
Abstract
Background
Niraparib has been authorized for maintenance treatment of epithelial ovarian cancer after first-line treatment with platinum, in partial or complete response.
Objectives
To evaluate the effectiveness and safety of maintenance niraparib in platinum-sensitive recurrent ovarian cancer (PSROC) patients in a tertiary hospital.
Materials and Methods
This retrospective observational unicentre study included women diagnosed with ovarian adenocarcinoma who received niraparib. Eligibility criteria encompassed women with PSROC, in response to platinum chemotherapy, and not previously treated with other PARPis. Data on demographics, comorbidities, BRCA mutation status, disease stage, treatment history and adverse events were recorded. Progression-free survival (PFS) and overall survival (OS) were estimated using the Kaplan–Meier method.
Results
A total of 33 patients were included, with a median age of 63.5 years. The majority of patients received niraparib at 200 mg/day based on Research on Adverse Drug Events and Report criteria. Median OS was 30 months (95% CI: 16.76–43.23), and median PFS was 8 months (95% CI: 2.48–13.52). Adverse effects were more frequent during the initial months of treatment, with most classified as CTCAE v5 grade 1–2. Dose reductions, interruption of treatment and discontinuations were observed due to haematologic toxicities primarily.
Conclusion
This real-world study showed that maintenance niraparib in PSROC patients had effectiveness and safety profiles consistent with clinical trials and other observational studies. Median PFS and OS were comparable to previous reports, and most adverse events were manageable with dose modifications. The results support the use of niraparib as a maintenance therapy option in this patient population.
Introduction
Ovarian cancer is the most common cause of death among gynecologic malignancies and is the fifth leading cause of cancer death in women in developed countries. It mainly affects postmenopausal women with a peak incidence between 55 and 65 years, and most of the patients are diagnosed at an advanced stage due to non-specific clinical symptoms.1,2
Epithelial ovarian cancer (EOC) accounts for more than 90% of the cases. Advances in the knowledge of histological and molecular characteristics have established the existence of five subtypes. High-grade serous ovarian cancer (HGSOC) is the most frequent one (75%) and it normally arises from a precursor lesion in the fallopian tube. 3
The standard treatment for EOC is cytoreductive surgery followed by platinum-taxane-based chemotherapy that can be associated with bevacizumab in advanced disease. Despite a high response rate to chemotherapy, 60–80% of patients will relapse in the first three years of follow-up.1–4
The advent of inhibitors of poly (ADP-ribose) polymerase (PARPis) enzymes has provided a welcome boost in the approach to this type of tumor. Olaparib was the first PARPi to come onto the market and was approved in 2014 by the European Medicines Agency (EMA) for the maintenance treatment of adult ovarian cancer relapse in patients who are in response (complete or partial) to platinum-based chemotherapy with BCRA1/2 mutation. 5
In November 2017, Niraparib has appeared for maintenance treatment in patients who are in response (complete or partial) to platinum-based chemotherapy after relapse regardless of BRCA status. 6 In 2018, the latest PARPi currently on the market, Rucaparib, was authorized, indicated for the maintenance treatment of patients in relapse, sensitive to platinum, who fully or partially respond to platinum-based chemotherapy. 7 Evidence regarding PARPis suggested that maintenance therapy with them could be considered a good strategy for patients with platinum sensitivity.
Currently, Niraparib and Olaparib have been authorized for maintenance treatment after first-line treatment with platinum, in partial or complete response (CR), both by the EMA and by the FDA. However, the approvals are too recent to have real-life efficacy data. 8
The ENGOT-OV16/NOVA study, which led to the approval of Niraparib in this setting, demonstrated an increase in progression-free survival (PFS) compared to those in the placebo group, both in patients with BRCA mutations (21 months vs. 5.5 months), and in the overall BRCA wild-type population (9.3 months vs. 3.9 months). 9 Afterwards, the NORA (platinum-sensitive recurrent ovarian cancer [PSROC]) and PRIME (newly diagnosed) trials showed that patients with a body weight <77 kg or a platelet count <150 × 103/μL can initiate niraparib maintenance therapy at 200 mg/day with a lower incidence of adverse events (AEs) and no reduction in efficacy.10,11
Real-world evidence is associated with higher external validity than clinical trials in the target population, which often provide a managed environment with high internal validity but may not represent the true nature of clinical practice due to strict exclusion criteria. A recently published study by the Grupo Español de Investigación en Cáncer Ginecológico (GEICO) demonstrated that tolerability and activity of niraparib maintenance therapy for PSROC in Spanish real-world population was consistent with the pivotal study. However, these data are from the use of the drug through expanded access, these treatments had to request authorization through regulatory agencies and therefore do not accurately describe the current moment. 12
The objective of our study is to evaluate the efficacy and safety of niraparib in patients with recurrent ovarian cancer with platinum-sensitive disease, in response to prior platinum treatment, under conditions of immediate access to the drug with marketing authorization and financing agreement in the indication studied, and see to what extent these results are similar or not to those obtained in clinical trials and other existing studies in this field.
Materials and methods
Study design and population
A single-centre, retrospective, observational and descriptive study which included women diagnosed with recurrent ovarian cancer who received niraparib was performed between August 2017 and December 2022 in a tertiary hospital of the Public Health System of Andalusia, Spain.
Patients were identified from the Electronic Prescription System (ATHOS®), all patients who started treatment with niraparib for the indication studied during the detailed period were selected.
The study was designed in accordance with the Strengthening the Reporting of Observational Studies in Epidemiology reporting guidelines.
Eligibility criteria
Patients were selected with the following criteria:
Women older than 18 years diagnosed with PSROC in response (complete or partial) to platinum-based chemotherapy, starting niraparib for maintenance following standard-of-care treatment. Previous treatment with PARPi was not allowed.
Study variables and analysis
The following data were registered:
Variables to describe the baseline characteristics of the patients
Demographic variables – patients’ age.
Body mass index.
Comorbidities (arterial hypertension, diabetes, thyroid disease, previous breast cancer, asthma).
Eastern Cooperative Oncology Group (ECOG) of Performance Status (PS) recorded in the medical record before starting treatment with niraparib.
BRCA mutation (somatic and germline): wild type, mutated or not determined.
Disease stage at diagnostic – Basal International Federation of Gynaecology and Obstetrics (FIGO) staging system at diagnostic.
Histological type of ovarian cancer
If neoadjuvant chemotherapy was received.
First-line treatment received.
Response to first-line platinum-based chemotherapy: partial response (PR) or CR.
Platinum-free interval (PFI; months). Platinum-resistant was defined as recurrence disease in less than six months, partially platinum-sensitive in 6–12 months and platinum-sensitive in 12 months or more.
Number of previous chemotherapy lines.
Radiologic response to last chemotherapy before niraparib administration: CR, PR or stable disease.
Effectiveness variables
Progression-free survival (months): PFS was defined as the time between the date of the initiation of niraparib and the date of progression or death by any cause.
Overall survival (OS; months): OS was defined as the time between the date of initiation of niraparib and the date of death by any cause.
Safety variables
Adverse events: To perform the safety analysis, haematological parameters were recorded as haemoglobin, platelets, leukocytes, neutrophils in order to determine possible AE such as anaemia, thrombocytopenia, leukopenia and neutropenia. In addition, the adverse effects reported by the patients and registered in the clinical record such as asthenia, nausea, vomiting, abdominal pain and hypertension were collected and classified according to the Common Terminology Criteria for Adverse Events v.5 (CTCAE). 13 The data were recorded at 1, 3, 6, 9 and 12 months later after its initiation. Haemoglobin, platelet, leukocyte and neutrophil levels were also recorded before starting niraparib. Patients with spikes in blood pressure during niraparib treatment reported in their medical records were also recorded. And if they had presented a hypertensive crisis that required emergency health care.
Dose reductions, interruption treatment and discontinuation treatment and their causes during the first year of treatment.
The outpoints were obtained from the electronic clinical records and the oncology pharmacy database until date of death or the established deadline (December 2022).
Statistical analysis
Quantitative variables were summarized with medians and interquartile ranges (IQR = quartiles 25 and 75) and categorical variables with percentages. OS and PFS probability were estimated through Kaplan–Meier method. Patients that did not experience the event (death and/or progression) at the study cut-off date were censored. Statistical analysis was carried out with the SPSS® 24.0 statistical software.
Ethics
In accordance with the Organic Protection of Data Law 15/1999, of 13 December (OPDL), and to protect patient's confidential data, patients were identified by a corresponding numerical code. So, it was not necessary to obtain informed consent.
Results
Patients’ characteristics
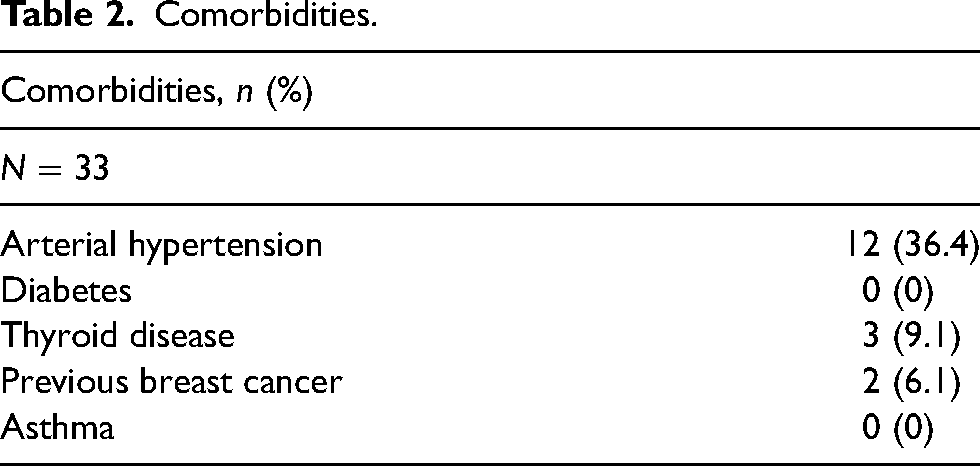
A total of 33 women were included in the study, with a median age of 63.5 (53.0–71.5). The baseline characteristics of the population are shown in Table 1. Regarding comorbidities, almost half of the population had some studied comorbidity (Table 2), the most prevalent was arterial hypertension (36.4%). A total of 45.5% of patients had an ECOG 0 at the beginning of niraparib treatment. Somatic BRCA mutation status was unknown in 51.5% of patients, meanwhile in four patients the germline BRCA was unknown. Most of the patients had FIGO stage III–IV at diagnosis of their ovarian cancer, 60.6% stage III and 24.2% stage IV. The predominant histology was high-grade serous ovarian cancer (88.0%).
Baseline characteristic population.
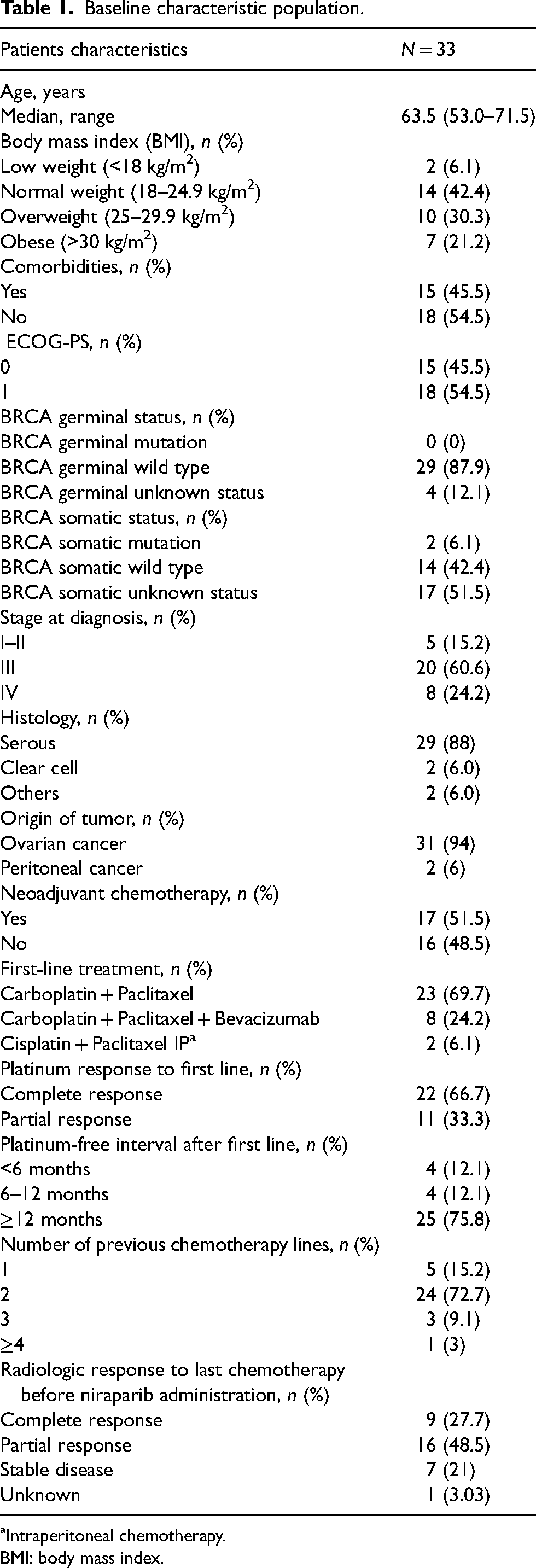
Intraperitoneal chemotherapy.
BMI: body mass index.
Comorbidities.
Most patients had a PFI more than 12 months (75.8%). Nine patients started niraparib treatment at 300 mg, all had platelet levels above 150.000/μL, but three of them weighed less than 77 kg. The rest of the patients except one, who started with 100 mg, started niraparib with 200 mg, based on Research on Adverse Drug Events and Report (RADAR) criteria. 14 Of these, two patients weighed more than 77 kg and did not have thrombocytopenia. The radiologic response to the last chemotherapy before niraparib administration was CR in 27.3% of the patients (Table 1).
Effectiveness
In terms of effectiveness, after the niraparib administration, the median OS was 30 months (95% CI: 16.8–43.2) (Figure 1). The median PFS was 8 months (95% CI: 2.5–13.5) (Figure 2). Median study follow-up was 20 months (95% CI: 13.1–26.9). All patients included received treatment with niraparib for a median of 4.3 months (IQR: 5.9).
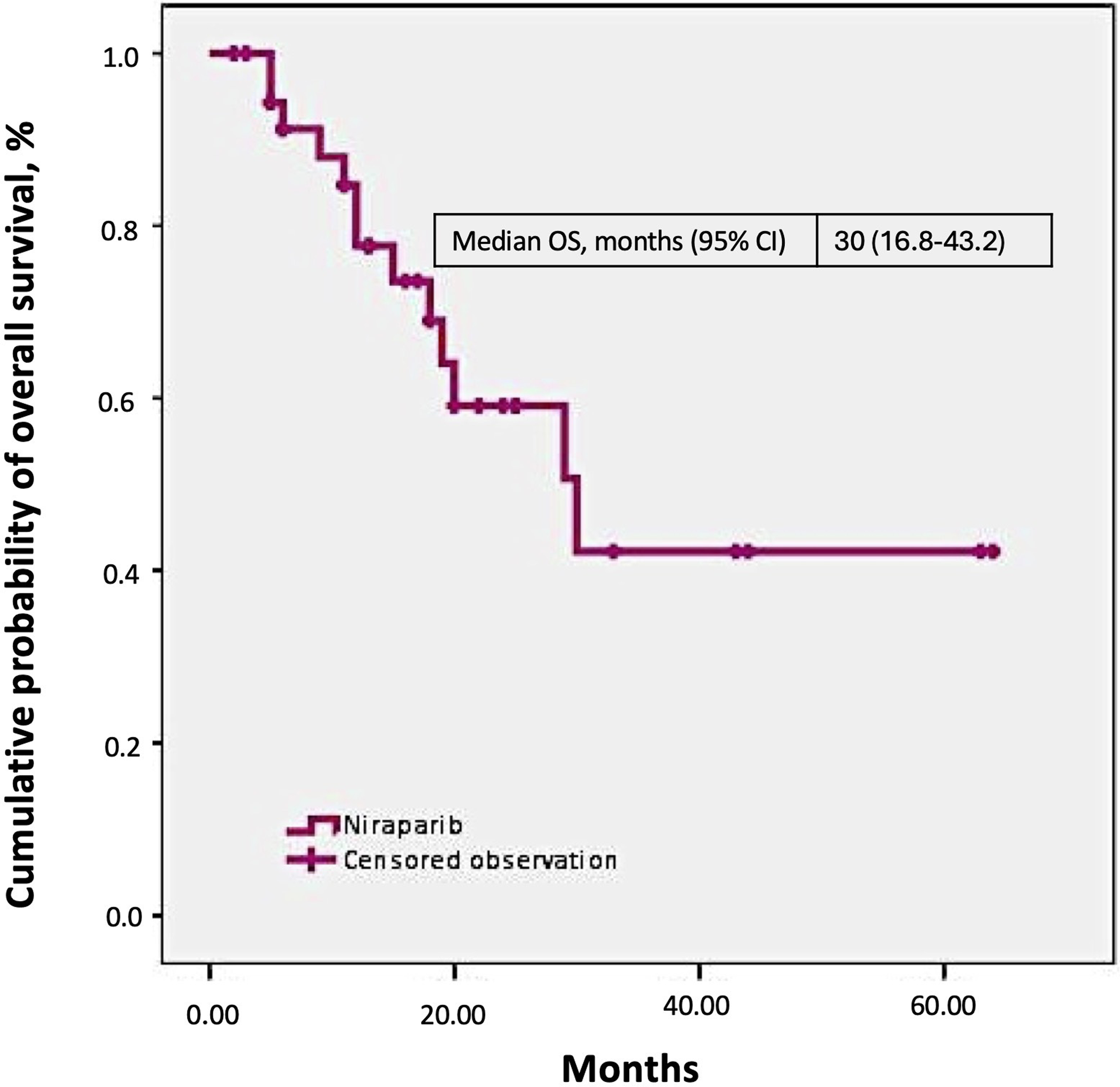
Overall survival (OS).
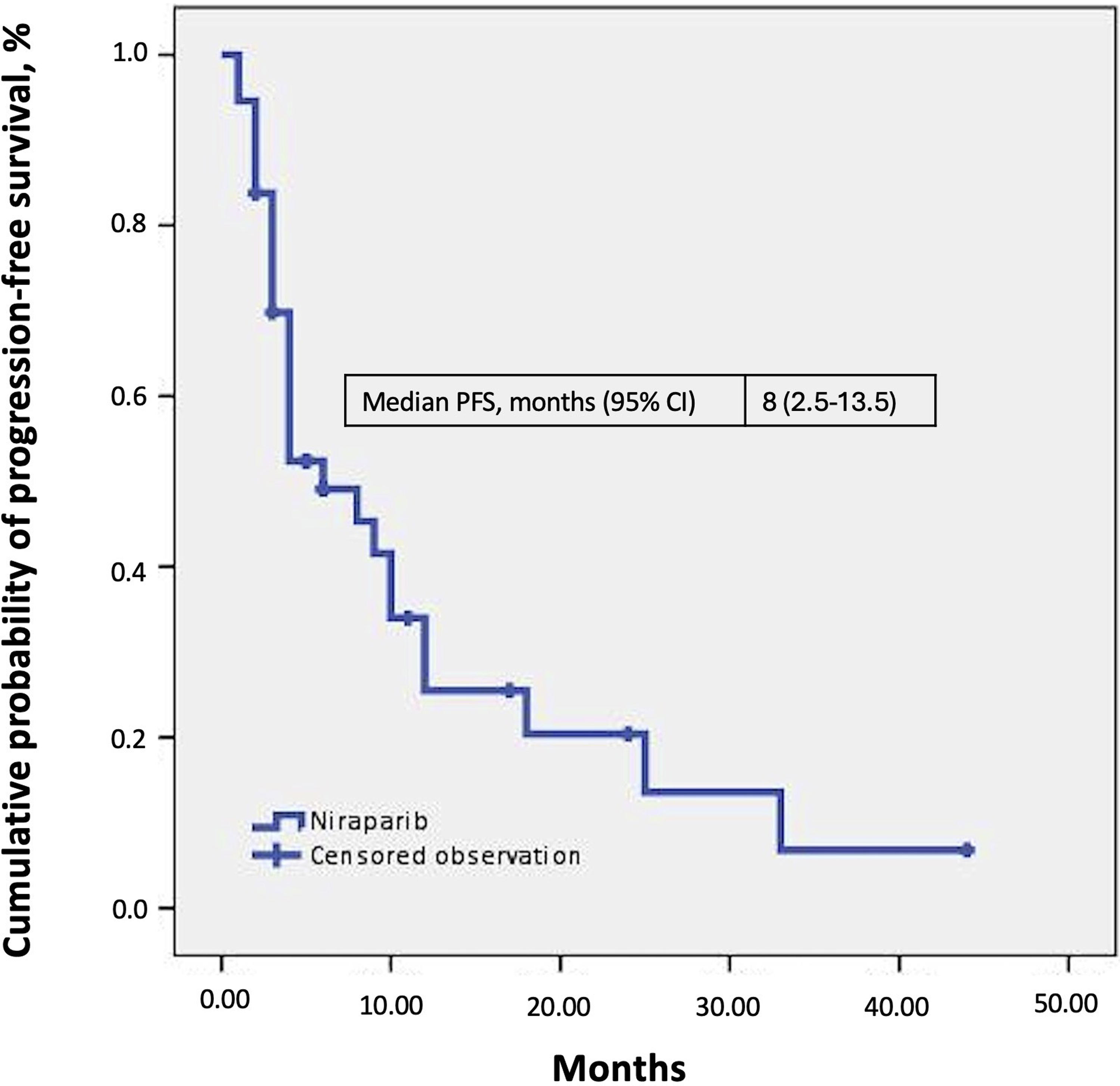
Progression-free survival (PFS).
Safety
In terms of safety, Table 3 provides details on treatment management of niraparib for toxicities control. Among the patients, 23 (69.7%) discontinued the drug, 19 patients discontinuing due to disease progression and four patients due to toxicity. Dose reduction and interruption treatment were observed in 18 (54.5%) and 19 patients (57.6%), respectively. All dose reductions and most treatment interruptions were due to adverse effects. Mainly, haematological toxicities.
Treatment management of niraparib for toxicities control.

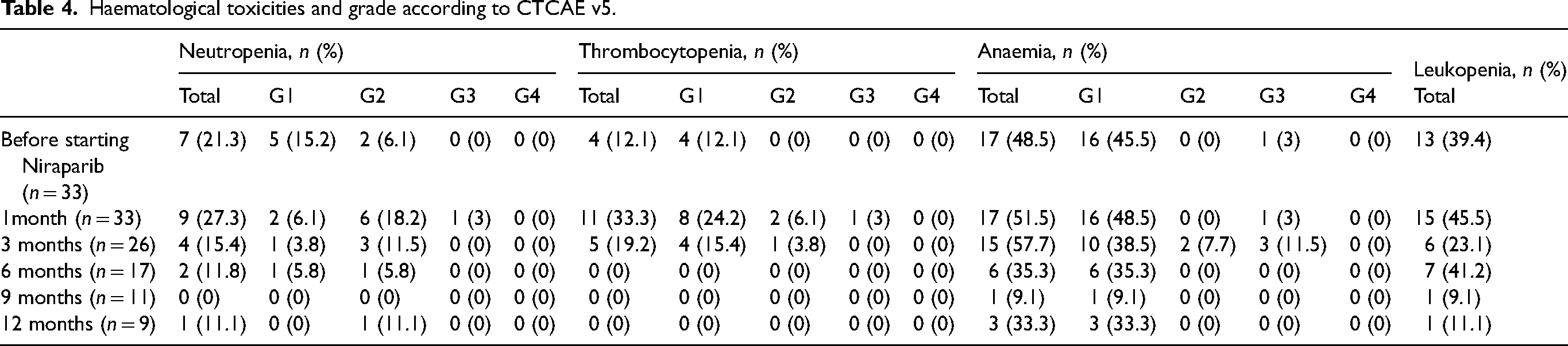
The haematological toxicities (Table 4) and the AEs reported by the patients throughout the treatment (Table 5) were more frequent at the beginning of treatment with niraparib, between first and third months. Most of the reported haematologic toxicities and/or AEs were classified as CTCAE v5 grade 1–2. Anaemia (12.1%) was the haematological toxicity that presented a higher prevalence of grade 3 toxicity (see electronic Supplementary Material 1 ‘Adverse events according to grade 3’and 2 ‘Adverse events: High blood pressure (HBP)’).
Haematological toxicities and grade according to CTCAE v5.
Grade of toxicities throughout treatment according to CTCAE v5 reported by the patient and registered in the medical record.

Blood pressure spikes during niraparib treatment were present in 14 patients, three of whom had a diagnosis of arterial hypertension before niraparib initiation. One episode of hypertensive crisis that required emergency medical attention was recorded. This happened during the first month of treatment with niraparib and the patient had no previous diagnosis of hypertension.
Discussion
This analysis shows data of niraparib in women receiving maintenance niraparib in PSROC in a mostly wild type BRCA population. Baseline characteristics of study patients are similar to those of the pivotal clinical trial 9 and other studies10,12,15 that demonstrated the utility of niraparib in PSROC; however, it differs from the cohorts of the other studies, in that it is a less polytreated population. Most of the patients had received two or fewer lines of prior treatment. This can be explained because the results of the cohort of the pivotal study 9 were published in 2016, and the cohort of the GEICO group 12 was closed in 2019. Niraparib has been available in Spain since 2019 and has been established as maintenance treatment for the PSROC after the second line in most cases.
Regarding effectiveness, the median PFS was 8 months, which is close to the results obtained in clinical trial cohorts of patients with wild-type BRCA (9.3 months in the ENGOT-OV16/NOVA4 trial; 11.1 NORA 10 trial), as well as in recently published GEICO group world data study 12 (8.6 months). The NORA study reported a higher PFS than the other studies, differences that could be explained by the variability in the patient population, since the NORA study includes a Chinese cohort of patients, and the rest of the studies were carried out in the US, Europe, Canada and Hungary. Very few studies publish OS data, and those that are published are immature data with many censored data. This is the case of the GEICO group, whose work OS (median) was of 30.7 months, but the authors justify that they are immature results because they have a lot of censored data at the time of analysis. However, despite this, it is very similar to the OS obtained in this study (30 months), even considering that a smaller cohort of patients is treated.
The median duration of follow-up, 20 months was similar between the different studies already mentioned, with a range between 15.8 months 10 and 23.1 months in the per-protocol populations of the GEICO group study. 12 Regarding OS, due to the short follow-up period of the studies, some have not reached it and others report immature data, so that the comparison of these results is inconclusive.
The dosage used in most of the population, almost 82.0%, has been based on the RADAR 14 criteria. If the data are compared with other studies9,10 with niraparib in this same indication, despite the methodological differences, the percentages of dose reductions (54.5%), treatment interruptions (57.6%) and discontinuations adverse related (12.1%) and their causes are similar. However, there are real-world data studies 15 looking at the safety of maintenance niraparib in ovarian cancer after platinum treatment, at a dose of 200 mg daily, show better safety data, reporting only 11.0% dose reductions, interruptions of 4.0% and discontinuations of 2.0%.
The AEs reported in the present study were the most common grade ≥ 3 AEs reported in the pivotal study, 9 patient-reported AEs (asthenia, vomiting, nausea and abdominal pain) and haematologic toxicities (neutropenia, thrombocytopenia, anaemia and leukopenia). Other authors have analyzed the toxicity of Niraparib focusing on the prevalence of the most reported adverse effects in pivotal studies. An example of this is the work of Gallagher, 15 comparing the three most common adverse effects, nausea, thrombocytopenia and fatigue, among the patients in his study, whose dosage was adjusted according to RADAR criteria, and those reported in the pivotal study where a fixed dose of niraparib of 300 mg every 24 h was used in all patients. The thrombocytopenia rate in Gallagher et al. was 14.0% (all grades) and 3.0% (grade 3 or 4) versus 61.0% (all grades); and 34.0% (grade 3 or 4) in the pivotal study. In the present study, the frequency of thrombocytopenia of all grades was higher than that of Gallagher et al. but less than the pivotal study; however, the prevalence of grade 3 was low (3.0%) and no patient presented grade 4.
Niraparib turned out to have a safety profile consistent with the data reported in clinical trials, as well as in other observational studies or real-life clinical trials. It should be noted that patient-reported adverse effects (nausea, vomiting, asthenia and abdominal pain) were collected from the electronic medical record, registered according to the usual clinical practice of the oncologist. This may lead to an underestimation of reported adverse effects, especially those that may be associated with a certain degree of subjectivity on the part of the oncologist or the patient, such as asthenia, nausea, vomiting or abdominal pain. In addition, the registry can be influenced by inter-individual factors that may be conditioned by the way of working and follow-up in the clinical history of each oncologist.
The main limitation of the study is that it is a retrospective observational study without randomization, in addition to reduced sample size. 16 Another limitation is that it is carried out in a single hospital centre and the results can be highly influenced by its practices.
Conclusion
Niraparib as maintenance therapy in non-BRCA PSROC constitutes a treatment option that improves PFS results in a tertiary hospital. The use of adjusted dosage of niraparib improves tolerance to treatment and does not appear to decrease efficacy. Niraparib has been shown to be a safe and easy-to-use drug.
To improve the characterization of the safety of niraparib, it would be interesting to incorporate standardized records of Patient-Reported Outcomes and measure whether these records and the measures taken improve the health outcomes of these patients.
Supplemental Material
sj-docx-1-opp-10.1177_10781552241252781 - Supplemental material for Efficacy and safety of niraparib in platinum-sensitive recurrent ovarian cancer: retrospective observational study in a tertiary hospital
Supplemental material, sj-docx-1-opp-10.1177_10781552241252781 for Efficacy and safety of niraparib in platinum-sensitive recurrent ovarian cancer: retrospective observational study in a tertiary hospital by Elena Prado-Mel, Paloma Suárez-Casillas, Lupe Rodríguez-de Francisco, Purificación Estévez-García and Rocío Jiménez-Galán in Journal of Oncology Pharmacy Practice
Footnotes
Author contributions
EPM and RJG, designed the study; PSC and LRF, collected the data; EPM and RJG, performed the analysis and interpreted the results; PSC and LRF, drafted the manuscript. All authors reviewed and approved the final version of the manuscript.
Data availability
The authors will provide the data when requested.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Informed consent statement
In accordance with the Organic Protection of Data Law 15/1999, of 13 December (OPDL), and to protect patient's confidential data, patients were identified by a corresponding numerical code. So, it was not necessary to obtain informed consent.
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.