
Abstract
Objective
Hormone receptor-positive (HR+), human epidermal growth factor receptor 2-negative (HER2-) breast cancer is the most common subtype. Abemaciclib, an inhibitor of cyclin-dependent kinases 4 and 6, was approved to reduce risk of recurrence in high-risk, HR+, HER2-, early breast cancer based on the monarchE trial. The most common adverse events reported in monarchE were diarrhea, neutropenia, and fatigue. Real-world tolerability data and incidence of adverse events with abemaciclib in the adjuvant setting versus the metastatic setting is lacking.
Data Sources
This is a retrospective analysis of HR+, HER2- breast cancer patients on abemaciclib from March 2018 to September 2021 at Robert H. Lurie Comprehensive Cancer Center in Chicago, Illinois. Incidence, grade of adverse events, dose reductions, and discontinuations were evaluated in patients taking abemaciclib in the adjuvant setting and the metastatic setting.
Data Summary
Of the 30 patients included in this analysis, 100% experienced an adverse event of any grade. During treatment, 12.5% treated in the adjuvant setting and 35.7% in the metastatic setting experienced grade ≥3 adverse events. Adverse events leading to discontinuation of abemaciclib occurred in 18.8% of patients in the adjuvant setting and 57.1% in the metastatic setting.
Conclusions
This data suggests abemaciclib is better tolerated in high-risk, HR+, HER2-, node-positive, early breast cancer treated in the adjuvant setting compared to the metastatic setting. Management of adverse events is crucial to help patients stay on therapy to improve clinical outcomes. Real-world tolerability of abemaciclib in both the adjuvant and metastatic settings is of importance.
Introduction
Breast cancer is the most common cancer among women and is a major cause of cancer death annually. 1 It is estimated that 297,790 new cases will occur in the United States in 2023 with an estimated 43,170 deaths. 1 Hormone receptor-positive (HR+), human epidermal growth factor receptor 2-negative (HER2-) breast cancer is the most common subtype, accounting for 68% of all breast cancers. 1 Approximately 90% of patients with breast cancer are diagnosed with early-stage disease and can develop recurrence, especially when classified as high-risk disease. Characteristics of high-risk disease include positive lymph nodes, higher grade, larger primary tumor stage, and higher Ki-67 scores. 2 Ki-67 index is a biomarker used to determine the risk of invasive disease recurrence as well as a proliferation score that is associated with worse prognosis. 3 Many patients experience disease recurrence within the first few years after diagnosis, therefore it is important to optimize adjuvant therapy to prevent early recurrences.
Early-stage treatment depends on the patient's risk of recurrence and includes a combination of surgery, radiotherapy, adjuvant or neoadjuvant chemotherapy, and endocrine therapy. 2 Chemotherapy is given to patients with lymph node-positive disease and/or those with high-risk of recurrence predicted through gene assays, such as Oncotype DX®. 3 Chemotherapy includes taxane and/or anthracycline-based regimens. 2 Endocrine therapy is indicated in all early-stage patients with detectable estrogen receptor (ER) and/or progesterone receptor (PR) expression regardless of chemotherapy use. 2 Most HR + breast cancer patients do not experience recurrence on standard adjuvant endocrine therapy, however, recurrence of disease within the first 10 years after diagnosis can occur in up to 20% of patients. 2 To further reduce this risk of recurrence, especially in high-risk HR+, HER2- breast cancer patients, more optimal adjuvant therapies are required to improve clinical outcomes.
Cyclin-dependent kinase 4 and 6 (CDK4/6) inhibitors can be used for HR + patients to optimize endocrine therapy. Abemaciclib is an oral, selective, and potent ATP-competitive inhibitor of CDK4/6 and blocks the progression of cells from G1 to S phase in the cell cycle. CDK4/6 inhibitors are given in combination with endocrine therapy for synergistic effects in the suppression of ER-mediated cell cycle progression. 4 Treatment with CDK4/6 inhibitors can suppress loss of single strand break repairs and point mutation/fusion alterations that are involved in endocrine therapy resistance mechanisms. 5
The Food and Drug Administration (FDA) approved abemaciclib on September 28, 2017 in combination with fulvestrant for disease progression following endocrine therapy in HR+, HER2-, advanced or metastatic breast cancer based upon the efficacy and safety of the MONARCH 2 study. 6 In MONARCH 2, patients on abemaciclib plus fulvestrant experienced a prolonged median progression-free survival (PFS) of 16.4 months and longer median overall survival (OS) of 46.7 months compared to patients treated with placebo plus fulvestrant who had a PFS of 9.3 months (P < 0.001) and an OS of 37.3 months (p = 0.01). 6 Subsequently, abemaciclib was studied in 2019 and approved in combination with a nonsteroidal aromatase inhibitor as initial therapy in metastatic HR+, HER2- breast cancer in the randomized, double-blinded, placebo-controlled, multicenter trial, MONARCH 3. 7 In this study, patients treated with abemaciclib benefited from a significantly prolonged median PFS of 28.2 months compared to 14.7 months in the placebo group (P < 0.0001). 7
In an effort to prevent recurrence in early-stage HR+, HER2- breast cancer patients, the monarchE trial, published in September 2020, was conducted to evaluate adjuvant abemaciclib in patients at high risk of recurrence. 8 The investigators defined high risk of recurrence as patients with ≥4 positive nodes, or 1–3 nodes plus either tumor size ≥5 cm, histologic grade 3, or central Ki-67 ≥ 20%. 8 MonarchE studied the addition of 2 years of abemaciclib treatment to standard endocrine therapy in patients who completed definitive locoregional therapy (with or without neoadjuvant or adjuvant chemotherapy). 8 The addition of abemaciclib in this trial demonstrated a 2-year invasive disease-free survival (IDFS) of 92.2% compared to 88.7% (P = 0.01) in endocrine therapy alone. 8 Abemaciclib also improved distance relapse-free survival (DRFS) with a 2-year DRFS rate of 93.6% compared to 90.3% with just endocrine therapy. These results led to the FDA approval of abemaciclib for adjuvant endocrine therapy on October 12, 2021 for high-risk patients. Abemaciclib is currently the only CDK4/6 inhibitor FDA approved in the adjuvant setting.
Although initial results from the monarchE trial showed a benefit in IDFS for all patients on abemaciclib, there were only positive OS results for patients with a Ki-67 score ≥20%. In the intention-to-treat population (patients with Ki-67 scores <20% but with other high risk criteria), the hazard ratio for OS was greater than 1, thus the FDA chose to initially approve abemaciclib only for high-risk patients with a Ki-67 score ≥20%. 9 However, upon additional follow-up of these monarchE patients at a median of 42 months after initiation of abemaciclib, there was a benefit in both OS and IDFS results for all abemaciclib patients regardless of Ki-67 score. 10 Therefore on March 3, 2023 the FDA approval removed the requirement of a Ki-67 score ≥20% via companion diagnostics.
After the publication of monarchE and subsequent FDA approval, more patients are now receiving abemaciclib in clinical practice and are requiring toxicity management. The most common adverse events reported in MONARCH 2, MONARCH 3, and monarchE were diarrhea, neutropenia, fatigue, nausea, vomiting, abdominal pain, decreased appetite, alanine aminotransferase/aspartate aminotransferase (ALT/AST) increases, and anemia.6–8 Diarrhea was the most frequent non-hematologic side effect occurring in about 80% of patients, generally within the first 4 weeks after starting abemaciclib.6–8 Other infrequent (<5%) but relevant adverse events with abemaciclib in the studies included venous thromboembolism (VTE) and interstitial lung disease (ILD)/pneumonitis.6–8
Although the Monarch trials give insight into abemaciclib adverse events, real-world data characterizing the tolerability, rates of discontinuations, and incidence of adverse events in different treatment settings is lacking. The ability of patients to tolerate abemaciclib in different stages of their cancer, is still of great concern. The objective of this study is to evaluate the tolerability and other real-world differences of abemaciclib in patients naïve to a CDK4/6 inhibitor and in combination with endocrine therapy in the adjuvant setting and the metastatic setting for HR+, HER2- breast cancer patients treated at Robert H. Lurie Comprehensive Cancer Center of Northwestern University in Chicago, Illinois.
Methods
Study design
We conducted a single-center, retrospective, observational, cohort study assessing tolerability and adverse effects of abemaciclib in patients with HR+, HER2- breast cancer in the adjuvant setting at high-risk of recurrence compared to abemaciclib in the metastatic setting. Patients were identified if treated from March 1, 2018 to September 23, 2021 at the breast oncology clinic at Robert H. Lurie Comprehensive Cancer Center of Northwestern University in Chicago, Illinois. The study was reviewed and approved by Northwestern Institutional Review Board (IRB) [STU00215898].
Study population
This study analyzed patients with early, high-risk and metastatic HR+, HER2- breast cancer taking first line abemaciclib at a starting dose of 150 mg by mouth twice daily. High-risk early breast cancer patients were defined, per the monarchE study, as ≥4 positive pathologic axillary lymph nodes or 1 to 3 positive axillary lymph nodes and at least 1 of the following: tumor size ≥5 cm, histologic grade 3, or centrally assessed Ki-67 ≥ 20%. We included all patients between the ages of 18 and 89 years that had a prescription for abemaciclib used in combination with endocrine therapy. Exclusion criteria included, patients receiving care or prescriptions for abemaciclib from a physician outside of Robert H. Lurie Comprehensive Cancer Center, those that were receiving abemaciclib as monotherapy, those that received abemaciclib after a different CDK4/6 inhibitor in the metastatic setting, patients taking any form of hormone replacement therapy or hormonal birth control, and vulnerable patient populations including those <18 years of age, prisoners, and cognitively impaired. Patients on monotherapy abemaciclib and those who were on other CDK4/6 inhibitors prior to abemciclib were excluded to ensure similar populations were evaluated in both settings. Only patients naïve to CDK4/6 inhibitors and those using abemaciclib in combination with endocrine therapy were included to prevent confounding results to abemaciclib tolerance and to follow FDA approvals in each treatment setting.
Data collection
We conducted a retrospective chart review using the electronic medical record. REDCap was used to collect data of 30 patients prescribed abemaciclib from March 1, 2018 to September 23, 2021. Treatment with abemaciclib was determined through outpatient prescription records in the electronic medical record. Adjuvant treatment versus metastatic treatment was determined via staging and physician notes in the electronic medical record. Patients were assessed from start date of abemaciclib for labs, adverse effects, treatment holds, dose adjustments and treatment discontinuations. Laboratory values including complete blood count and liver enzymes were collected for patients in each group ideally at baseline, every 2 weeks for the first 2 months, and then periodically thereafter for a total of 6 collections when data was available in the electronic medical record. Adverse effects were collected from the electronic medical record via office visit notes with patients’ primary breast oncologist and advanced provider practitioners, electronic medical record messages between patient and provider, and telephone encounters. These adverse events were graded based on common terminology criteria for adverse events (CTCAE) version 5.0. Tolerability outcomes collected included incidence of grade 3–4 adverse events, dose reductions/ holds, discontinuations, supportive care for adverse events, and time to adverse events.
Results
Patients
A total of 85 patients with a prescription for abemaciclib were screened from March 1, 2018 to September 23, 2021. Of these patients, 47 were excluded due to receiving abemaciclib second line in the metastatic setting after progression on an alternative CDK4/6 inhibitor. Additionally, 8 patients were excluded either due to pathology revealing HER + disease, never initiating abemaciclib, or being treated for local recurrence. The final study population consisted of 30 women eligible for inclusion and evaluation.
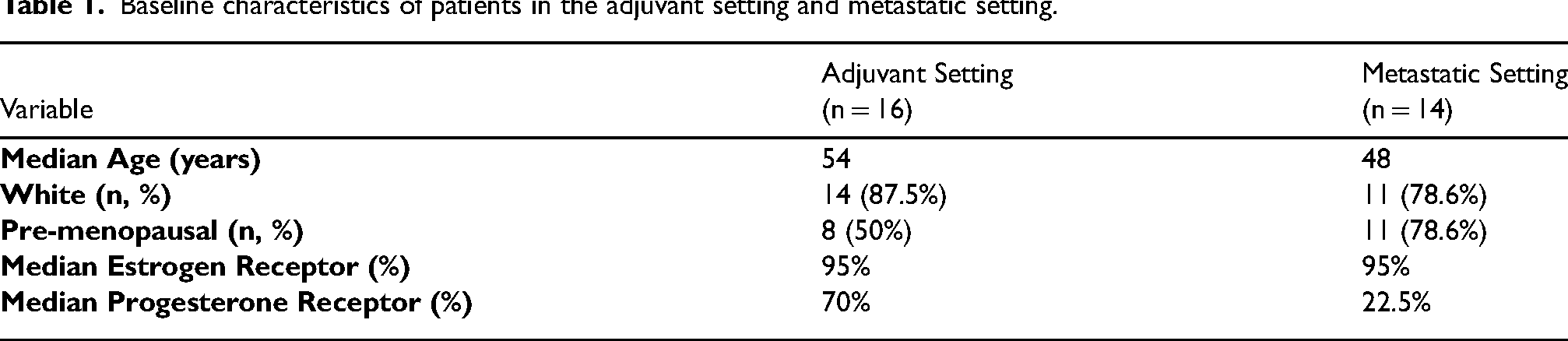
Thirty patients were included in the analysis: 16 patients receiving abemaciclib in the adjuvant setting and 14 patients receiving it in the metastatic setting. Baseline characteristics were similar between the two groups. In the adjuvant setting, the median age was 54 years old compared to 48 years old in the metastatic setting. The majority of patients in each setting were white. Pre-menopausal status at baseline was 50% in the adjuvant setting and 78.6% in the metastatic setting. Median ER expression was 95% in both settings and median PR expression was 70% in the adjuvant setting and 22.5% in the metastatic setting. A summary of patient characteristics can be found in Table 1.
Baseline characteristics of patients in the adjuvant setting and metastatic setting.
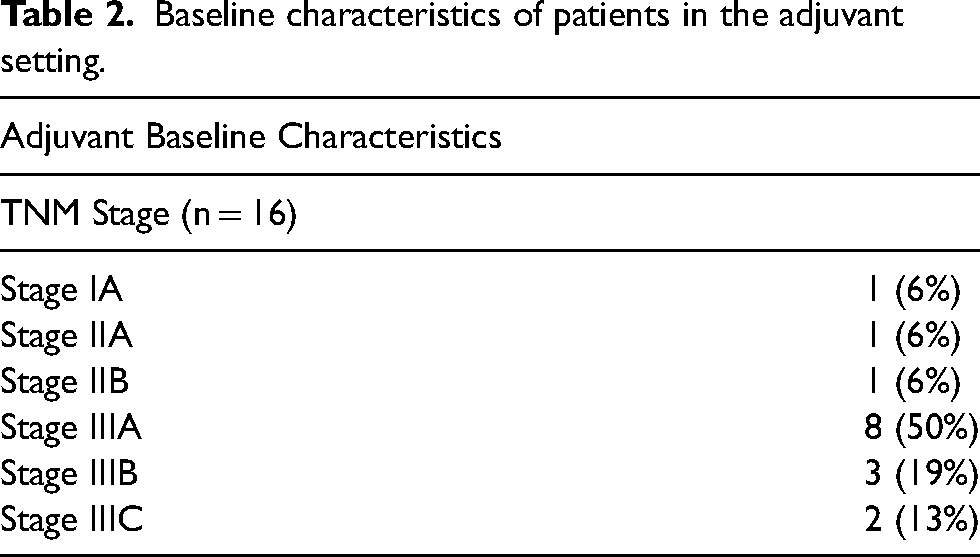
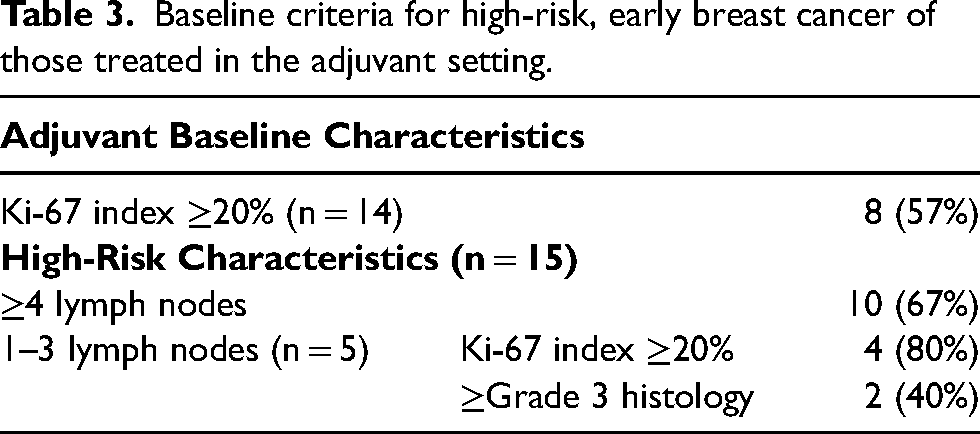
Patients in the adjuvant setting are classified by stage in Table 2 with most patients as stage IIIA, stage IIIB, and stage IIIC at 50%, 19%, and 13% respectively. Most patients (67%) in the adjuvant setting met criteria for high-risk, early breast cancer due to 4 or more positive lymph nodes. More than half of patients (57%) in the adjuvant setting had a Ki-67 index score of ≥20%. Full high-risk characteristics are demonstrated within Table 3.
Baseline characteristics of patients in the adjuvant setting.
Baseline criteria for high-risk, early breast cancer of those treated in the adjuvant setting.
Some patients had a significant delay prior to starting abemaciclib in the adjuvant setting, mostly due to recovery time after chemotherapy and/or radiation. For those receiving adjuvant abemaciclib, the median time from the completion of chemotherapy to starting abemaciclib was 206.5 days with a range of 92–465 days. There were 5 patients in the adjuvant setting that had a median time from end of chemotherapy to start of abemaciclib of greater than 250 days. Radiation was also given to 15 out of 16 patients in the adjuvant setting. The median time from completion of radiation to abemaciclib start date was 96 days with a range of 20–186 days.
Adverse events
In each setting (adjuvant vs metastatic), 100% of all patients experienced an adverse event of any grade as displayed in Table 4. Throughout treatment, 2 patients (12.5%) treated in the adjuvant setting and 5 patients (35.7%) in the metastatic setting experienced grade 3 or 4 adverse events. Any grade diarrhea was the most common adverse event occurring in more than 80% in both settings. Median time to diarrhea was 10.5 days for patients treated in the adjuvant setting and 11 days in the metastatic setting. In the adjuvant setting, 4 patients (25%) had abemaciclib held due to diarrhea for a median of 6 days. In the metastatic setting, only 1 patient had abemaciclib held due to diarrhea for 5 days. Many patients required loperamide for diarrhea, 15 patients (93.7%) in the adjuvant setting and 12 patients (85.7%) in the metastatic setting. The second most frequent adverse event was any grade nausea with 7 patients (43.8%) in the adjuvant setting and 7 patients (50%) in the metastatic setting. Fatigue was also common occurring in 31.3% of patients in the adjuvant setting and 35.7% in the metastatic setting.
Adverse events of patients treated in the adjuvant setting and metastatic setting.
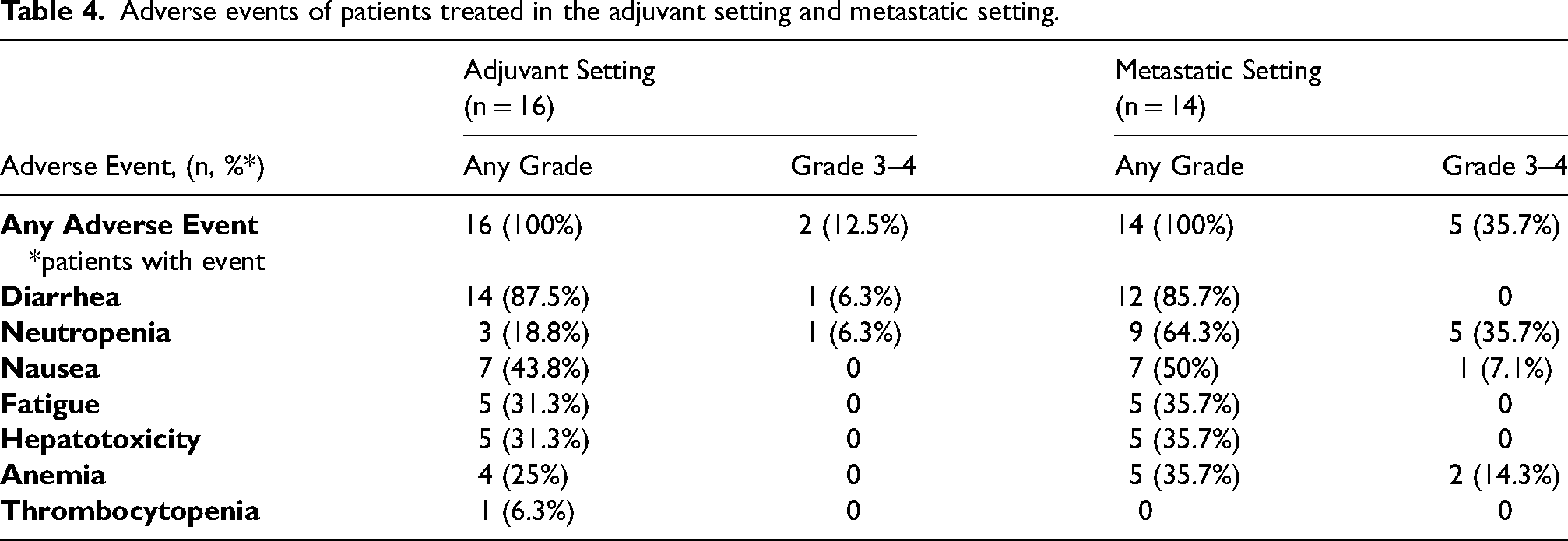
Hematologic toxicities were higher in the metastatic setting than the adjuvant setting with 5 patients (35.7%) and 1 patient (6.3%) developing grade 3–4 neutropenia respectively. A total of 2 patients, 1 patient in each setting, required growth factor support for neutropenia with filgrastim. In the adjuvant setting, 25% of patients experienced any grade anemia (0% grade 3–4) and 35.7% (14.3% grade 3–4) in the metastatic setting. Hepatotoxicity was slightly higher in the metastatic setting with 5 patients (35.7%) experiencing elevated liver enzymes versus 5 patients (31.3%) in the adjuvant setting (Table 4), but no grade 3–4 reactions occurred in either group. There was a median time to onset of elevated liver enzymes of 14 days in the adjuvant setting and 19.5 days in the metastatic setting. There was no treatment associated ILD or VTE events observed in either group. Overall, there were more grade 3–4 adverse events in the metastatic setting for neutropenia, anemia, and nausea compared to patients treated in the adjuvant setting.
Dose modifications
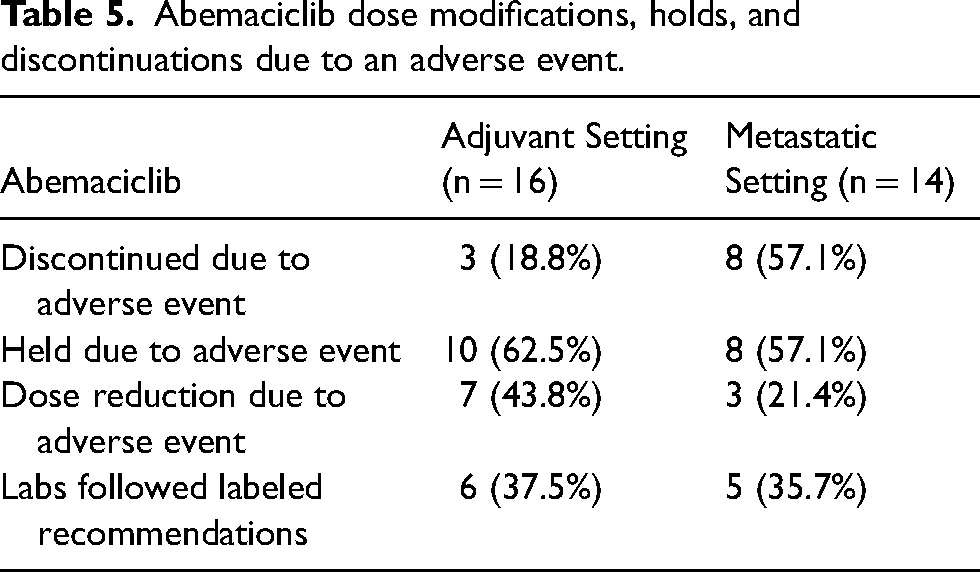
Table 5 displays all dose modifications of abemaciclib in the adjuvant and metastatic setting. The percentage of patients that had to discontinue abemaciclib due to an adverse event was 18.8% in the adjuvant setting and 57.1% in the metastatic setting. Dose holds due to adverse events were required for 62.5% of patients in the adjuvant setting (median hold time of 8 days) versus 57.1% of patients in the metastatic setting (median hold time of 6 days). Median time to dose discontinuation due to an adverse event was 154 days in the adjuvant setting and 122 days in the metastatic setting. The percentage of patients that required a dose reduction due to toxicity was 43.8% in the adjuvant setting and 21.4% in the metastatic setting. Median time to dose reductions of abemaciclib was 29 days for patients in the adjuvant setting and 107 days for patients in the metastatic setting. The timing of follow-up laboratory monitoring recommended in the abemaciclib package insert was not followed diligently in either setting with a 37.5% compliance rate in the adjuvant setting and 35.7% compliance rate in the metastatic setting.
Abemaciclib dose modifications, holds, and discontinuations due to an adverse event.
Discussion & conclusions
To our knowledge, this is the first analysis to characterize the tolerability and real-world differences of abemaciclib utilization in both the high-risk adjuvant setting and the metastatic setting for HR+, HER2- breast cancer. This single-site, retrospective analysis found that abemaciclib was better tolerated in the adjuvant setting as there was a lower incidence of grade 3–4 adverse events. Higher grade 3–4 adverse events in the metastatic setting were mainly due to hematologic effects (neutropenia and anemia), but there was also a higher rate of any grade nausea, fatigue, and hepatoxicity. This study found no new safety concerns and supports data from MONARCH 3 and monarchE, in which the main adverse events consisted of diarrhea and neutropenia. Interestingly, there was no difference in the rate of diarrhea between the two groups but as previously reported the diarrhea occurred early in the treatment course and was responsive to loperamide treatment. In our analysis the rate of any grade neutropenia in adjuvant patients was low, which could be attributed to the long treatment break between chemotherapy and radiation before abemaciclib initiation in some patients but is likely multi-factorial. The delayed start of abemaciclib in the adjuvant group could have improved overall tolerability by allowing time for patients to recover after chemotherapy and/or radiation.
In the metastatic setting, there was also a higher rate of discontinuations due to adverse events which could be directly correlated to the higher rate of grade 3–4 adverse events in these patients. The difference in the discontinuation rate could be attributed to abemaciclib being the only treatment option in the high-risk adjuvant setting compared to the metastatic setting, in which there are more treatment options including additional CDK4/6 inhibitors, other targeted therapies, and chemotherapy. While there were more dose reductions and treatment holds in the adjuvant setting, this could be contributed to provider strategies to improve tolerance and avoid discontinuations prior to the recommended 2-year treatment period.
The discontinuation rate of abemaciclib due to adverse events in the adjuvant setting in this analysis was 18%. A recent abstract presented by Tolaney and colleagues described factors that were associated with a greater risk of discontinuation of abemaciclib in the monarchE patients. 11 This exploratory analysis found that patients 65 years of age and older, those with 1–3 positive nodes, and/or those with 4 or more pre-existing comorbidities had a higher risk of discontinuation. 11 The analysis also demonstrated a majority of discontinuations of abemaciclib occurred within the first 6 months of treatment highlighting the need for early control of adverse events due to abemaciclib. 11 While our study did not specifically look at patient factors associated with discontinuation, the aforementioned abstract may explain some of the reasons for treatment discontinuation in our patients.
Limitations of this study include its retrospective nature which cannot control for adverse events due to other causes. Although there is a small sample size in this analysis, it is still clinically relevant to help practitioners describe the tolerability of abemaciclib in their different patient populations. Additionally, adverse events were extracted from the electronic medical record from pharmacist and physician notes and these definitions did not always meet prespecified objective criteria. When provider documentation was lacking, assumptions were made based on lab findings or note context.
For patients with early, high-risk HR+, HER2- breast cancer, literature has demonstrated that abemaciclib has decreased the risk of recurrence. Patients may have suboptimal outcomes if abemaciclib is discontinued prior to the adjuvant treatment period of 2 years, therefore, it is important to characterize tolerability concerns of abemaciclib in these patients. Characterizing these patterns in dose reductions, holds and discontinuations as described above can help physicians better manage adverse events to abemaciclib through brief dose holds to allow for adverse events to improve. This study also helps illustrate the management of toxicities with dose adjustments and medication holds, which in turn may reduce medication discontinuations. Abemaciclib in the metastatic setting has been standard of care for some time and it is important to characterize reasons for treatment discontinuation other than progression. While this study was just the beginning to understanding these patients and abemaciclib, hopefully longer follow up and additional studies on abemaciclib tolerability will allow for optimal management of this medication for HR+, HER2- breast cancer patients.
Footnotes
Acknowledgements
The authors would like to thank the Department of Pharmacy at Northwestern Memorial Hospital and the Robert H. Lurie Comprehensive Cancer Center, which are supported by the Northwestern University Institutional Review Board.
Author contributions
EA and AS conceived the study and TD, EA, and AS researched literature. TD participated in protocol development, data collection, data analysis, interpretation of data and gaining ethical approval through Northwestern University Institutional Review Board. EA and AS participated in the research concept, patient selection, and interpretation of data. TD wrote the first draft of the manuscript. All authors reviewed and edited the manuscript and EA and AS approved the final version of the manuscript.
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.