
Abstract
Introduction
The utilization of oral chemotherapy agents for cancer treatment has witnessed a steady rise in recent years. The pivotal determinant for the success of oral chemotherapy lies in the adherence of cancer patients to the prescribed treatment. This study aims to explore oral chemotherapy adherence and identify factors influencing medication adherence among cancer patients.
Methods
A total of 103 cancer patients participated in this descriptive study. Data were collected using the Oral Chemotherapy Adherence Scale, the Turkish Translation of the Beliefs about Medicines Questionnaire (BMQ-T) and The Functional Living Index-Cancer.
Results
Of the participants, 66% reported good adherence to oral chemotherapy. Key findings indicate that access to health services (β = −1.473, p = 0.009), cancer stage (β = −1.570, p = 0.015) and the BMQ-T subscale of General Overuse (β = .696, p = 0.041) were independent predictors of medication adherence.
Conclusion
The study observed medication non-adherence in one-third of patients undergoing oral chemotherapy. Primary contributors to non-adherence included difficulties in accessing health services, advanced cancer stage and the belief that drugs are over-recommended by doctors. These results underscore the need for a heightened focus on preventable factors, such as improving access to health services and addressing beliefs about drug overuse, to enhance medication adherence in patients receiving oral chemotherapy.
Implications for practice
Nurses hold a crucial role in ensuring patients adhere to their prescribed medications. Factors such as difficulty in accessing health services, advanced cancer stage and the belief in drug overuse recommendation by doctors are significant contributors to non-adherence. Attention should be directed towards preventable factors, including improving access to health services and addressing beliefs about drug overuse, to enhance medication adherence in patients undergoing oral chemotherapy.
Introduction
Cancer incidence and mortality are rapidly growing worldwide. According to Global Cancer Statistics, there were an estimated 19.3 million new cancer cases and nearly 10 million cancer deaths in 2020, compared with 18.1 and 9.6 million, respectively, in 2018.1,2 In Turkey, the rate of cancer incidence was 225.1 per 100.000 in 2018. 3 Cancer has been the second most common cause of death after circulatory system diseases across the country. 4
Although parenteral administration is an essential route in the medical treatment of cancer, more oral chemotherapeutic drugs are increasingly used in cancer treatment.5–7 These drugs can be categorized based on their classification and the stage of the cell cycle that they affect. 8 This new era of oral options began in 1998 with the approval of capecitabine, and over the course of the following ten years, additional targeted agents including imatinib, gefitinib, lapatinib and nilotinib were also approved. It is projected that 25% of the agents in the oncology pipeline will be available in an oral formulation in the future.9,10
Oral chemotherapy has many advantages in comparison to parenteral chemotherapy; it does not require vascular access, it can have easier administration than intravenous treatment, the frequency of hospitalization is lower, the time spent in the care for the person is less, it is associated with a better quality of life, it reduces the interference of the treatment in work and social activities, it creates a stronger sense of control and freedom over the patient's treatment and illness.11–13 Even though the patient's responsibility increases with oral chemotherapy, 14 most patients prefer it if they do not compromise the outcome of the treatment.15–17 Additionally, the total cost of oral therapy is generally lower than the cost of parenteral therapy.
Nonetheless, oral chemotherapy also has disadvantages including sub-optimal adherence, 9 side effects and misconceptions about convenience of this type of chemotherapy. 18 As the dosing regimens are frequently complicated, even the most medically advanced patient and family may find it difficult to manage symptoms, side effects and adverse events in addition to taking medications.9,19 Moreover, adherence to oral therapy may be negatively impacted by the fact that patients do not receive the same level of oversight and monitoring as those receiving intravenous treatment. 15 Therefore, when applying an oral treatment at home, attention should be paid to adherence. 20 Oral medication adherence is a multifactorial and complex issue that can significantly change the treatment outcome.6,16 Hence, to achieve desired outcomes, the patient's adherence with the treatment is just as important as for the diagnostic accuracy and disease treatment.16,21,22
In cancer patients, the factors especially associated with non-adherence are demographic factors such as age, gender, patients’ beliefs, complex treatment plans, inadequate communication with healthcare professionals, insufficient social support, quality of life, number of drugs taken, cancer stage, treatment timing due to food intake, duration of chemotherapy, medication-related burden and adverse effects have been identified.13,16,21,23 It has been assumed that cancer patients adhere to their medication particularly well because of the severity of disease. On the other hand, some studies from the literature have shown that this is not always true, and adherence rate for medicine vary between 16% and 100% depending on the medication and measurement method.5,24,25
Patients who are administered intravenous cancer treatment are monitored closely in infusion centres, whereas patients who are prescribed oral therapy receive their medications remotely. 6 Nurses play an essential role in ensuring that patients take their medications as prescribed. In order to support patients, nurses should first identify the influencing factors related to patients’ medications adherence. 21 Determining the adherence status of patients receiving oral chemotherapy treatment and the factors influencing adherence with treatment is a significant element in tailoring the individualized education and follow-up of the patients. 26 Therefore, the objective of this present study was to investigate the status of patients’ oral chemotherapy adherence to medications and the determinants of non-adherence to medication in cancer patients receiving oral chemotherapy.
Methods
Study design, sample and setting
The research is a descriptive study conducted in a single oncology centre. Data were collected between 15 May 2018 and 15 December 2019. Patients with any cancer who were taken regular follow-up visit at the university hospital's oncology outpatient clinic were invited to take part in this study. The criteria for inclusion: (a) age over 18 years; (b) had used at least one oral chemotherapy medication for at least one month; (c) was able to read and respond the questions; (d) voluntary participation to the study; and (e) signed an informed consent document. The criteria for exclusion: (a) cognitive impairment; (b) major psychiatric diseases; (c) a concurrent life-threatening disease or clinically unstable health status; and (d) not able to give informed consent. Eleven patients who had a current prescription for oral chemotherapy did not agree to take part in the study. Therefore, they were excluded. Eventually, 103 cancer patients were assessed.
Data collection procedure
This study was carried out in the oncology outpatient clinic. Participants comprised those who attended to the outpatient clinic for a routine clinic follow-up visit. Detailed clinical evaluations of the patients were carried out by clinicians in the field of oncology. Patients whose clinical evaluations were completed by the clinician were invited to take part in the study. Participants who voluntarily interested in participating in the study were interviewed in outpatient rooms, and signed an informed consent document was received. During this interview, participants were given information about research and research forms and asked to fill out the forms. Afterwards, the researcher looked for any missing answers and, if possible, patients were asked to respond to the missing items. This process took about 25–30 min. All forms were confidential. No payments were given to the patients for completing the forms.
Measures
The data were collected with the participant assessment form, Oral Chemotherapy Adherence Scale (OCAS), Beliefs about Medicines Questionnaire [BMQ-Turkish Translation (BMQ-T)] and The Functional Living Index-Cancer (FLIC) form.
The participant assessment form was designed to obtain data on socio-demographic (gender, age, education level, employment and marital status, access to health services and socio-economic status) and clinical (type and stage of cancer, duration of disease, presence or absence of distant metastases, the duration of receiving oral chemotherapy medications etc.) characteristics of the participants.
Oral Chemotherapy Adherence Scale was developed by Bagcivan and Akbayrak to evaluate patients’ adherence to oral agents in cancer treatment. 21 It is used for the patients who use oral agents for at least one month. The scale consists of 19 items in total. A five-point Likert-type is used in the scoring of the scale. The patients mark the most proper expression on a five-point Likert answer option from 5 = always to 1 = never. The highest score on the scale is 95, the lowest score is 19. The sum of each item’ scores on the scale constitutes the total score of the scale. A high score for the total scale shows that adherence with oral chemotherapy treatment is high/good. The total scores are used in the evaluation of the scores obtained from the scale; a score of 84 and higher is evaluated as ‘good adherence’ and a score of 83 and lower is evaluated as ‘low adherence’.
Beliefs About Medicines Questionnaire (BMQ) was used to assess the patients’ perceptions and expectations about medication. This scale was developed by Horne et al. 27 The validity and reliability of the Turkish version of the questionnaire [BMQ-Turkish Translation (BMQ-T)] was done by Cinar et al. 28 It includes 18 items in five-point Likert type, as in the original version, and consists of two sections: Specific and General. The Specific section consists of two sub-sections: Specific Necessity (High score indicates strong belief in the effectiveness and necessity of prescribed drugs – five items) and Specific Concerns (High score indicates high concern about the potential adverse effects of prescribed drugs – five items). The General section consists of two sub-sections, General Harm (High score shows strong beliefs that drugs are ‘harmful’, ‘addictive’, ‘poison’ – four items) and General Overuse (High score shows strong beliefs that drugs are overused by doctors – four items). The mean scale score is calculated by summing the scores of the items in each sub-section and dividing them by the number of items. The lowest score that can be obtained from each section is 1, the highest score is 5.
Functional Living Index-Cancer was developed and validated by Schipper et al., 29 and the validity and reliability of this scale was measured by Bektas and Akdemir in Turkish culture. 30 The aim of FLIC is to determine the impact of disease and treatment symptoms on all areas of an individual's life (functional abilities, psychological and physical capacity). The seven Likert-type scale comprises questions about the past two weeks, past month or today's situation. The scale consists of five sub-dimensions: ‘physical functioning’ (nine items), ‘psychological functioning’ (six items), ‘current well-being (cancer-related difficulties)’ (three items), ‘social functioning’ (two items) and ‘gastrointestinal symptoms (nausea)’ (two items) and consists of 22 questions in total. The lowest score on the scale is 22 and the highest score is 154. High score indicates a high level of functional status.
Data analysis
The SPSS (24.0) software program was used in the evaluation of the data. The suitability of the continuous data with a normal distribution was measured using the Kolmogorov–Smirnov test. Descriptive statistics were presented as the median values with interquartile range (IQR) (25th and 75th percentiles) and frequency (percentage). As variables were not normally distributed, Mann–Whitney U test was performed for analysis. Chi-square and Fisher's exact test were used for the comparisons of categorical variables.
Binary logistic regression analysis was performed using variables that showed significance in univariate analysis. Status of adherence as defined by the OCAS was used as dependent variables. Each independent variable was last included in the regression model, and then all the factors were combined in the ‘Enter’ method. When the compatibility of the model was tested using the Hosmer–Lemeshow test, it was found to be an adequate model (χ2 = 5088, df = 8, p = 0.748). A p-value of <0.05 was accepted as statistically significant.
Ethical considerations
The approval of the University of Health Sciences ethics committee was obtained for the study (Session No: 2018/3). The study was carried out in accordance with the Helsinki Declaration, and written informed consent to participate was given by the respondents. The study's purpose, confidentiality and privacy were all explained in depth to all participants. No ethical issues arose during the present study.
Results
General characteristics of the participants
The median age of patients was 63.0 years (IQR, 58.0–69.0), 57.3% were female, the median duration of disease was 26.37 months (IQR, 16.23–46.70), the most prevalent form of cancer was colorectal cancer (52.4%) and OCAS median score of participants was 87.0 (IQR, 82.0–90.0). Further details about the participants’ characteristics are given in Table 1. A total of 56.3% of the patients said they had drug-related side effects. When these side effects are examined; 42.7% of patients reported dyspepsia/appetite loss, 33% reported fatigue and 31.1% reported nausea and vomiting (n folds because a patient gave more than one answer) (not shown).
Socio-demographic and clinical characteristics of the patients (N = 103).
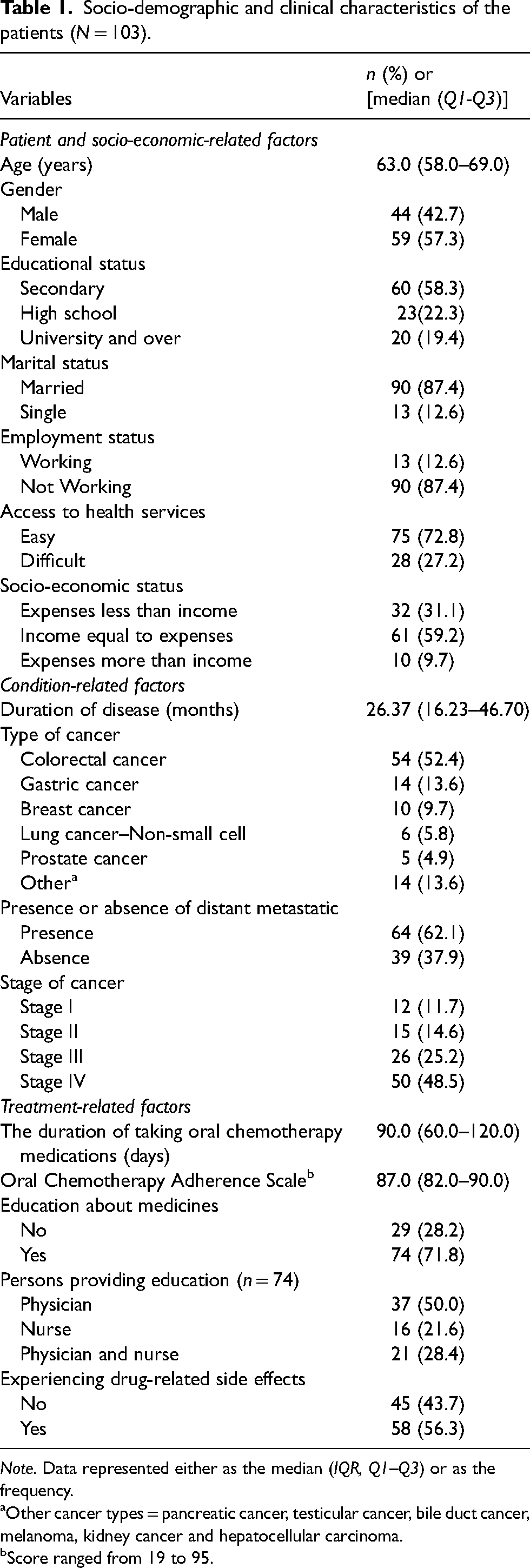
Note. Data represented either as the median (IQR, Q1–Q3) or as the frequency.
Other cancer types = pancreatic cancer, testicular cancer, bile duct cancer, melanoma, kidney cancer and hepatocellular carcinoma.
Score ranged from 19 to 95.
Clinical and demographic factor relation with adherence to oral chemotherapy
The participants’ characteristics and their comparison with their medication adherence status are given in Table 1. Overall, 66.0% of the patients were considered to have a good medication adherence. Patients who have easier access to healthcare services have higher medication adherence scores than those with difficult access (p = 0.010). The group that did not adhere to oral chemotherapy had significantly higher stage 4 cancer patients (p = 0.011). None of the other variables had an effect on medication adherence (p > 0.05) (Table 2).
Comparison of the socio-demographic and clinical characteristics of the patients with the medication adherence status (N = 103).
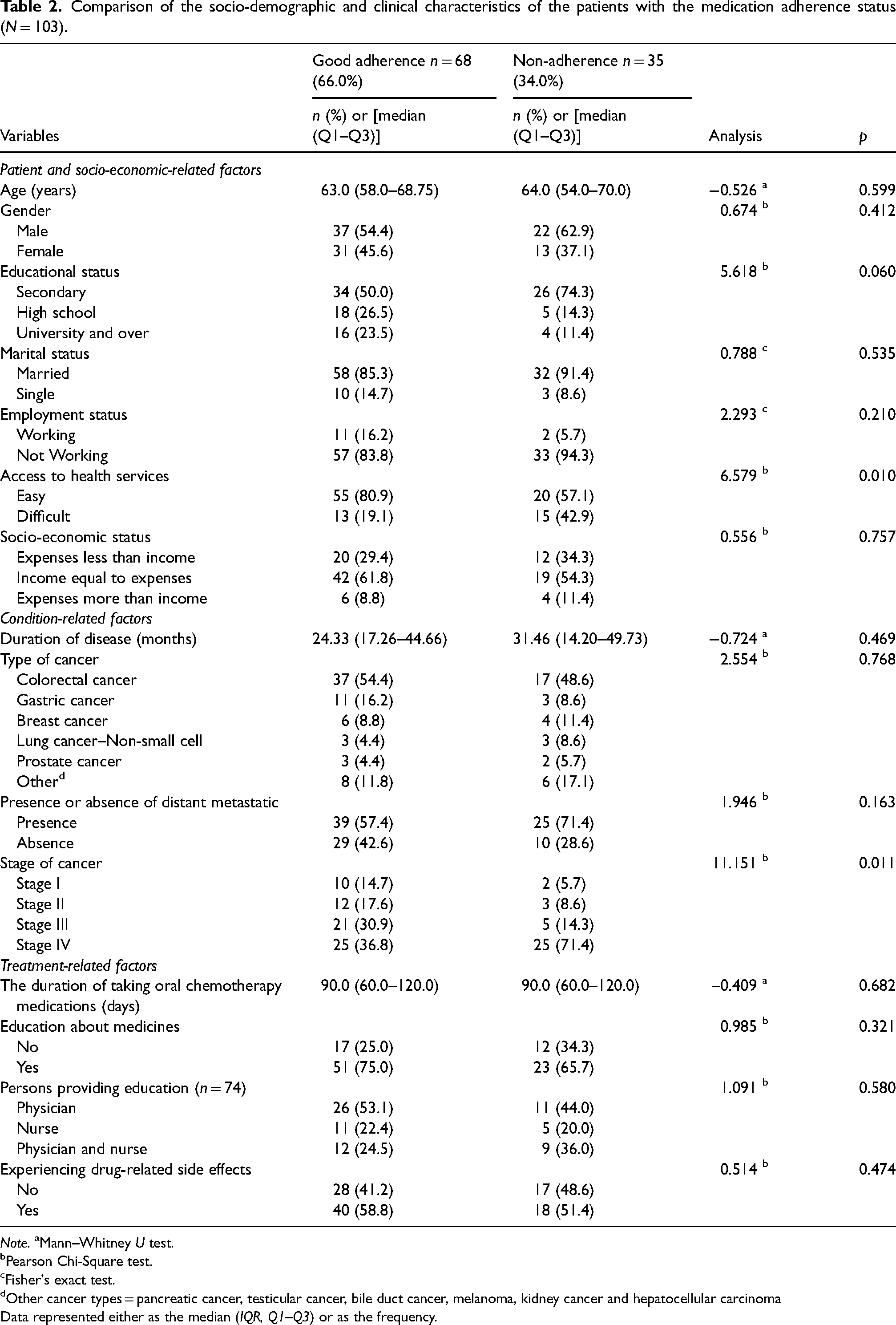
Note. aMann–Whitney U test.
Pearson Chi-Square test.
Fisher's exact test.
Other cancer types = pancreatic cancer, testicular cancer, bile duct cancer, melanoma, kidney cancer and hepatocellular carcinoma
Data represented either as the median (IQR, Q1–Q3) or as the frequency.
Table 3 shows BMQ-T scores and FLIC scores according to the medication adherence. The BMQ-T-General Overuse median score was found statistically significantly higher in the non-adherent group (p = 0.001). The total FLIC and gastrointestinal system (GIS) symptoms median scores of the patients in the adherent group were statistically significantly higher (respectively, p = 0.049; 0.041).
BMQ-T and FLIC scale scores relation with adherence to oral chemotherapy.
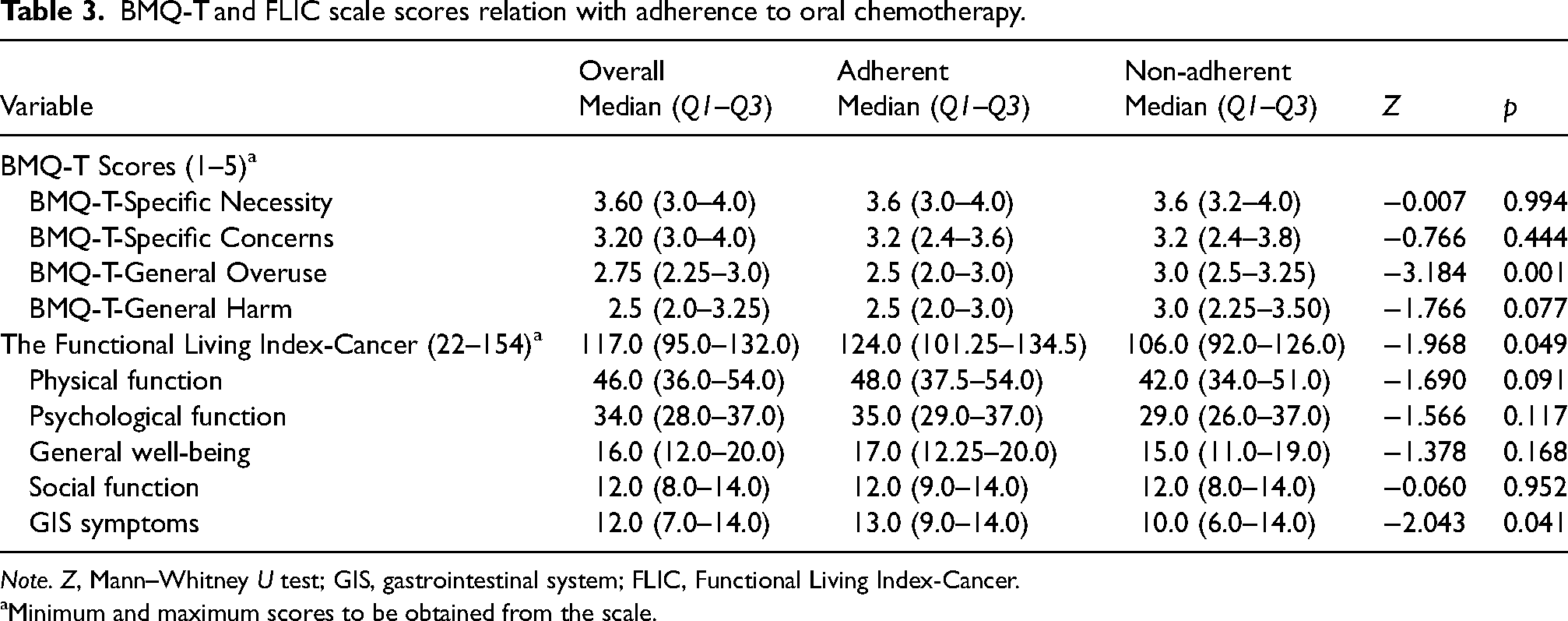
Note. Z, Mann–Whitney U test; GIS, gastrointestinal system; FLIC, Functional Living Index-Cancer.
Minimum and maximum scores to be obtained from the scale.
Factors affecting non-adherence
The results of the Binary Logistic Regression analysis that were significantly related to patients’ adherence to oral chemotherapy are shown in Table 4; 29% of the total data of access to health services, cancer stage, general overuse, GIS symptoms and functional life could predict the adherence to medication (Nagelkerke R Square: 0.295). Patients who have a high belief that drugs are overused (BMQ-T-General Overuse) (95% CI [1.027–3.919], p = 0.041), patients with difficult access to healthcare services (95% CI [0.076–0.693], p = 0.009) and advanced cancer stage (95% CI [0.059–0.739], p = 0.015) were more likely to be non-adherent.
Binary logistic regression analysis of risk factors associated with medication non-adherence.
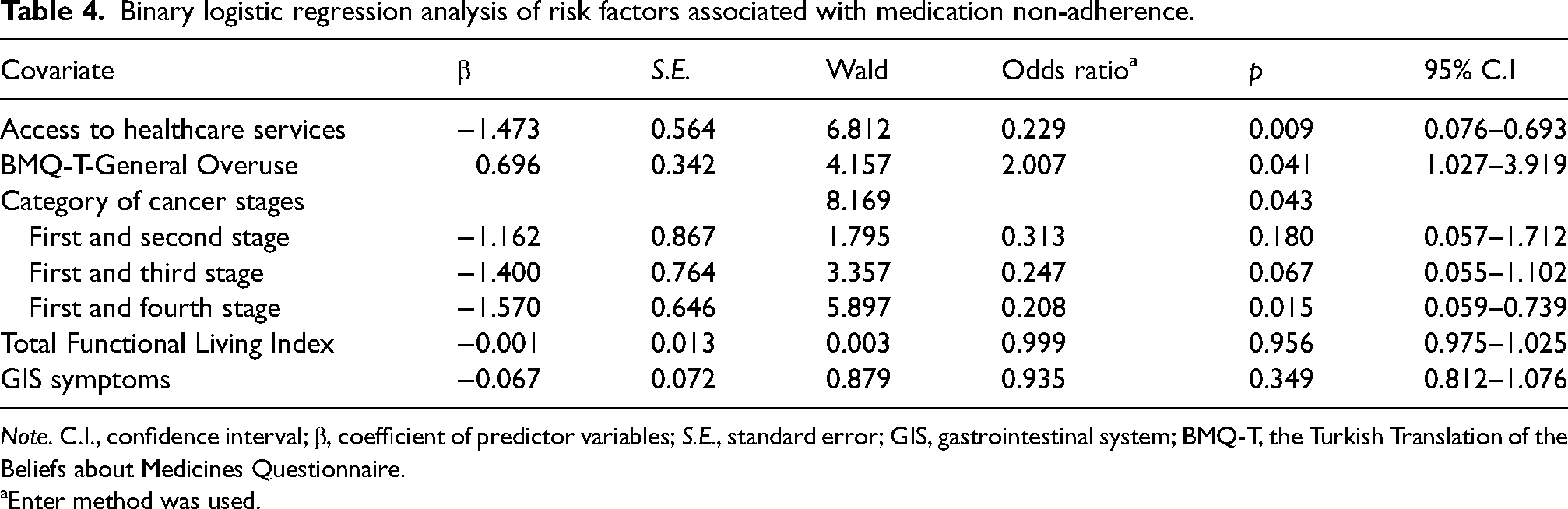
Note. C.I., confidence interval; β, coefficient of predictor variables; S.E., standard error; GIS, gastrointestinal system; BMQ-T, the Turkish Translation of the Beliefs about Medicines Questionnaire.
Enter method was used.
Discussion
In this study, the state of adherence to oral chemotherapy and the factors that related to it were examined. The proportion of patients who adhered to their medications well was 66.0%. Non-adherence was more common in cancer patients who had difficulty in accessing health services, had advanced cancer stage and had a high negative view about the way in which medicines are prescribed and beliefs that they are overused by physicians (BMQ-T-General Overuse score). On the contrary, it was found that patients with high total functional life scores and good GIS symptoms generally had higher levels of medication adherence. It was determined that the most significant factors related to non-adherence were the difficulty of accessing health services, advanced cancer stage and the belief that medications are overused in general. In the small study conducted by Bhattacharya et al., only 23.3% of 43 participants were found to be non-adherent to oral chemotherapy. 31 In this study, the most important reason for non-adherence reported by the participants was ‘forgetting’. 31 In another study conducted by Jacobs et al. found that patients’ adherence with prescribed oral chemotherapy medications was 89.3% for 12 weeks. 32 Similarly, a study of adherence to oral chemotherapy by Krikorian et al. found that most patients (90–100%) were adherent to oral chemotherapy. 10 However, Hirao et al. found that the proportion of patients showing good medication adherence was 56.4%. 13
In the treatment that requires taking individual responsibility, ease of access to health services is important in terms of the continuity of treatment and management of emerging symptoms. 23 It was found in this study that patients with easy access to health services were more adherent. Patients receiving oral chemotherapy mostly apply their treatments at home. It is significant that patients have easy access to health care and home care services in oral chemotherapy treatment. Problems with access to these services lead to undesired situations such as inadequate follow-up, lack of communication between healthcare personnel and the patient, having problems with prescriptions, side effects, ineffective management of side effects and having problems with the evaluation of beliefs and attitudes related to treatment. Studies show that many socio-demographic factors, including education level, race and socio-economic status, do not have a consistent effect on medication adherence. 33 Although there is no effect between these demographic data and adherence in this study, it should not be ignored that these factors can indirectly affect access to health services. A study that examined patient preferences regarding different treatment methods in breast cancer patients found that the majority of patients preferred to take daily tablets (63%) rather than monthly injections. Analysis of reasons for choice revealed that convenience is an essential issue regardless of patients’ preferences. 34
In this study, advanced cancer stage was found to be an effective factor on non-adherence. When the current literature is reviewed, there was no study examining the relationship between cancer stage and oral chemotherapy adherence. Xu et al. found that while the adherence rate was 86.2% in the first place, this rate decreased to 28.7% in the third year and to 17.7% in the fifth year. 35 Although the cancer stages were not examined in Xu et al.'s study, it is seen that there was a significant decrease in medication adherence within five years. 35 Indirectly, it can be assumed that the state of cancer has also advanced during this period. Advanced cancer patients may feel that oral chemotherapy is less effective because of the medication form. It should also be noted that cancer patients receiving oral chemotherapy typically do not receive the same amount of instruction, training and follow-up as patients receiving intravenous chemotherapy. The state of disharmony increasing as the stage progresses situation may be associated with the fact that stage 4 cancer patients have to interrupt their treatment due to the side effects (pain, nausea-vomiting, fatigue, imbalance in blood parameters and general condition disorder) they experience because of the disease and treatment. In order to understand the reasons of this situation, more in-depth research is needed.
Most studies on medication adherence have concluded that negative beliefs on medications are a significant obstacle to good adherence.36–38 In this study, it was found that patients with strong beliefs that oral chemotherapeutic medications were overused by physicians in general were in the non-adherence group. Higher scores on the General Overuse reflect a negative attitude about the way in which drugs are prescribed and beliefs that doctors overused them. 39 This may be due to the patients’ perception that the drugs are toxic and overused. In a study of 258 women with breast cancer, a state of knowledge, belief and distrust about the patient's treatment resulted in less use of effective adjuvant therapies. The authors emphasized the need to clearly present not only the risks but also the benefits associated with the drugs, taking into account the patient's trust and concerns in the medical system. 40 The majority of patients prefer oral therapy over intravenous therapy, mainly owing to the ease of receiving care at home.6,17 However, oral therapy would be preferred by nearly two-thirds of the patients over intravenous therapy if the effectiveness of oral therapy is equivalent to intravenous therapy and the toxicity is not more. Therefore, patients need full details on the effectiveness and toxicity of the oral option to intravenous treatment to prefer oral chemotherapy. 23 Saratsiotou et al. found that the most significant factor associated with undesirable adherence to treatment was the patient's belief in the effectiveness of the treatment. 41 In this study, 16.7% of the patients who believed that their treatments were effective and 62.5% of those who did not believe reported non-adherence. At the same time, patients’ attitudes towards medication adherence are also related to their understanding of the disease and treatment. 32 Therefore, healthcare providers, and particularly nurses, should also address patients’ beliefs, knowledge and attitudes about medications to improve their adherence to medication.
In addition to the management of symptoms, adherence with oral chemotherapy is necessary to achieve the desired clinical response. Patients who experience side effects are more likely to not adhere with cancer treatments. 42 It is seen from the result of our study that the functional status and QoL of patients who are adherent to medication are better. Similarly, some studies have found a negative correlation between poor quality of life and medication adherence.43,44 Based on our results, patients with high quality of life are more adherent to oral chemotherapy medication may be due to the advantages such as ease of administration of the medication, less need for hospitalization, makes their lives easier and provides a valuable option for the treatment of cancer patients. Patients taking oral chemotherapy experience adverse effects such as diarrhoea, fatigue, nausea and vomiting which can have a considerable negative impact on their QoL, especially when combined with symptoms of cancer. Side effects of oral chemotherapy medications can influence medication non-adherence. Therefore, oral chemotherapy can be a difficult for these patients to tolerate, making medication non-adherence a problem to consider.6,7,13 In the study, Hirao et al. found that having diarrhoea was related to medication non-adherence. 13 In this study, adherence to medication was found to be greater in patients with good GIS symptoms, and this issue is a condition that should not be ignored.
Limitations
There are some limitations in our study. The first limitation of this study is related to the generalizability of the results. Although this study made a valuable contribution in understanding the factors influencing adherence to oral chemotherapy medications, it was conducted only in a training and research hospital and has a modest sample size. The second limitation was the use of self-reporting method in measuring medication adherence, as it is considered the simplest and cheapest method to be easily applied in clinical setting. Therefore, the study's findings may have been affected by misunderstanding, misremembering or misinterpreting the questions. However, the evaluation of medication adherence with a scale that was developed for patients using only oral chemotherapy and whose validity and reliability has been made improve the quality of the study. Therefore, the tools used in this study can be considered suitable for achieving the specified aim.
Conclusions
In this study, it was shown that about one-third of the patients were non-adherent to oral chemotherapy medications. This study also showed that when the cancer stage increased and beliefs that about medications have been overused by doctors could negatively influence patients’ medication adherence. It was also found that patients who had easier access to health services had higher medication adherence. In addition, patients with better functional status and QoL and patients with fewer GIS symptoms were found to have higher medication adherence.
According to the results of this study, as nurses, it is one of the important issues to evaluate the access status of patients to health services and to contact those who cannot access and do not come for regular follow-up. In addition, adequate training on the necessity of medications and why they are used, evaluating patients’ beliefs about medications is also an important issue. It is especially significant to evaluate the medication adherence of advanced cancer patients. Therefore, healthcare providers, especially nurses, should try to understand the characteristics and lifestyles of patients, develop plans to include drug-taking behaviour in everyday practice, play an important role in the education and support of patients, and support their education in this direction.
Footnotes
Author contributions
FIC, EU and CP designed the study; CP, collected the data; FIC performed the analysis; FIC and EU interpreted results; FIC and EU drafted the manuscript. All authors reviewed and approved the final version of the manuscript.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.