
Abstract
Introduction
There remains a need to determine whether certain subgroups of newly diagnosed multiple myeloma (NDMM) derive the same benefit from high-dose chemotherapy–autologous stem cell transplant (HDT-ASCT). We describe our institutional experience highlighting the impact of age, obesity, and renal impairment on outcomes after HDT-ASCT for patients with NDMM in a real-world setting.
Methods
A total of 449 consecutive patients were included in this retrospective analysis.
Results
No difference in median progression free survival or overall survival was seen for patients with age > 65, body mass index (BMI) > 30 kg/m2, or estimated glomerular filtration rate < 60 mL/min/1.73 m2 when compared to those without these characteristics. From a safety standpoint, there were no differences in the incidence of transplant-related mortality or secondary malignancy among subgroups.
Conclusion
For patients with NDMM undergoing HDT-ASCT, there is no difference in outcomes based on age, BMI, or renal function, and the presence of one or more of these factors should not preclude patients from HDT-ASCT.
Introduction
Induction chemotherapy followed by high-dose chemotherapy and autologous stem cell transplant (HDT-ASCT) with subsequent maintenance therapy is a standard of care for patients with transplant-eligible newly diagnosed multiple myeloma (NDMM).1–3 Moreover, clinical trials have investigated novel induction regimens with incorporation of an anti-CD38 monoclonal antibody to a triplet backbone of lenalidomide, bortezomib, and dexamethasone as well as second-generation proteasome inhibitor carfilzomib-based combinations leading to improvement in depth and duration of response.4–6 While these landmark clinical trials have influenced the treatment paradigm for NDMM, they have historically excluded or underrepresented patients who are elderly, obese, or have renal impairment due to concern for excessive toxicities. With a median age of 69 years at the time of diagnosis, as well as renal failure being one of the presentations for NDMM, patients with these characteristics represent the real-world population seen in everyday clinical practice. 7 Obesity continues to be a major health comorbidity in the United States with potential impact on chemotherapy dosing and outcomes after ASCT. Retrospective studies and registry-based analyses have addressed outcomes in some of these categories, however, these studies are limited by inclusion of heterogenous patient populations, variations in institutional practices related to transplant, and patient selection bias influencing outcomes. Hence, there remains a need to determine whether age, obesity, or renal dysfunction influence outcomes after HDT-ASCT for patients with NDMM and whether findings of these previously reported studies are replicated in a real-world setting.
Methods
This retrospective, single-center study was conducted to analyze the impact of patient characteristics including older age, defined as patients >65 years, obesity, defined as body mass index (BMI) ≥ 30 kg/m2, and impaired renal function, defined as estimated glomerular filtration rate (eGFR) < 60 mL/min/1.73 m2 at the time of ASCT, on clinical outcomes after HDT-ASCT. All adult patients at the Medical University of South Carolina with NDMM who underwent HDT-ASCT between February 2012 and August 2022 were included. Approval was obtained from the institutional review board with the study conducted according to the Declaration of Helsinki. Patients were included if they had NDMM and had undergone induction chemotherapy followed by HDT-ASCT with day +100 response available at the time of data cutoff. HDT was administered as a one-time intravenous (IV) infusion of melphalan. Melphalan was given at a dose of either 200 mg/m² or 140 mg/m² with the total dose based on adjusted body weight with a 25% correction factor (adjusted body weight 25 = ideal body weight +0.25 (actual body weight – ideal body weight)). ASCT was performed either in the inpatient or outpatient settings based on physician discretion. Supportive care and infectious prophylaxis were administered as per institutional guidelines and standard operating procedures. Patients initiated maintenance chemotherapy at or around day +100 post-ASCT. The choices of induction and maintenance regimens, transplant eligibility, and melphalan dosing (standard or reduced) were physician dependent and underlying rationale for physicians’ decision could not be accurately determined due to the retrospective nature of the study. Relevant data pertaining to patient demographics, disease characteristics, performance status, comorbidities, treatment history, and safety and efficacy outcomes were extracted by investigators from the electronic health record (EHR). Adverse events were graded based on Common Terminology Criteria for Adverse Events (CTCAE) v5.0. 8 Responses were assessed based on International Myeloma Working Group Response criteria 9 at different time points including prior to HDT-ASCT, day +100 post-ASCT, and then yearly post-ASCT. Overall survival (OS) was calculated as the time from initiation of induction chemotherapy to death or last contact, and progression free survival (PFS) was calculated as the time from initiation of induction chemotherapy infusion to disease progression, death, or last contact.
Data are presented as counts with percentages for categorical variables and medians with ranges for continuous variables. Categorical variables are compared between cohorts using chi-square or Fisher exact tests, with continuous variables compared using Mann-Whitney U tests. Kaplan-Meier survival curves and log-rank tests were used to examine OS and PFS by age, BMI, and renal function. Cox proportional hazards regression models were used to estimate hazard ratios (HR) and 95% confidence interval (CI) for age, BMI, and renal function with OS and PFS while adjusting for disease stage, cytogenic risk profile, induction and maintenance treatment, best response, and melphalan dose. A p-value <0.05 was considered statistically significant and analyses were conducted in SPSS v28.
Results
At the time of data cutoff, a total of 449 consecutive patients with NDMM patients had received HDT followed by ASCT. Of these 449 patients, 154 (34%) were older than 65 years at the time of ASCT. Additionally, 205 (46%) were identified to have a BMI ≥ 30 kg/m2 and 72 (16%) patients had renal impairment at the time of HDT-ASCT. Median follow up for the entire patient population was 29 months (range 1–128 months). Baseline characteristics of these patients for each of the category are shown in Table 1.
Baseline patient and disease characteristics.
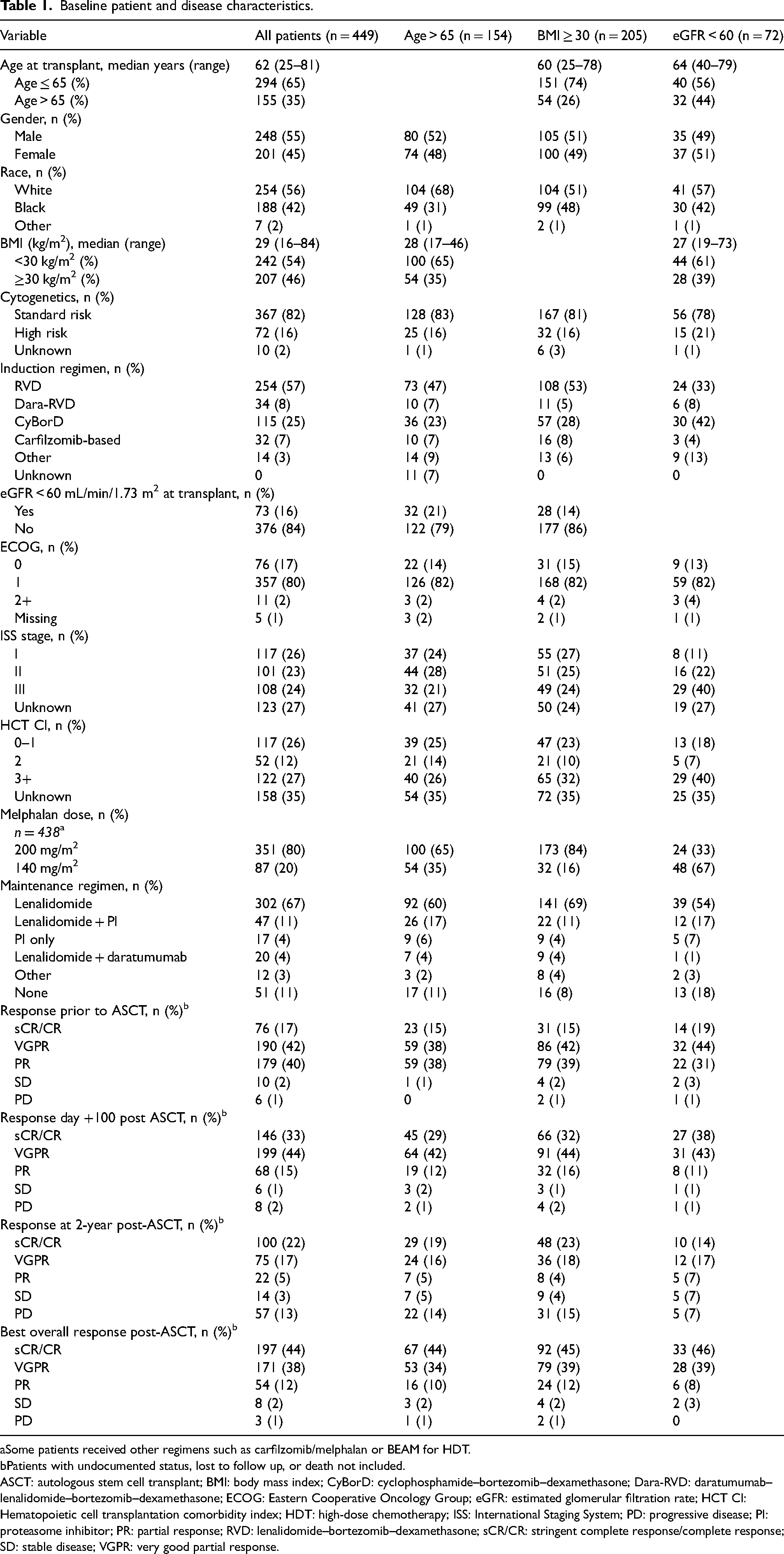
Some patients received other regimens such as carfilzomib/melphalan or BEAM for HDT.
Patients with undocumented status, lost to follow up, or death not included.
ASCT: autologous stem cell transplant; BMI: body mass index; CyBorD: cyclophosphamide–bortezomib–dexamethasone; Dara-RVD: daratumumab–lenalidomide–bortezomib–dexamethasone; ECOG: Eastern Cooperative Oncology Group; eGFR: estimated glomerular filtration rate; HCT CI: Hematopoietic cell transplantation comorbidity index; HDT: high-dose chemotherapy; ISS: International Staging System; PD: progressive disease; PI: proteasome inhibitor; PR: partial response; RVD: lenalidomide–bortezomib–dexamethasone; sCR/CR: stringent complete response/complete response; SD: stable disease; VGPR: very good partial response.
Best overall response rates (ORR) post-ASCT were 95% in both patients ≤65 and >65 years of age with similar rates of very good partial response (VGPR) in age ≤ 65 (38%) and age > 65 (40%) (p-value = 0.69) at day +100 post-ASCT (Table 2). Median PFS was numerically higher in patients ≤65 years of age (52 months, range 0.5–86) compared to patients >65 years of age (50 months, range 1–97), but these differences were not statistically significant (p = 0.44) (Figure 1). Median OS was not reached in patients ≤65 years of age (range 0–123) and was 83 months (range 0.5–128 in patients >65 years of age). This difference in OS was not statistically significant (p = 0.67) (Figure 1). From a safety standpoint, transplant-related mortality (TRM) was seen in 3 patients (1%) ≤65 years of age compared to 4 patients (2%) >65 years of age. Secondary hematological malignancies including myelodysplastic syndrome/acute myeloid leukemia (MDS/AML) were seen in 5 patients (2%) ≤65 years of age compared to 2 patients (1%) >65 years of age.
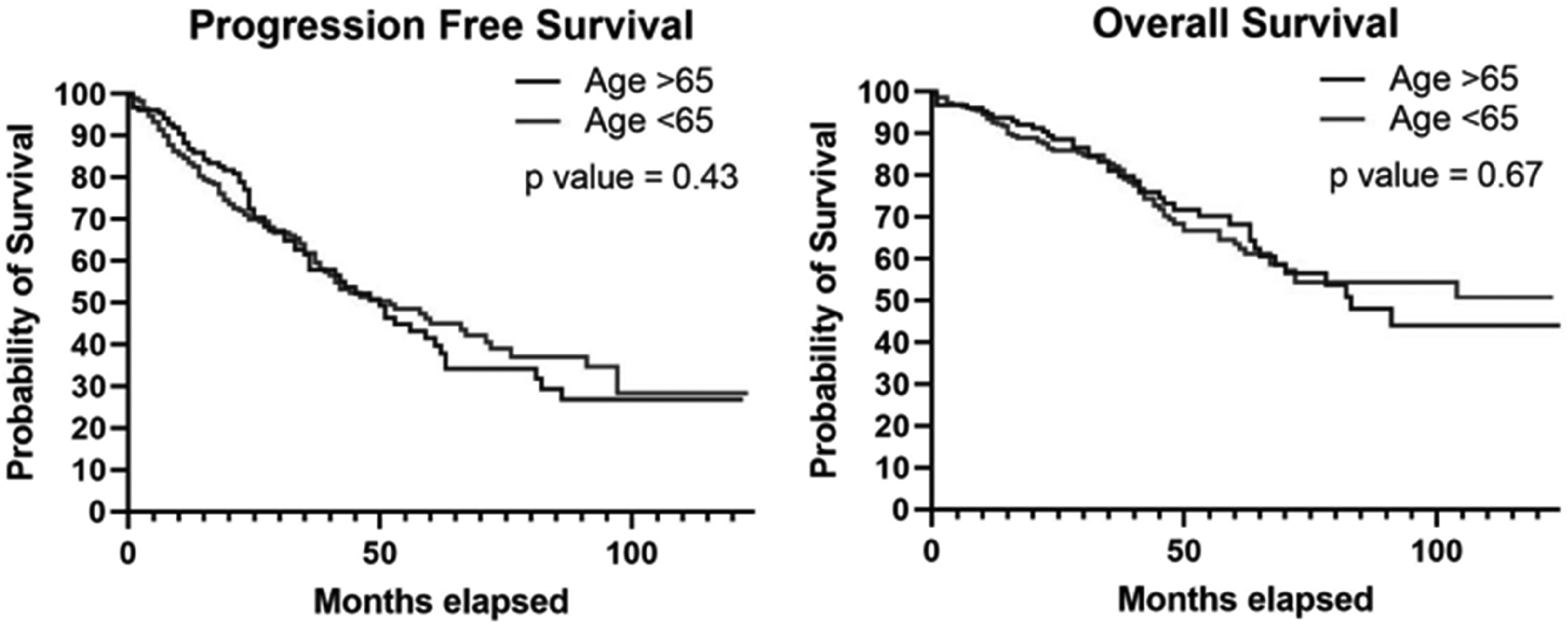
PFS and OS based on age. OS: overall survival; PFS: progression free survival.
Survival outcomes and response rates by factors of age, renal function, and BMI.

,BMI: body mass index; eGFR: estimated glomerular filtration rate; NR: not reached; PFS: progression free survival; ORR: overall response rate; OS: overall survival; VGPR: very good partial response.
When analyzing for renal function at the time of ASCT, best ORR post-ASCT were similar for patients with eGFR < 60 mL/min/1.73 m2 and those with eGFR > 60 mL/min/1.73 m2 (93% vs. 95%, respectively, p-value = 0.65). Similarly, at day +100 post-ASCT, VGPR was seen in 39% and 38% of the patients in the impaired and normal renal function groups, respectively (p-value = 0.91). Median PFS was 53 months (range 0.5–67) in patients with eGFR < 60 mL/min/1.73 m2 compared to 50 months (range 0.5–97) in patients with normal renal function, and this difference was not statistically significant (p = 0.64) (Figure 2). Median OS was 70 months (range 0.5–128) in patients with eGFR < 60 mL/min/1.73 m2 compared to 104 months (range 0.5–123) in patients with normal renal function (p = 0.16) (Figure 2). From a safety standpoint, TRM was seen in 4 (5%) patients with eGFR < 60 mL/min/1.73 m2 compared to 3 (1%) patients with normal renal function. Secondary MDS/AML were seen in 2 (3%) patients with eGFR < 60 mL/min/1.73 m2 compared to 5 (1%) patients with normal renal function.

PFS and OS based on renal function. OS: overall survival; PFS: progression free survival.
While evaluating BMI impact, best ORR post-ASCT was 94% in patients with BMI ≥ 30 kg/m2 compared to 95% in patients with BMI < 30 kg/m2 (p = 0.69). At day +100 post-ASCT, VGPR was seen in 38% of patients with BMI > 30 kg/m2 and 40% of patients with BMI < 30 kg/m2 (p = 0.69). Median PFS was numerically superior in patients with BMI ≥ 30 kg/m2 (58 months, range 1–97 months) compared to patients with BMI < 30 kg/m2 (48 months, range 0.5–97 months), but these differences were not statistically significant (p = 0.21) (Figure 3). Median OS was not reached (1–123 months) in patients with BMI ≥ 30 kg/m2 and was 82 months (range 0.5–128 months) in patients with BMI < 30 kg/m2 (p = 0.36) (Figure 3). From a safety standpoint, TRM was seen in 3 (1%) patients with BMI ≥ 30 kg/m2 compared to 4 (2%) patients with BMI < 30 kg/m2. Secondary MDS/AML were seen in 2 (1%) patients with BMI ≥ 30 kg/m2 compared to 5 (2%) patients with BMI < 30 kg/m2.
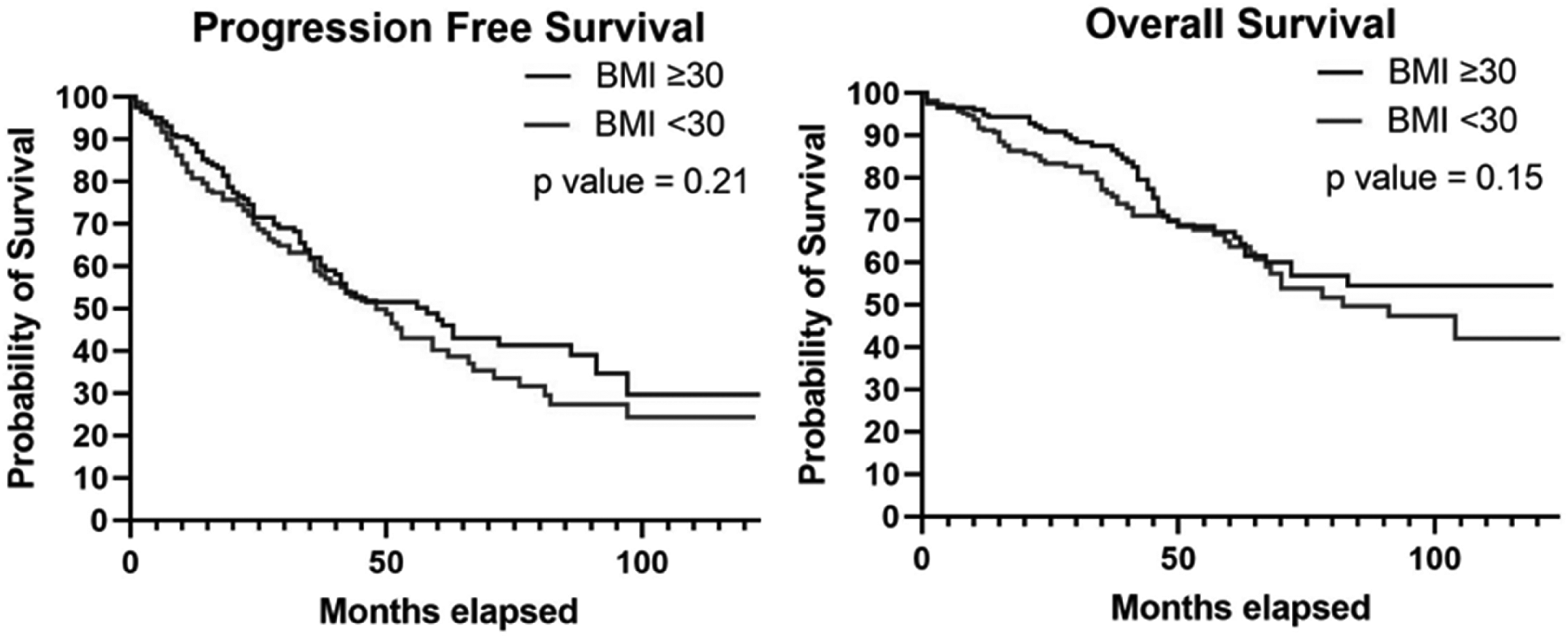
PFS and OS based on body mass index. OS: overall survival; PFS: progression free survival.
In the univariable analysis for the entire population, high-risk cytogenetics, defined as presence of deletion 17p, t(4;14), or t(14;16), (HR = 2.121, CI 1.499–3.003) and less than VGPR as best response (HR = 3.328, CI 2.388–4.637) were associated with inferior PFS whereas use of single agent lenalidomide maintenance was associated with superior PFS (HR = 0.639, CI 0.469–0.871) and OS (HR = 0.642, CI 0.436–0.945). Older age, obesity, and renal dysfunction at the time of ASCT were not found to have any statistically significant impact on PFS or OS (Table 3). After adjusting for other factors including disease stage, cytogenetics, melphalan dose, and induction and maintenance regimens, a multivariable analysis showed only eGFR <60 mL/min/1.73 m2 was associated with longer PFS (HR 0.581, CI 0.355–0.954) (Table 4).
Univariate analyses of factors associated with PFS and OS.
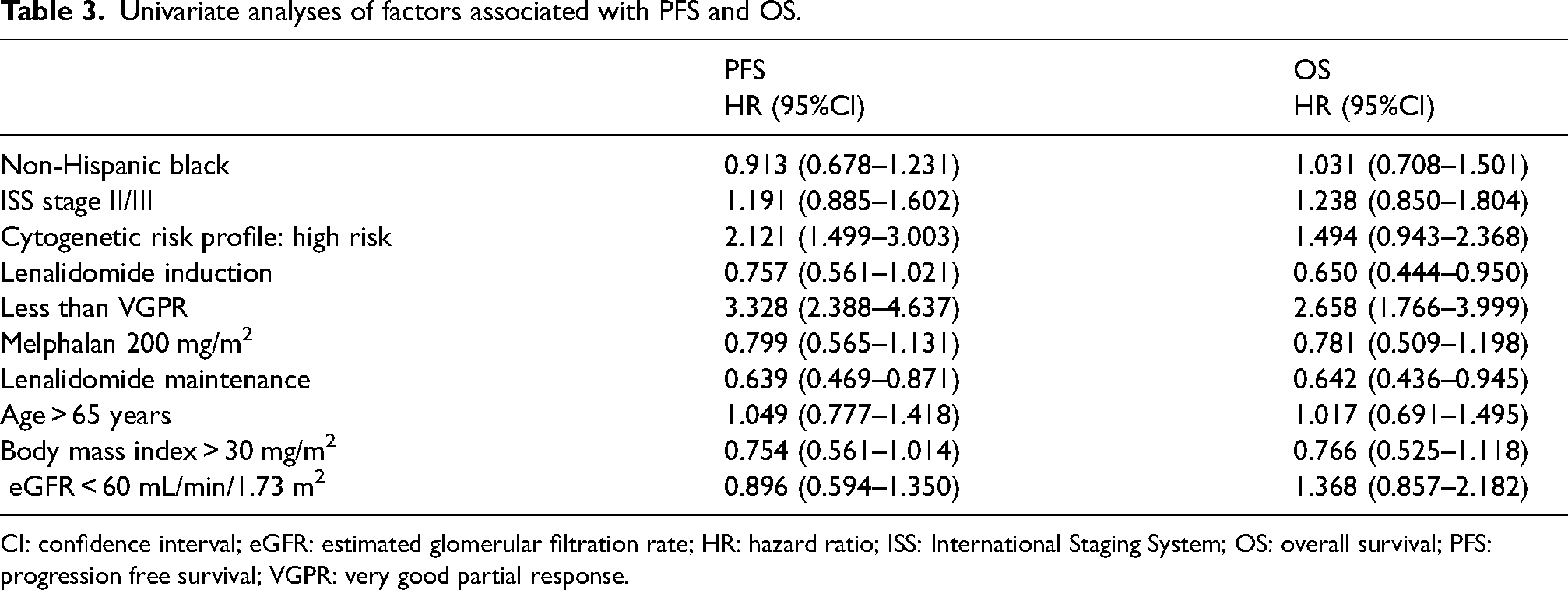
CI: confidence interval; eGFR: estimated glomerular filtration rate; HR: hazard ratio; ISS: International Staging System; OS: overall survival; PFS: progression free survival; VGPR: very good partial response.
Multivariable analyses of factors associated with PFS and OS.
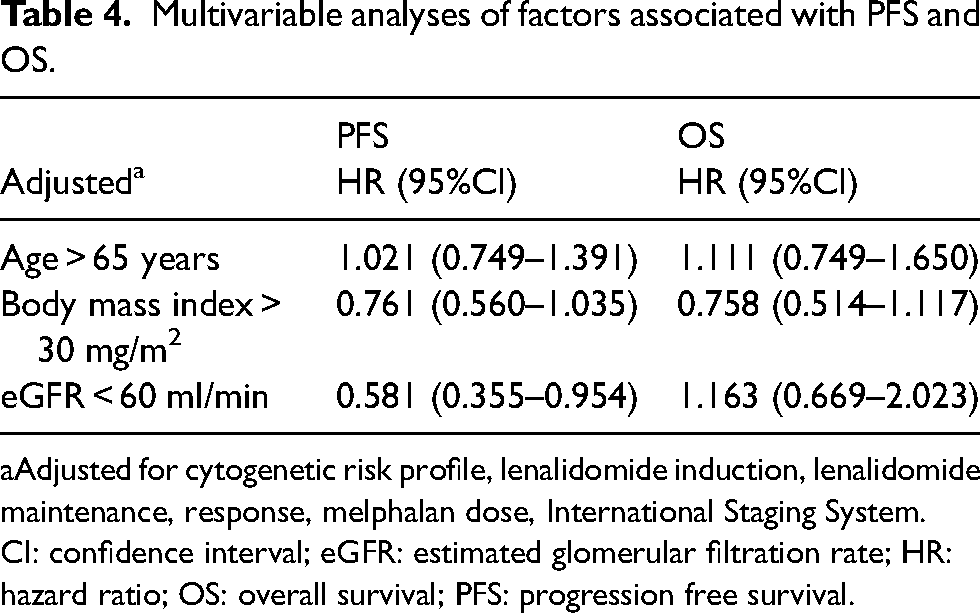
Adjusted for cytogenetic risk profile, lenalidomide induction, lenalidomide maintenance, response, melphalan dose, International Staging System.
CI: confidence interval; eGFR: estimated glomerular filtration rate; HR: hazard ratio; OS: overall survival; PFS: progression free survival.
Discussion
Multiple myeloma is the third most common hematologic malignancy that affects a relatively heterogenous patient population. 9 Induction chemotherapy followed by HDT-ASCT with subsequent maintenance therapy is a standard of care for patients with transplant-eligible NDMM.1–3 Studies evaluating the role of upfront versus delayed transplant for patients with NDMM have clearly demonstrated improvement in PFS without an improvement in OS, establishing the role of HDT-ASCT as an effective treatment modality. Certain patient-related and disease-related characteristics that are likely to impact outcomes after chemotherapy have not been studied comprehensively in clinical trials due to concerns for excessive toxicities. Specifically, the impact of older age, obesity, and renal dysfunction on efficacy and safety of current standard of care HDT-ASCT is of great interest given the incidence and prevalence of these characteristics in patients with NDMM. 9 Our study with single-center data over a period of 10 years demonstrated no differences in the depth and duration of response as well as treatment-related toxicities associated with HDT-ASCT for patients with age >65 years, BMI >30 kg/m2 or eGFR <60 mL/min/1.73 m2.
Median age at the time of diagnosis for multiple myeloma is 69 years with a majority of patients diagnosed in the sixth or seventh decade of life. 9 Attal et al. and Richardson et al. have comprehensively established the role of HDT-ASCT for NDMM such as the DETERMINATION trial and IFM 2009 excluded patients with age > 65, making real-world application of these results unclear.1,3 Hence, we chose age > 65 years as the cutoff to define the elderly to specifically address outcomes in this patient population. With at least one-third of the patients >65 years of age at the time of HDT-ASCT in our study, this analysis provides important clinical information for patients commonly seen in real-world practice. As shown in previous real-world studies, our study affirms the efficacy and safety of HDT-ASCT in older patients and re-emphasizes that age alone should not preclude patients from consideration of this treatment modality. While we used age > 65 as our cutoff, other registry-based studies have used an even higher age cutoff to define older patients (age > 70 years) and found no significant differences in safety and efficacy of HDT-ASCT. 10 On the contrary, hematopoietic cell transplantation specific comorbidity index (HCT-CI) and performance status when evaluated as predictors of outcomes after ASCT showed inferior OS in patients with a higher HCT-CI score and worse performance status. 11 These findings raise the need for using alternative patient and disease-related characteristics to determine transplant eligibility instead of chronological age. Nearly 95% of the patients in our study with age > 65 years had an excellent performance status of Eastern Cooperative Oncology Group (ECOG) 0–1. Although data was missing for HCT-CI in one-third of the patients, 40% of the patients had HCT-CI score of 0 to 2 highlighting the low-comorbidity burden in this elderly patient population. While patient selection for ASCT in our study was physician dependent and cannot be reliably determined in a retrospective analysis, it is important to highlight that factors like performance status and comorbidity burden were likely determinants of patient eligibility for ASCT. Moreover, at least one-fifth of the patients had dose modification of melphalan to 140 mg/m². This could be explained by the comorbidity burden and performance status of the patient population that commonly influence melphalan dosing. Due to a small number of patients with worse performance status (2 or higher) and missing data on HCT-CI, we cannot reliably validate the impact of performance status and HCT-CI on outcomes in our study.
Obesity continues to be a major healthcare issue in the United States. According to 2017–2018 data from the National Health and Nutrition Examination Survey (NHANES), more than 2 in 5 adults (42.5%) are considered obese. 12 The role of obesity in plasma cell disorders and underlying pathophysiological mechanisms of myelomagenesis have been thoroughly investigated by Parikh and colleagues and obesity was noted to increase the risk of transformation of monoclonal gammopathy of unknown significance to symptomatic multiple myeloma and possibly lead to poor outcomes in patients undergoing HDT-ASCT. 13 Given the increased prevalence of obesity in the United States and its potential implications for therapies and disease outcomes, assessing the impact of obesity on safety and efficacy of treatment options for patients with NDMM is of great importance. Historically, obesity has had implications for patient selection and chemotherapy dosing in patients undergoing HDT-ASCT. A large registry-based analysis did not reveal an overall effect of BMI on PFS, OS, or nonrelapse mortality. 14 Our findings indicate that obese patients can receive high-dose melphalan without increased TRM, and obesity should not be a contraindication to undergoing autologous transplantation. One of the strengths of our analysis includes data from a single institution with no heterogeneity in weight used (actual, ideal or adjusted) for chemotherapy dosing as commonly seen in larger registry-based studies. Due to small sample size, we could not study the impact of extremes of weight (underweight or morbidly obese) on outcomes.
Renal impairment is a frequent presentation at diagnosis in patients with multiple myeloma and is associated with adverse prognostic consequences. 9 Although renal impairment, if mild to moderate, is not associated with an increased risk of TRM after ASCT, it leads to more myelosuppression and gastrointestinal toxicities. 15 These patients are often considered ineligible for HDT-ASCT and especially excluded from clinical trials due to concerns for excessive toxicities. Hence, it remains unclear whether renal impairment truly has a negative prognostic impact on long-term outcomes in multiple myeloma if these patients are offered effective therapy. Previously published registry-based analysis and multicenter retrospective study have shown HDT-ASCT is safe and effective in patients with moderate and severe renal insufficiency without excessive TRM.16,17 Similarly, while renal impairment at the time of diagnosis conferred inferior OS, multiple myeloma progression after transplant was not affected by any stage of renal failure. 17 In our study population, at least 15% of the patients who underwent ASCT had some degree of renal impairment. Our data clearly indicated high-dose melphalan and ASCT is safe in patients with renal impairment with no excessive increase in the incidence of TRM. Multivariable analysis after adjusting for other patient and disease-related factors affecting outcomes revealed better PFS for patients with renal impairment. This is likely related to sample size and results need to be interpreted with caution. Given that the number of patients with renal impairment were small, a subgroup analysis of outcomes stratified by melphalan dosing was not possible. Due to the retrospective nature of the analysis, no information was available on engraftment kinetics and gastrointestinal toxicities. Moreover, no information was available on improvement in renal function or independence from dialysis post-ASCT. Our analysis indicates that HDT-ASCT remains a safe and effective option for patients with renal impairment provided they have adequate performance status and receive dose-modified melphalan.
There are several limitations in our study that deserve to be highlighted. Although the depth and duration of response with ASCT as seen in our study are similar to what has been reported in clinical trials and other real-world experiences, an inherent limitation of this analysis is its retrospective nature, and hence, the results need to be interpreted with caution. We only included patients that were referred for transplant consultation and eventually underwent ASCT at our center. While there is a fair representation of the elderly, obese, and renally impaired patient population, there is potential bias of excluding many patients who deferred or were deemed ineligible for ASCT due to potential barriers of frailty, medical comorbidities, and poor performance status. The majority of patients received induction and maintenance chemotherapy with community providers and, hence, data on safety of these regimens was not available. Moreover, response assessments were only performed at specific time points for Center for International Blood and Marrow Transplant Research (CIBMTR) reporting (pre-ASCT, day +100, and yearly after ASCT); hence, these response assessments are limited when compared with the prospective settings of a clinical trial. Due to the limitations of a small sample size, we were unable to investigate special subgroups, including very old (age > 75 years), morbidly obese (BMI > 40 kg/m2) or patients with end-stage renal disease on dialysis. This may in turn mask subgroup heterogeneity in the associations of age, obesity, and renal dysfunction with clinical outcomes of ASCT. Nevertheless, our work is strengthened using data from a single center over a period of 10 years, reducing variability of practice patterns and improving reliability of our findings. More importantly, this data set incorporates collaboration of care between community physicians and an academic medical center for patients with NDMM and is a true reflection of the real-world management of these patients. While our findings are supportive of offering equitable access to effective treatment modalities including ASCT to the elderly, obese, and those with renal dysfunction, more research is needed to confirm these findings and elucidate any potential subgroup differences in outcomes in larger sample sizes of patients with these characteristics.
Conclusion
Older age, obesity, and renal dysfunction, although commonly seen in patients with NDMM, had no statistically significant impact on efficacy and safety of HDT-ASCT in a large cohort of patients treated in a real-world setting. With the continued expansion of therapeutic options for multiple myeloma, presence of these risk factors should not preclude patients from receiving effective treatments, including ASCT, in clinical trials as well as routine clinical practice.
Footnotes
Author contributions
JB, KG, AV, and HH wrote the manuscript. All authors were involved with data collection and statistical analysis and reviewed final manuscript before submission.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.