
Abstract
Introduction
Due to the high toxicity of antineoplastic drugs, handling their packaging could lead to the chemical contamination of hospital environments and exposure risks to healthcare professionals and patients. This study aimed to assess the contamination of two main surfaces: the outer primary packaging of oral antineoplastic drug formulations (n = 36) available on the Swiss market and the surface of secondary packaging of injectable antineoplastic drug preparations (n = 60) produced by the pharmacy of a Swiss hospital and carriers used for transport (n = 5).
Methods
Samples were collected using a validated wipe sampling method. The simultaneous analysis of 24 antineoplastic drugs: 5-fluorouracil, busulfan, carboplatin, cyclophosphamide, cytarabine, dacarbazine, daunorubicin, docetaxel, doxorubicin, epirubicin, etoposide, gemcitabine, idarubicin, ifosfamide, irinotecan, methotrexate, oxaliplatin, paclitaxel, pemetrexed, raltitrexed, topotecan, treosulfan, vinblastine, vincristine) and 1 antiviral compound (ganciclovir) was performed by UHPLC–MS/MS.
Results
A total of 58% and 90% positive results were obtained for the primary packaging of oral chemotherapies and for the secondary packaging of injectable preparations, respectively. The highest quantities found on the primary packaging for oral chemotherapies and on the surface of closed leak-proof bags were 111 ng of methotrexate and 19 ng of gemcitabine, respectively. Gemcitabine (69%) and cyclophosphamide (38%) were the two most common contaminants found on the packaging of injectable preparations and carriers, regardless of the chemotherapy preparations.
Conclusion
Trace levels (ng) of antineoplastic drugs can be found on most surfaces of all evaluated pharmaceutical products. Thus, suitable personal protective equipment is mandatory for healthcare professional handling antineoplastic drugs.
Keywords
Introduction
Chemotherapy is one of the main approaches for cancer treatment; drugs can be used to kill tumor cells or prevent them from dividing. Conventional antineoplastic drugs are known for their high toxicity and reactivity. Despite their action on cancer cells, they are well known for their inability to differentiate from normal cells, leading to the targeting of healthy cells as well and causing serious adverse effects, such as gastrointestinal toxicity and bone marrow suppression. The three main families of antineoplastic drugs can be classified according to their action on DNA: antimetabolites that act on DNA replication; compounds that alter the replication and transcription of DNA by adding alkyl groups to DNA (e.g. nitrogen mustards), by generating covalent DNA adducts (e.g. platinum derivatives), by breaking the DNA structure (e.g. anthracyclines) or by inhibiting topoisomerase (e.g. campthothecin derivatives); and antineoplastic drugs that can affect mitosis (e.g. vinca and taxus alkaloids).
Based on the type of cancer and its stage, chemotherapy can be administered orally or by injection. This treatment can be administered alone or in combination with other therapeutic approaches, such as surgery, radiotherapy, or biologic therapy (immunotherapy and some targeted therapies).
In a hospital setting, the preparation and administration of these drugs are the responsibility of healthcare professionals. Due to their hazardous nature, antineoplastic drugs should be handled with care and under strict measures to protect operators and the environment from exposure to these highly toxic drugs. The two most widely used guidelines worldwide are from the International Society of Oncology Pharmacy Practice (ISOPP) and the National Institute for Occupational Safety and Health (NIOSH). 1 One of the main reference guidelines in Europe is from the European Policy Recommendations—Preventing occupational exposure to cytotoxic and other hazardous drugs. 2 Guidelines and regulations are needed to ensure the safety of workers at risk of exposure to these highly toxic compounds, whose main routes are dermal absorption, inhalation of aerosols or ingestion. 3
Although guidelines and safe handling practices have been implemented in many countries to improve the safety of healthcare professionals and their environment, concerns about occupational exposure to antineoplastic agents persist: residual traces of antineoplastic drugs are still found on various work surfaces after completion of cleaning procedures,4–8 as well as in biological samples (such as blood or urine) of health staff handling these products.9–11 Recent studies have also demonstrated the presence of antineoplastic drugs on primary packaging4,12–15 or on the outside of injection vials.4–6,12,15–23 These trace residuals on the outer surfaces of product containers, as well as contamination on all surfaces where the packages are stored, represent a potential occupational exposure risk to the health professionals who handle these drugs.
Therefore, the purpose of this study was to evaluate the potential contamination of packaging containing chemotherapy preparations handled by healthcare professionals in the oncology and hematology care units of a Swiss hospital. Two kinds of packagings were evaluated. First, we analyzed the primary packaging of oral formulations (blisters, plastic, and glass vials) containing various antineoplastic drugs (methotrexate, idarubicin, cyclophosphamide, and etoposide) available on the Swiss market. The second type was the surface of closed plastic leak-proof bags containing an injectable chemotherapy preparation produced by the hospital pharmacy, as well as the carriers used to circulate them in the chemotherapy preparation unit (i.e. between the logistic room and cleanroom). For this purpose, wipe samples were analyzed by an ultra-high performance liquid chromatography coupled with tandem mass spectrometry (UHPLC–MS/MS), which allows for the identification and quantification of 24 antineoplastic drugs (5-fluorouracil, busulfan, carboplatin, cyclophosphamide, cytarabine, dacarbazine, daunorubicin, docetaxel, doxorubicin, epirubicin, etoposide, gemcitabine, idarubicin, ifosfamide, irinotecan, methotrexate, oxaliplatin, paclitaxel, pemetrexed, raltitrexed, topotecan, treosulfan, vinblastine, vincristine) and 1 antiviral preparation (ganciclovir).7,24
Materials and methods
Chemicals and reagents
All solvents were of MS grade (except dimethyl sulfoxide), and all chemicals were obtained at the highest analytical quality available. Formic acid and ammonium hydroxide were purchased from Merck (Darmstadt, Germany). Methanol (MeOH) and dimethyl sulfoxide (DMSO) were purchased from Sigma-Aldrich (Buchs, Switzerland). Ultrapure Type 1 water was obtained from a Milli-Q purification system from Millipore (Bedford, MA, USA).
Dacarbazine (DAC) was obtained from Tokyo Chemical Industry (Zwijndrecht, Belgium). Etoposide (ETO), oxaliplatin (OXA), and topotecan hydrochloride (TPT) were purchased from Toronto Research Chemicals (North York, ON, Canada). Busulfan (BU), cytarabine (CYT), daunorubicin hydrochloride (DAU), doxorubicin hydrochloride (DOX), epirubicin hydrochloride (EPI), ganciclovir (GANC), gemcitabine hydrochloride (GEM), methotrexate (MTX), paclitaxel (PTX), vinblastine sulfate (VBL), and vincristine sulfate (VCR) were obtained from the European Pharmacopoeia (Strasbourg, France). Raltitrexed (RTX) and treosulfan (TREO) were obtained from Sigma-Aldrich (Buchs, Switzerland). Irinotecan hydrochloride (IRI), docetaxel trihydrate (DOC), 5-fluorouracil (5-FU), cyclophosphamide monohydrate (CYC), idarubicin hydrochloride (IDA), carboplatin (CARB), ifosfamide (IFO), and pemetrexed (PEM) were purchased from Merck (Darmstadt, Germany).
[2H8]-Cyclophosphamide monohydrate, [13C,2H3]-methotrexate, [2H5]-paclitaxel, [13C,15N2]-5-fluorouracil and [13C6]-irinotecan were purchased from Alsachim (Strasbourg, France).
Stock solutions of standards and internal standards were prepared by dissolving standard compounds in DMSO at 1 mg mL−1 and 0.2 mg mL−1, respectively, and were kept at −80 °C until use.
Safety considerations for the handling of antineoplastic drugs
Due to the high toxicity of antineoplastic drugs, their manipulation requires strict safety precautions to limit exposure to analysts and their environment. Thus, all the experiments involving the handling of toxic compounds were performed in a specialized laboratory called Cytoxlab. 25 The negative pressure used in this room allowed us to contain any potential contamination. All powders were weighed and solubilized under a safety weighing enclosure with an incoming horizontal airflow equipped with HEPA H14 filters (ST1 Safety weighing Enclosure 1200, a1-envirosciences GmbH, Düssekdorf, Germany). Most dilutions were performed using an automated liquid handling workstation (Tecan Freedom EVO®, Männedorf, Switzerland). All instruments and materials in contact with toxic compounds were treated as hazardous waste. Personal protective equipment (gloves, gowns, masks, etc.) was chosen based on recommendations in the literature.1,2,26–29
UHPLC–MS/MS instrumentation
The UHPLC system was composed of an Agilent 1290 binary pump and an autosampler with a thermostat and column oven (Agilent, Waldbronn, Germany). Separation was carried out with an Acquity Premier CSH Phenyl-Hexyl column (1.7 μm, 2.1 × 100 mm) from Waters (Milford, MA, USA). The mobile phase consisted of two phases: mobile phase A consisted of 10 mM aqueous formic acid (pH 4.9) adjusted with ammonia, and mobile phase B consisted of pure methanol (MeOH). The flow rate was fixed at 0.34 mL.min−1, and the following gradient elution program was used: 0–0.5 min, 2% MeOH; 0.51–2 min, 2–50% MeOH; 2.01–7 min, 50–95% MeOH; 7.01–8 min, 95% MeOH; 8.01–10 min, 95–2% MeOH; and 10.01–13 min, 2% MeOH. The autosampler and column temperatures were maintained at 8 °C and 25 °C, respectively. The injection volume was 2 μL.
A coupled triple quadrupole mass spectrometer (MS/MS) 6500+ (AB Sciex, CA, USA) was used in MRM mode with an electrospray ionization interface (ESI). MS was used in negative mode (ESI-) for the detection of 5-fluorouracil and in positive mode (ESI+) for the other analytes. The other MS optimized parameters used in this study were based on a previously published validation method. 7
Analyzed compounds and UHPLC–MS/MS sensitivity
The selection of the 24 targeted antineoplastic drugs was based on their use in a hospital pharmacy and analytical considerations. Ganciclovir, an antiviral compound, was added to the list of targeted compounds because it was also prepared by the hospital pharmacy via the same procedure and environment as conventional chemotherapy preparations. This substance is considered mutagenic according to the European Chemicals Agency. 30
The limits of detection (LODs) and limits of quantification (LOQs) for the 25 targeted compounds analyzed by the UHPLC–MS/MS method are reported in Table 1.
Limit of detection (LOD) and limit of quantification (LOQ) of 24 antineoplastic drugs and 1 antiviral drug (ganciclovir) analyzed.
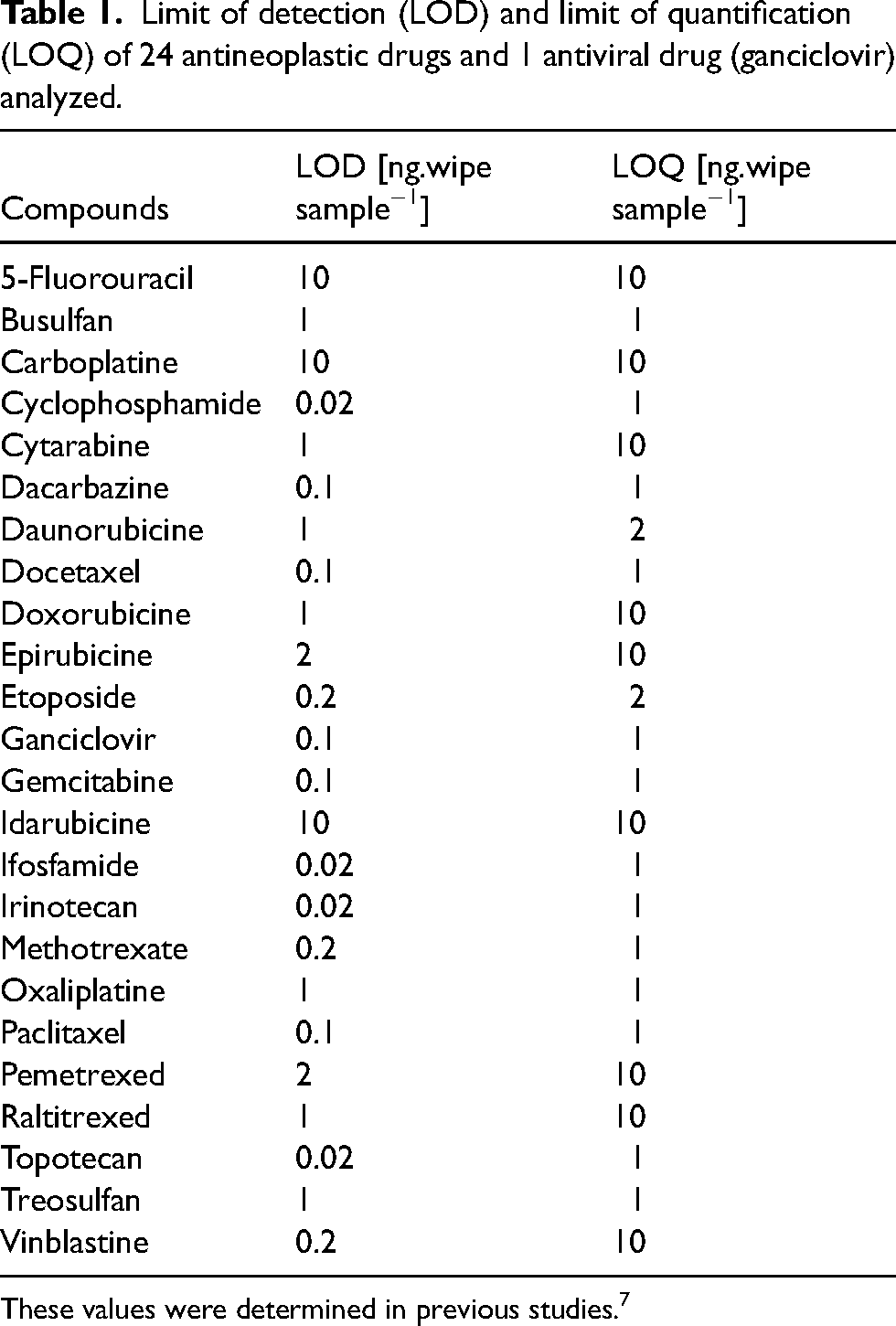
These values were determined in previous studies. 7
Sample preparation
Stock solutions of standards were prepared by dissolving standard compounds in DMSO at 1 mg.mL−1 and were kept at −80 °C until use. Stock solutions were thawed at room temperature for 30 min and vortexed a few seconds before use.
Calibration and quantification samples were obtained by pooling and diluting 25 standard stock solutions and 5 internal standard stock solutions. For each antineoplastic drug, the linear range was constructed with 8 calibration samples containing a concentration of target molecules from 0.5 to 400 ng.mL−1. The final concentration of the internal standards was 5 ng.mL−1 each.
Tested pharmaceutical formulations
Primary packaging of oral chemotherapy formulations
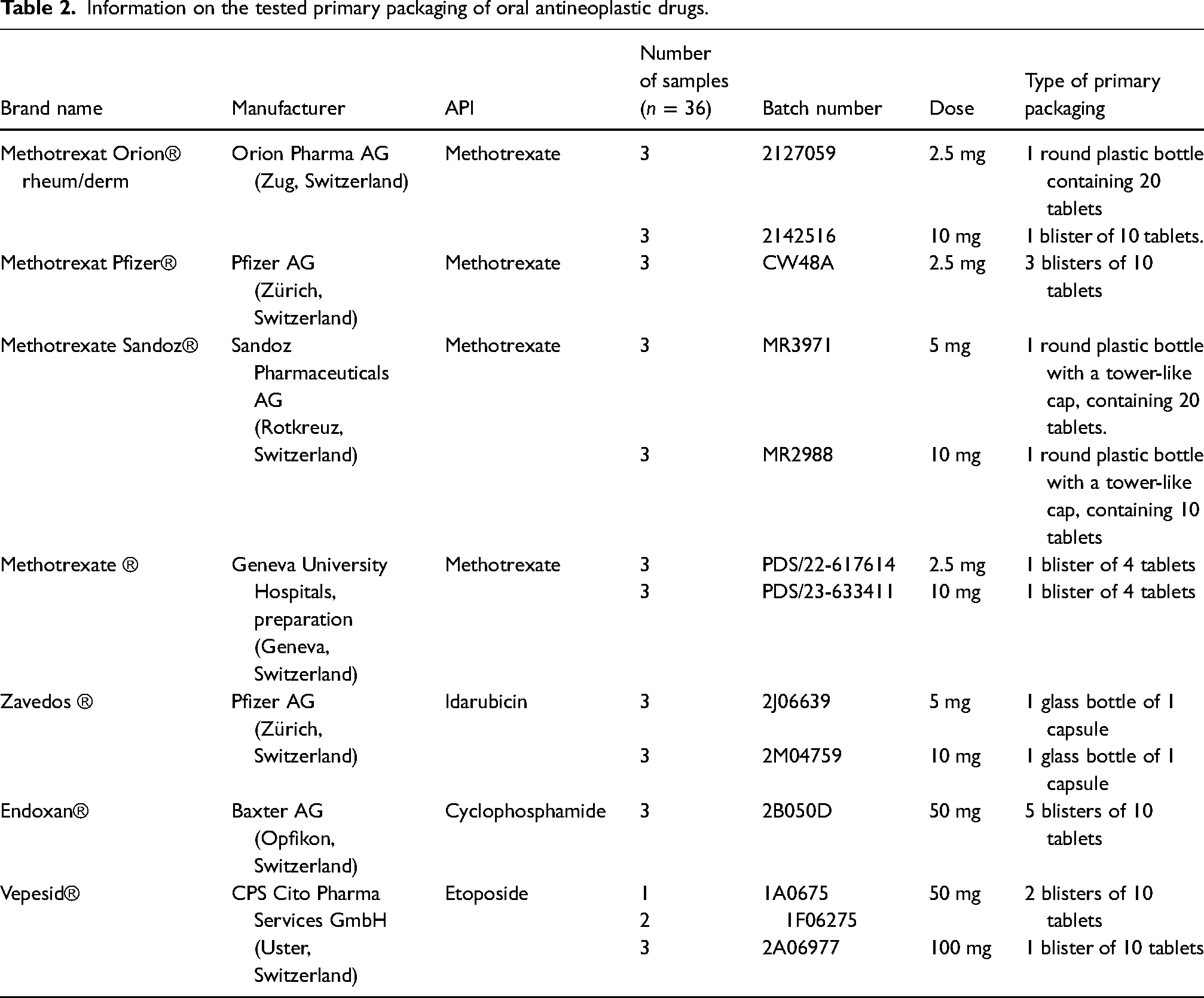
To monitor occupational exposure and quantify trace contamination of the drugs on the primary packaging, 36 blisters or bottles were analyzed with a validated wiping method.7,24 The selection of medications depended on the availability of the drug in solid form on the Swiss market and on the possibility of determining the active pharmaceutical ingredient (API) with the analytical method used. Medications were either borrowed from the hospital's logistic unit, ordered or provided by suppliers when possible. For each pharmaceutical formulation, three distinct secondary packagings were purchased, from which one primary packaging (one blister, one plastic bottle or one glass bottle) was sampled for analysis. Details of the analyzed products are shown in Table 2.
Information on the tested primary packaging of oral antineoplastic drugs.
Two operators performed the sampling at the same time to minimize the spread of contamination: the first operator opened the secondary packaging and organized the material without touching the primary packaging. Hence, no contamination could be present on their gloves. The second operator carried out the wiping procedure on the primary packaging. In this case, gloves were changed after each sampling. Depending on the type of packaging, the sampling was applied either to the outer walls and the vial cap for the bottles or to the surface of one blister containing the oral formulation. After each wipe, the primary packaging was dried with tissue and replaced in its original packaging. Samples were collected either directly in the care unit or in the dedicated laboratory, Cytoxlab, whenever possible.
Secondary packaging of injectable chemotherapy preparations
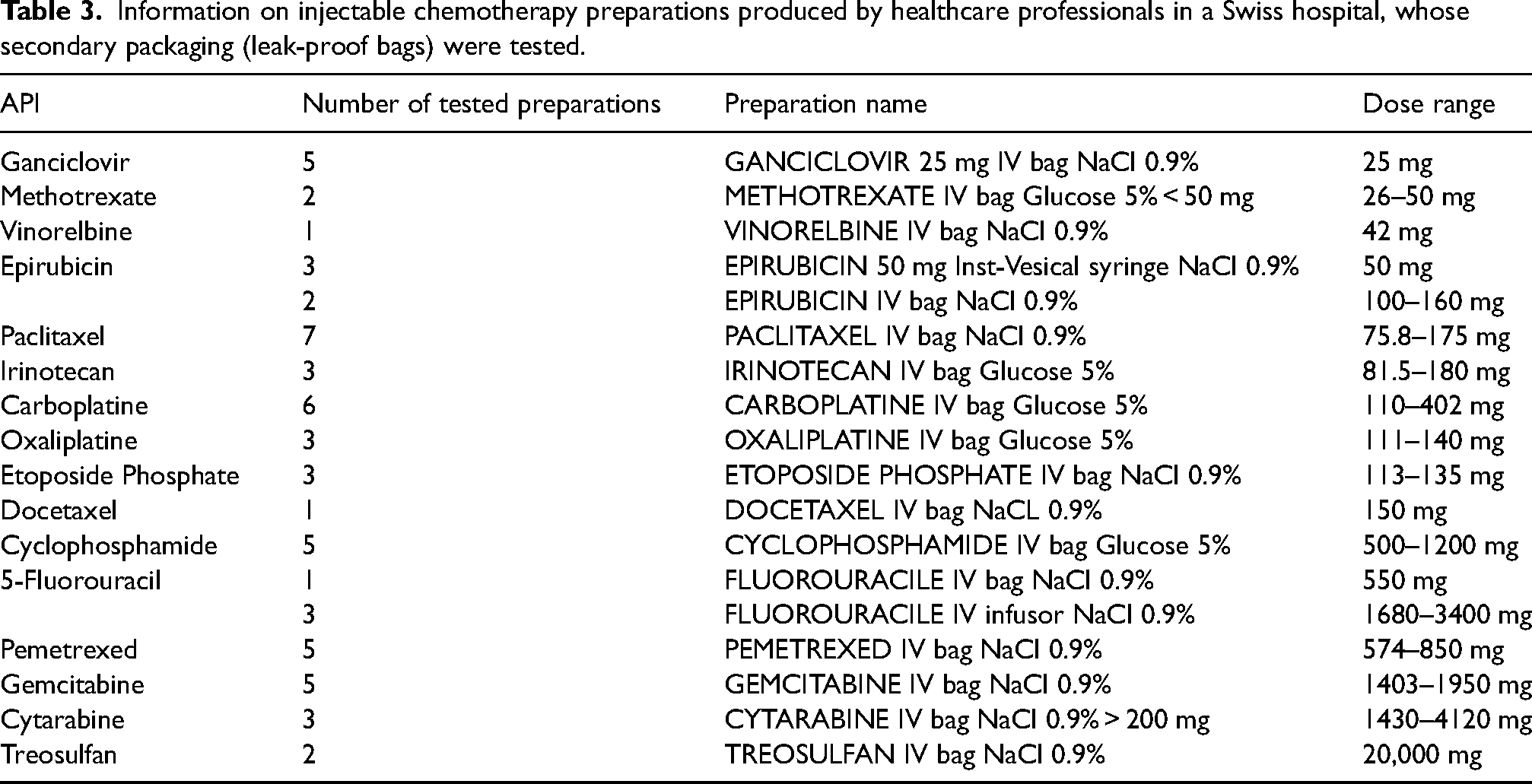
All the preparations of injectable formulations containing conventional antineoplastic drugs, are centralized at the pharmacy of the hospital. The final step of the production consists of placing the chemotherapy preparation in a leak-proof bag (Figure 1), which is sealed before transport. 26 Once the closed leak-proof plastic bags had been deposited in the fixed carrier (FC) used for transport and storage, the bags were picked up to analyze their surface area. The outer surfaces of 60 leak-proof bags with diverse chemotherapy preparations, as shown in Table 3, were tested. Samples were collected over several weeks. The same analytical method was used as described previously.
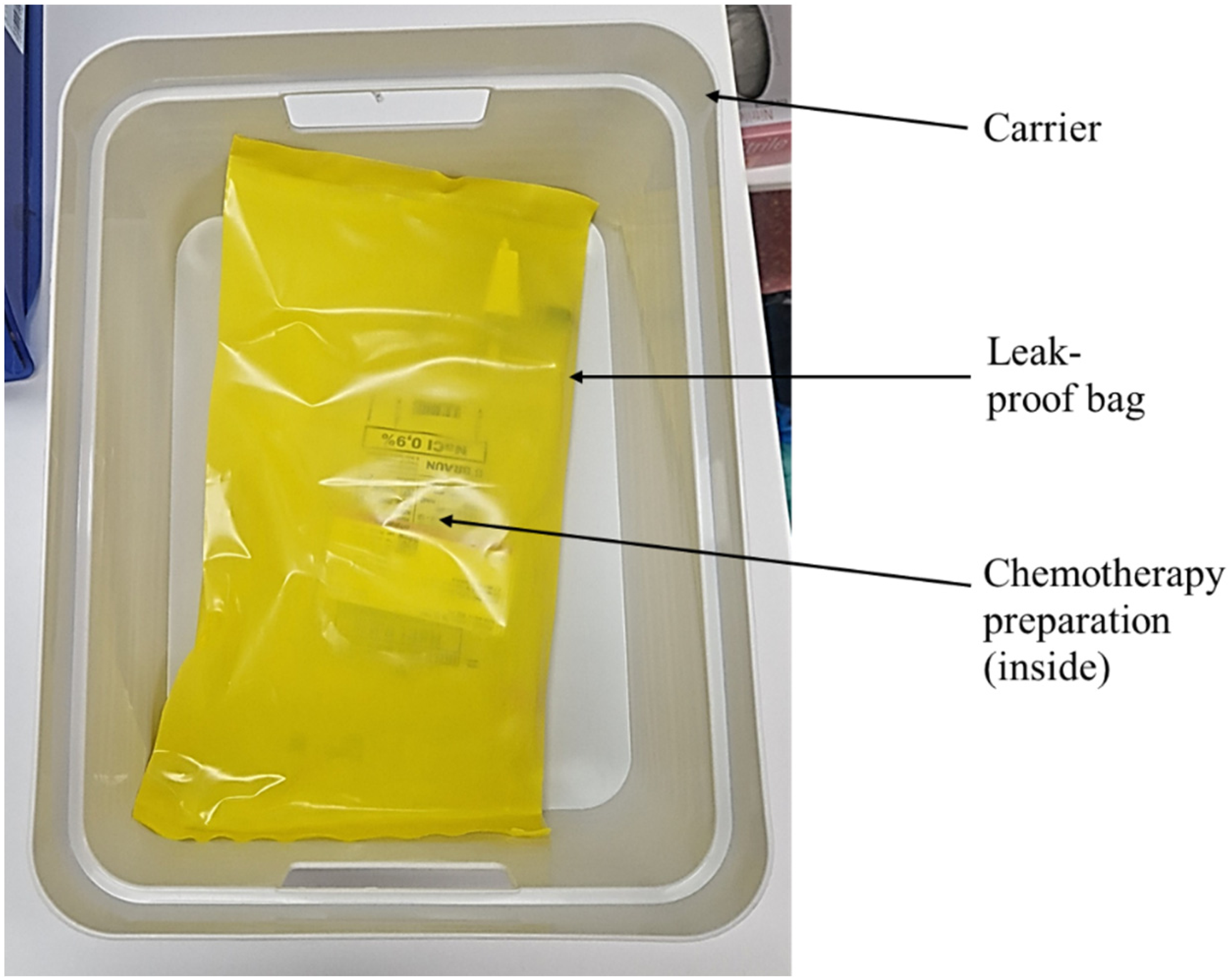
Picture of a leak-proof bag containing an injectable chemotherapy preparation, deposited on a carrier.
Information on injectable chemotherapy preparations produced by healthcare professionals in a Swiss hospital, whose secondary packaging (leak-proof bags) were tested.
Mobile and fixed carriers
As shown in Figure 2, once the antineoplastic drug formulations are prepared in a closed biosafety cabinet (BSC) type III (grade A), they are individually placed in leak-proof plastic bags, which are immediately sealed in a cleanroom (grade C). Then, they are stacked in one of the 10 mobile carriers (MCs) to allow their transport. These carriers are disinfected with Klercide® solution (70% denatured ethanol with water for injection) before and after entry into the cleanroom. When these preparations reach the logistic room, they are transferred to an FC to reduce contact between the formulation and the environment. Then, the mobile carrier is returned to the cleanroom, and the cycle continues. Since the carriers are used to circulate products between the cleanroom and logistic room, these carriers are also in close contact with other antineoplastic products (raw API, conditioning, preparation, and leak-proof bags). Following the results of the leak-proof plastic analyses, the data collection was extended by evaluating the surfaces of both types of carriers (four mobile and one fixed carrier). The same analytical method was used as described previously.
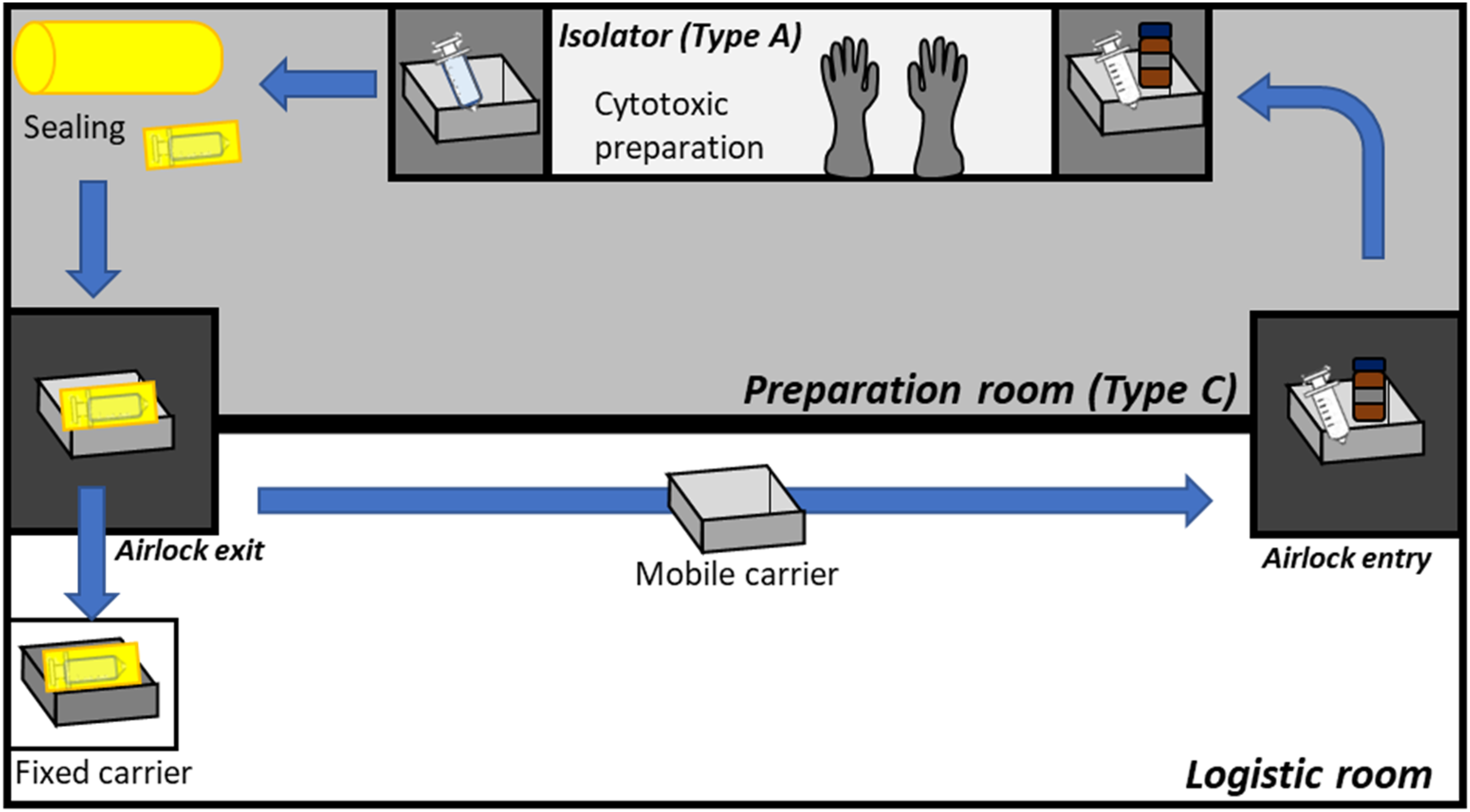
Chemotherapy preparation and transportation cycle with mobile and fixed carriers in the chemotherapy preparation unit of the hospital pharmacy.
Wipe sampling method
Samples were obtained according to the wipe sampling procedure developed and described in a previous study 24 : a swab (TX716, Texwipe, Kernersville, North Carolina, USA) made of polyester was moistened with 75% isopropanol and used to wipe all surfaces. The swab was subsequently desorbed in 2 mL of diluent. After shaking for 10 min, 980 μL of the desorbing solution was transferred into a glass vial, followed by the addition of 20 μL of a mixed internal standard solution (at 5 ng.mL−1 each). The solution was then analyzed via UHPLC‒MS/MS.
Results and discussion
Evaluation of primary packaging for oral formulation
The results obtained for the chemical contamination of primary packaging of oral formulations available on the Swiss market are reported in Table 4. No contamination was observed for five formulations available on the market and the highest average contamination detected (108.2 ng) is obtained for a plastic bottle containing tablets of methotrexate.
Surface contamination results obtained for the evaluation of 36 primary packaging of oral antineoplastic drugs available on the Swiss market.
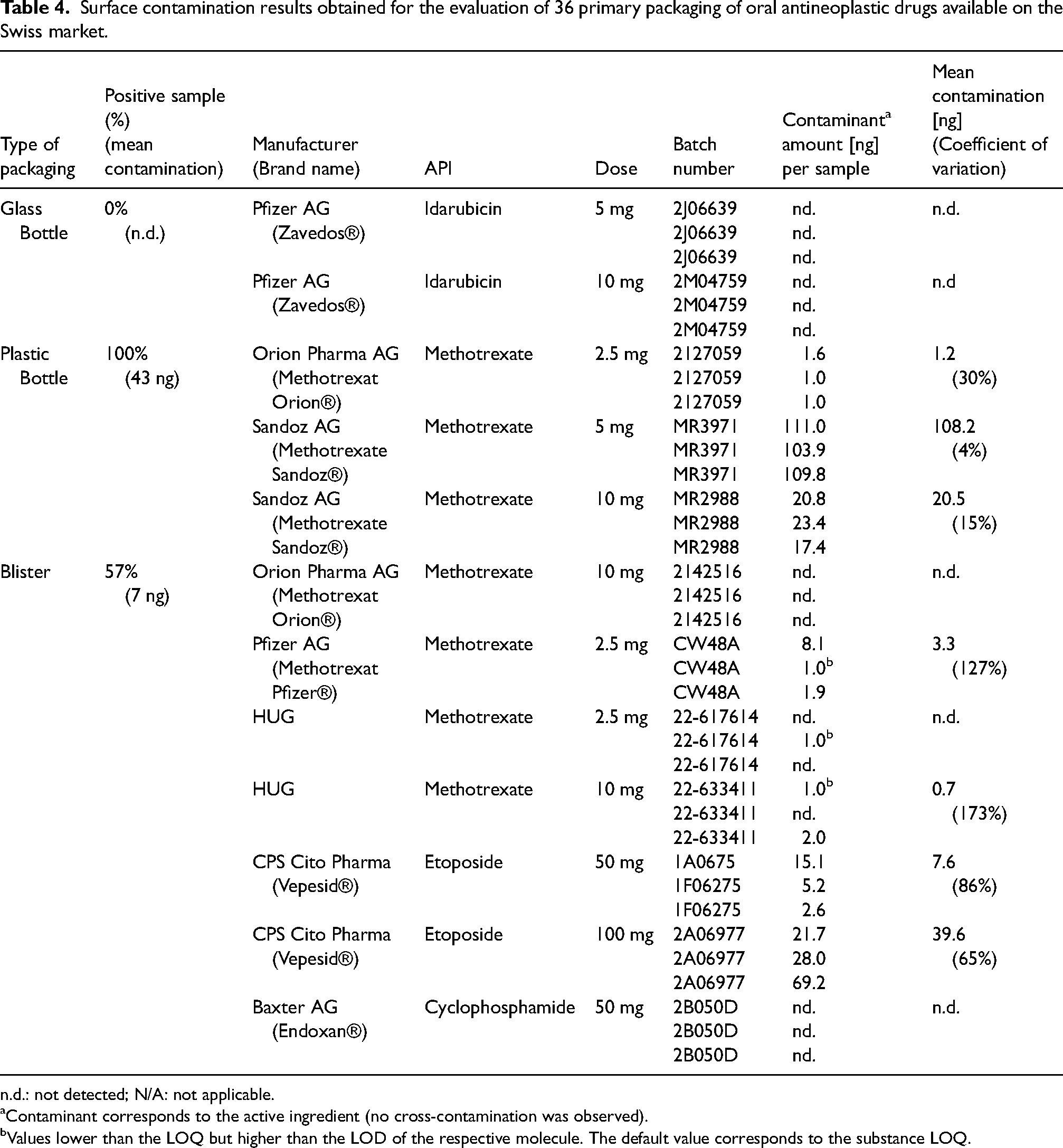
n.d.: not detected; N/A: not applicable.
Contaminant corresponds to the active ingredient (no cross-contamination was observed).
Values lower than the LOQ but higher than the LOD of the respective molecule. The default value corresponds to the substance LOQ.
Out of the 36 samples, 58% of the primary packaging were positive for contamination (i.e. with values higher than the respective limits of detection). All etoposide blisters were contaminated (Table 5). Contamination was also found in 71% of the methotrexate packs. No traces were detected on idarubicin packages or on cyclophosphamide blisters. The highest contaminant amount detected was 111.0 ng on one plastic bottle containing methotrexate from Sandoz®. The mean contamination level was 15.2 ng per sample. The contamination detected on the surface of the primary packaging was related to the corresponding API. No cross-contamination was observed.
Trace contamination of primary packaging of oral antineoplastic drugs tested, listed per active ingredient and percentage of positive samples.

All the plastic bottles were contaminated, as was more than half the blisters (57%). However, no contaminants were detected on the surface of the glass bottles (idarubicin). The average contaminant concentration was greater for plastic bottles (43 ng per sample) than for blisters (7 ng per sample). This outcome could be related to the type of packaging material used: plastic surfaces are more porous and lipophilic than glass surfaces, which are inert and impermeable; therefore, plastic packages allow for less complete chemical decontamination after filling. The variability could also be related to the sampling method. Indeed, the shape of the blisters may not be optimal for cleaning. Another hypothesis is the absence of, or poor chemical decontamination achieved by the manufacturer.
The contaminant amount detected in this study were slightly higher than those observed on the outer blister packages of oral anticancer drugs available in Japan. 14 Indeed, contamination levels between 50.1 and 63.4 ng were detected on the external surface of the bottle of methotrexate tablets. Nevertheless, the contamination levels observed on the primary packaging of oral antineoplastic drugs available on the Swiss market were clearly lower (factor of 20) than those observed on vials containing antineoplastic drugs for injection available on the same market investigated during a previous study. 16
Evaluation of closed leak-proof bags containing an injectable antineoplastic drug preparation and carriers
As indicated in Table 6, 90% of the leak-proof bags and all the carriers were contaminated. The contaminant levels per leak-proof bag and carrier are summarized in Figure 3. The highest total contamination per sample (i.e. the sum of all individual contaminant amounts per sample) was slightly lower than the 40 ng found on the fixed carrier. The average total contaminant level was 3.5 ng per sample (including leak-proof bags and carriers). These detected quantities, which were in the same range as the results obtained for the primary packaging of oral formulations, remained low, that is at trace levels. Several assumptions could explain the presence of contamination. For example, in the preparation room, there are at least two operators: one in charge of preparing the chemotherapy formulation in the isolator and another who assists the main operator in transferring the different products and sealing the final preparations. Although the assistant disinfects each product entering and leaving the airlock and transfer room, they may not change gloves between each handling. Another source of contamination could be the method used for carrier cleaning. Indeed, no chemical decontamination procedure is implemented, and the outer surfaces of these mobile carriers are only systematically sprayed with a Klercide® solution (70% denatured ethanol with water for injection) before entering the airlock of the cleanroom. However, no chemical decontamination is applied to the fixed carrier. Alcohol disinfection only acts against microorganisms and not against chemical contaminants. 31
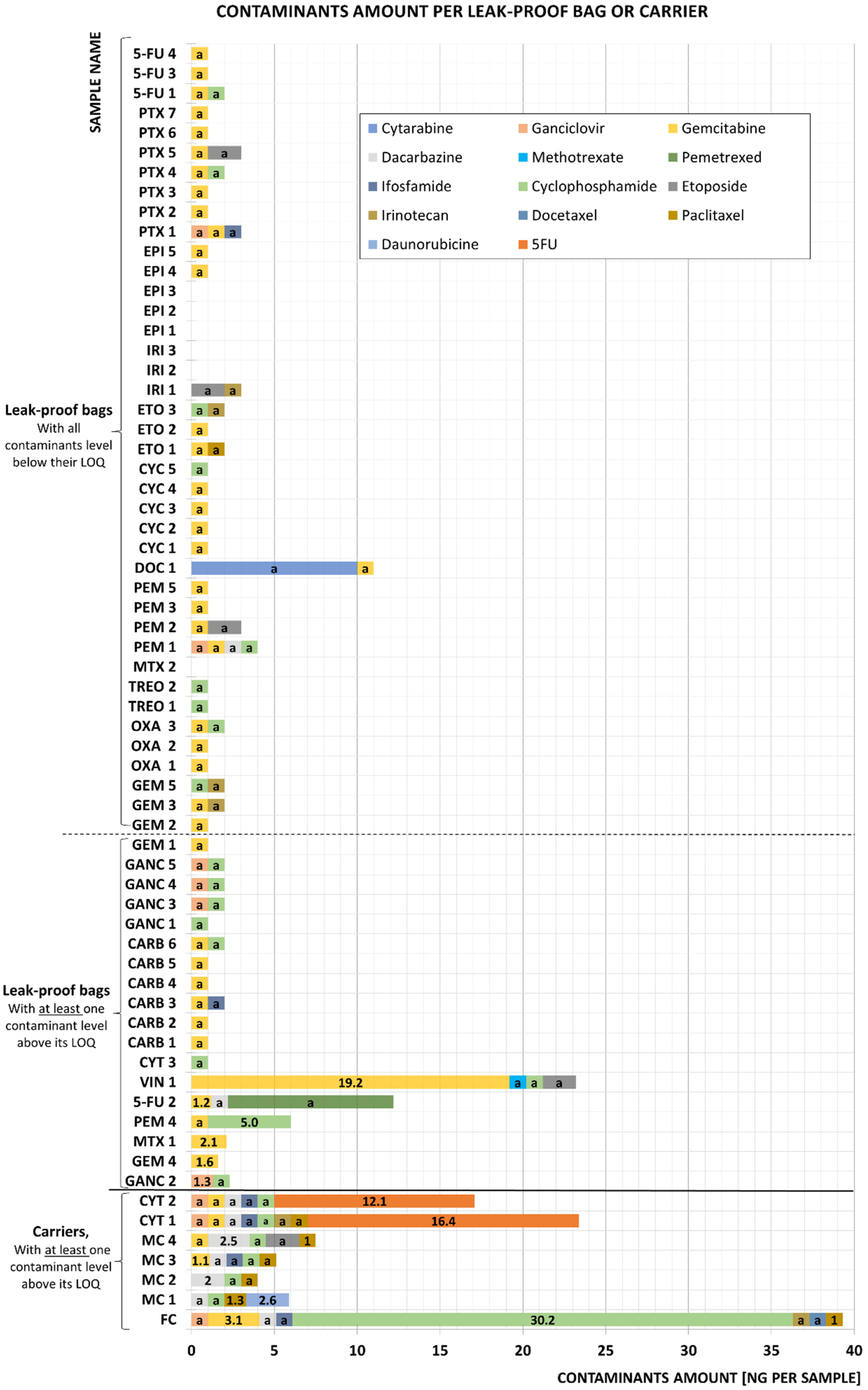
Contamination levels of the leak-proof bags and carriers. The sample names correspond to the API.
Trace contamination of leak-proof plastic bags containing chemotherapy preparations and the carriers on which these bags are placed in the cleanroom.
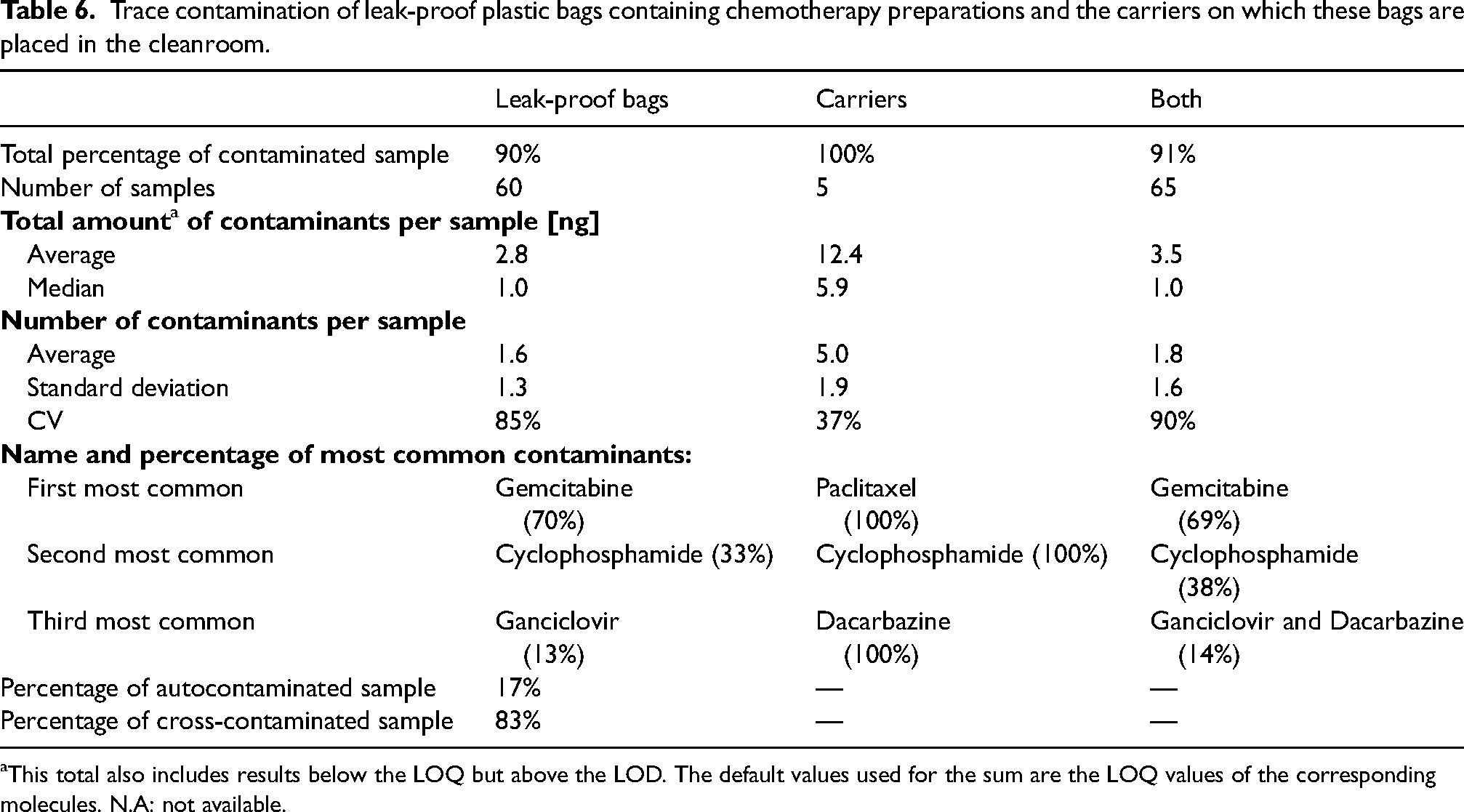
This total also includes results below the LOQ but above the LOD. The default values used for the sum are the LOQ values of the corresponding molecules. N.A: not available.
The type of contamination was mainly cross-contamination: 83% of the samples had a trace of a compound other than its API, while on only 17% of the samples, the API corresponded to one of the surface trace contaminants (autocontamination). Regarding the number of contaminants per sample, leak-proof bags and carriers had an average of 1–2 and 5 contaminants, respectively. The dispersion around the average was also greater among leak-proof bags (85%) than among carriers (37%). The main source of contamination is certainly the preparation of the injectable formulation of chemotherapy itself. Indeed, during preparation in the BSC, the operators’ gloves become contaminated and, in turn, contaminate the primary packaging. Thus, any subsequent handling of the primary packaging contributes to dispersion of the contamination. As the leak-proof bags are handled by the same people (without changing gloves) who take out the formulations produced in the BSC, the latter are contaminated. And the contamination of the leak-proof bags in turn contaminates the carriers. This is verified by the decreasing concentrations of contamination levels the further we move away from the heart of the preparation. However, three samples contained unusually high amounts of contaminants: 16 ng and 12 ng of 5-FU (on CYT 1 and CYT 2, respectively) and 19 ng of gemcitabine (on VIN 1). These results could be explained by contact with leak-proof bags with higher level of contaminations or when handling with contaminated gloves.
The two most common contaminants detected on the closed leak-proof bags and carriers were gemcitabine and cyclophosphamide, which were found in 69% and 38% of the samples, respectively. Other contaminants, such as ganciclovir, dacarbazine, paclitaxel, ifosfamide, irinotecan, and etoposide, were also found in fewer samples (between 8% and 14%). Finally, a small proportion (2–3%) of the samples were contaminated with 5-fluorouracil, cytarabine, methotrexate, pemetrexed, docetaxel, and daunorubicin. These results could be related to the preparation frequency and the amount of active ingredient used for infusions. Indeed, the two most commonly detected contaminants were APIs, which were most often prepared by the hospital pharmacy and whose concentrations were among the highest.
The presence of chemical contamination on leak-proof bags, even at low levels, could be considered problematic. The main objective of the packaging is to protect the environment and healthcare professionals who handle this preparation until it is administered to patients by avoiding direct contact with the product (especially in the event of a leak). Nevertheless, although the leak-proof bags do not prevent completely the chemical contamination, the use of these bags greatly reduces the risk of contamination. Indeed, the contamination levels detected on the primary packaging of injectable antineoplastic drug solutions were between 0.005 and 90 ng.cm−2,32–38 which is clearly higher than the average contamination detected in this study (3.5 ng per leak-proof bag corresponding to 0.0033 ng.cm−2).
Conclusion
Of the 36 primary packaging tested for oral antineoplastic drugs, 58% of the samples were contaminated. The average contaminant concentration was 15.2 ng per sample. The nature of the packaging material and the absence of suitable chemical decontamination methods could be the main explanations for the contamination. For trace contamination of leak-proof bags, 90% of the samples had at least one trace contaminant. All the carriers were contaminated. The average total contaminant concentration was 3.5 ng per wipe sample. The use of carriers to store freshly produced chemotherapy preparations before they are sent to the care units at least partially explains the chemical contamination of the leak-proof bags. Even though several antineoplastic drugs were detected, the level of contamination was relatively low (trace levels) and was similar to the contamination levels recorded on the primary packaging of the oral formulations. However, to avoid chronic exposure of healthcare personnel to these highly toxic compounds, the use of individual protective equipment, particularly suitable gloves, is strongly recommended when handling these products until administration.
Chemical contamination of injectable chemotherapy preparations could be reduced (or even eliminated) by modifying preparation flow at the pharmacy by adding a chemical decontamination step either for the carriers between each use or for the leak-proof bag before sending them to the care units. In the case of oral formulations, chemical decontamination of packaging before use is not realistic, and reducing exposure undeniably requires wearing suitable gloves when handling primary packaging. However, manufacturers should increase their efforts to implement validated decontamination procedures to ensure the supply of uncontaminated and safe packaging.
Footnotes
Authors contribution
N.N. contributed to the concept and analysis of the work, analyzed and interpreted the data, drafted and contributed to the version to be published. V.V. contributed to the concept and analysis of the work and approved and revised to the version to be published. L.B., L.F., S.R., and P.B. contributed to the concept of the work, approved and revised to the version to be published. S.F. supervised the work, contributed to the concept and analysis of the work, approved and revised to the version to be published.
Data availability
The data will be made available upon request.
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.