
Abstract
Background
Capsaicin is a highly selective agonist of the transient receptor potential vanilloid 1. The adhesive capsaicin patch provides a high capsaicin concentration (8%) directly in the painful area – its efficacy in benign peripheral neuropathic pain (diabetic neuropathy or postherpetic neuralgia) has recently been described in the literature. However, there is scant evidence of its efficacy in chemotherapy-induced peripheral neuropathy (CIPN). This is a concern for patients with multiple myeloma, who suffer from peripheral neuropathic pain induced by first-line treatments (bortezomib or thalidomide).
Aim
To describe improved control of CIPN in patients with multiple myeloma using adhesive capsaicin 8% patch.
Methods
We opted for a retrospective observational case series. Between October 2017 and October 2020, we collected clinical data from adult multiple myeloma patients affected by CIPN who were administered the capsaicin 8% patch in our palliative care outpatient clinic. We compiled Numerical Pain Rating Scale (NPRS) scores, patients’ medication needs and performance status before and after patch application.
Results
Two women and five men with an average age of 62.85 years received bortezomib. Two patients (28.57% of the sample) also received thalidomide. The average NPRS score before patch application was 6.42/10. Five of the seven patients (71.42%) received a mean daily oral morphine dose of 52.85 mg/day, five (71.42%) received gabapentinoids and one (14.28%) received antidepressants. The average NPRS score decreased to 4/10 seven days after patch application, while the mean daily oral morphine dose remained stable. Performance status improved slightly in two patients (28.57%) and remained stable in the rest. One patient (14.28%) required an extra analgesic dose during patch application.
Conclusions
Capsaicin 8% patch application appears to reduce pain intensity in patients with multiple myeloma suffering from CIPN.
Keywords
Introduction
The Catalan Institute of Oncology (ICO) runs a specialist cancer hospital which has been equipped with an early intervention clinic for multiple myeloma since February 2013, led by the palliative care team and integrated with the clinical haematology service. In 2020, the hospital cared for 280 multiple myeloma patients and their families.
Multiple myeloma is the second most common bone marrow neoplasm and accounts for 10% of all haematologic malignancies worldwide. 1 Despite being incurable, 2 it has a median survival time of 5–10 years which has increased thanks to the latest treatment advances.3,4 In western Europe, around 5 multiple myeloma cases per 100,000 inhabitants are diagnosed each year. 3
Though patients may present few symptoms or remain asymptomatic for long periods, the symptom burden is often high. Prevalence and incidence of pain are 80% and 100%, respectively. 5 Other symptoms in order of prevalence include: tingling in feet and hands; asthenia; insomnia; dyspnoea; loss of appetite; constipation; and emotional disturbances. 6 All such symptoms may be related to peripheral nerve compressions. The high symptom burden warrants a multidimensional assessment and joint follow-up by palliative care teams, preferably early. 7
The published incidence of chemotherapy-induced peripheral neuropathy (CIPN) ranges from 10 to 100% depending on the study. 8 Factors influencing this variability include: (a) type of cytostatic agent; (b) treatment schedule administered (total dose, dose/cycle, number of cycles, infusion time); (c) combinations of cytostatics; (d) tumour type; (e) patient characteristics or concomitant use of other neurotoxic drugs; and (f) CIPN diagnosis and assessment criteria or technique. 9 Several antineoplastic agents are known to cause CIPN (taxanes, vinca alkaloids, epothilone, platinum derivatives, bortezomib and thalidomide). 9
Capsaicin in pain management
The chemical compound capsaicin (8-methyl-N-vanillyl-6-nonenamide) is an oleoresin derived from the hot chilli pepper (capsicum). 10 It is a highly selective agonist of the transient receptor potential vanilloid 1 (TRPV1),11,12 expressed on nociceptors in both the central and peripheral nervous system.10,13–15 This receptor was originally known as vanilloid receptor 1 (VR1) and later formally named TRPV1. 16
TRPV1 receptors are involved in pain transmission and modulation and integration of various painful stimuli. 10 TRPV1 is a non-selective cation channel. When activated by capsaicin, sodium and/or calcium ions flow through TRPV1 into the cell and depolarise nociceptors, leading to action potential firing and, ultimately, an itching sensation. 17 Overstimulation of TRPV1 can cause a reversible reduction of epidermal nerve fibre density and thus a defunctionalisation of nociceptors, which reduces neuropathic pain. 18
Existing evidence on capsaicin in neuropathic pain management
One of the first studies on the general role of topical capsaicin demonstrated that whereas low-dose topical capsaicin has limited efficacy as an analgesic in musculoskeletal and neuropathic pain, high-dose capsaicin, when tolerated, can potentially provide long-term analgesia in certain neuropathic conditions.19,20 The tolerability of the capsaicin 8% patch (CP8), the paucity of systemic effects (these are almost exclusively local) and the decreased need for concomitant systemic analgesics have made it the target of several studies in the last decade that demonstrate its effectiveness in managing neuropathic pain.10,13–15 Some results show that peripheral neuropathy patients treated with CP8 have pain relief within 24 h and improved function and quality of life.14,15,21 High-concentration topical capsaicin patches have several indications for neuropathic pain including postherpetic neuralgia, painful diabetic peripheral neuropathy, complex regional pain syndrome, post-oncological surgery neuralgia, post-amputation pain and craniofacial pain.13,15,22–26
Capsaicin use for management of CIPN has also been established.9,14,15,21,27–29 However, more published evidence is needed.
Case series objectives
The increased use of chemotherapy to tackle the rising neoplasm incidence in Spain will lead to likely occurrence of side effects including CIPN. These side effects will require appropriate management. 30
In this case series, we set out to expand the evidence for using adhesive capsaicin 8% patch in pain management. Specifically, we review and describe the pain control response following CP8 application in multiple myeloma patients with CIPN.
Methodology
Study design
We conducted a single-centre retrospective descriptive analysis of a case series of multiple myeloma patients affected by peripheral neuropathy induced by bortezomib and/or thalidomide. Since few patients receive CP8 treatment currently, we would not have achieved a sufficient sample size to justify a prospective study.
We reviewed the medical records of seven adult patients with no cognitive impairment who received symptom management support in our multiple myeloma early intervention clinic between October 2017 and October 2020. The patients were offered CP8 in addition to conventional CIPN treatment.
Table 1 describes in full the clinical and demographic characteristics of the seven patients. The patients had an average age of 62.85 years. Five patients (71.42%) received bortezomib as monotherapy while two (28.57%) received both bortezomib and thalidomide. Patients also received specific analgesia for peripheral neuropathy and adjuvant treatment prior to patch administration: five patients (71.42%) received gabapentinoids, one patient (14.28%) received antidepressants and five patients (71.42%) received opioids.
Demographic and clinical and characteristics of the sample.
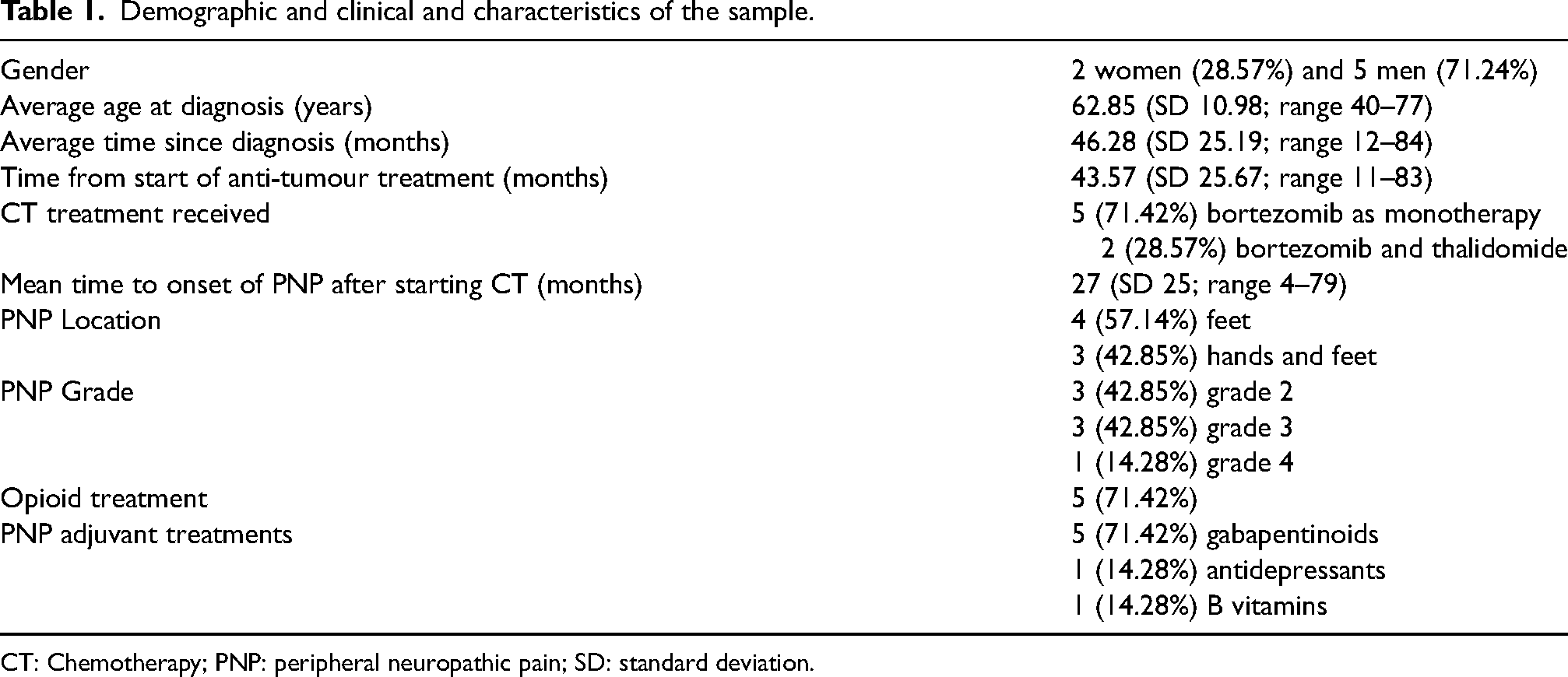
CT: Chemotherapy; PNP: peripheral neuropathic pain; SD: standard deviation.
We wrote to the Institutional Review Board (IRB) prior to conducting our research. Since our case series is a retrospective, observational study based exclusively on medical records and with no risk to patients, the IRB confirmed that their approval was not necessary.
Data collection
We used case report forms to collect patient data. We anonymised the forms and assigned each one a consecutive number. We stored this information in a password protected Excel file along with the matching numbers of patients’ anonymised medical records. Thus, we ensured data anonymisation during the study and ensured an absence of personal information in this manuscript that would enable participants to be identified.
We collected data for a variety of variables:
Patient demographics (sex, age) Multiple myeloma (date of diagnosis, date chemotherapy started) Peripheral neuropathy (location, date of onset, grade 1 to 5 on the NCI-CTC v3 scale)
9
Pain before patch application and post-application pain at 7 days related to CP8 (Numerical Pain Rating Scale (NPRS), total daily oral morphine dose, type and dose of other adjuvant treatments, need for extra doses during patch application) Pre- and post-application functional performance using the Palliative Performance Scale (PPS) Other data related to CP8 application (total rounds, time between applications, patch repetition, reasons for repeating patch application or not).
Applying the capsaicin 8% patch
CP8 is applied in accordance with an institutional protocol. 31 Anaesthesiologists from our Pain Unit who are also experts in neuropathic pain (they are members of the Spanish Pain Society or Asociación Española del Dolor) helped facilitate implementation of the protocol in said unit.
Before patch application, patients are informed verbally and in writing about the technique, necessary precautions and expected side effects. Patients’ questions are addressed and they sign the informed consent document.
CP8 is applied on an outpatient basis by an experienced nurse. The treatment room should be spacious and well-ventilated and have running water available. Patients are advised to wear comfortable clothing to the appointment. The patch protocol is as follows:
The procedure begins by cleaning the treatment area. Skin should be unbroken, dry and irritation-free skin. Hair may be trimmed to improve patch adherence but shaving is to be avoided. The area is treated with a lidocaine/prilocaine 25 mg/g anaesthetic cream for 60 min which is then removed before patch application. The treatment area is defined and the patch trimmed, if necessary. The patch is placed so as to completely seal over the painful cutaneous area affected by dynamic or static allodynia. Patch adherence can be helped by applying pressure or with tape, gauze or bandages. The patch remains on the skin for the indicated time (30 min on the feet (i.e. peripheral neuropathy) or 60 min in other locations (i.e. postherpetic neuralgia)). The patch is removed by rolling it in on itself and is disposed of in a medical waste bag. A cleansing gel is applied for at least 1 min, followed by gentle cleaning with ample water and soap. Pain is assessed during both patch application and removal. If needed, patients are provided with supportive treatment (cold compresses or oral analgesics as per their regular regimen). Before discharge, patients and their families are given verbal and written recommendations for post-application care and verbal health education:
Patients should avoid local heat application, hot showers or intense exercise and refrain from touching or scratching the treated area. Patients are informed that localised adverse effects are common and usually subside in a few days. Discomfort from localised adverse effects can be alleviated with quick-relief medication and non-frozen cold packs placed on the treated area, though direct contact with the skin should be avoided. Patients are advised on when to contact their doctor if symptoms persist. Patients are informed of the medication contained in the patch.
The NPRS is used to monitor pain during patch application and following removal and analgesics are administered if necessary. Patients are administered a rescue dose of their usual analgesia if their NPRS score is greater than 4–5/10 or if they complain of pain or a burning sensation.
Further applications of the patch are considered on a case by case basis. If after 3–4 months, the patient has a NPRS score greater than 4–5/10 and/or requires more than three rescue doses of their usual analgesia, and provided the outcome of the previous patch application was good, patch application is repeated.
Follow-up procedure
A follow-up call is made 7 days after patch application to monitor side effects and assess pain improvement. Patch application can be repeated every 4 months based on the patient's needs.
Results
Table 2 and supplementary Table 3 illustrate our key findings:
We observed an improvement in the intensity of pain caused by CINP, especially after the first CP8 application:
The NPRS score improved by 2.42 points (from an average of 6.42 (strong pain) to 4 points (moderate pain)) 7 days after application, the difference being statistically significant (p = 0.0422). Since the p-value is less than 0.05 and enables us to reject the null hypothesis, our findings would suggest that CP8 treatment was the determinant of pain reduction. Two patients (28.57%) had a decreased need for adjuvant treatment after CP8 application (not statistically significant). Only one patient (14.28%) required an extra dose of their usual analgesia during patch application. The need for extra doses of analgesia for neuropathic pain decreased from 0.57 on average to 0.43 (not statistically significant). Regarding patients’ functional status :
Four patients (57.14%) maintained the same PPS score pre- and post-patch application. Two patients improved their PPS score by 10 points. Another patient's score decreased 20 points owing to poor pain control due to disease progression and issues unrelated to CP8 treatment. (The results of the funcionality data analysis were not statistically significant.) Analysing the total daily oral morphine dose shows the following:
The mean dose remained the same pre- and post-application of CP8. One patient (14.28%) maintained the same dose, two patients (28.57%) decreased their dose and two patients (28.57%) increased their dose because of pain in other locations attributable to multiple myeloma (patient no. 3 experienced pain in the right rib cage / patient no. 4 experienced lumbar pain). The other two patients (28.57%) did not receive opioid treatment. The outcome of the analysis of the differences in the total daily oral morphine dose and extra doses needed pre- and post-application of CP8 was not statistically significant. When asked whether they would repeat CP8 treatment:
The majority of patients (n = 6, 85.71%) indicated they would repeat treatment with the patch. One patient (14.28%) would not repeat the patch citing ineffectiveness. One patient (14.28%) did not know.
Pre and post-CP8 application results.
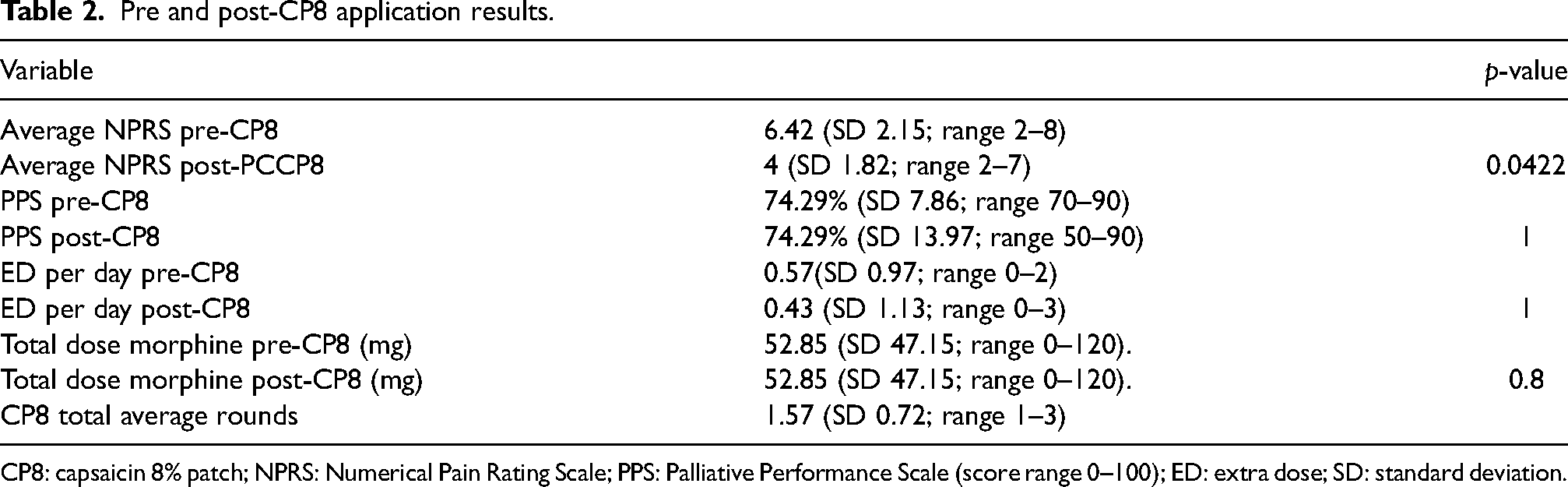
CP8: capsaicin 8% patch; NPRS: Numerical Pain Rating Scale; PPS: Palliative Performance Scale (score range 0–100); ED: extra dose; SD: standard deviation.
Patch application was repeated in three patients, resulting in a total of one application in four patients (57.14%), two applications in two patients (28.57%) and three applications in one patient (14.28%).
Discussion
Our case series reveals that CP8 application in multiple myeloma patients with CIPN induced by bortezomib or thalidomide can reduce pain perception where patients are already receiving adjuvant pain treatment, with almost no side effects.
Comparison with existing literature
Our observed improvement of CIPN pain following CP8 treatment aligns with the scant literature available to date and adds to the strength of the evidence.9,14,15,21,27–29
Most previous studies looked specifically at postherpetic neuralgia and diabetic neuropathy.10,18,20–25,32,33
In a recent study of CP8 and colon cancer patients, the authors conclude, in concurrence with Smith et al., that the patch is an effective treatment for pain associated with CIPN in patients treated with oxaliplatin. 20 Furthermore, patients with lower sensitivity to neurotoxic agents have a better response to treatment and pain reduction. 15
One recent study looked at intraepidermal and subepidermal nerve fibres, quantified by image analysis, in skin biopsies before and after CP8 application. 29 It concluded that CP8 treatment can lead to regeneration and restoration of sensory nerve fibres. In addition, a recent review of CIPN pain treatment summarises that CP8 is one of the treatments of choice for localised neuropathic pain and concludes that it may have a disease-modifying effect because it can promote regeneration and restoration of nerve fibres in the skin. 28 Other studies concur that the patch may have disease-modifying effects, in addition to demonstrating CP8 effectiveness for CIPN control.28,29
Another recent review of combined treatments for any form of neuropathic pain – including cancer-related – recommends considering CP8 in addition to opioid treatment for localised pain. The evidence for topical combination therapy remains controversial, but the authors believe that current evidence supports systematic use of CP8 therapy in combination with conventional treatment. 34
Limitations
Our case series is not without certain limitations that affect the strength of the evidence. Firstly, the results are from a retrospective analysis in which the intervention cannot be controlled for. Secondly, we have not been able to study against any comparator, which would strengthen the evidence if the results were in favour of CP8 application. Lastly, the sample analysed is small in spite of the inclusion period. The impact of a small sample size on results cannot be calculated and may result in an overestimation of treatment effects (Moore, 2013). These limitations should be taken into account when interpreting the results and drawing conclusions about the strength of the evidence.
The low number of patients involved in the study and the fact that the disease is progressive – the appearance of new lesions leads to greater reliance on analgesia – are confounding factors that do not permit a stable comparison between subjects. Furthermore, in studies with small sample sizes, the probability of finding extreme results is greater. The fact that we found a statistically significant result should therefore be interpreted cautiously. Though we observed clinically significant differences pre- and post-patch application, the small sample size means that differences in the outcome would need to be much greater to achieve statistical significance.
Conclusions
Notwithstanding the limitations described above, we can conclude that our results may be indicative of the clinical benefit of CP8 treatment for CIPN. The published recommendations on CP8 application in patients with neuropathic pain are similar to those used by our group.27,28 Side effects are transient and limited to the time period around patch application. 28 Given the characteristics of local application and the clinical benefits for pain relief and possible disease-modifying effects, adding CP8 to conventional CIPN treatment may benefit the patient by decreasing their pain perception and reducing concomitant medication needs. However, this observation should be corroborated, at the very least with prospective studies involving a larger sample size. The best evidence would be achieved by conducting a controlled clinical trial against a comparator.
Application of CP8 appears to provide relief for multiple myeloma patients with CIPN, especially after the first application. There is a need for more comprehensive studies on a larger number of patients with different diagnoses – and treated with different chemotherapy drugs – to better establish CP8 effectiveness. Prospective studies would enable CP8 application to be observed over the long term against a control group and would also enable the number of effective doses to be established. All of this would inform the development of an evidence-based protocol for CP8 use. A prospective study with a larger, controlled sample would also limit possible confounders and mitigate the aforementioned limitations stemming from a small sample size.
Supplemental Material
sj-docx-1-opp-10.1177_10781552241230887 - Supplemental material for Adhesive capsaicin 8% patch for improved control of pain caused by chemotherapy-induced peripheral neuropathy in patients with multiple myeloma: A single-centre, seven-case series
Supplemental material, sj-docx-1-opp-10.1177_10781552241230887 for Adhesive capsaicin 8% patch for improved control of pain caused by chemotherapy-induced peripheral neuropathy in patients with multiple myeloma: A single-centre, seven-case series by Deborah Moreno-Alonso, Sílvia Llorens-Torromé, Blanca Corcoy de Febrer, María Amandi García, Gala Serrano-Bermúdez, Jordi Trelis-Navarro, Victor Mayoral-Rojals and Ancor Serrano-Afonso in Journal of Oncology Pharmacy Practice
Footnotes
Acknowledgements
The authors wish to thank the staff of the Palliative Care Service at the Catalan Institute of Oncology in L’Hospitalet. Likewise, the staff of the Pain Clinic in Hospital Universitario de Bellvitge. The authors are grateful to Kelsie Pettit DipTrans for English language and copy editing support following peer review feedback.
Author's contribution
DM-A, SL-T, BCF and MAG contributed to this paper in all the phases, from the design, data analysis, writing and reviewing. GS-B, JT-N, VM-R and AS-A contributed to the interpretation of the data and reviewing of this paper since the draft phase. All the authors approved the final version of the manuscript.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.