
Abstract
Introduction
Immune checkpoint inhibitors (ICIs) are linked with various cutaneous side effects ranging from mild to life-threatening. Herein, we present a unique case of palmar-plantar erythrodysesthesia (PPE) in a patient treated with atezolizumab.
Case report
A 72-year-old white man was diagnosed with Tumor, node, metastasis (TNM) stage IIIA lung adenocarcinoma in November 2022. He underwent right lower lobectomy and mediastinal lymphadenectomy followed by adjuvant cisplatin-pemetrexed. As of May 2023, he did not have any evidence of relapse. He then started switch maintenance therapy with atezolizumab. At 24 weeks, the patient developed erythematous palmar skin lesions, followed by blisters and peeling of both palms, which were associated with swelling and pain, consistent with grade 2 PPE.
Management and outcome
Causality assessment between nivolumab and PPE via adverse drug reaction probability scale revealed a score of 5. Atezolizumab was continued, and he started on a cream consisting of trolamine and 75% water to palms twice daily. A follow-up visit 6 weeks later showed significant improvement in symptoms and appearance of palmar lesions.
Discussion
Cutaneous side effects are commonly seen with ICIs. PPE is a common dermatologic toxicity of certain tyrosine kinase inhibitors (TKIs). This effect has been previously reported with combination therapies consisting of an ICI plus a TKIs, but not with ICI monotherapy. Awareness of this potential side effect of ICIs would prevent unnecessary work-up, and lead to its prompt diagnosis and treatment.
Keywords
Introduction
Immune checkpoint inhibitors (ICIs) are extensively used in the contemporary treatment of various cancers. The vast majority of patients treated with ICIs tolerate these treatments relatively well. When they occur, ICI side effects range from mild to life-threatening.1,2,3 Below, we present a case of palmar-plantar erythrodysesthesia (PPE) occurring in a patient treated with atezolizumab for lung cancer.
Case report
A 72-year-old Caucasian man was diagnosed with lung adenocarcinoma in November 2022. He was a former heavy cigarette smoker with a 20-pack-year smoking history. A low-dose computed tomography (CT) for lung cancer screening in October 2022 identified a right lower lobe mass and a left upper lobe nodule. Other medical conditions included chronic obstructive pulmonary disease, diabetes mellitus type 2, coronary artery disease, peripheral vascular disease, hypertension, hyperlipidemia, and chronic kidney disease stage 2.
In November 2022, CT-guided lung biopsy showed lung adenocarcinoma. A positron emission tomography scan showed no distant metastatic lesions. The patient underwent a right lower lobectomy and mediastinal lymphadenectomy in January 2023. The primary right lower lobe mass measured 3.7 × 3.2 × 1.6 cm. While all margins were all clear, there was lymphatic invasion and visceral pleural invasion. 1/15 sampled lymph nodes (at station 7) showed evidence of metastatic disease. Therefore, cancer staging by Tumor, node, metastasis (TNM) was IIIA (pT2 pN2 MO).
He received four cycles of adjuvant chemotherapy with cisplatin-pemetrexed in March–May 2023. Patients tolerated the chemotherapy well with only moderate anemia related to antineoplastic therapy. A restaging CT scan did not show any evidence of relapse. He then started switch-maintenance adjuvant therapy with atezolizumab 1200 mg IV every 3 weeks in June 2023, with a plan to complete 12 months.
In December of 2023 (6 months after initiation of atezolizumab), the patient developed erythematous palm lesions, followed by multiple blisters and peeling of both palms which was associated with swelling and pain (Figure 1(a) and (b)). He did not have any history of allergy or similar symptoms in the past. He was assessed by a dermatologist and was diagnosed with grade 2 PPE.
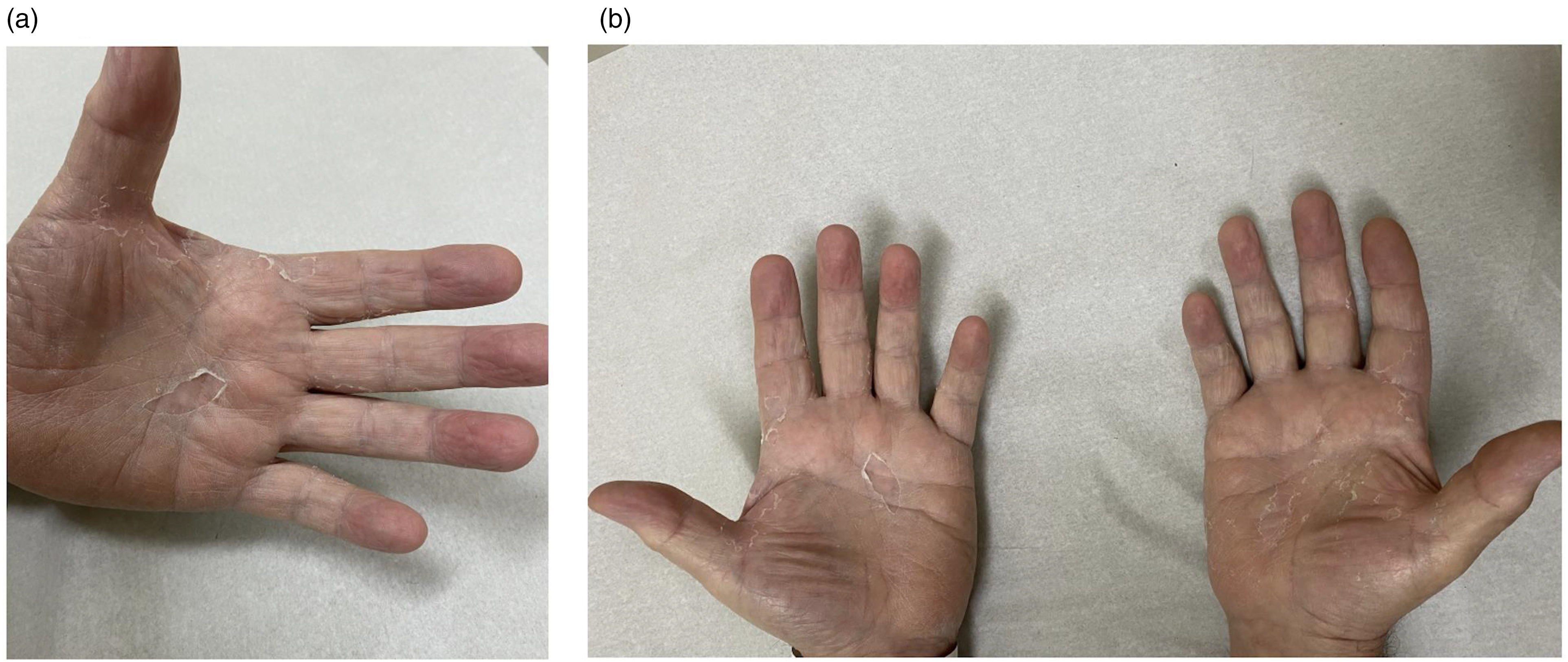
Erythematous palmar skin lesions, blisters, and peeling of the epidermis of both palms, associated with swelling and pain.
Management and outcome
Causality assessment between atezolizumab and PPE via adverse drug reaction (ADR) probability scale 4 revealed a score of 5 (Table 1). Atezolizumab was continued since his skin manifestation was localized to palms and only grade 2. The patient was started on a cream consisting of trolamine and 75% water topically every 12 h. A follow up visit 6 weeks later showed clinical and symptomatic improvement consistent with a near-complete resolution of lesions.
The Naranjo ADR probability scale questionnaire in the index patient.
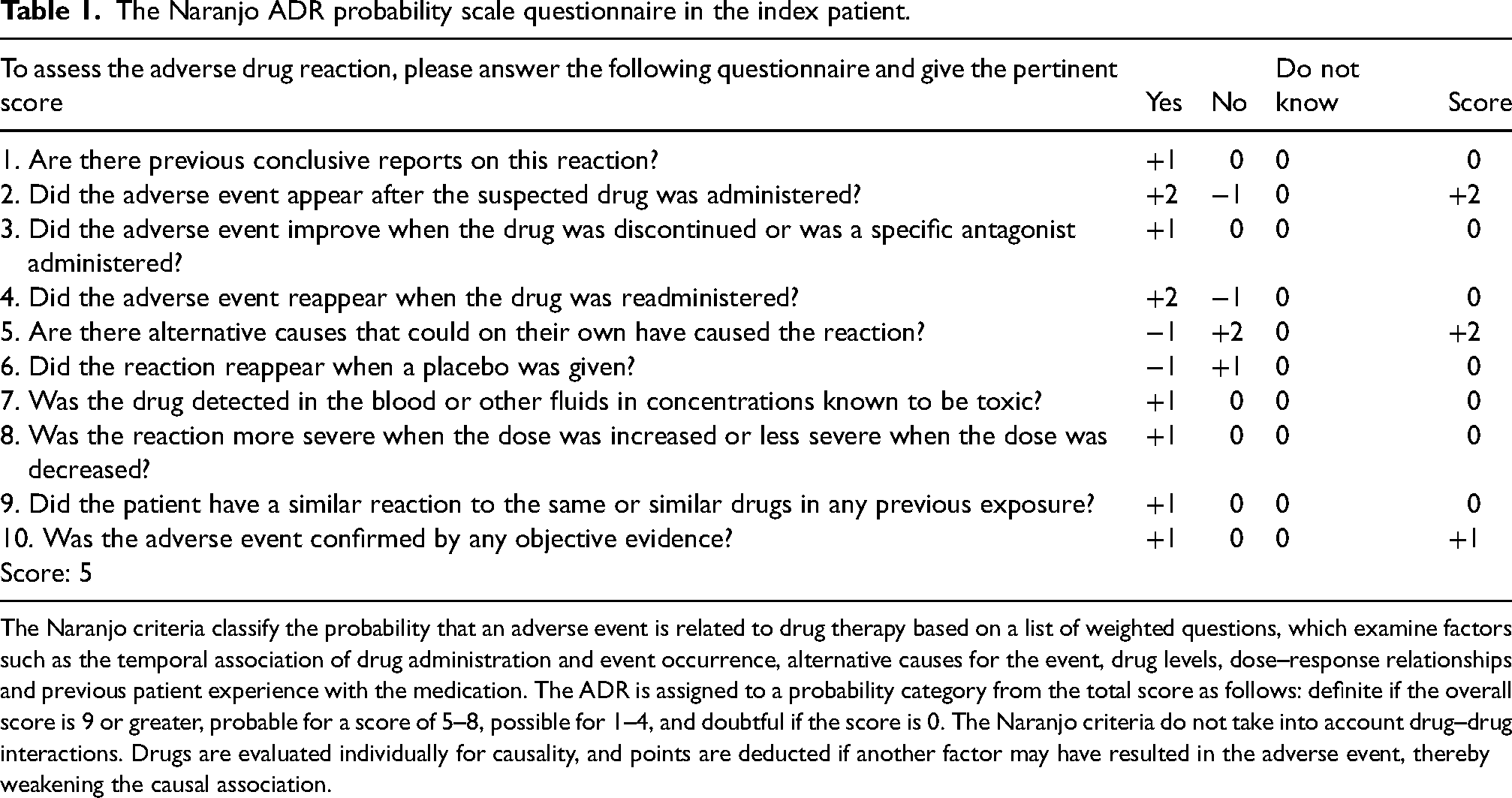
The Naranjo criteria classify the probability that an adverse event is related to drug therapy based on a list of weighted questions, which examine factors such as the temporal association of drug administration and event occurrence, alternative causes for the event, drug levels, dose–response relationships and previous patient experience with the medication. The ADR is assigned to a probability category from the total score as follows: definite if the overall score is 9 or greater, probable for a score of 5–8, possible for 1–4, and doubtful if the score is 0. The Naranjo criteria do not take into account drug–drug interactions. Drugs are evaluated individually for causality, and points are deducted if another factor may have resulted in the adverse event, thereby weakening the causal association.
Discussion
ICIs such as anti-programed cell death 1 (PD-1) and programed cell death ligand 1 (PD-L1) monoclonal antibodies are used in treatment of many cancers.1,3,5 Atezolizumab is a monoclonal antibody which binds PD-L1 (expressed by tumor cells) and prevents its interaction with PD-1 (receptors on activated T and B cells) and subsequently removes the inhibition of anti-tumor immune response. 6 It is approved for the treatment of several malignancies including lung cancer, bladder, and hepatocellular carcinoma. 7 ICIs are generally well-tolerated, however, various side effects, mostly autoimmune effects, have been reported with their use. Cutaneous manifestations are common and affect up to 50% of patients on ICIs.8,9 These reactions are usually mild and can almost always be managed without interruption or dose adjustment of ICIs. However, in rare cases, they can be serious and necessitate immediate discontinuation of ICI and administration of high dose steroids.3,7 In less than 1% of cases, Stevens-Johnson syndrome/toxic epidermal necrolysis (SJS/TEN) has been reported with the use of nivolumab, pembrolizumab (PD-1 inhibitors),3,10,11 and ipilimumab (monoclonal antibody against common T cell antigen-4).12,13
PPE (also known as hand–foot syndrome) is characterized by erythema, edema, pain, tingling, blistering, and occasional ulceration affecting the palmar aspects of the hands and/or plantar aspects of the feet.14,15 It is a common dermatologic toxicity of multikinase inhibitors such as sorafenib, cabozantinib, and sunitinib that exhibit antiangiogenic effects.15,16 PPE has been reported in up to 60% of patients treated with cabozantinib for advanced/inoperable hepatocellular carcinoma and in nearly 30% of patients treated with sorafenib for metastatic renal cell carcinoma17,18
Several clinical trials explored combinations of ICIs with tyrosine kinase inhibitors (TKIs) for the treatment of renal cell carcinoma and gastrointestinal cancers.19,20 Combination therapy with regorafenib plus nivolumab has been evaluated in gastric and colorectal cancers.5,21 Notably, Fukuoka et al. 5 reported PPE of any grades in 70% of patients treated with this combination. Also, one of the most frequent grade 3 treatment-related adverse events were papulo-erythematous skin rash (12%) and PPE (10%). Another study reported PPE as one of the main side effects of the combination therapy with cabozantinib plus nivolumab in patients with advanced renal cell carcinoma. 16 This article also revealed that a higher cabozantinib exposure (with a similar dose of nivolumab) was associated with an increased risk of PPE. Based on the results of these studies, PPE was most probably a side effect of multikinase inhibitors. Notwithstanding, PPE has not been previously reported as a side effect of monotherapy with an ICI, which makes our case unique.
In our case, causality between atezolizumab use and PPE via the Naranjo nomogram questionnaire was probable. This patient had never been exposed to any drugs associated with PPE, and the last dose of chemotherapy with cisplatin-pemetrexed was administered 7 months prior to the PPE occurrence. Atezolizumab was the only new therapy he was receiving at the time PPE developed.
Clinicians and pharmacists need to be aware of this side effect of ICIs to prevent unnecessary work-up and costs. Topical treatment with skin emollients/hydration creams and close clinical monitoring are helpful in many cases. Further research is necessary to assess the definitive causality (and severity) of PPE related to ICIs. If our hypothesis is correct, we expect more reports of PPE in the setting of ICI use in the future years.
Footnotes
Author contribution
All authors accept direct responsibility for the manuscript and fully meet the authorship criteria. CD conceived the study and obtained the patient's consent for publication. FT wrote the first draft of the manuscript. CD and FT researched the literature, reviewed, edited, and approved the final version of the manuscript.
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Informed consent
Informed consent for this publication was obtained from the patient before the submission of this case report.