A systematic review and meta-analysis
Supplemental material, sj-docx-2-opp-10.1177_10781552231190104 for Nivolumab for newly and recurrent glioblastoma multiforme treatment: A systematic review and meta-analysis by Alexandre Wendell Araujo Moura, Sirlene da Silva Rodrigues, Taciana Freire de Oliveira, Beatriz Marques Lobato, Natalia Neto Pereira Cerize and Patricia Léo in Journal of Oncology Pharmacy Practice
Supplemental Material
sj-docx-3-opp-10.1177_10781552231190104 - Supplemental material for Nivolumab for newly and recurrent glioblastoma multiforme treatment: A systematic review and meta-analysis
Supplemental material, sj-docx-3-opp-10.1177_10781552231190104 for Nivolumab for newly and recurrent glioblastoma multiforme treatment: A systematic review and meta-analysis by Alexandre Wendell Araujo Moura, Sirlene da Silva Rodrigues, Taciana Freire de Oliveira, Beatriz Marques Lobato, Natalia Neto Pereira Cerize and Patricia Léo in Journal of Oncology Pharmacy Practice
Supplemental Material
sj-docx-4-opp-10.1177_10781552231190104 - Supplemental material for Nivolumab for newly and recurrent glioblastoma multiforme treatment: A systematic review and meta-analysis
Supplemental material, sj-docx-4-opp-10.1177_10781552231190104 for Nivolumab for newly and recurrent glioblastoma multiforme treatment: A systematic review and meta-analysis by Alexandre Wendell Araujo Moura, Sirlene da Silva Rodrigues, Taciana Freire de Oliveira, Beatriz Marques Lobato, Natalia Neto Pereira Cerize and Patricia Léo in Journal of Oncology Pharmacy Practice
Supplemental Material
sj-docx-5-opp-10.1177_10781552231190104 - Supplemental material for Nivolumab for newly and recurrent glioblastoma multiforme treatment: A systematic review and meta-analysis
Supplemental material, sj-docx-5-opp-10.1177_10781552231190104 for Nivolumab for newly and recurrent glioblastoma multiforme treatment: A systematic review and meta-analysis by Alexandre Wendell Araujo Moura, Sirlene da Silva Rodrigues, Taciana Freire de Oliveira, Beatriz Marques Lobato, Natalia Neto Pereira Cerize and Patricia Léo in Journal of Oncology Pharmacy Practice
Supplemental Material
sj-docx-6-opp-10.1177_10781552231190104 - Supplemental material for Nivolumab for newly and recurrent glioblastoma multiforme treatment: A systematic review and meta-analysis
Supplemental material, sj-docx-6-opp-10.1177_10781552231190104 for Nivolumab for newly and recurrent glioblastoma multiforme treatment: A systematic review and meta-analysis by Alexandre Wendell Araujo Moura, Sirlene da Silva Rodrigues, Taciana Freire de Oliveira, Beatriz Marques Lobato, Natalia Neto Pereira Cerize and Patricia Léo in Journal of Oncology Pharmacy Practice
Supplemental Material
sj-tiff-7-opp-10.1177_10781552231190104 - Supplemental material for Nivolumab for newly and recurrent glioblastoma multiforme treatment: A systematic review and meta-analysis
Supplemental material, sj-tiff-7-opp-10.1177_10781552231190104 for Nivolumab for newly and recurrent glioblastoma multiforme treatment: A systematic review and meta-analysis by Alexandre Wendell Araujo Moura, Sirlene da Silva Rodrigues, Taciana Freire de Oliveira, Beatriz Marques Lobato, Natalia Neto Pereira Cerize and Patricia Léo in Journal of Oncology Pharmacy Practice
Footnotes
Acknowledgements
The authors thank all fellow authors whose publications could be included in our meta-analysis.
Author contributions
AWAM, PL, SSR, TFO and BML conceived and designed the experiments.
AWAM, SSR, TFO and BML performed the experiments.
AWAM, SSR, PL and NNPC analyzed the data.
AWAM wrote the paper.
AWAM, SSR, PL and NNPC critically reviewed for intellectual content.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Ethical statement
Ethics statement was not required since the research is a systematic review and meta-analysis of previously published studies.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Supplemental material
Supplemental material is available for this article online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.