
Abstract
Background
Immune checkpoint inhibitor (ICI)-associated acute interstitial nephritis (AIN) is a recognized complication of immunotherapy (IO), but literature on its management and outcomes is limited.
Methods
We retrospectively reviewed patients who received ICIs and developed biopsy-proven or clinically-suspected ICI-associated AIN at the University of Virginia Comprehensive Cancer Center from 2012–2023. We analyzed baseline characteristics and clinical outcomes, including treatment interruption and rechallenge rates. Acute kidney injury (AKI) was defined as a ≥ 1.5-fold increase in baseline creatinine under seven days, a two-fold increase above the upper limit of normal, or an increase by ≥0.3 mg/dL. Kidney function returning to within 0.3 mg/dL or less than twice baseline was considered complete (CRc) and partial (PRc) recovery, respectively.
Results
We identified 12 cases of ICI-AIN: four by biopsy (33%) and eight (67%) by clinical suspicion. Two patients received anti-CTLA-4 and anti-PD1, six received anti-PD1 alone, and four received chemo-immunotherapy. The majority (58%) of patients developed AIN within the first 5 cycles. Eight patients developed ≥ Grade 3 AKI, and six developed multiple irAEs. ICI was permanently discontinued in seven patients (58%) and temporarily interrupted in four (30%). The CRc and PRc rates were 67% and 8%, respectively. Upon AIN onset, the best disease response was stable disease in five patients, partial response in three, and progressive disease in three. Median overall survival was 4.87 years, and progression-free survival was 1.5 years.
Conclusions
Rechallenge with IO after kidney irAE may be possible in some patients but requires careful evaluation on an individual basis.
Keywords
Introduction
Immune checkpoint inhibitors (ICI) are increasingly being used for the treatment of various solid tumors. With proven efficacy in both metastatic and early-stage solid tumors, their use is expected to increase significantly. The first ICI approved by the Food and Drug Administration in 2011 was ipilimumab, a monoclonal antibody against cytotoxic T-lymphocyte antigen-4 (CTLA-4), for the treatment of advanced melanoma. Subsequently, the two most widely prescribed programmed cell death protein-1 (PD-1)-targeting ICIs, nivolumab and pembrolizumab, were approved in 2015 for melanoma. Since then, atezolizumab, durvalumab, cemiplimab, avelumab, dostarlimab, and relatlimab have been approved by the Food and Drug Administration (FDA) for various indications. Collectively, ICIs have advanced to gain indications in front-line metastatic and even neoadjuvant and adjuvant therapies for over 30 tumor types. 1
ICIs have substantially improved the outcomes of several malignancies. However, with the expanded utilization of these therapies, an increasing number of immune-related adverse events (irAEs) have been reported. In a meta-analysis of 125 clinical trials of PD-1 and programmed death ligand-1 (PD-L1) inhibitors involving over 20,000 patients, the overall incidence of irAEs was as high as 66.0%, with 14.0% of patients experiencing grade 3 (G3) or higher AEs, as determined by the Common Terminology Criteria of Adverse Events (CTCAE) criteria. Some of the most common high-grade irAEs are hepatitis, colitis, and neutropenia, although immune-mediated dysfunction of nearly every organ has been observed. 2
Acute interstitial nephritis (AIN), although a rare irAE, is the most common form of nephrotoxicity following ICI administration. 3 Unlike most drug-induced AIN, immune-mediated AIN presents similar to autoimmune disease, with biopsies typically showing tubular rather than glomerular injury. Characteristic features include edema, tubulitis, and interstitial infiltration of CD4 + and CD8 + lymphocytes. 4 Urine studies often show sterile pyuria and white blood cell casts. 5 The most common clinical manifestation is acute kidney injury (AKI), as defined by a rising creatinine (Cr), which is seen in 2% of patients receiving ICIs. Furthermore, 1% of patients exhibit electrolyte derangements, and 0.5% require dialysis. 6 Case reports suggest that the incidence of ICI-induced AKI may be far higher in clinical practice. 7 As with most irAEs, the standard-of-care treatment is ICI cessation and corticosteroid initiation. Although AIN is a rare but potentially devastating sequela of ICI therapy, the presentation, management, and outcomes of patients have been poorly characterized in the literature. In particular, the rate of ICI rechallenge remains unexplored in the literature.
We present one institution's experience with the diagnosis and treatment of ICI-induced AIN to improve the detection and management strategies for the growing number of patients receiving ICIs today.
Methods
A single-center, retrospective observational study was performed by searching the electronic medical records of all patients who received CTLA-4 inhibitors or PD-1/PD-L1 inhibitors from January 1, 2012 to January 1, 2023, at the University of Virginia Comprehensive Cancer Center. Patients with a Cr increase ≥1.5-fold from baseline within the prior seven days, 2-fold increase above the upper limit of normal, or an increase in serum creatinine by ≥0.3 mg/dL were screened for AIN. AIN cases associated with a possible kidney immune-related adverse event (irAE) were identified by clinical documentation by a consulting nephrologist, histological confirmation by kidney biopsy, or after mutual consensus by OE and JP performing the retrospective chart review. Patient demographics, cancer diagnosis and staging information, concomitant medications, comorbidities, baseline characteristics, clinical course, management, rates of treatment interruption and rechallenge, and subsequent patient outcomes were collected. AKI severity was staged according to the Common Terminology Criteria for Adverse Events (CTCAE) criteria. 8 Baseline creatinine was defined as the last stable serum creatinine value before the patient developed AKI according to the criteria above. Complete resolution of the irAE was defined as return of kidney function within <0.3 mg/dl of baseline creatinine by the end of steroid course. Partial resolution was defined as creatinine >0.3 mg/dl from baseline, but less than two times the patient's baseline creatinine level by the end of the steroid course. No response was recorded if the patient's kidney function remained above two times the baseline creatinine level or if kidney function continued to deteriorate.
This study was approved by the institutional review board of the University of Virginia. Statistical analysis was performed using SPSS Version 28 for Windows (IBM Corp., Armonk, NY, USA). Independent sample t-tests and chi-square analyses were used for univariate comparisons. Overall survival (OS) was defined as the time between diagnosis and the date of death, and patients alive at the time of data collection or lost to follow-up were censored at the date of the last follow-up. Progression-free survival (PFS) was defined as the time between diagnosis and disease progression, as established clinically by an oncologist and/or on imaging by a radiologist; patients who did not progress at the time of data collection or were lost to follow-up were censored at the date of last follow-up. OS and PFS were assessed using Kaplan–Meier and Cox regression methods. P-values less than 0.05 were considered statistically significant.
Results
Baseline patient characteristics and ICI treatment
Of the 1979 patients who received ICI therapy for various indications, 12 (0.6%) had biopsy-proven or clinically suspected AIN. Four patients (33%) had biopsy-proven AIN and 8 (66%) had clinically suspected ICI-associated AIN. Among the 12 patients with ICI-AIN, the median age at diagnosis was 69 years (IQR: 57–86), the male-to-female ratio was 2:1, and 9 (75%) were white. The median body mass index (BMI) was 28 kg/m2 (21–39). The diagnoses for which patients were undergoing ICI therapy were non-small cell lung cancer (NSCLC) (42%), urothelial cancer (33.3%), melanoma (16.7%), and hepatocellular carcinoma (HCC) (8.3%) (Table 1).
Baseline characteristics of patients undergoing ICI therapy.
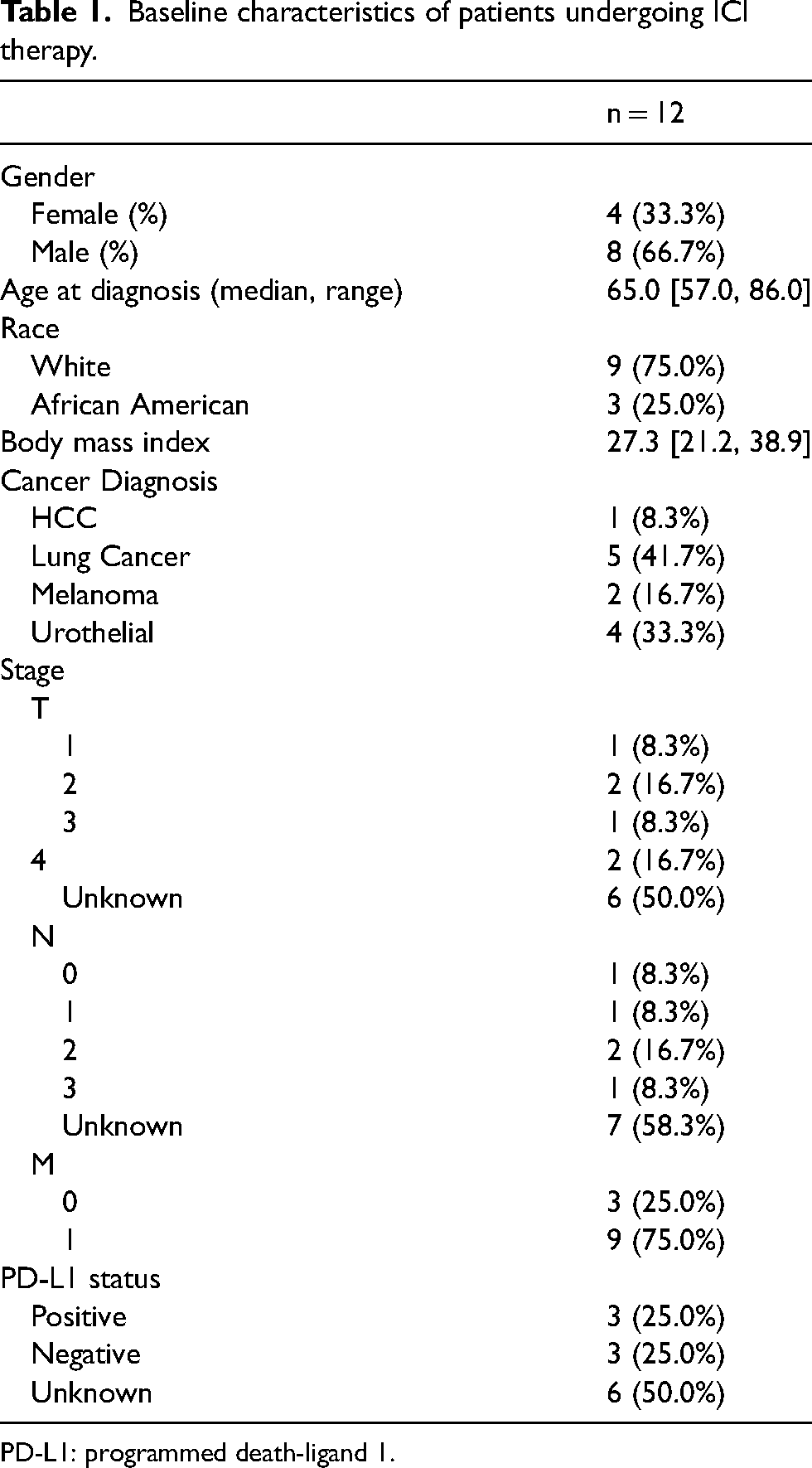
PD-L1: programmed death-ligand 1.
In terms of therapy type, two patients (17%) received a combination of anti-CTLA-4 and anti-PD-1, six patients (50%) received anti-PD-1 alone and four patients (33%) received chemo-immunotherapy. Three patients (25%) were on concurrent nonsteroidal anti-inflammatory drugs (NSAIDS) and five patients (42%) were on proton-pump inhibitors (PPI) concomitantly. Intent of ICI was adjuvant in 30% of patients and palliative in 70% of patients (Table 2).
Treatment characteristics of patients undergoing ICI therapy.
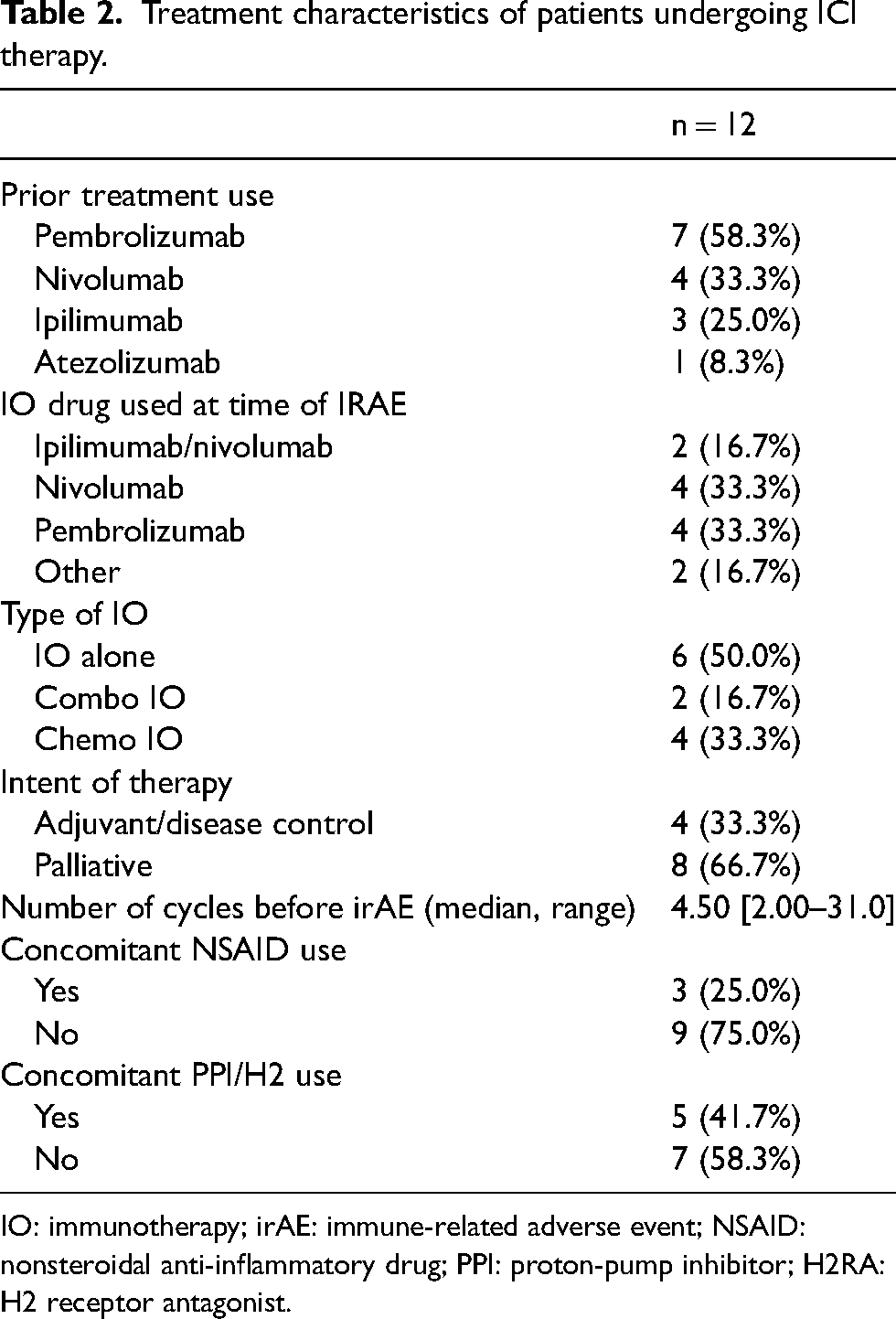
IO: immunotherapy; irAE: immune-related adverse event; NSAID: nonsteroidal anti-inflammatory drug; PPI: proton-pump inhibitor; H2RA: H2 receptor antagonist.
Diagnosis, management, and outcomes
All patients had baseline and pre-treatment complete blood cell count and metabolic panels, demonstrating a median baseline white blood cell (WBC) count of 7.54 × 109/L [4.32–13.9], platelet count of 276 × 109/L [96.0–423], hemoglobin of 11.9 g/dL [8.00–14.2], sodium of 137 mEq/L [118–147], potassium of 4.35 mEq/L [3.80–6.40], blood urea nitrogen of 43.5 mg/dL [21.0–62.0], and creatinine of 3.20 mg/dL [1.50–8.50]. Eleven of the twelve patients (92%) underwent urinalysis (UA) testing, with a median UA WBC count of 0 × 109/L [0–70.0]. Leukocyte esterase results demonstrated large amounts in two patients (17%), moderate in two (17%), small in two (17%), trace in one (8%), and an absence in four (33%). For UA eosinophil testing, nine patients had none (75%), two had rare counts (17%), and one had missing results (8%). On UA protein testing, four had 1 + protein (33%), one had 2+ (8%), four had trace (33%), and two had no detection (17%). On UA blood testing, one patient had moderate (8%), one had small (8%), three had trace (25%), and six had none (50%).
Four patients (33%) developed a G2 AKI, five patients (42%) developed G3 AKI, and three patients (25%) developed G4 AKI. The median number of immunotherapy cycles before AIN onset was 4.5 (2.0–31.0), and seven patients (58%) developed AIN within the first five cycles. Eight patients (66%) developed CTCAE ≥ G3 AKI. The median increase in creatinine (Cr) was 2.65 (1.0–7.3). Ten patients (83.3%) underwent imaging with ultrasound (80%) or CTAP (50%), which showed “mild hydronephrosis” in five patients (50%) and “no abnormalities” in the remaining five (50%). Four patients (33.3%) underwent renal biopsy, and 11 (91.7%) received nephrology consultation. ICI was temporarily interrupted in four patients (30%) and permanently discontinued in seven patients (58%). All patients received steroids. Median steroid dose was 1.0 mg/kg/day (0–2.0). The median duration of ICI interruption was 221 days, and the median duration of steroid use was 4.0 weeks (0–8.0) (Table 3).
Immune related adverse events and outcomes.
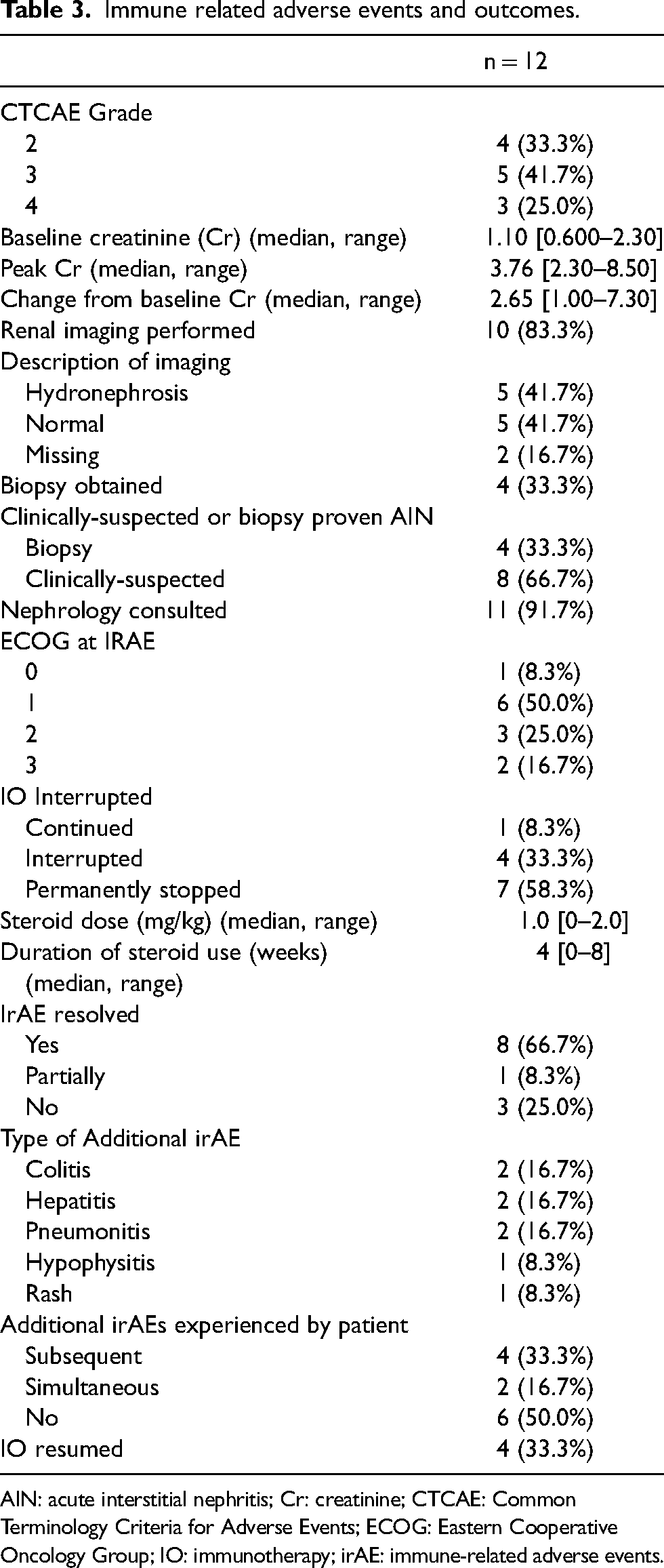
AIN: acute interstitial nephritis; Cr: creatinine; CTCAE: Common Terminology Criteria for Adverse Events; ECOG: Eastern Cooperative Oncology Group; IO: immunotherapy; irAE: immune-related adverse events.
Rate of CRc (complete response) and PRc (partial response) of AIN were 67% and 8%, respectively. Additional irAEs were observed in 50% of patients, concurrently in two patients (17%) and subsequently in four patients (33%). The most common additional irAEs were colitis (16.7%), hepatitis (16.7%), and pneumonitis (16.7%) (Table 3).
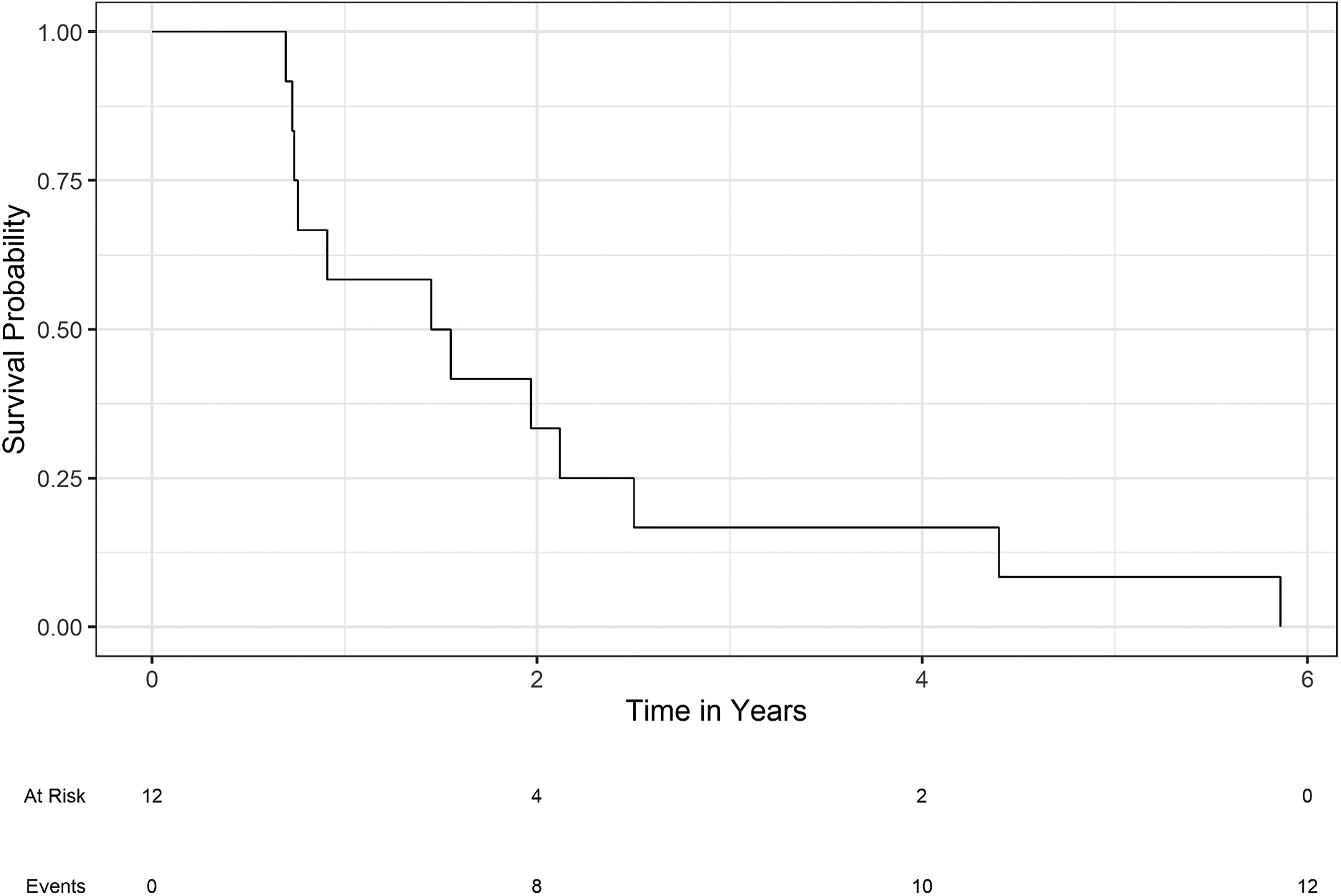
In four patients (33%), ICI was resumed after resolution. At a median follow-up time of 160 days, three patients (25%) continued to receive anti-PD-1 therapy following rechallenge until progressive disease (PD), additional irAEs, or therapy completion (Table 3). At the time of AIN onset, the best disease response of the underlying malignancy to ICI therapy was stable disease (SD) in five patients (42%), PR in three patients (25%), and PD in three patients (25%). For the entire cohort of patients who developed AIN, the median OS from the date of diagnosis was 4.87 years (95% CI 2.48–7.26; Figure 1); for stage IV patients, the median OS was 3.81 years (95% CI 2.12–5.50). The median PFS was 1.5 years for all patients (95% CI 0.76–2.24; Figure 2).
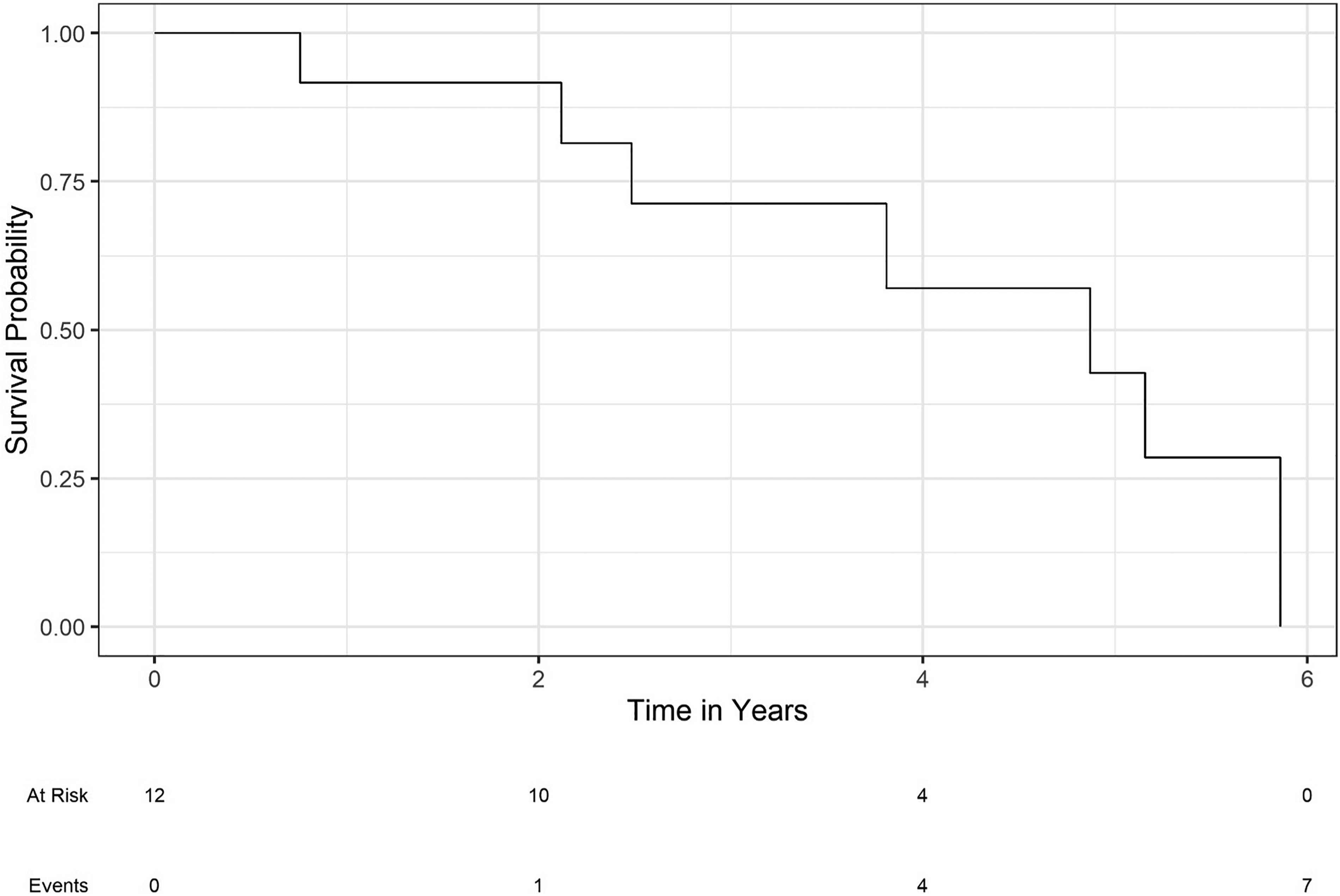
Overall survival of all patients receiving ICI therapy who developed an irAE.
Progression-free survival of all patients receiving ICI therapy who developed an irAE.
Discussion
In this retrospective single-institution study, we found that the incidence of ICI-associated AIN in patients receiving ICI therapy for various cancers was relatively rare, although it often coincided with the development of additional irAEs and permanent discontinuation of cancer treatment, with only a handful of patients tolerating ICI rechallenge.
Only 0.6% of 1979 ICI-treated patients within our cohort were diagnosed with AIN, either through biopsy or clinical suspicion. It is conceivable that not all patients who developed AKI were recognized and reported as AIN; thus, the true incidence of renal irAEs may be higher in patients receiving ICI therapies. Although kidney biopsy remains the gold standard for diagnosis, one-third of our patients underwent treatment based solely on clinical suspicion, yielding relatively efficacious responses. Biopsy may be helpful if the clinical presentation is ambiguous, as ICI-induced AKIs could originate from alternative or concurrent causes such as glomerular disease.5,9 Considering the risks and costs associated with kidney biopsy, a deferred biopsy approach for patients with AKI refractory to initial corticosteroid therapy may be reasonable.
Interestingly, half of our patients exhibited imaging findings consistent with hydronephrosis; however, these cases were mild and, therefore, unlikely contributors to the observed AKIs. This suggests that hydronephrosis in patients with AKI on ICIs could serve as a screening tool before more invasive diagnostic approaches are considered to confirm AIN. Further research is needed to validate this approach as the possible relationship between hydronephrosis and AKI prognosis in the setting of irAEs remains incompletely explored in the literature.
A significant proportion of patients who developed ICI-induced AIN were receiving concomitant PPIs (42%) and NSAIDs (25%), medications known to be associated with drug-induced AIN. 10 PPI and NSAID use in the setting of immunotherapy has been demonstrated to be a risk factor for AKI in several studies,11–13 though not all.14–17 One study in particular found that patients who were on PPIs at the inception of ICI therapy had a quicker onset of AKI development compared to patients on ICI with AKI from other causes. 13 Nonetheless, in appropriate patients, alternatives such as famotidine could be considered to potentially reduce AIN risk during ICI therapy. 18 There is currently no consensus on how to approach medication management during treatment cycles. Further research is required to explore whether there is a significant benefit in the cessation of such drugs prior to ICI initiation.
All patients in our cohort were treated with steroids, typically 1 mg/kg/day for a median of four weeks. 75% of our patients achieved complete or partial resolution of their AIN, underscoring the relative manageability of AIN for the majority of patients when recognized and treated appropriately with a prolonged steroid course. Steroid regimens for ICI-induced nephritis vary in the literature, with different degrees of response depending on the dose or taper timeline.9,19 A prior study by Manohar et al. found that patients who exhibited complete recovery received higher initial doses (median of 2.79 mg/kg per month). 9
Unfortunately, the onset of ICI-AIN invariably led to therapy delay, interruption, and/or discontinuation in a significant proportion of patients, with a median treatment interruption duration of 160 days. Around half of our patients developed additional irAEs, such as colitis, hepatitis, and pneumonitis, further validating data that suggests the development of one irAE heightens the risk of subsequent irAEs. 2 Seven of the 12 patients who developed AIN permanently discontinued the ICI therapy. Four patients attempted ICI rechallenge with anti-PD1 monotherapy and tolerated treatment until disease progression, therapy completion, or an additional irAE. Our data suggest that a cohort of patients can tolerate ICI resumption after treatment with ICI-induced AIN.
Although irAEs can alter a patient's treatment and disease course, the risk of irAEs should not preclude treatment, as multiple studies have demonstrated a net benefit of improved survival in many cancers, even with the development of irAEs.20–24 The decision to rechallenge after an irAE should be made on an individual basis, factoring in the patient's overall condition and preference as well as irAE type and severity, among other considerations. Evidence from retrospective studies has been mixed. Some findings suggest that rechallenge is a feasible approach for multiple cancers, including NSCLC 25 and urothelial cancer. 26 However, other studies have shown variable overall response rates and toxicities with rechallenge.27–30 Outcomes are largely dependent on the irAE type, where complications such as myocarditis and myositis tend to be more fatal. 28 In the case of AIN, a study by Dolladille et al. identified 276 cases of ICI-associated nephritis in which only 4 of the 78 patients who were rechallenged developed irAE recurrence, all of which were the same as the initial event. Therefore, of the various irAEs, AIN may be more amenable to ICI rechallenge, however prospective studies are needed to better evaluate for differences in overall response rates and survival outcomes.
The limitations of this study include its retrospective nature, as well as an element of selection bias, as our chart review may not have captured all patients who developed AKI on ICI. The threshold of >1.5-fold increase or twice the upper limit of normal for creatinine may have inadvertently excluded milder cases of ICI-induced AIN, potentially limiting the scope of identified cases. Additionally, the eight patients with clinically suspected AIN may have had alternate etiologies of AKI, although AIN was favored in these cases based on a constellation of clinical findings, including supporting results from diagnostic tests by the nephrologist. Given the rare overall incidence of AIN at our institution, subgroup analyses (i.e., cancer type and ICI ICI-rechallenge) to better characterize these events were also limited.
This study highlights the rare incidence of ICI-associated AIN. The occurrence of irAEs can substantially impact the prognosis of patients, particularly those already at severe stages of disease and those who develop multiple irAEs; therefore, increased vigilance for signs and symptoms precipitating adverse events is needed. Further development of an AKI biomarker/risk calculator tool for early recognition and subsequent care of patients with suspected ICI-AIN would require a larger multicenter collaboration to better report and understand this complication. The successful toleration of PD-1 inhibitor rechallenge in a subgroup of patients bolsters this approach as a viable treatment strategy in the otherwise challenging landscape of post-irAE management. As ICI therapy continues to rise—particularly for cancers where clinical benefit outweighs potential risk—it is crucial to quantify complications, such as AIN, and analyze outcomes with a forward approach towards optimizing diagnosis and treatment and improving overall patient survival.
Footnotes
Author contributions
OE, AB, JP, JX, JS, and VK contributed to writing the original draft. OE and JP were involved with data collection. JP and BH performed the statistical analysis. OE, RP, AB, JX, JS, and VK were involved in revising the manuscript. All authors reviewed and approved the final version of the manuscript.
Data availability
The data available in this study can only be obtained from the authors.
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Research ethics and patient consent
This work was reviewed by the University of Virginia Institutional Review Board and approved according to protocol #HSR 24436. All studies were conducted in a HIPAA-compliant manner and in accordance with the Declaration of Helsinki.