
Abstract
Introduction
Patients with hematologic malignancies often receive multiple medications, leading to potential drug-drug interactions (DDIs). Identifying and managing these DDIs is crucial for ensuring patient safety and effective care. This study aimed to identify and describe DDIs and associated factors in hematologic malignancy patients.
Methods
This prospective interventional study was conducted at a referral center and included hospitalized patients with hematologic malignancies who were receiving at least four concurrent medications. A pharmacist initially compiled a comprehensive list of all medications through patient interviews and medication reviews, and subsequently, identified and categorized potential DDIs using the Lexi-interact® and Micromedex® databases. The clinical pharmacist then evaluated the clinical impact of the identified DDIs in every individual patient and provided appropriate interventions to resolve them.
Results
A total of 200 patients met the inclusion criteria for the study, with 1281 DDIs identified across 337 distinct types. The majority of identified DDIs exhibited major severity (52.1%) and pharmacokinetic mechanisms (50.3%), with an unspecified onset (79.4%) and fair evidence (67%). Of the identified DDIs, 81.1% were considered clinically significant, prompting 1059 pharmacotherapy interventions by the clinical pharmacist. Additionally, a significant relationship was observed between the number of drugs used during hospitalization and the occurrence of DDIs (P < 0.001, r = 0.633).
Conclusion
DDIs are highly prevalent among hospitalized patients with hematologic malignancies, with their occurrence increasing alongside the number of medications administrated. The intervention of a clinical pharmacist is crucial to evaluate the clinical impact of these DDIs and implement effective interventions for their management.
Introduction
Every year, millions of people experience adverse medication events, accounting for up to 5% of hospital admissions. While some adverse drug reactions are unforeseeable, many others are preventable. Drug-drug interactions (DDI) represent a particularly serious type of adverse drug event, often anticipated based on prior reports, clinical research, and pharmacologic knowledge. 1 DDIs are preventable medication errors which can lead to severe or even fatal adverse effects, defined as the occurrence of a dangerous combination of medications in an individual patient. 2 They significantly contribute to morbidity and mortality worldwide, leading to adverse clinical events, reduced therapeutic effects, increased drug toxicity, as well as compromised treatment outcomes and adherence.3,4
Cancer patients are particularly vulnerable to DDIs due to the multiple medications they often take for cancer treatment and comorbidities. 5 Although numerous studies have evaluated DDIs in general populations and thoroughly discussed the associated risks to patient safety.6–8 not enough attention has been given to this in cancer patients, especially those with hematological malignancies. In comparison with solid tumors, patients with hematologic malignancies typically undergo more intensive and complex treatments, resulting in prolonged hospitalization, primarily due to complications such as cytopenia. Thus, they are at a higher risk for drug-related problems (DRPs), including DDIs. 9 These issues can potentially escalate morbidity rates, prolong hospital stays, and increase mortality in this population of patients. 10
Clinical pharmacists play a crucial role to identify and resolve DRPs, thereby optimizing drug efficacy and reducing side effects. They achieve this by providing essential information on the rational use and administration of drugs, as well as potential interactions. 11 However, due to a lack of robust professional relationships among medical oncologists/hematologists, clinical pharmacists, and general practitioners, many potential DDIs go unnoticed or fail to receive proper intervention.12,13 The present study aimed to identify and describe DDIs among hospitalized patients with hematologic malignancy and assess the pharmacotherapy intervention by the clinical pharmacist. A secondary objective was to explore potential factors associated with DDIs.
Methods
Study design and setting
This prospective interventional research was conducted at the Research Institute for Oncology, Hematology, and Cell Therapy (RIOHCT), a referral center in Iran, affiliated to Tehran University of Medical Sciences (TUMS), during a 6-month period from February 2023 and late August 2023. The study protocol received approval from the Ethics Committee for Human Research (IR.TUMS.TIPS.REC.1401.089).
Patient population and data collection
The study included hospitalized adult patients diagnosed with any hematologic malignancy who were receiving at least four medications. Hematologic malignancies refer to a group of neoplastic disorders affecting lymphoid and hematopoietic tissues. 14 Exclusion criteria comprised a language barrier and nonmalignant conditions.
A pharmacist conducted structured interviews with patients to obtain the best possible medication history (BPMH), and collected data on demographic characteristics plus medical history. Subsequently, the patient's current medications were recorded from the physician's orders and the nursing drug Kardex.
Identification of DDIs
After compiling a comprehensive list of medications, potential DDIs were detected using the Lexi-interact® and Micromedex® DDI checker databases. Where there was divergence in the severity rating, the higher rating was considered. Each DDI found in either or both databases were counted once in the analysis.
Categorization of DDIs
DDIs were further analyzed and categorized based on their severity, mechanism, onset, and level of evidence.
Severity: The severity rating scale was based on the categories provided by the Micromedex® and Lexi-interact® databases.
Contraindicated: Co-administration of drugs is prohibited due to severe adverse outcomes. Major: Pose the risk of life-threatening effects or significant alteration of treatment efficacy. Moderate: May worsen the patient's condition or impact the effectiveness of the drugs involved. Minor: Have negligible clinical impact and do not necessitate significant intervention. Excellent: Supported by multiple randomized clinical trials (RCTs) or a combination of an RCT and numerous case reports. Good: Characterized by a single RCT and fewer than two case reports. Fair: This may be based on more than two case reports, a theoretical interaction based on known pharmacology, or less than two case reports supplemented with other data. Poor: Evidence comprises fewer than two case reports without additional supporting data. Rapid: Occurs within 24 h of drug co-administration, necessitating swift identification and management. Delayed: Emerge after 24 h, requiring ongoing vigilance throughout the treatment period. Unspecified: The timing is not clearly defined or categorized into rapid or delayed. Pharmacokinetic: Changes in drug absorption, distribution, metabolism, or excretion. Pharmacodynamic: Enhanced or diminished therapeutic effects, as well as adverse effects. Unknown: The specific underlying mechanism is not currently understood or identified.
Evidence:
Onset:
Mechanism:
Assessment of clinical impact of DDIs and clinical pharmacist interventions
A clinical pharmacist initially evaluated the identified DDIs to assess their clinical impact and determine the need for pharmacotherapy intervention for each individual patient. If intervention was required, advice on management was communicated to the attending hemato-oncologist.
Statistical analysis
The collected data were analyzed using IBM SPSS Statistics software, version 26. Descriptive statistics summarized the demographic and clinical characteristics of the patient population, including means ± standard deviations (SD) for continuous variables, as well as frequencies and percentages for categorical variables. Spearman's correlation test was used for comprehensive analysis, controlling for potential confounding variables such as age, gender, number of drugs used during hospitalization, and type of hematologic malignancy. The level of statistical significance was set at P < 0.05.
Results
Patient's characteristics
A total of 281 patients were initially evaluated for participation. Of these, 81 patients did not meet the inclusion criteria, leaving 200 patients to be included in this study. The average age of the studied patients was 38.9 years (range 18 to 73 years), with 60.5% being male. The majority of patients (39%) had diploma-level education. Non-M3 acute myeloid leukemia (AML) was the most common hematologic malignancy (52.5%) among the studied patients. More than half of patients (53.5%) had at least one comorbidity, and 71% had received at least one medication prior to hospitalization, with an average of 1 home medication per patient. The majority of patients (82%) received more than 10 medications during their hospital stay, with an average of 15 hospital medications per patient. Table 1 summarizes the demographics and characteristics of the studied patients.
Characteristics of studied patients (N = 200).
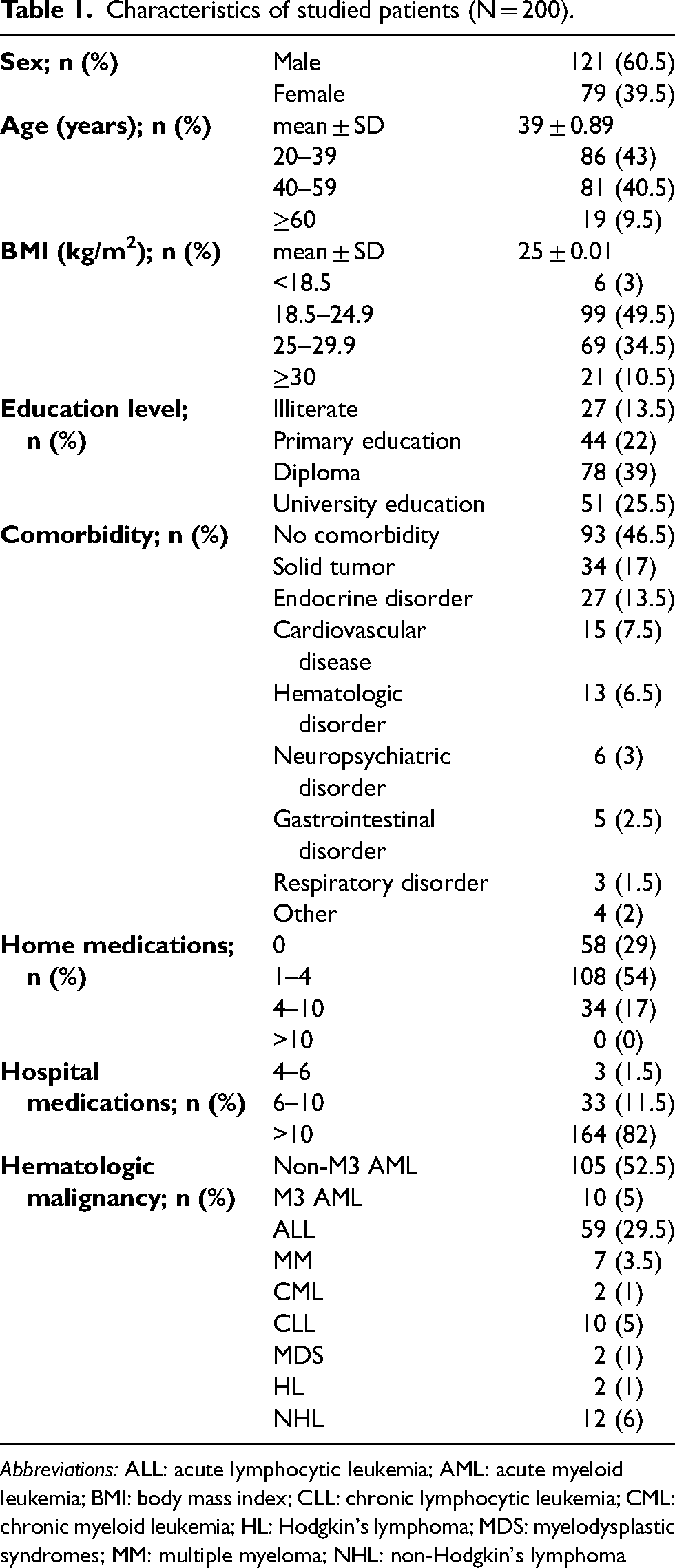
Abbreviations: ALL: acute lymphocytic leukemia; AML: acute myeloid leukemia; BMI: body mass index; CLL: chronic lymphocytic leukemia; CML: chronic myeloid leukemia; HL: Hodgkin's lymphoma; MDS: myelodysplastic syndromes; MM: multiple myeloma; NHL: non-Hodgkin's lymphoma
Identified DDIs
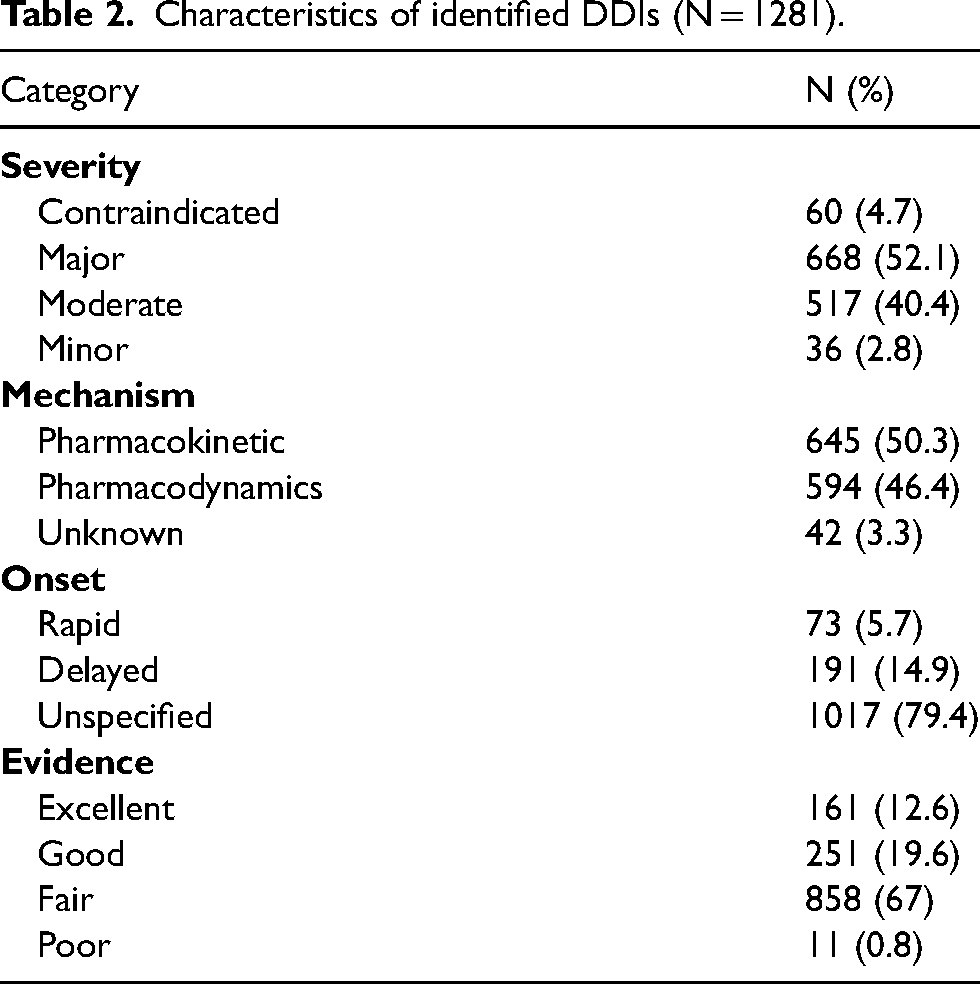
In total, 1281 potential DDIs across 337 distinct types were identified and subsequently evaluated for the necessity of clinical interventions. The prevalence of DDIs observed in this study was 92%. Among the 1281 identified DDIs, 147 involved at least one anticancer agent, representing an 11.5% prevalence of interactions involving oncologic drugs. On average patients experienced 6.4 DDIs, with the highest number recorded at 26 per patient. Notably, 8% of studied patients did not exhibit any DDIs. Among the medications, fluconazole (26%), ciprofloxacin (18%), voriconazole (15.5%), dexamethasone (14%), and aprepitant (11.5%) were found to be responsible for the majority of interactions. The majority of identified DDIs had major severity (52.1%) and pharmacokinetic mechanisms (50.3%), with an unspecified onset (79.4%) and fair evidence (67%). A notable discrepancy was observed in the classification of interaction severity between the Lexi-Interact® and Micromedex® databases. Out of the 1281 identified DDIs, 990 (77.3%) exhibited divergent severity ratings between the two tools. Further details on the characteristics of identified DDIs in studied patients are reported in Table 2.
Characteristics of identified DDIs (N = 1281).
Clinical impact of DDIs and pharmacotherapy interventions
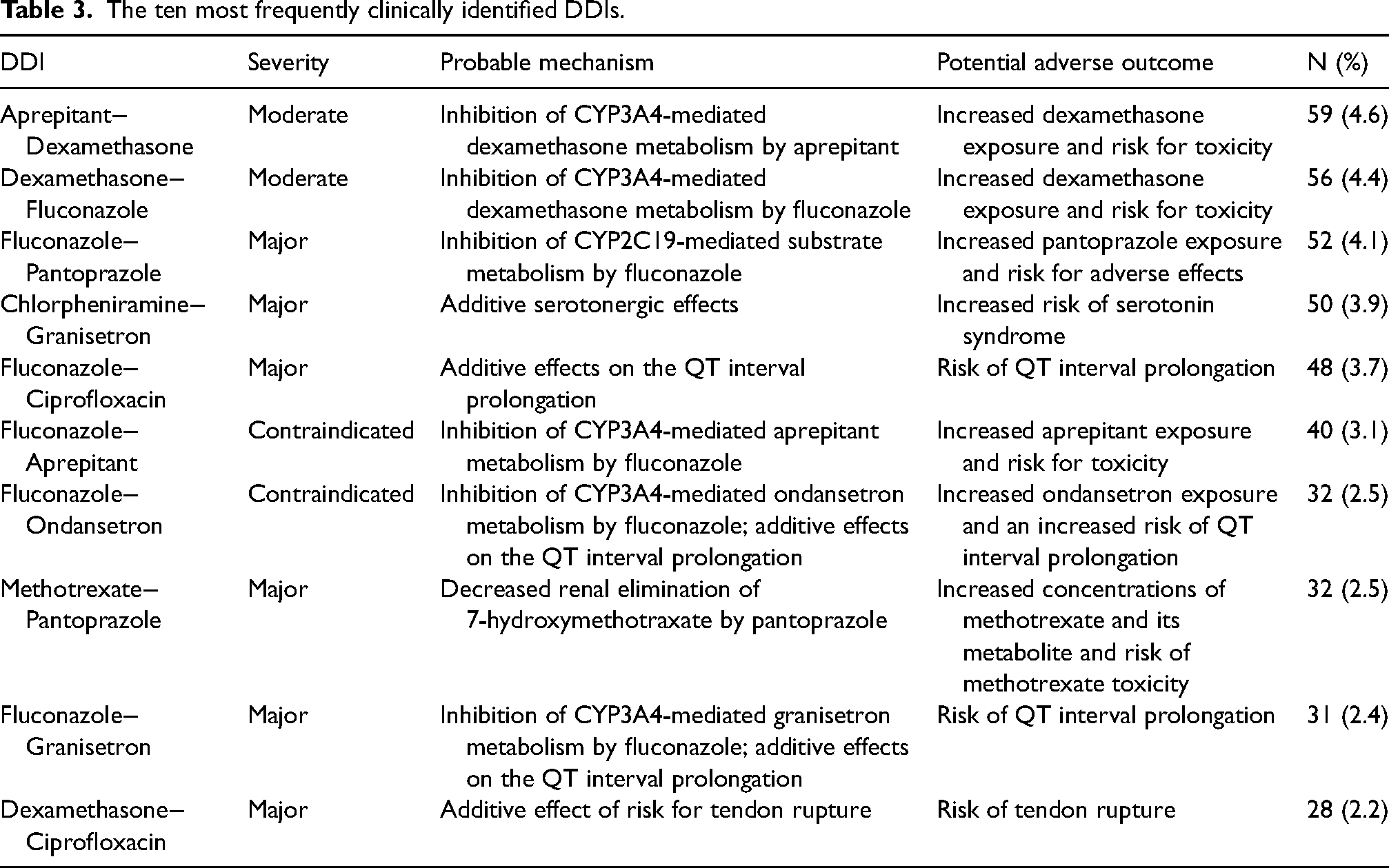
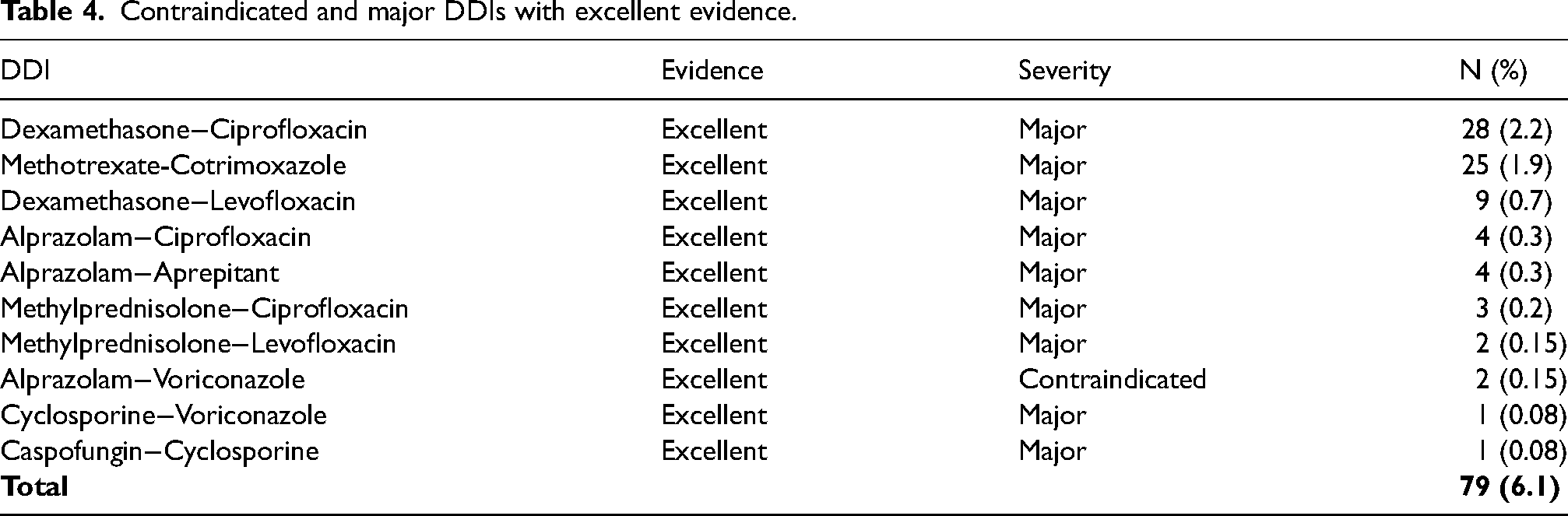
Of the identified DDIs, 81.1% were considered clinically significant, necessitating pharmacotherapy intervention. Aprepitant−dexamethasone (4.6%), dexamethasone−fluconazole (4.4%), and fluconazole−pantoprazole (4.1%) were the most frequently identified DDIs among the patients. However, severe DDIs (those categorized as contraindicated or major in severity), supported by excellent evidence, were prevalent in only 6.1% of patients. Table 3 presents the ten most commonly identified clinically significant DDIs, while Table 4 outlines the severe DDIs supported by excellent evidence.
The ten most frequently clinically identified DDIs.
Contraindicated and major DDIs with excellent evidence.
A total of 1059 interventions (averaging 5.2 per patient) were performed by the clinical pharmacist to address these clinically identified DDIs. The most common type of intervention was monitoring therapy (81.4%), followed by stopping drugs (6.4%) and change in time of drug administration (6.1%). Table 5 and Figure 1 present the characteristics of interventions conducted by the clinical pharmacist to manage identified DDIs.
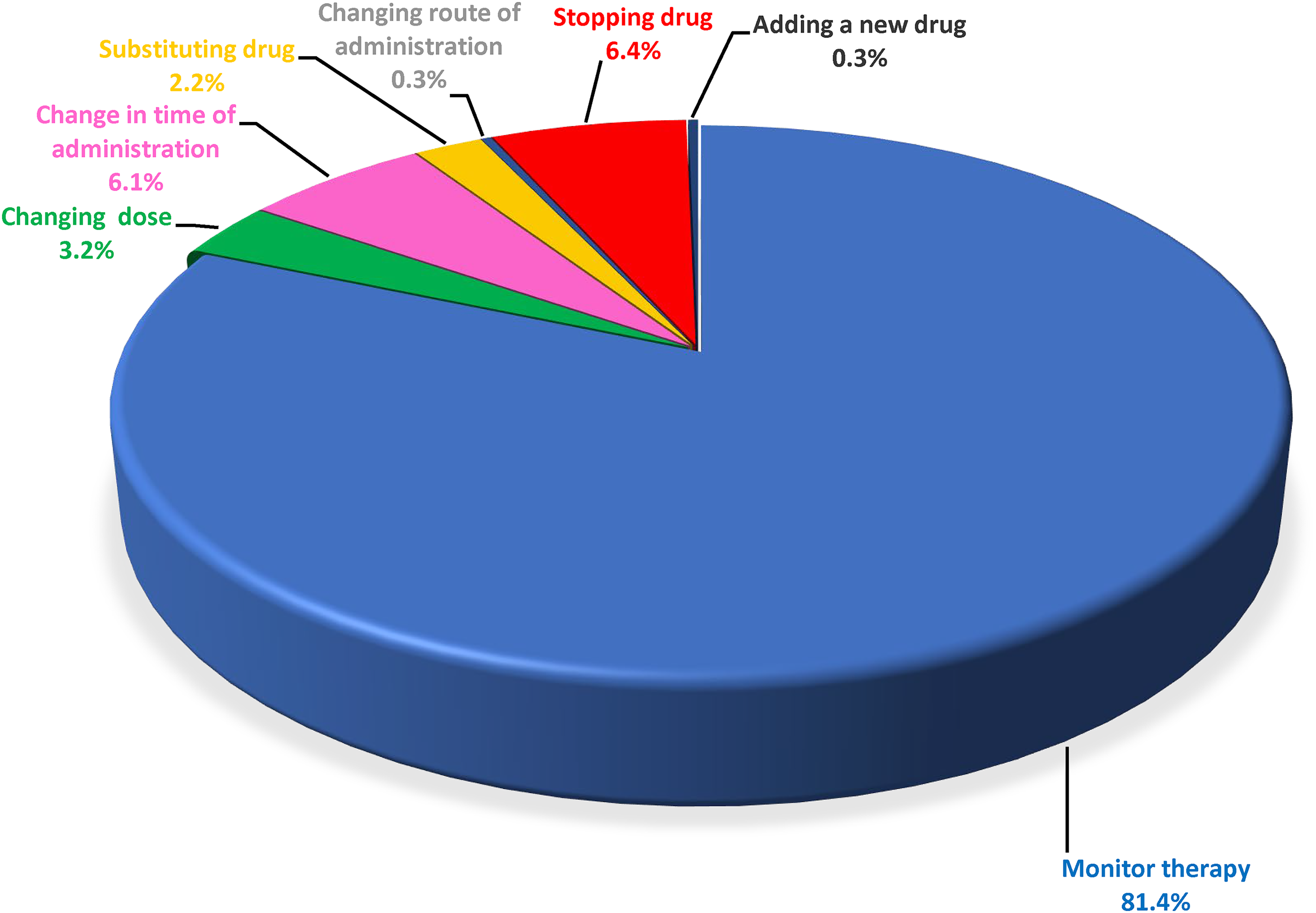
Types of clinical pharmacist's interventions for managing identified DDIs.
Description of clinical pharmacist interventions (1059) for managing clinically identified DDIs.
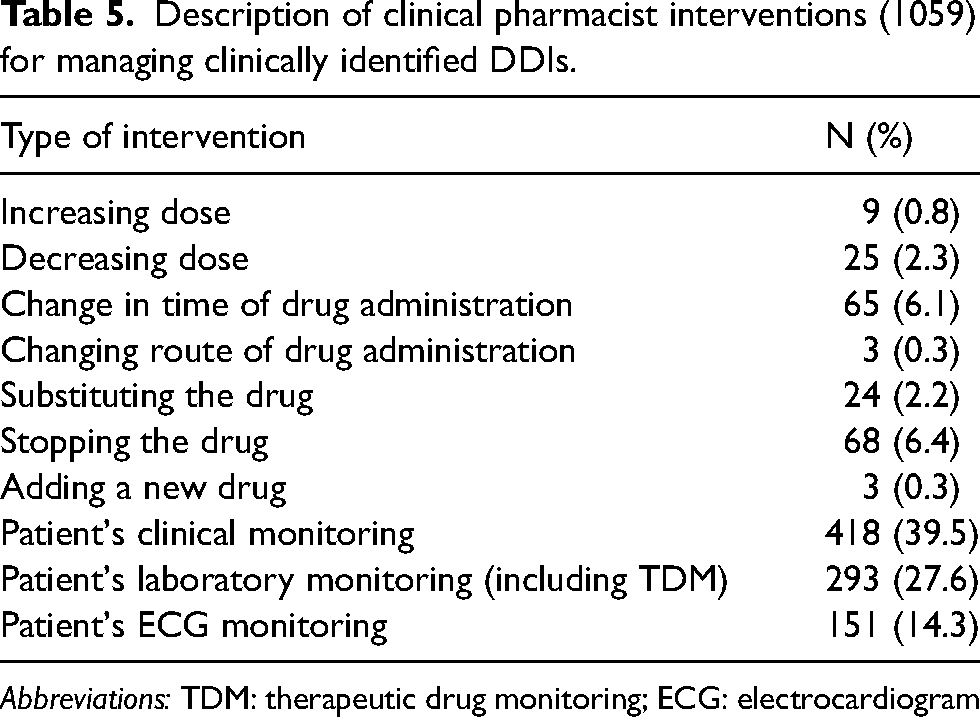
Abbreviations: TDM: therapeutic drug monitoring; ECG: electrocardiogram
Related Factors to DDIs
A significant relationship was observed between the number of drugs used during hospitalization and the occurrence of DDIs (P < 0.001, r = 0.633). Furthermore, the correlation coefficient suggests that 40% of the variability in the occurrence of DDIs can be explained by the number of drugs used (R2 = 0.40). However, no significant relationship was found between the occurrence of DDIs and factors such as age, gender, and the type of malignancy (P = 0.711, 0.057, 0.547, respectively). Figure 2 displays the correlation between the number of administrated drugs and the occurrence of DDIs.
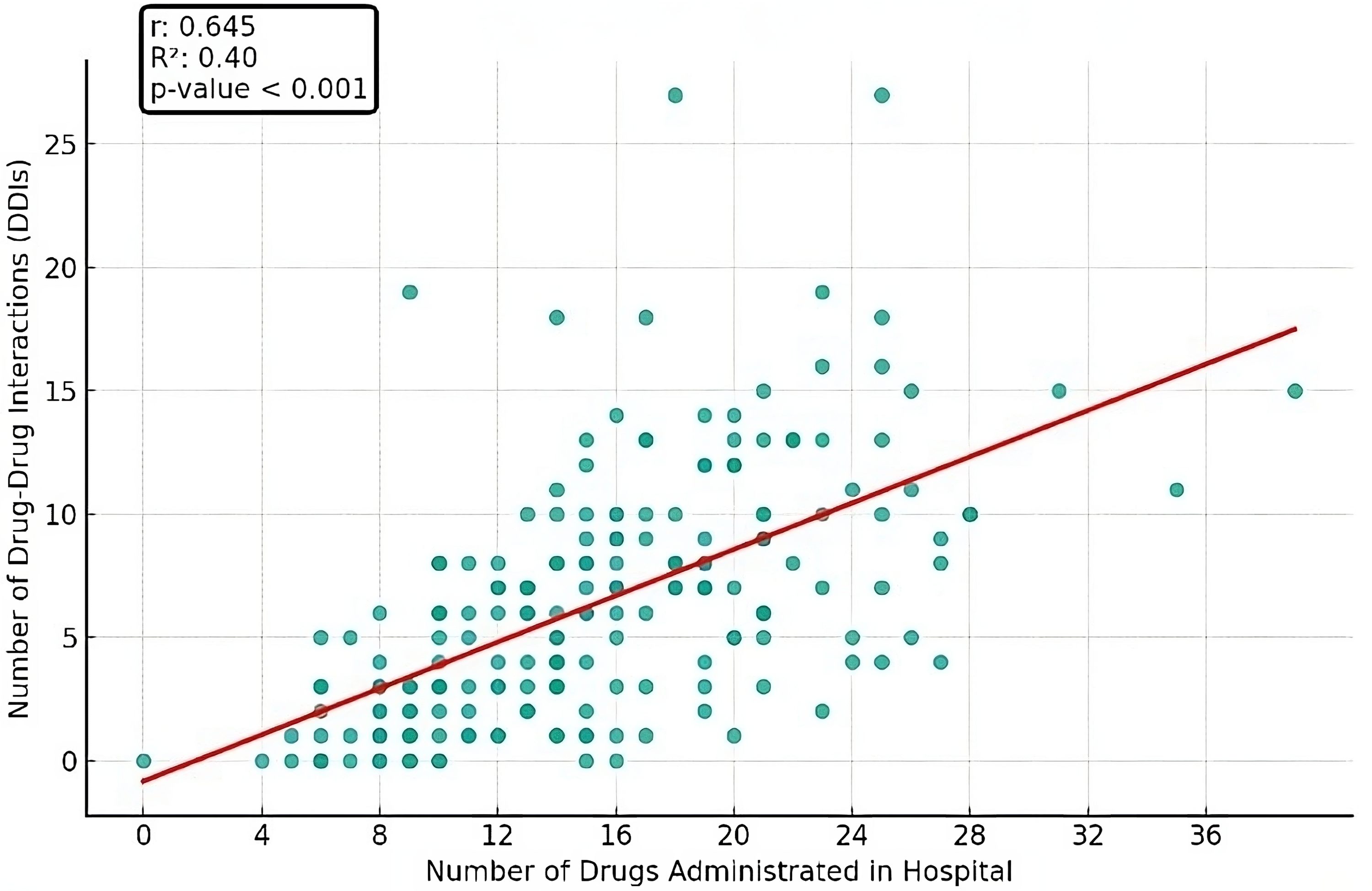
Correlation between the number of drugs administrated during hospitalization and the occurrence of DDIs. *Darker points indicate a repetition of a DDI in different patients.
Discussion
The complexity of medication regimens, including both anticancer drugs and medications for managing comorbidities, appears to be the primary reason for the high prevalence of DDIs among patients with hematologic malignancies. Similar studies have also indicated a significant prevalence of DDIs in this population of patients.15,16 We found that medications prescribed for the prevention of comorbid conditions, such as antimicrobial agents and antiemetics, exhibit the highest potential for interactions with other drugs, including anticancer agents. A network analysis conducted on hospitalized patients with hematologic malignancies further confirmed that DDIs were among the major causes of DRPs, with the majority of causative drugs (93%) for DRPs being related to supportive care. 17 Other similar studies have consistently reported fluconazole, granisetron, and dexamethasone as the most commonly implicated medications in DDIs among cancer patients.15,16,18
This prevalence is largely attributed to the pharmacokinetic properties of these medications. 19 For example, azole antifungals such as fluconazole and voriconazole, extensively used in the prevention and treatment of invasive fungal infections, act as potent inhibitors of cytochrome P450 (CYP) enzyme systems. This inhibition can disrupt the metabolism of other drugs, potentially leading to drug toxicity. 20 Similarly, fluoroquinolones such as ciprofloxacin, widely used for preventing or treating febrile neutropenia in cancer patients, inhibit CYP1A2, which can impair the elimination of substrate drugs.21,22 Antiemetics are also commonly used in cancer patients due to the high risk of nausea and vomiting associated with chemotherapy. Medications such as ondansetron, granisetron, aprepitant, dexamethasone, and olanzapine pose potential risks for DDIs due to their distinct pharmacokinetic profiles and metabolism pathways.23,24 Additionally, corticosteroids such as dexamethasone, are crucial drugs in hematologic patients used for antiemetic purposes, premedication, and anti-tumor effects. They act as both substrates for P-glycoprotein mediated efflux from cells and inducers of P-glycoprotein production. Hence, these medications have also a high potential for interaction with other drugs. 25
A notable proportion of DDIs involved cancer treatment protocols, with 11.5% of the interactions including at least one oncologic drug. This suggests that many DDIs can be anticipated and managed proactively in oncology settings. Additionally, interactions between pre-hospitalization medications and hospital-prescribed cancer treatments were also significant, indicating the need for comprehensive management strategies. Further studies could explore these interactions to better predict and manage DDIs in oncology settings.
Another concern with adverse effects due to DDIs is QT interval prolongation and the risk for torsade de pointes, as highlighted in our study. Combinations of QT-interval prolonging drugs such as arsenic, tyrosine kinase inhibitors, azole antifungals, fluoroquinolones, 5HT3 antagonists, opioids, and psychotropic agents are frequently encountered in hemato-oncology practice, underscoring the need for careful electrocardiogram (ECG) monitoring and management to mitigate the potential for severe outcomes.26,27 Other studies have also emphasized the importance of recognizing interactions leading to QT prolongation in cancer patients and the need for careful monitoring to prevent adverse cardiac events. 28
The most common intervention by clinical pharmacists in this study involved monitoring therapy, encompassing both clinical and laboratory aspects. The comparative analysis of DDI prevalence across studies highlights the critical importance of integrating pharmacokinetic and pharmacodynamic considerations into DDI management strategies. 29 Since many drugs administered to cancer patients are essential for which suitable alternatives barely exist, discontinuing interacting drugs is often not straightforward. Thus, in many cases, close patient monitoring, especially through therapeutic drug monitoring (TDM), can effectively manage DDIs without compromising the primary treatments. 30 Other studies also highlight the importance of close monitoring by clinical pharmacists as an effective strategy for the management of DDIs.31,32
The utilization of interaction checker databases, such as Lexi-interact® known for its good sensitivity, and Micromedex® recognized for its good specificity, facilitates the initial detection of DDIs. 33 However, the reliability of these databases is often fair, as observed in our study. We identified significant discrepancies in the classification of interaction severity between these two databases. Specifically, approximately more than 77% showed divergent severity ratings. For instance, Lexi-Interact® might categorize an interaction as ‘moderate’ with a recommendation for monitoring, while Micromedex® could classify the same interaction as ‘major,’ advising against co-administration. Therefore, each identified DDI requires clinical analysis within the context of the individual patient, necessitating a tailored approach. The expertise and critical evaluation provided by clinical pharmacists and hemato-oncologists were pivotal in discerning relevant DDI from irrelevant ones, highlighting the importance of interdisciplinary collaboration in DDI management. 34 Additionally, further studies are needed to enhance the level of evidence regarding the clinical impact of DDIs.
Conclusion
In conclusion, our study highlights the significant prevalence and clinical implications of DDIs among hospitalized patients with hematologic malignancies. As the number of medications administered to these patients increases, so does the likelihood of occurrence of interactions. Although interaction checker databases provide useful insights, the indispensable role of clinical pharmacists in assessing the clinical impact of identified DDIs and enacting appropriate interventions cannot be overstated. Moving forward, proactive interventions led by clinical pharmacists to identify and manage DDIs should be a priority in hematology care.
Footnotes
Acknowledgments
We would like to thank all the staff at Shariati Hospital for their help and support.
Authors’ contribution
BS and MV designed the study; SZ and EH collected the data; BS, KS, and MV performed the analysis and interpreted the results; SZ and EH drafted the manuscript. All authors reviewed and approved the final version of the manuscript.
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.