
Abstract
Objective
To provide an integrated approach for deprescribing practice in oncology setting.
Data sources
The data on deprescribing in oncology settings has been retrieved from the PubMed, Scopus and Google Scholar. We used “deprescribing,” “potentially inappropriate medication” and “cancer” as a keyword for the conducting general search. The articles relevant to guidelines or tools used to deprescribe in cancer care were included.
Data summary
The nature of cancer, its treatment strategies, adverse effects of therapy and multimorbidity impact negatively on quality of life (QoL). Further, they invite polypharmacy which puts the patient at higher risk of drug-related problems like drug interactions, adverse drug reactions and addition of potentially improper medications, etc. In older adults with cancer, the incidence of potentially inappropriate medications (PIMs) was between 41% and 52%. Over the decades, multiple strategies have been developed to assess the appropriateness of therapy. One such approach is deprescribing. OncPal and oncoSTRIP (Systematic Tool to Reduce Inappropriate Prescribing) are the cancer specific guidelines whereas BEERs criteria, Screening Tool to Alert to Right Treatment/Screening Tool of Older Person's Prescriptions criteria (START/STOPP criteria), medication appropriateness index (MAI) are the cancer nonspecific tools to identify PIM among cancer patients. Here, we provided an integrative approach and algorithm for deprescribing in oncology setting which includes patient and caregiver goals, life expectancy (LE), review of medications, determining medication appropriateness, assessment of time to benefit (TTB), symptomatic and asymptomatic care, identifying medications to cease, implementation of the plan, monitoring and reviewing.
Conclusion
Deprescribing in oncology setting is a novel and effective patient-centric approach to counteract the use of PIM, which helps to mitigate polypharmacy, drug–drug interactions, and adverse effects.
Introduction
Cancer is among the most devastating group of human illness, exhibiting with millions of deaths across the globe. 1 The burden of cancer incidence and mortality is rapidly growing worldwide. In 2020, 18.1 million new cases and 10.0 million cancer-related deaths were reported globally. However, it is anticipated that there will be 16.4 million cancer-related deaths and 28.4 million new instances of cancer by 2040. 2 Breast, lung, colorectum, stomach and prostate cancers are among the most prevalent types of cancer with an occurrence rate of 46%. 3 Cancer exhibits with a wide array of clinical presentations, which could ultimately hinder the patient's daily functioning and quality of life. Typically, surgery, radiation and/or systemic therapy (chemotherapy, hormonal treatments, targeted biological therapies) are used effectively in the management of cancer patients. 4
Patients with cancer are often prescribed with medications to alleviate the initial symptoms, followed by a chemotherapy and supportive medications. 5 In addition, multimorbidity is a health crisis that affects the individuals and challenges health care system. Risk of multimorbidity is significantly high in cancer patients. 6 Data suggests that cancer patients are 30% more likely to have multimorbidity compared to non-cancer patients. 7 Hence, multimorbidity patients are often exposed to polypharmacy as most of the comorbid conditions are managed by medications. 8 Polypharmacy often leads to the development of drug interactions and serious adverse drug reactions (ADRs). 9 Furthermore, polypharmacy increases the risk of patient getting prescribed with potentially inappropriate medications (PIMs). 10 In older adults with cancer, the incidence of PIM was between 41% and 52%. 11 Polypharmacy at the end of life has been associated with significant symptom burden and decreased quality of life. Another aspect is that patients at the end stage often require medications to manage various symptoms. 12 Hence, oncologists might have a dilemma in determining the rationality of non-cancer specific medications. 11 A range of tools have been developed to assist the physician in evaluating the appropriateness of a therapy and to overcome the problems associated with polypharmacy. The most commonly used approach in cancer patients is deprescribing of drugs.
Deprescription is a systematic process of identifying and discontinuing drugs in instances in which existing or potential harms, outweigh existing or potential benefits within the context of an individual patients’ goals. 13 This approach has been shown to reduce the pill burden in patients with limited life expectancy and improve overall quality of life. 14 Hence, we conducted a review of deprescribing strategy and proposed an integrative approach and algorithm that could ease the physician in overcoming polypharmacy.
We conducted a general search in PubMed, Scopus, and Google Scholar using “deprescribing,” “potentially inappropriate medication” and “cancer” as a keyword to retrieve articles on guidelines or tools used to deprescribe in cancer care.
Deprescribing in oncology: what is known to date?
The increasing pharmacotherapeutic burden by polypharmacy may result in non-adherence to the recommended course of treatment, and increased risk of drug-related toxicities. Also, when patients reach the terminal stage of illness, their responses to medications vary which is certainly due to variations in pharmacokinetic properties. 15 In light of these, it has been suggested that medication use in patients with life limiting illnesses should be routinely assessed for potentially inappropriate or unnecessary medications to reduce polypharmacy and complications associated with it. Henceforth, certain tools (Beer's criteria, MAI and START/STOPP criteria, Oncpal guideline, OncoSTRIP) have been developed to assist healthcare practitioners. 16
Tools specifically for cancer patients
Oncpal guideline
Cancer patients switched from curative chemotherapy or radiotherapy to palliative care continue taking drugs with possible side effects or no immediate benefit. Given that, patients with shorter life expectancy continue to get a wide range of drugs even after switching to palliative care in an effort to avoid comorbid conditions. After this transition is made, the patient's quality of life should be the main focus of care, along with easing cancer-related symptoms and managing comorbid disease. 17 According to a recent review potentially inappropriate medicines are common in palliative cancer patients. 18 Furthermore, there were no reports evaluating the effects of terminating PIMs in patients with palliative cancer. A study conducted by Lindsay et al., developed a specialized oncological palliative deprescribing guideline that assists in identifying PIMs to aid in the rationalization of medicines. 19
In addition, the European Pharmaceutical Market Research Association's anatomical categorization list was used to systematically review each medication class to develop a distinct tool for medication de-escalation i.e., OncPal deprescribing guideline with an acceptance rate of 94%.19,20 The high prevalence of PIMs among palliative cancer patients—70% of whom took at least one PIM—indicates the potential benefits of using guidelines in clinical practice. 20
OncoSTRIP
The OncoSTRIP polypharmacy assessment tool is used for discontinuation of potentially inappropriate medications with respect to a limited life expectancy. 21 STRIP consists of five steps: (a) questioning the patient about their medication use, (b) conducting a structured pharmaceutical analysis by a pharmacist, (c) agreeing on an optimized treatment plan by physician and pharmacist, (d) making the new treatment plan definite through shared decision-making with the patient and (e) following up and monitoring. 22 While STRIP is already commonly used in Dutch primary care, the method can be specified for cancer patients. In 2019, Elze Vrijkorte et al., developed “OncoSTRIP,” a polypharmacy evaluation technique specifically designed for cancer patients by focusing on optimizing their medication regimen. The objective is to seamlessly incorporate this method into the standard care provided to older individuals diagnosed with cancer. 21 Future studies are needed to identify possible high-risk subpopulations and to assess the effects of OncoSTRIP polypharmacy on patients’ outcomes. 21
Steps involved in oncoSTRIP deprescribing
Polypharmacy anamnesis
The polypharmacy anamnesis step's objective was to compile all pertinent data regarding the patients’ medication usage. The following details were covered: drug type, dosage, indication, start date, initial prescriber, effect, adverse drug effects, practical issues (such as compliance), and, if pertinent, additional medical history information. 21
Concise geriatric assessment
Adult comorbidity evaluation 27 (ACE 27), Eastern Cooperative Oncology Group performance status were the scoring systems used in the concise geriatric assessment, to evaluate comorbidity, performance and frailty, respectively.23,24
Polypharmacy analysis
The pharmaceutical analysis was framed by the assessment of eight potential drug-related problems (DRPs): the need for additional drug therapy, the need for unnecessary drug therapy, ineffective treatment, (potential) adverse effects, clinically relevant contraindications or interactions, under- or overdosing, and practical drug use issues/optimizations. A recently developed “OncoSTRIP list of medications eligible for deprescribing in older cancer patients” allows to identify PIMs and classify them among the potential DRPs. 21
Polypharmacy treatment plan
Following the analysis, the treating oncologist and hematologist were given access to the patient's electronic medical record to review the pharmacist's suggestions. The treating doctor went over the planned drug changes with the patient, after the patient accepted the recommendations. 21
Tools non-specifically for cancer patients
Beers criteria
The Beers criteria is a frequently used method to deprescribe in the overall geriatric population. The Beers criteria are commonly applied on the palliative cancer population although it has been developed for the geriatric population. Zhou et al. used the Beers criteria to estimate the frequency of six specific classes of PIMs in chemotherapy order templates for hematologic malignancies. 25 In 45% of these order templates, medications considered as PIMs by the Beers criteria were found. However, it could also be considered that the Beers criteria are not a perfect match to deprescribe in the cancer. 26
START/STOPP criteria
ADRs in older people currently represent a serious and growing public health problem. 27 Polypharmacy and inappropriate prescribing (IP) are wellknown risk factors for ADRs, which commonly cause adverse clinical outcomes in older people. 28 IP encompasses PIMs and potential prescribing omissions (PPOs). STOPP/START criteria for potential IP in older people recognize the dual nature of IP by including a list of PIMs (STOPP criteria) and PPOs (START criteria). 29
Medication appropriateness Index
The medication appropriateness index (MAI) is a questionnaire to assess the futility of the drugs used. It can be used to determine why the discontinued drug was inappropriate. Domingues et al. applied a modified version of MAI for cancer patients at the time of palliative care transition in a prospective study. They included 71 patients and found polypharmacy in 85% of cases. Using the MAI, 28% of drugs used could be suspended. 30
Our approach towards deprescribing in oncology set-up or oncology pharmacy practice
Patient and caregiver goal
The frequent continuation of potentially ineffective therapies may also be the result of poor communication and insufficient shared decision-making between patients and prescribers. To overcome this situation, deprescribing calls for prompt patient-family-physician discussion of the risk/benefit ratio of drugs and careful observation of symptoms during the following weeks. The goals of care should be periodically reevaluated when the situation gets worse to make sure the treatment target stays in line with the patient's preferences. 23
In certain circumstances, the benefits of deprescribing medications may exceed the risks; however, patients should collaborate with healthcare providers to determine which medications can be stopped. This is critical because patients should be at the Centre of every deprescribing decision. 16
In some patients deprescribing may be viewed as threatening and a sign that the doctor has “given up” on the patient. Hence, it's critical to inform the patient and their loved ones that the medication's intended purpose has altered and that it now poses a greater risk of harm than good. Several patients also frequently find it relieving to avoid taking a lot of pills. The deprescribing process should ideally be carried out with the patient's and/or their families consent to ensure that it is as safe and effective as possible without adversely affecting the patient's quality of life (QoL). 12
Life expectancy (LE)
This may be computed using internet calculators (https://eprognosis.ucsf.edu/calculators/) which provides projected individual survival rates. For instance, those with cancer and other concomitant conditions including hypertension, diabetes, and high cholesterol have an estimated average LE of fewer than 8 years. Therefore, it is obvious to avoid or stop taking drugs intended to prolong life or prevent disability, especially when the amount of time required to obtain the anticipated benefits from the drugs exceeds the estimated life expectancy of a particular person and when they do not provide symptomatic benefits. 31
For example, A study included adults with a life expectancy of one month to one year, randomly divided between whether to continue or discontinue statins, suggested that stopping statins is safe and may have benefits such as improved quality of life, the need for fewer non-statin medications, and a corresponding reduction in medication costs. 32
Review medications
The pharmacist should review all drugs and determine whether the patient is taking any over-the-counter (OTC) or substitute medications in addition to the ones that have been prescribed. 11 A list of medications can be utilized, although lists omit current medication with a frequency that can be as high as >80% in older people. If patients are asked to bring all their medication to consultations, the accuracy of the correct record of the medications they are taking greatly improves. 32
Medication appropriateness
There are several factors for determining whether drugs may no longer be necessary or in which the risk of damage may outweigh the risk of benefit. Although these lists are useful in recognizing drugs that might be inappropriate, each drug needs to be examined based on its indication, the patient's level of symptom intensity, the goals of therapy, and life expectancy using Beer's criteria, MAI, START and STOPP Criteria, OncPal guideline and oncoSTRIP. 11
Time to benefit
The two key factors that must be taken into account in patients with life-limiting illnesses, including cancer, are time to benefit (TTB) and life expectancy (LE). TTB can be described as the amount of time it takes for a drug's anticipated benefits to occur. TTB is often not applied to symptom-driven treatment when TTB = 0. For instance, analgesics for low back pain may result in renal insufficiency, but the analgesic's benefits set in right away. TTB is a concept applied to preventative treatments that have immediate risks but delayed benefits.
For instance, glycemic therapy for diabetes may result in acute hypoglycemia and fewer vascular problems years down the road. When an intervention has an immediate risk and a delayed benefit, it is preventive and ought to be targeted at older persons with an LE that is higher than the TTB. LE > TTB, the drug may be beneficial and should be continued. However, the physician must also consider whether time to benefit is less than time to harm (TTH) (TTB < TTH). When LE = TTB, the physician should respect the values and choices of the patient and their family. As estimations of LE and TTB are derived from population estimates, there may be ambiguity when applying to specific individuals. Patient goals and preferences should always be taken into account when there is uncertainty. 33
The “time to benefit”—a phrase employed within the framework put forward by Holmes et al., and defined as the period of time it takes for a population to experience the desired impact of the drug—is another consideration of appropriate medication use in patients with life-limiting illnesses. Certain medications that are frequently recommended to treat comorbid illnesses have a “time to benefit” that can range from several months to years. For example, statins are frequently prescribed for the primary prevention of cardiovascular disease but offer no particular benefits for patients in terms of symptoms. Depending on the outcome and indication, statins’ expected TTB is greater than 2 years. In many cases, this may extend beyond the patient's life expectancy, which calls into doubt the treatment's risk to benefit ratio. 16
Symptomatic and asymptomatic oriented care
The management of various chronic asymptomatic conditions in older adults entails both immediate risks and delayed benefits, similar to preventive measures. For instance, treating hypertension can lead to sudden orthostatic hypotension and falls, while reduced cardiovascular outcomes may take months or even years to manifest. Similarly, glycemic treatment for diabetes can cause immediate hypoglycemia, with a decrease in vascular complications observed in the distant future. In situations where an intervention carries immediate risks but offers delayed benefits, it should be considered preventive and targeted towards older adults with a longer life expectancy that surpasses the time required to achieve those benefits. In light of this, the framework for individualized prevention also applies to the management of a wide range of illnesses in older people. TTB is not taken into account in symptom-oriented care, in contrast to the treatment of asymptomatic disorders, because the harms and benefits occur immediately. Any treatment to a bothersome symptom could result in immediate benefits for the patient, hence the TTB is 0. For instance, analgesics for low back pain may result in renal insufficiency, yet analgesia has immediate positive effects. TTB and the framework that connects LE and TTB are therefore not useful for symptom-focused therapy. 31
According to previous reports, taking a lot of medications at the end of life has been associated with elevated symptom burden and a lower quality of life. Another factor is that patients receiving end-of-life care frequently require medications to treat a variety of symptoms; as a result, deprescribing unnecessary medications is important to prevent polypharmacy. The patient's exposure to a greater number of medications also increases the chance of drug interactions. Hence, it is crucial to give priority to medications like pain relief, anxiolytics, and antiemetics that can alleviate symptoms right away.12,14
Identify medications to cease
A multidisciplinary team discussion aids in determining which medications to stop using;
Drugs with no obvious benefits: It is vital to address medication that: takes a long time until benefit, outside of the patient's expected lifespan, such as statins that take longer than a year to provide a benefit, being ineffective in patients with a short expected survival time; has no known benefit after a particular age, independent of the patient's life expectancy, such as bisphosphonates that do not protect women over 80 who have never had a hip or vertebral fracture from hip or spinal trauma.
32
Drugs with undesirable adverse effects are no longer indicated and those that are inappropriate in older people such as those on the beers criteria, MAI, START and STOPP criteria, OncPal guideline, oncoSTRIP.11,34
Plan and implement cessation
The medications without a clear benefit and some of the medications with undesirable adverse effects can be selected for deprescribing
There are certain drugs that need to be scaled down, in order to avoid causing withdrawal symptoms or disease recrudescence. These include alpha-blockers, antidepressants, anti-convulsant, antipsychotics, digoxin, and benzodiazepines. These can cause serious side effects if they are abruptly stopped. Family members and patients should be informed about the possible side effects of these drugs and how to react in case of occurrence of such a problem. 16
Consider stopping medication one at a time. 11
Monitor and review
The team's pharmacist takes a leading role in monitoring for symptom return and reviewing medications against current symptoms and goals of care.
25
The process of deprescribing should be monitored carefully in follow-up appointments to identify clinical problems that may occur and to respond to misunderstandings and doubts about the process that may arise
Application or step-wise procedure to practice deprescribing from our study
Many practical deprescribing principles can be applied to the last year of life. The initial step is to ensure an accurate record of current medications, followed by confirming the necessity of each medication and identifying the associated disease state. Additionally, it is important to assess compliance and the presence of adverse reactions. Based on this information, medications that are no longer necessary or unsuitable for older individuals (according to the Beers criteria, MAI, START and STOPP Criteria, OncPal guideline, oncoSTRIP) should be identified and ceased. Simplification of the drug regimen, ideally to once daily, should be attempted and any changes made in collaboration with the patient and caregiver, with frequent follow-up and support. It is essential to gradually wean off medications such as benzodiazepines, anticholinergics, and steroids over several weeks to minimize the risk of adverse withdrawal effects. To avoid complications, it is advisable to modify one or two medications at a time since the number of medications discontinued may predict the occurrence of withdrawal effects. Some of these medications are recognized as inappropriate for older patients, and it should be noted that despite the challenges of withdrawal, the benefits of discontinuation may outweigh the difficulties. With this background, we present a framework/algorithm for deprescribing among the cancer patients and their end stage of life (Figure 1).
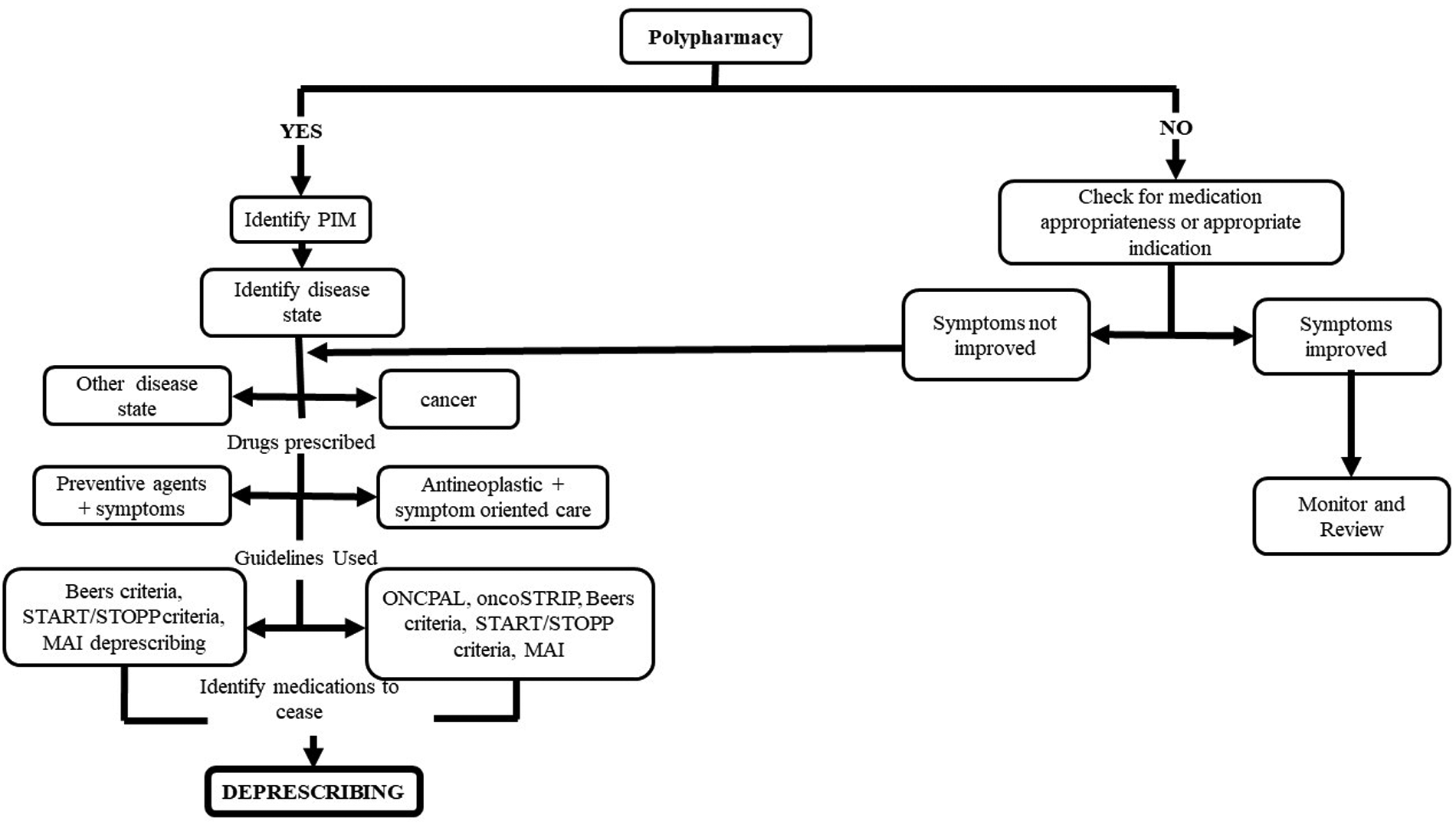
Algorithm for deprescribing practice in oncology care.
Conclusion
Multimorbidity in patients with cancer can lead to adverse drug events, polypharmacy, prescribing of PIMs and potential drug–drug interactions. A patient-centric approach towards deprescribing can rationalize medication use, aligning each medication with the patient's goals of care. Tools and resources for both clinicians and patients can support the process of deprescribing, with the goal of minimizing harm and improving quality of life.
Footnotes
Authors’ contributions
Concept: RKC and UVM; literature Search: BR and RKC; literature review: BR, AL, and AB; writing original draft: BR, AL, and AB; editing and review: RKC and AS. UVM holds the final responsibility of the article.
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.