
Abstract
Objective
Tyrosine kinase inhibitors (TKIs) have successfully changed the natural course of chronic myeloid leukaemia (CML). Although they are highly effective drugs, their clinical benefit is conditioned by adherence. This study aims to analyse the adherence of CML patients treated with TKIs and to identify the main factors influencing their adherence to TKIs treatment.
Material and methods
An 8-month prospective, observational, multicentre study which included patients diagnosed with CML on treatment with TKIs attending the outpatient departments (OPD) of the Pharmacy Services of the participating hospitals. Adherence was assessed using two methods: the Simplified Medication Adherence Questionnaire (SMAQ) and the register of treatment dispensations from the OPDs. To analyse the predictors of adherence, a questionnaire was developed to report demographic and socio-economic information on the patients.
Results
A total of 130 patients enrolled in this study. Adherence rate was 56.9% (n = 74) among individuals, not conditioned by the type of drug used: imatinib (54.8%), nilotinib (63.6%) or dasatinib (54.3%) (p = 0.67). The patient educational level (p = 0.047) and employment status (p = 0.028) were predictors of non-adherence to treatment.
Conclusions
Adherence is one of the most relevant parameters affecting the effectiveness of highly effective chronic treatments. Approximately half of our patients showed inadequate adherence to treatment with TKIs, with employment status and the individual's level of education emerging as the determining factors.
Keywords
Introduction
Chronic myeloid leukaemia (CML) is a myeloproliferative process that accounts for 15% of all leukaemia. 1 The proliferating cells of this haematological neoplasm are characterised by the presence of the Philadelphia chromosome, which is formed due to a reciprocal translocation between chromosomes 9 and 22 and the subsequent rearrangement of the BCR-ABL1 gene. 1
Up until the development of tyrosine kinase inhibitors (TKIs), CML was a disease associated with short survival. Nevertheless, the emergence of these drugs changed the disease landscape, achieving response and survival rates that often allow CML to be transformed into a chronic process. 2 TKIs are orally administered antineoplastic drugs, thus providing patients with a level of freedom and autonomy that cannot be achieved with intravenous drugs, which improves substantially their quality of life. 2 TKIs high efficacy leads them to be prescribed over long periods of time (years in most cases), consequently, a potential barrier to the therapeutic success of this type of medication must be considered: adherence.
Currently, lack of treatment adherence is considered a worldwide public health problem, with negative consequences for both patients and healthcare systems, as it constitutes one of the main causes of treatment failure. In recent years, adherence has increased due to the growing number of polymedicated individuals with chronic pathologies and the higher life expectancy. 3
Generally, therapeutic non-adherence is a phenomenon that often goes unnoticed by healthcare professionals as patients are often unaware of the consequences and do not report it, eventually affecting treatment effectiveness and safety. 3 Thus, adherence is conditioned by the action of several variables that may be related both to the medication and to the patient himself. We hypothesised that identifying the risk factors that predict therapeutic non-adherence is essential, as this would allow us to prevent or address it at an early stage through the design of individualised strategies for each patient.4,5
This study aims to assess the adherence to TKIs in patients with CML and to determine which patient- and medication-related factors may be responsible for non-adherence.
Material and methods
Design and population of study
This is an observational and prospective multicentre study, carried out over 8 months (February to September 2015), in which we analysed the degree of adherence and the possible factors that might condition it, among those patients with a diagnosis of CML who came to collect their oral treatment at the outpatient departments (OPDs) of the different pharmacy services in the participating hospitals.
The study included patients with a diagnosis of CML, aged ≥18 years and who had been on treatment with TKIs for at least 3 months.
A sample size was not estimated because this is a transversal study that only aims to evaluate the adherence of each patient at a specific moment during their treatment, in order to later analyse the correlation between the result and the socioeconomic characteristics of the patient.
Data collection and results evaluation
A combination of two methods was used to analyse adherence:
Simplified Medication Adherence Questionnaire (SMAQ). This is a tool initially validated for the assessment of adherence in HIV patients, although it has also been used to analyse adherence in other chronic conditions, whereby patients can be grouped into adherent versus non-adherent.
6
The patient was classified as “non-adherent” when at least one of the following circumstances was confirmed:
Occasionally forgetting to take medication. Not taking the medication at the same time. Stop taking the medication because of feeling unwell. Neglecting to take the medication at the weekend. Any forgetfulness of administration in the last week, or not taking the medication >2 full days since the last visit. Dispense records (DR) of the treatment in the last 6 months from the different OPDs. For this purpose, the percentage of medication dispensed was determined using the formula: [(total doses prescribed – doses not dispensed) X 100/total doses prescribed]. A patient was considered “non-adherent” if the percentage was <90%.
Individuals who showed a lack of adherence to treatment by any of these two methods were classified as “non-adherent patients”.
For the reporting of demographic and social information on each patient (gender, age, employment status, educational level, self-care, and family support), a third questionnaire developed specifically for this study was completed (Annexe I in the Supplemental Material).
Clinical data and information regarding adverse reactions were obtained from the medical records of the patients, including age at diagnosis, years of treatment, adverse reactions and TKI used.
Statistical analysis
Statistical analysis was performed to determine which factors may significantly influence adherence. Data evaluation was performed in a descriptive and stratified manner in accordance with patient adherence (adherent versus non-adherent). A multivariate binary logistic regression analysis was carried out to study the relationship between the dichotomous dependent variable and the set of explanatory variables, using IBM SPSS Statistics v. 25.0 software (IBM Corporation, Armonk, NY, USA).
A goodness-of-fit analysis of the multivariate model was carried out using the ‘Deviance’ measure. The Chi-square contrast based on this Deviance provided p-values that indicated which explanatory variables included in the binary logistic regression model were valid and really influenced adherence to TKIs.
Statistical significance was established with a value of p ≤ 0.05.
Ethical aspects
In order to guarantee the confidentiality of the data of the participating individuals, the information was treated in a dissociated manner, in such a way that the identification of the subjects became impossible.
All patients received a Patient Information Sheet and signed Informed Consent for their participation in the study.
This work was approved by each of the Clinical Research Ethics Committees corresponding to the participating hospitals (code LOH-IMA-2013-01).
Results
The study included a total of 130 patients, among whom 55.4% (n = 72) were male. The mean age of the population was 58.9 years [20–90], and the average time on treatment with TKIs was 4.7 years [0.6–13].
Treatment adherence was found to be correct in 56.9% (n = 74) of individuals, whereas 43.1% (n = 56) were identified as non-adherent.
By the time of the study, 63.1% (n = 82) of patients were on imatinib, 25.4% (n = 33) on nilotinib and 11.5% (n = 15) on dasatinib. Adherence did not vary according to the drug used (54.8% imatinib, 63.6% nilotinib and 54.3% dasatinib; p = 0.67).
A total of 54.6% (n = 71) of patients experienced some adverse drug-related reactions (ADRs) during their treatment. ADRs were reported in 52.4% (n = 43) of patients on imatinib; 66.7% (n = 22) in the case of individuals receiving nilotinib and 40% (n = 6) dasatinib (Figure 1).

Percentage distribution of adverse drug reactions (ADRs) occurred in individuals according to the tyrosine kinase inhibitor (TKI) received.
Demographic, socioeconomic and medication-related data collected for statistical analysis on their relationship to adherence are listed in Table 1. Educational level (p = 0.047) and the individual's employment status (p = 0.028) were identified as the factors significantly influencing treatment adherence (Table 1).
Factors influencing adherence in patients with chronic myeloid leukaemia (CML) treated with tyrosine kinase inhibitors (TKIs).
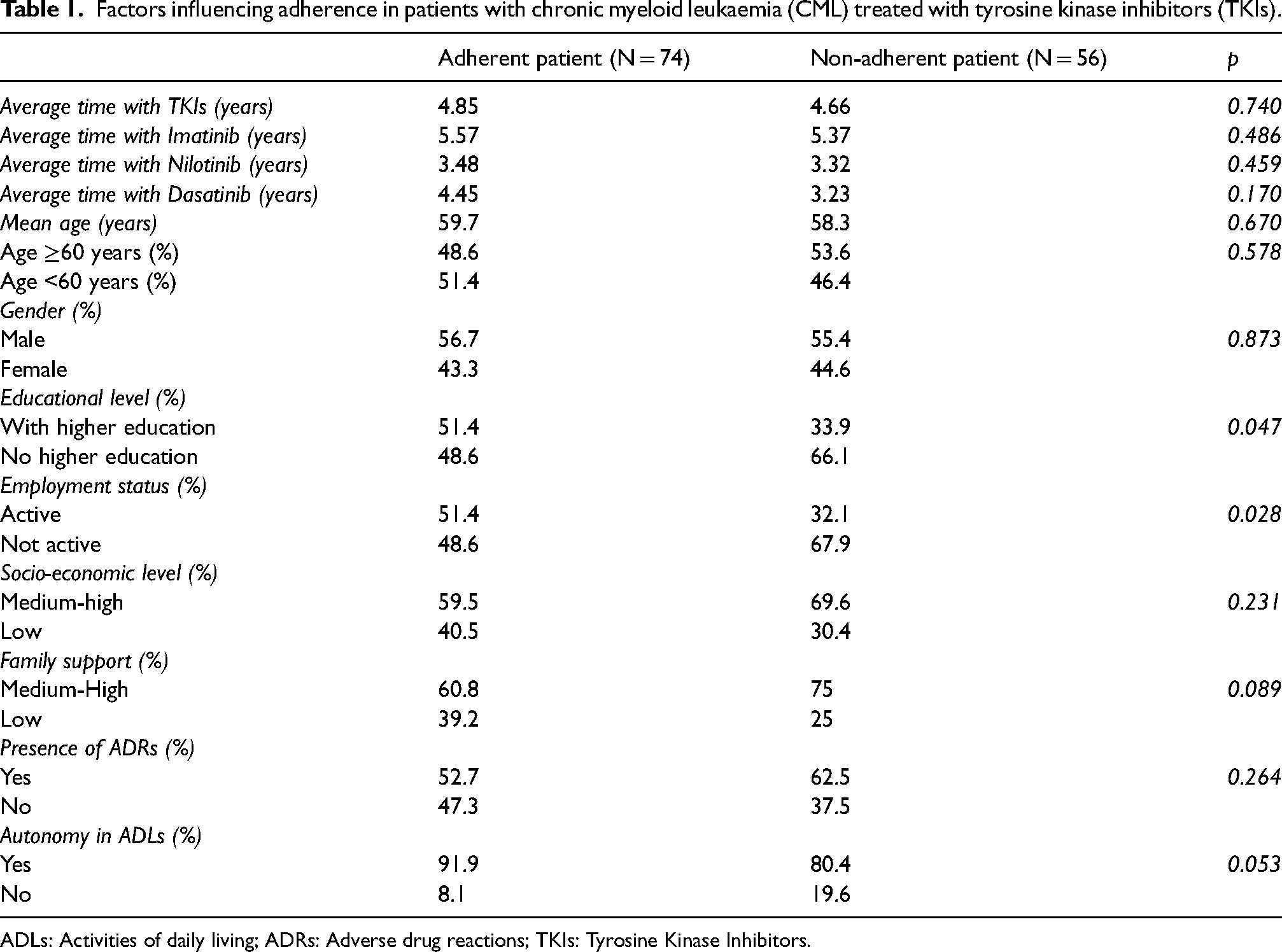
ADLs: Activities of daily living; ADRs: Adverse drug reactions; TKIs: Tyrosine Kinase Inhibitors.
Discussion
Oral antineoplastic drugs have provided patients with a level of autonomy and quality of life that intravenous treatments are unable to achieve. However, these drugs have the disadvantage of potentially leading to non-adherence by patients, which jeopardises their efficacy.7,8 Therapeutic non-adherence is currently considered one of the main public health problems affecting both the patient and the healthcare system and is considered a major factor interfering with drug safety and effectiveness, since it worsens patient quality of life, raises morbidity and mortality, and increases the use and cost of healthcare resources. 3
Patient adherence to treatment has been extensively studied in different healthcare fields. Nevertheless, available data on adherence to oral therapy in the field of oncohaematology are limited. Initially, cancer patients would be expected to have high adherence to their treatment due to the perceived severity of their disease. However, in a study involving breast cancer patients receiving anastrozole as adjuvant therapy, adherence was observed to decline over time. During the first year of therapy, about 75% of patients achieved optimal adherence to treatment, while this rate decreased to about 60% after the third year. 8 Similarly, in our study, for a mean treatment time of approximately 5 years, the proportion of adherent individuals was 56.9%, which was independent (p = 0.67) of the TKI used (imatinib (54.8%), nilotinib (63.6%) and dasatinib (54.3%).
Adherence to a given treatment for a chronic disease is considered a complex phenomenon that fluctuates over time due to more than 250 factors, resulting in a challenge to maintain adherence in the long term. 5 Toxicity is well-known as one of the aspects that most strongly compromises adherence and therefore the effectiveness of treatment. 9 Despite the high selectivity of the TKIs for their therapeutic target, they are not exempt from a wide range of adverse effects, which in some cases require medical care to mitigate them. 10 A trial that evaluated adherence to imatinib in patients with CML showed how prevention, early detection and management of adverse effects linked to imatinib improved adherence and reduced the discontinuation rate due to toxicity, which is around 5%. 10 Furthermore, this analysis showed a strong correlation between adherence and pharmacological response, where subjects with approximately 90% adherence showed a 95% probability of achieving a greater molecular response at 6 months. 10 In our study, even though more than 50% of the patients experienced some type of ADRs, no correlation was found between the development of adverse effects and the degree of adherence (p = 0.264). Likewise, no differences were observed among the adherence obtained for each of the TKIs (p = 0.67), so that therapeutic adherence seems to be independent of the drug administered, without reflecting an influence on adherence of the safety profile and the standard dosing regimen of each TKI (more complex in nilotinib due to its dosing interval and the higher number of tablets required for dose completion).
Regarding individual characteristics, it is known that aspects such as age, culture and educational level, among others, are factors that may condition adherence to treatment. 11 Thus, previous studies have shown that although older individuals may have multiple pathologies and greater confusion or forgetfulness concerning medication administration, it is the younger subjects who tend to be less adherent, as they question therapeutic recommendations to a greater extent and play down the importance of compliance with the prescribed treatment.12,13 However, our results show no differences in adherence between patients over and under 60 years of age when stratifying patients according to their age (p = 0.578).
On the other hand, more educated and wealthy people, although they have a better understanding of their disease and the therapeutic guidelines dictated by their doctor, they tend to be more critical and question them to a greater extent than less educated patients. 13 However, in the present study, we found that the rate of non-adherence was significantly higher in patients with no education than in those with a higher level of education (p = 0.047). Furthermore, although it is true that in this case, socioeconomic status did not seem to influence the degree of adherence (p = 0.231), the employment situation of the individual strongly conditioned adherence, revealing that unemployed patients were significantly less adherent (p = 0.028), suggesting a correlation between the economic situation of the patients and their adaptation to the therapeutic plan.
Likewise, family support is yet another factor that appears to be relevant for maintaining correct adherence. 13 In cases of social isolation, the loss of therapeutic monitoring and control of the disease is more frequent, which is why family members and/or caregivers play a fundamental role in promoting self-management and involvement of the patient in dealing with their pathology, particularly when the individual experiences difficulties to perform daily living activities. 13 When adherence was evaluated regarding patients with and without family support, no significant differences were observed between adherent and non-adherent individuals, as both groups showed high family support (60.8% versus 75%, respectively). However, patients who were not independent in carrying out activities of daily living (ADLs) were mostly non-adherent to treatment (19.6% versus 8.1%). Although not statistically significant (p = 0.053), this trend is a considerable difference in absolute terms and could therefore be another determinant of adherence in our study population.
Among the possible limitations of this study is the use of a previously unvalidated proprietary survey, designed to report information on demographic and socioeconomic factors that could influence the adherence of our patients. This included subjective outcomes such as the patient's perception of tolerance to treatment and the interviewer's assessment of the individual's socioeconomic status. However, the information regarding toxicity was contrasted with the subject's medical history, and the pharmacist's assessment of the individual's socioeconomic elements did not disagree with the data provided by the patient in any case. Apart from this, we also used the SMAQ survey which, although it was easily applicable to our CML patients on treatment with TKIs, is a tool that was originally validated for the assessment of adherence to antiretroviral therapy for human immunodeficiency virus (HIV), so we lack previous experience on its use in other types of populations.
This study aimed to analyse adherence to TKIs for CML in a significant number of patients, and at the same time, to evaluate those variables concerning the individual and the medication that could affect adherence. Almost half of CML patients investigated showed inadequate adherence to treatment with TKIs, with employment status and educational level being the main demographic and socio-economic factors conditioning treatment adherence.
Determining which factors may be predictors of adherence in our patient population will enable us to detect those subjects at risk of therapeutic non-adherence and, therefore, eligible for a more exhaustive pharmaceutical intervention, thus anticipating and avoiding possible therapeutic failure. Future work will analyse whether different healthcare approaches can improve adherence rates in these patients.
Supplemental Material
sj-pdf-1-opp-10.1177_10781552231196130 - Supplemental material for Risk factors determining adherence to tyrosine kinase inhibitors in chronic myeloid leukaemia
Supplemental material, sj-pdf-1-opp-10.1177_10781552231196130 for Risk factors determining adherence to tyrosine kinase inhibitors in chronic myeloid leukaemia by Betel Del Rosario García, María Micaela Viña Romero, Virginia González Rosa, Carolina Alarcón Payer, Leonor Oliva Oliva, Francisco Javier Merino Alonso, Gloria Julia Nazco Casariego and Fernando Gutiérrez Nicolás in Journal of Oncology Pharmacy Practice
Footnotes
Author Contributions
FGN, designed the study, defined the intellectual content and gained ethical approval; BRG, MMVR, VGR, CAP, LOO, collected the results and performed the data analysis; BRG, searched the literature and clinical studies and drafted the manuscript; All authors reviewed and approved the final version of the manuscript.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Ethical Approval
FGN, designed the study, defined the intellectual content and gained ethical approval; BRG, MMVR, VGR, CAP, LOO, collected the results and performed the data analysis; BRG, searched the literature and clinical studies and drafted the manuscript; All authors reviewed and approved the final version of the manuscript.
Supplemental Material
Supplemental material is available for this article online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.