
Abstract
Introduction
Olanzapine use for chemotherapy-induced nausea and vomiting (CINV) in hematological malignancies, for multi-day chemotherapy, and with a steroid-sparing antiemetic strategy is poorly understood. This study investigated if olanzapine is associated with improved prevention of CINV when added to a steroid-sparing antiemetic regimen in patients with acute leukemia receiving intensive, moderately emetogenic, multi-day chemotherapy.
Methods
This was a single-center, retrospective cohort study in patients with acute leukemia. Patients who received olanzapine for CINV prevention were compared to those who did not. All patients received a 5-HT3 antagonist. Adult patients receiving moderately emetogenic, multi-day, intensive chemotherapy for acute leukemia were included. Patients were excluded if they received steroids greater than physiological doses during the study period. The primary endpoint was the complete response of CINV (no emesis or rescue antiemetic usage).
Results
This study included 58 patients, 12 patients received olanzapine and 46 patients were in the control group. Baseline demographics were similar. In the study population, 89.7% had acute myeloid leukemia, median age was 54 (interquartile range 42–63) years, 34.5% were female, 27.6% had prior CINV. Complete response of CINV was similar between groups, 4 (33.3%) and 15 (32.6%) patients in the olanzapine and control groups, respectively. Safety events were similar between groups.
Conclusion
Patients with acute leukemia receiving multi-day intensive chemotherapy are at high risk for CINV. The limited data in this study suggests that olanzapine use within a steroid-sparing antiemetic regimen was well tolerated and associated with similar incidence and severity of CINV compared to the control group.
Introduction
Uncontrolled chemotherapy-induced nausea and vomiting (CINV) can negatively impact the quality of life of patients with cancer and has been associated with poorer prognosis.1,2 Multi-day chemotherapy regimens, commonly utilized in hematological malignancies, pose an additional challenge of overlapping pathophysiology of acute and delayed nausea and vomiting combined with anticipatory emesis on subsequent chemotherapy days.3,4 Suboptimal antiemetic regimens, with single-agent 5-HT3 receptor antagonists, may be given to these patients receiving intensive regimens due to concerns for steroid-induced immunosuppression.5,6 In fact, retrospective data reports 67–80% of patients with acute myeloid leukemia (AML) experience breakthrough CINV despite standard prophylaxis.5,6
Olanzapine is an atypical antipsychotic agent that has been shown to prevent acute and delayed CINV in patients with mainly solid tumors receiving single-agent or single-day regimens.7–11 National Comprehensive Cancer Network® (NCCN®) Antiemesis Guidelines recommend olanzapine 5 to 10 mg once daily regimen on days 1 to 4 in combination with a 5-HT3 antagonist, dexamethasone, and an neurokinin-1 receptor (NK-1) antagonists (such as fosaprepitant) as an option for highly emetogenic chemotherapy. 12 For moderately emetogenic chemotherapy, NCCN Guidelines recommend olanzapine for days 1 to 3 in combination with a 5-HT3 antagonist and dexamethasone as an option. 12 Antiemetic regimens containing olanzapine are recommended if steroid-sparing strategies are used; however, there are minimal data in patients with acute leukemia receiving multi-day intensive chemotherapy. 12
This study sought to examine the role of olanzapine in preventing CINV from high-intensity, moderately emetogenic (as defined by the NCCN Guidelines), multi-day chemotherapy regimens in patients with acute leukemia. We hypothesized that an antiemetic regimen containing olanzapine is associated with increased complete response of CINV for patients with acute leukemia receiving multi-day intensive chemotherapy. Complete response of CINV is defined as absence of emetic episodes or rescue antiemetic usage (“once” or “as needed” orders).
Methods
This was a retrospective cohort study of CINV in patients with acute leukemia receiving moderately emetogenic, multi-day, intensive chemotherapy. Those who received olanzapine as antiemetic prophylaxis were compared to those who did not. This study was approved by the University of Maryland Institutional Review Board.
Patients were included if they were at least 18 years old, received cytarabine, cladribine, filgrastim +/- mitoxantrone or gemtuzumab vedotin (CLAG, CLAG-M, CLAG-GO) or cytarabine, mitoxantrone, and pegaspargase (HAM-pegA) chemotherapy regimens from November 2015 to May 2022. Subsequent chemotherapy cycles for the same patient that would otherwise meet study criteria were excluded. Patients were included in the olanzapine group if they received at least one dose of enteral olanzapine within the 24 hours prior to any dose of chemotherapy. Patients were excluded if they were on olanzapine chronically, received olanzapine after CINV onset, received nonstandard CINV prophylaxis (5-HT3 antagonist with or without olanzapine), or received steroids greater than physiological doses (defined as greater than prednisone 20 mg or dexamethasone 3 mg steroid equivalence) during the study period. Steroids less than physiological doses (such as those used to prevent or treat hypersensitivity reactions) were acceptable due to their minimal CINV effect.
The primary endpoint was complete response of CINV (no emesis or use of rescue antiemetic) in the overall phase (0–120 hours after last chemotherapy). The secondary endpoints were complete response of CINV in the acute (0 to 24 hours after last chemotherapy) and delayed (24 hours after last chemotherapy to 120 hours after last chemotherapy) phases, time to first CINV (emesis or use of rescue antiemetic), severity of CINV (based on number of emetic episodes and antiemetic doses used in patients who vomited or used rescue antiemetic), days with CINV (number of study days patient experienced CINV), tolerability of olanzapine.
Data were collected via retrospective chart review of provider and nursing notes, flow sheet assessments, electrocardiograms (EKG), and medication administration records. Tolerability of olanzapine was assessed based on notating reports of fatigue, confusion, sedation, sleep disturbance, dizziness, hallucinations, xerostomia, and extrapyramidal symptoms (EPS), as well as documentation of QTc prolongation. All EKG completed during the study period were evaluated for QTc prolongation. If patients received more than one baseline (prior to chemotherapy) EKG, then the EKG closest to the time of chemotherapy initiation was used. If patients received more than one EKG in the overall phase, then the EKG with the highest QTc was used. QTc prolongation was noted if QTc during treatment was increased from baseline by at least 60 ms or >500 ms. All medications administered during the study period were evaluated. Medication package inserts were used to determine if other medications may contribute to the risk of EPS or QTc prolongation.
Definitions
Complete response was defined as no emesis or use of rescue antiemetics in the overall phase. CINV was defined as emesis or use of rescue antiemetics. Prevention antiemetics were defined as scheduled antiemetic doses administered to avoid symptoms of nausea and/or vomiting from occurring or worsening (must not be “once” or “as needed” orders). Rescue antiemetics were defined as antiemetic doses administered in response to symptoms of nausea and/or vomiting “once” or “as needed” orders). Acute phase was defined as the time period from the start of chemotherapy to 24 hours after the last dose of chemotherapy. Delayed phase was defined as the time period from 24 hours after the last dose of chemotherapy to 120 hours after the last dose of chemotherapy. The number of vomiting episodes and doses of rescue antiemetics used were used as surrogate markers for CINV severity. Days with CINV was defined as number of study days the patient experienced emesis and/or use of rescue antiemetics. Early discontinuation of olanzapine was defined as stopping the medication order for scheduled olanzapine prior to completion of all chemotherapy doses.
Institutional practice
At our institution, patients with relapsed or refractory AML or mixed phenotype acute leukemia often receive one of the following high-intensity regimens: cladribine 5 mg/m2 and cytarabine 2000 mg/m2 intravenously (IV) daily on days 1 to 5 (CLAG 13 ), CLAG with mitoxantrone 10 mg/m2 IV daily on days 1 to 3 (CLAG-M 13 ), CLAG with gemtuzumab ozogamicin 3 mg/m2 IV on days 1 and 4 (CLAG-GO 14 ), or cytarabine 3000 mg/m2 IV every 12 hours for 5 doses on days 1 to 3, and mitoxantrone 6 mg/m2 IV daily on days 1 to 3 with pegasparagase 2000 units/m2 IV on day 4 (HAM-pegA 15 ).
The standard prevention antiemetic regimen was single-agent ondansetron 16 mg orally once daily on days 1 to 5 prior to each dose of cytarabine. Olanzapine 5 mg orally twice daily on days 1 to 5 then 5 mg orally twice daily as needed for nausea or vomiting on days 6 and 7 was added to the above chemotherapy regimens in October 2020. 16
Statistical analysis
This study used a convenience sample of all patients who met inclusion and exclusion criteria. Descriptive statistics were reported for the study population. Histograms were used to assess normality. A chi-square or Fischer's exact test was used to compare the proportion of complete response and safety endpoints. The Wilcoxon rank sum test was used to analyze severity of CINV and days with CINV. Subgroup analyses were performed for acute and delayed phases. A Kaplan-Meier curve with log rank test was used to evaluate the time to first loss of complete response. A p-value of <0.05 was considered statistically significant.
Results
Of the 718 patients screened, 73 patients met inclusion criteria, and 15 patients were excluded. Nine patients were excluded for receiving steroids greater than physiological doses during chemotherapy, two patients were excluded for receiving olanzapine after CINV onset, two patients were excluded for early discontinuation of chemotherapy, and two patients were excluded for receiving nonstandard CINV prophylaxis. The study assessed 58 patients, with 12 in the olanzapine group and 46 in the control group.
Baseline demographics were similar between groups (Table 1), including known risk factors for CINV of age, female gender, prior CINV, alcohol use, and history of anxiety. In the overall population, the median age was 54 (interquartile range 42–63) years, 34.5% were female, and 27.6% had prior CINV. All patients received a 5-HT3 antagonist for CINV prevention.
Baseline demographics.
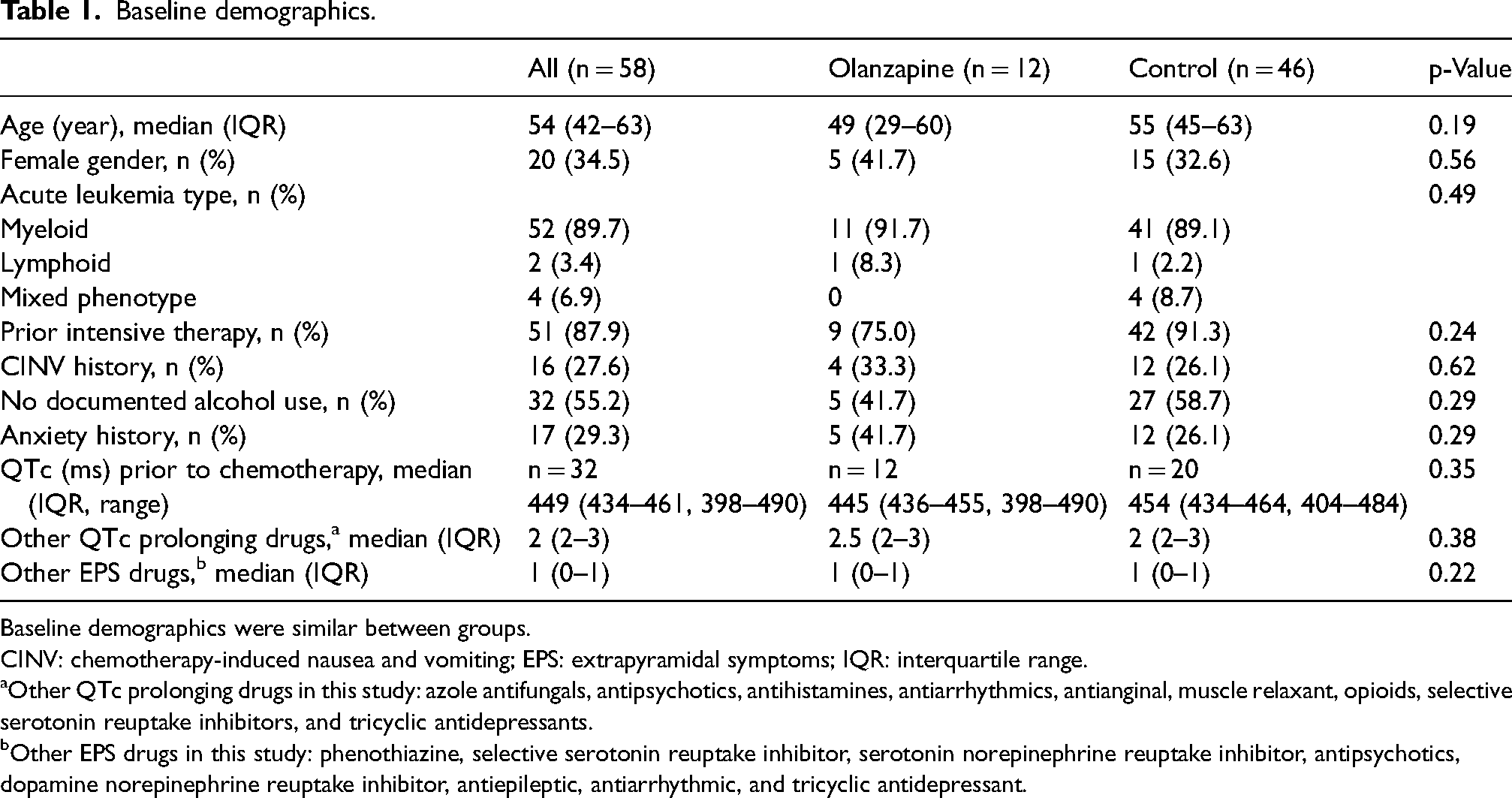
Baseline demographics were similar between groups.
CINV: chemotherapy-induced nausea and vomiting; EPS: extrapyramidal symptoms; IQR: interquartile range.
Other QTc prolonging drugs in this study: azole antifungals, antipsychotics, antihistamines, antiarrhythmics, antianginal, muscle relaxant, opioids, selective serotonin reuptake inhibitors, and tricyclic antidepressants.
Other EPS drugs in this study: phenothiazine, selective serotonin reuptake inhibitor, serotonin norepinephrine reuptake inhibitor, antipsychotics, dopamine norepinephrine reuptake inhibitor, antiepileptic, antiarrhythmic, and tricyclic antidepressant.
Complete response of CINV occurred in only 19 (32.8%) patients in the study overall phase, 4 (33.3%) patients in the olanzapine group and 15 (32.6%) patients in the control group (p = 0.96). Complete response of CINV in the acute and delayed phases, number of antiemetic rescue doses, number of emetic episodes, time to CINV, and days with CINV were also similar between groups (Table 2).
Retrospective chemotherapy-induced nausea and vomiting outcomes.
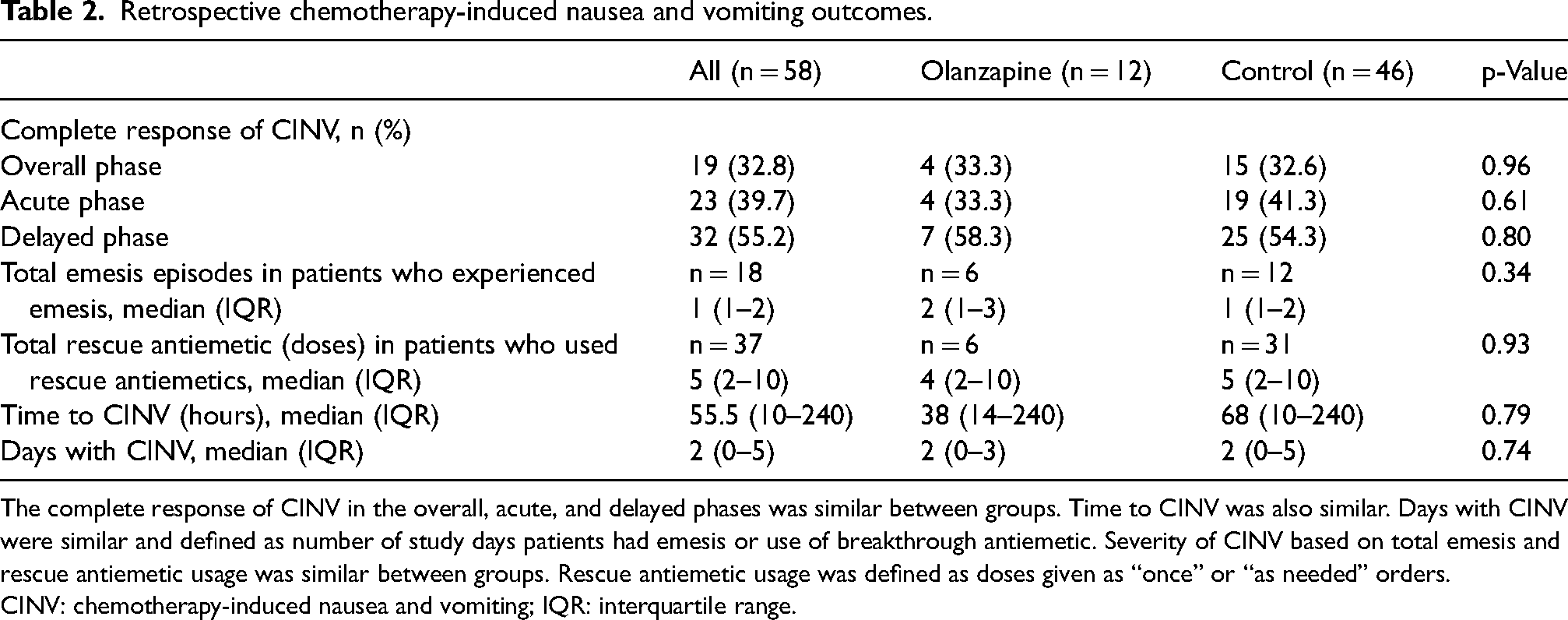
The complete response of CINV in the overall, acute, and delayed phases was similar between groups. Time to CINV was also similar. Days with CINV were similar and defined as number of study days patients had emesis or use of breakthrough antiemetic. Severity of CINV based on total emesis and rescue antiemetic usage was similar between groups. Rescue antiemetic usage was defined as doses given as “once” or “as needed” orders.
CINV: chemotherapy-induced nausea and vomiting; IQR: interquartile range.
The most common olanzapine regimen was olanzapine 5 mg orally twice daily. Only one patient received olanzapine 5 mg orally once daily. All 12 patients in the olanzapine group received scheduled olanzapine on days 1 to 5 but 4 patients continued on schedule olanzapine after day 5. These 4 patients experienced acute CINV, which likely led to the clinical decision to continue olanzapine scheduled after day 5.
Incidences of safety endpoints were similar between groups (Table 3). No patients developed extrapyramidal symptoms. One patient in the olanzapine group developed QTc prolongation with baseline QTc of 455 ms that increased to 585 ms. This led to early discontinuation after receiving 8 doses of olanzapine 5 mg orally twice daily. This patient also received two other medications (5 doses of ondansetron and 6 doses of hydroxyzine concomitantly) that may cause QTc prolongation. No serious adverse events occurred in the olanzapine group, and no other patients discontinued olanzapine early.
Retrospective safety outcomes.
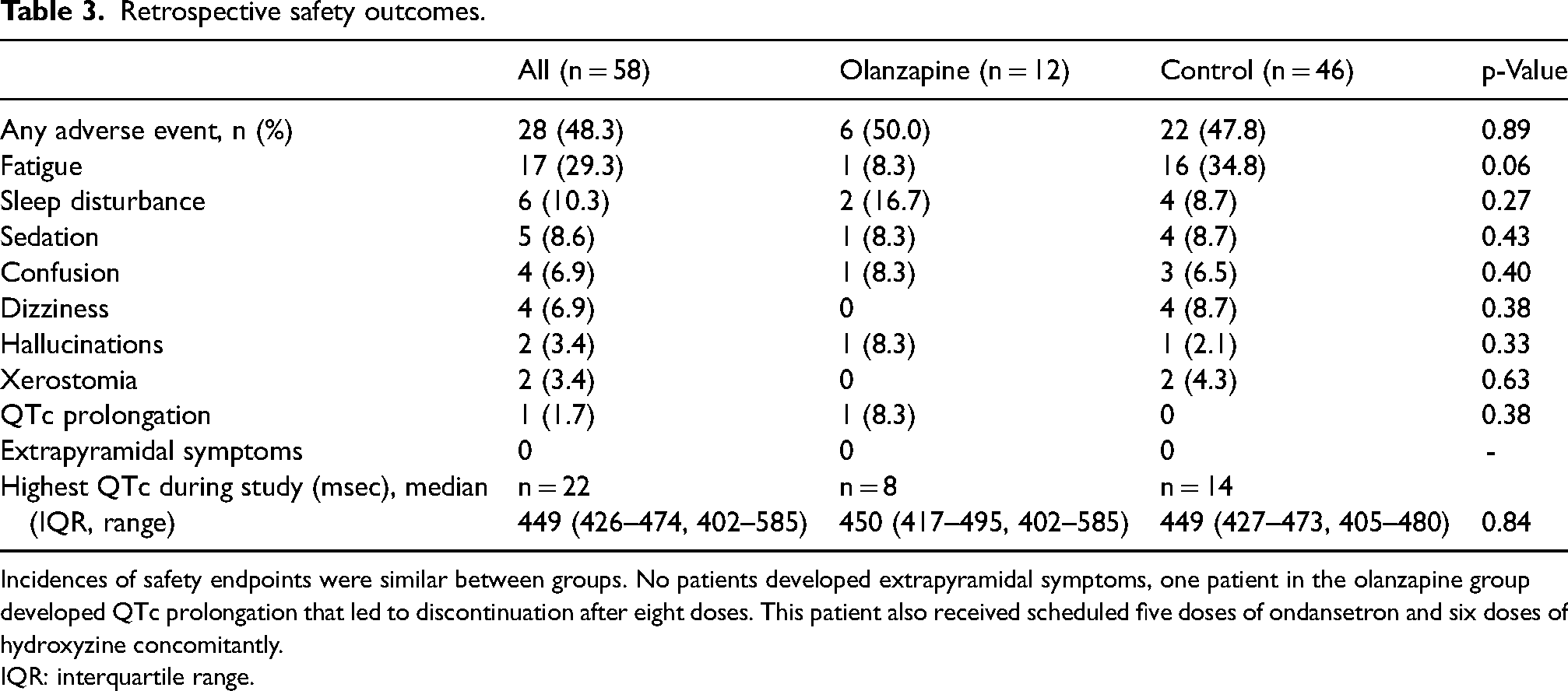
Incidences of safety endpoints were similar between groups. No patients developed extrapyramidal symptoms, one patient in the olanzapine group developed QTc prolongation that led to discontinuation after eight doses. This patient also received scheduled five doses of ondansetron and six doses of hydroxyzine concomitantly.
IQR: interquartile range.
Discussion
Olanzapine was associated with good tolerability and similar incidence of emesis and use of breakthrough antiemetics between the study and control group of patients with acute leukemia receiving moderately emetogenic, multi-day, intensive chemotherapy.
Complete response of CINV in this study was low but comparable to literature in similar patient populations.5,17 While the individual agents in the chemotherapy studied are categorized as having moderate emetic potential, the multi-day administration schedule may have a compounding effect on CINV risk due to overlapping pathophysiology of acute and delayed nausea and vomiting. 5 Thus, patients receiving multi-day intensive chemotherapy may require close monitoring during this time to ensure adequate CINV support.
Patients who require a steroid-sparing strategy often receive suboptimal antiemetic regimens with serotonin antagonist monotherapy requiring a different approach to CINV control. 5 For these patients, the NCCN Guidelines recommend olanzapine as an option because it has been consistently shown to prevent both nausea and vomiting in highly emetogenic regimens for patients with solid malignancies receiving single-day chemotherapy.7–12 Studies in hematopoietic stem cell transplant have found olanzapine to be effective in preventing CINV associated with highly emetogenic conditioning regimens.17–20
Olanzapine has demonstrated effectiveness in patients with hematological malignancy as a rescue antiemetic by Monson et al. and as a prophylactic antiemetic by Clemmons et al. Monson et al. conducted a retrospective cohort review of 150 patients receiving hematopoietic stem cell transplants. 21 Most patients received two-drug antiemetic prevention regimen with serotonin antagonist and dexamethasone. Olanzapine was associated with a complete response in 30% of patients experiencing breakthrough CINV. Similarly, Clemmons et al. 17 conducted a randomized placebo-controlled trial of 101 patients with hematological malignancy receiving multi-day chemotherapy or single-day or multi-day conditioning regimen for hematopoietic stem cell transplantation (HSCT). Patients received a combination of fosaprepitant, ondansetron, and dexamethasone, with or without olanzapine. Olanzapine exhibited a superior response in managing CINV, reducing nausea and emesis during the delayed and overall phases, though not in the acute phase. However, the chemotherapy subgroup where all patients received multi-day chemotherapy (comprising only 33 patients) found no difference in complete response of CINV between olanzapine and placebo in all study periods. Notably, the HSCT subgroup, consisting of 68 patients, likely played a substantial role in the study findings, showing significant enhancement in CINV complete response during the delayed and overall phases. However, this subgroup included both multi-day (63.2%) and single-day (36.7%) conditioning regimens. The study did not specifically analyze multi-day chemotherapy/conditioning regimen. Our study was centered on multi-day chemotherapy, albeit with limitations due to sample size. The incidence of CINV was higher in our study likely due to sparing use of corticosteroids for prophylaxis.
While olanzapine's potential to prevent CINV in patients receiving multi-day regimens for hematological malignancy remains uncertain, promising data exist in patients with solid malignancy. The OFFER study was a multicenter, randomized, double-blind, placebo-controlled trial of olanzapine plus triple antiemetic regimen for prevention of CINV with multi-day highly emetogenic chemotherapy. 22 All 349 patients received three consecutive days of cisplatin and triple antiemetic regimen with fosaprepitant, ondansetron, and dexamethasone. Olanzapine improved complete response of CINV and nausea incidence in the overall and delayed phases but not the acute phase. The overall incidence of complete response was higher in the OFFER study with highly emetogenic cisplatin compared to our study with moderately emetogenic chemotherapy, potentially due to the longer duration of multi-day chemotherapy (3 days vs our 4 or 5 days) and sparing use of steroids in our study. The promising findings in the OFFER study should be further validated in other multi-day chemotherapy regimens and in the hematological malignancy population.
To the best of our knowledge, our study was the first to explore whether olanzapine can help prevent CINV in patients with acute leukemia with a steroid-sparing antiemetic regimen. The most common regimen in this study was olanzapine 5 mg twice daily for days 1 to 5 only. Our institution chose to use a shorter course of olanzapine rather than continuing for 2 days after chemotherapy per guideline recommendations since the duration of chemotherapy was longer than those previously studied. This is within the variations of olanzapine regimens described in literature.7,9,10,17–19,23,24 Further studies are needed to determine the best olanzapine antiemetic prophylactic regimen for multi-day chemotherapy.
There are a few limitations that should be considered when interpreting the present study. The retrospective nature relied on accurate documentation, may be subject to information bias, and may not accurately inform the causality of adverse events. However, we adhered to strict definitions consistent with the literature to minimize the impact and prevent it from having disproportionate effects. This study is limited by the lack of reporting of nausea as it is difficult to evaluate nausea retrospectively. We used the surrogate marker of rescue antiemetic usage but this may represent either nausea or emesis and is also limited by patient underreporting. Olanzapine regimen was not fully standardized which may confound results of this study. However, the outlier patient received olanzapine 5 mg once daily, which has demonstrated efficacy and recommended as an option by the NCCN Guidelines.9,12 Not all leukemia intensive chemotherapy regimens were included in this study and may limit the generalizability of the results. This is also a single-institution study with a small sample size and used a convenience sample which limited statistical power.
Limited data herein suggests safety and efficacy. Future studies are needed to evaluate the best strategy to prevent multi-day chemotherapy-induced nausea and vomiting. Prospective studies could offer added value in understanding nausea control—an area of concern due to its subjective nature, risk of patient underreporting, possibility of clinician underestimation, and high impact on patient quality of life. 25
Conclusion
Patients with acute leukemia receiving multi-day intensive chemotherapy are at high risk for CINV. The limited data in this study suggests that olanzapine use within a steroid-sparing antiemetic regimen was well tolerated and associated with similar incidence and severity of CINV compared to the control group.
Footnotes
Author contributions
GH contributed to conceptualization, methodology, formal analysis, investigation, writing—original draft preparation, visualization, supervision, and project administration. CB contributed to conceptualization, methodology, investigation, writing—review and editing, and supervision. JL contributed to conceptualization, methodology, investigation, and writing—review and editing. VD, AE, and SN contributed to methodology, and writing—review and editing. AD contributed to conceptualization, methodology, investigation, writing—review and editing, supervision, and project administration.
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.