
Abstract
Introduction
A hypoxic tumor microenvironment inhibits the normal functioning of immune cells. Studies have hypothesized that anticoagulants that can penetrate and bind to factor Xa in the tumor microenvironment, can enhance T-cell function and augment immunotherapy activity. This study compared objective response rate and progression-free survival of lung cancer patients on concomitant immunotherapy treated with direct-acting oral anticoagulants versus enoxaparin.
Methods
This single-center retrospective study included 73 adults with stage-IV lung cancer who received at least two cycles of immunotherapy and one month of anticoagulant therapy with direct-acting oral anticoagulants (Arm A) versus enoxaparin (Arm B) between June 1, 2016, to September 30, 2022. Primary endpoint was objective response rate, and secondary endpoints were rates of complete response, progression-free survival, incidence of thrombotic events, and major bleeding.
Results
Objective response rate at 6 months was 24.5% versus 25% while progression-free survival at 6 months was 54.7% versus 45% in Arm A versus Arm B, respectively. Complete response rates at 6 months were 7.5% in Arm A versus 0% in Arm B. One patient in Arm A and two in Arm B had a recurrent deep vein thrombosis. Nine patients in Arm A and two in Arm B were diagnosed with new deep vein thrombosis. One patient in Arm B was diagnosed with new pulmonary embolism. Two major bleeding events occurred in Arm B.
Conclusions
Our study suggests a trend toward improved progression-free survival at 6 months with no new safety concerns in lung cancer patients on concurrent immunotherapy and direct-acting oral anticoagulants.
Keywords
Background
Immune checkpoint inhibitors (ICIs) have revolutionized cancer care and have demonstrated strong and durable responses even in highly advanced stages. Given the ubiquitous use of ICIs across various malignancies, it is important to identify factors that are associated with improved immunotherapy response.
It has been suggested that a hypoxic tumor microenvironment (TME) inhibits the normal metabolism of immune cells, T-cell infiltration, and T-cell function.1,2 Furthermore, vaso-occlusion caused by intravascular cancer-associated thrombosis has been shown in several preclinical models to lead to limited tumor perfusion and hypoxia.1,2 It has also been proposed that coagulation factors might promote resistance to ICI therapy and contribute to tumor evasion.3,4 Upregulation of the coagulation-initiating tissue factor (TF) on cancer cells leads to tumor growth, angiogenesis, and metastasis. 5 The complex TF-coagulation factor VIIa (FVIIa) leads to the formation of coagulation factor Xa (FXa). 6 The activation of protease-activated receptors (PAR), specifically PAR 2, by cancer cell-expressed tissue factor (TF) and FVIIa or coagulation factor Xa (FXa), promotes tumor progression.7,8 In a mouse model with mutant PAR that is not cleaved by FXa by Graf et al., slower tumor growth and a higher concentration of anti-tumor cytotoxic lymphocytes were observed in the tumor stroma. 9 These preclinical models indicate that there might be a synergistic effect between ICI and FXa inhibitors. Rivaroxaban, but not low-molecular weight heparins, was shown to inhibit tumor growth, indicating that the tissue penetrance of direct-acting oral anticoagulants (DOACs) enable them to reach FXa in the TME to specifically target the PAR 2 cell-autonomous signaling pathway and consequently enhance the infiltration of cytotoxic T cells and dendritic cells to the tumor site.7,9,10,11 Conversely, heparins, which depend on antithrombin for FXa inhibition, are largely restricted to the intravascular and perivascular space and were not shown to enhance ICI efficacy.7,9,10,11 Rivaroxaban-treated mice were also shown to reduce the growth of programmed cell death ligand-1 (PD-L1)-expressing tumor associated macrophages, whose presence in the TME supports angiogenesis and metastasis. This observation lends further credence to the hypothesis that DOACs may enhance immunotherapeutic agents.7,9 Similarly, Metelli et al. showed that thrombin inhibition with dabigatran enhanced efficacy of anti-programmed-cell-death-protein (PD)-1 therapy by blocking the release of transforming growth factor β (TGF-β), an immunosuppressive cytokine released by active platelets. 4
The role of the effect of anticoagulation on ICI response merits being evaluated clinically, particularly in cancers with higher incidences of thrombosis, such as lung cancer.12,13,14 Furthermore, it has been suggested that highly thrombotic cancers, such as lung cancer, may derive greater benefit from the combination of DOACs and immunotherapy since the TME is more hypoxic which inhibits the normal T-cell function. 2 Cancer-associated thrombosis is the second leading cause of morbidity and mortality in oncology patients. 15 With current practice for patients who require therapeutic or prophylactic anticoagulation, the class of anticoagulation is not selected based on whether the patient is receiving immunotherapy. Data from retrospective studies suggest that the incidence of VTE is between 2.6 and 30.3% and the incidence of arterial thromboembolism ranges from 1 to 6% in patients treated with immunotherapy. 14 In addition, it has not been established whether the use of anticoagulation therapy can effectively reduce the incidence of thromboembolism in cancer patients treated with ICIs. 14
Our study aimed to add to the limited body of clinical research by determining whether the therapeutic or prophylactic use of DOACs compared to enoxaparin is associated with improved 6-month overall response rate (ORR) and progression-free survival (PFS) in patients with advanced stage lung cancer who are receiving concurrent ICI therapy.
Patients and methods
Design and setting
This single-center retrospective chart review was conducted across a large metropolitan hospital system comprised of seven hospitals from June 1st, 2016, through September 30th, 2022. Patients aged 18 and older with advanced lung cancer (ICD-10 code C34) who received concurrent treatment with an immunotherapy agent (pembrolizumab, atezolizumab, nivolumab, cemiplimab, ipilimumab, or durvalumab) and an anticoagulant for at least one month were included. Patients who received concurrent therapeutic or prophylactic doses of a DOAC (apixaban, rivaroxaban, or edoxaban) were included in Arm A while those who received therapeutic or prophylactic doses of enoxaparin were included in Arm B. Considering this was a historical cohort, patients were treated per the physician's discretion and according to the best available data and guideline recommendations at the time of treatment initiation. Patients were identified using the reporting functionality within the electronic health record (EHR). To limit confounders, patients were excluded if they transferred care to another institution that did not share an EHR with our hospital, received less than two cycles of ICI therapy, or had stage I-III lung cancer. This study was approved by the Institutional Review Board at our institution with a waiver for informed consent.
Outcomes
The primary endpoint of the study was ORR defined as the proportion of patients with complete response (CR) or partial response (PR). To ensure reproducibility and accuracy of results, response was classified as CR, PR, stable disease (SD), or progressive disease (PD) according to the revised Response Evaluation Criteria in Solid Tumors (RECIST) guidelines (version 1.1) as well as iRECIST to address the limitation of RECIST 1.1 in cases of pseudo-progression under immunotherapy as documented in oncologist's progress notes or radiologist's report.16,17 Additional secondary endpoints included rates of CR, PFS, overall survival (OS), incidence of arterial or thrombotic events while on treatment with immunotherapy and anticoagulation, and incidence of major bleeding according to International Society on Thrombosis and Haemostasis (ISTH) criteria. 18
Data collection
Baseline demographics including race, age, sex, type of malignancy, stage of malignancy, eastern cooperative oncology group (ECOG) performance status, number of prior lines of therapy, pre-existing comorbid conditions (including hypertension, hyperlipidemia, coronary artery disease, congestive heart failure, diabetes, and chronic kidney disease), type of immunotherapy, dose of immunotherapy, number of cycles of immunotherapy, and home medications (non-steroidal-anti-inflammatory drugs (NSAIDs), aspirin, and erythropoietin stimulating agents (ESAs)).
Statistical analysis
Descriptive statistics were performed to summarize patient demographics and clinical variables. Categorical variables were summarized with percentages, while continuous variables were summarized using mean, median, standard deviation, interquartile 25th and 75th percentiles, and range. Treatment duration was calculated as the period between initial drug administration and treatment discontinuation. PFS was calculated from initial ICI administration to the date of radiological or clinical disease progression, last follow-up, or death from any cause.
Results
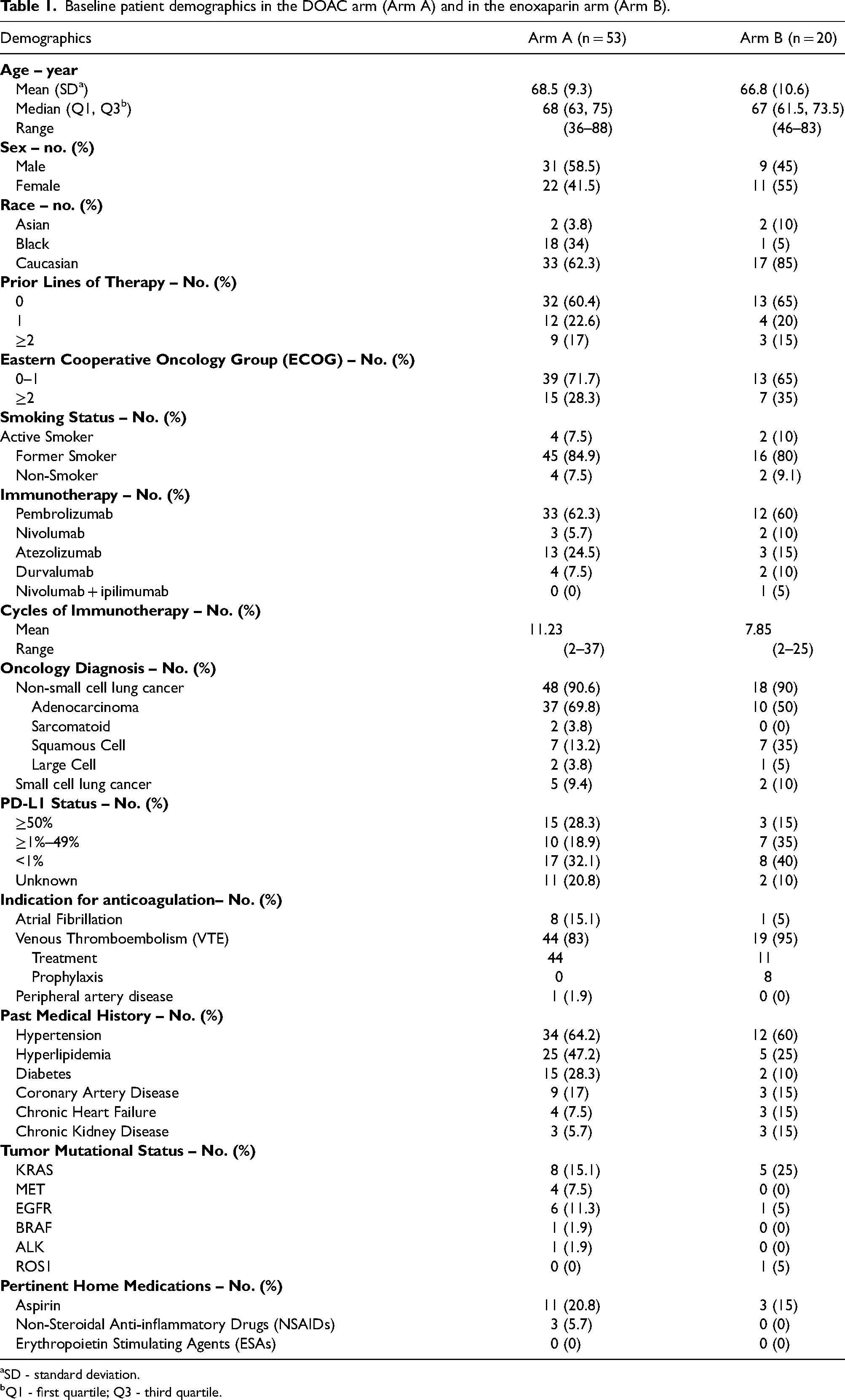
Between June 1st, 2016, and September 30th, 2022, a total of 1039 patients with cancer on immunotherapy were identified. Among those, 357 patients were deemed eligible to be considered for inclusion. Of 357 eligible patients, 73 patients (53 patients in Arm A and 20 patients in Arm B) met the inclusion criteria (Figure 1). The demographic characteristics of the two arms are depicted in Table 1. The median age was 68 (IQR: 12) and 67 (IQR: 12) in the DOAC and enoxaparin populations, respectively. Approximately, 59% and 45% were males in the DOAC and enoxaparin populations, respectively. Most of the study population had an ECOG status of zero to one (60.4% in Arm A versus 65% in Arm B). The majority received pembrolizumab (62.3% in Arm A versus 60% in Arm B) followed by atezolizumab (24.5% in Arm A versus 15% in Arm B). Approximately 90% of the total population was diagnosed with non-small cell lung cancer (NSCLC); the most common histologic subtypes were adenocarcinoma (69.8% in Arm A versus 50% in Arm B) and squamous cell (13.2% in Arm A versus 35% in Arm B). The most common indication for anticoagulation was either treatment or prophylaxis for VTE across both populations (83% in Arm A versus 95% in Arm B). Mutations in the KRAS gene were the most common genomic alterations in both Arm A and Arm B at 15.1% and 25%, respectively. Home medications were evaluated to assess for confounding factors that could impact safety, namely bleeding. Of note, 20.8% and 15% of patients in Arm A and B, respectively, were on concomitant aspirin for cardiovascular protection. Three patients in Arm A were receiving NSAIDs.
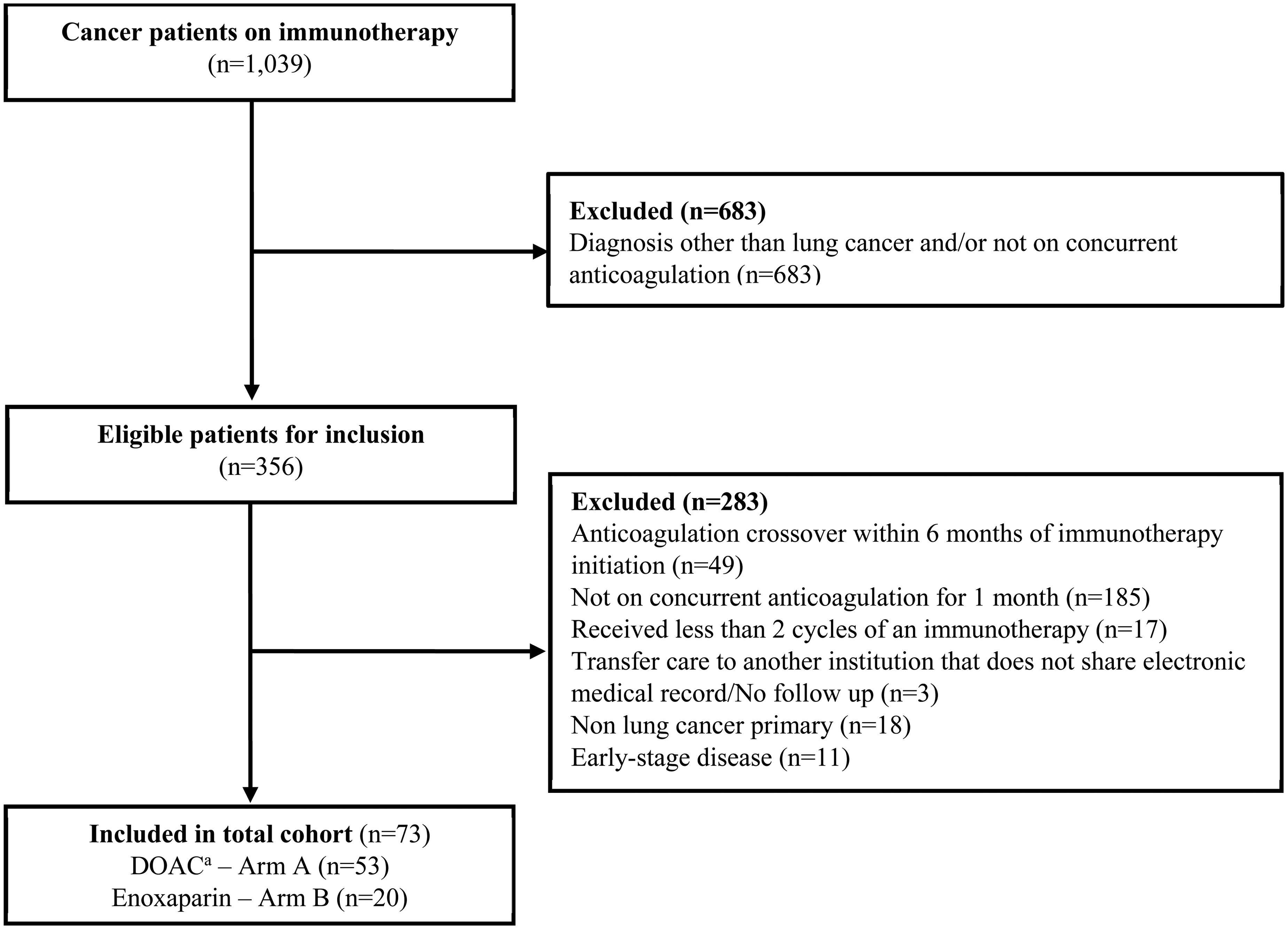
Eligibility flow diagram.
Baseline patient demographics in the DOAC arm (Arm A) and in the enoxaparin arm (Arm B).
SD - standard deviation.
Q1 - first quartile; Q3 - third quartile.
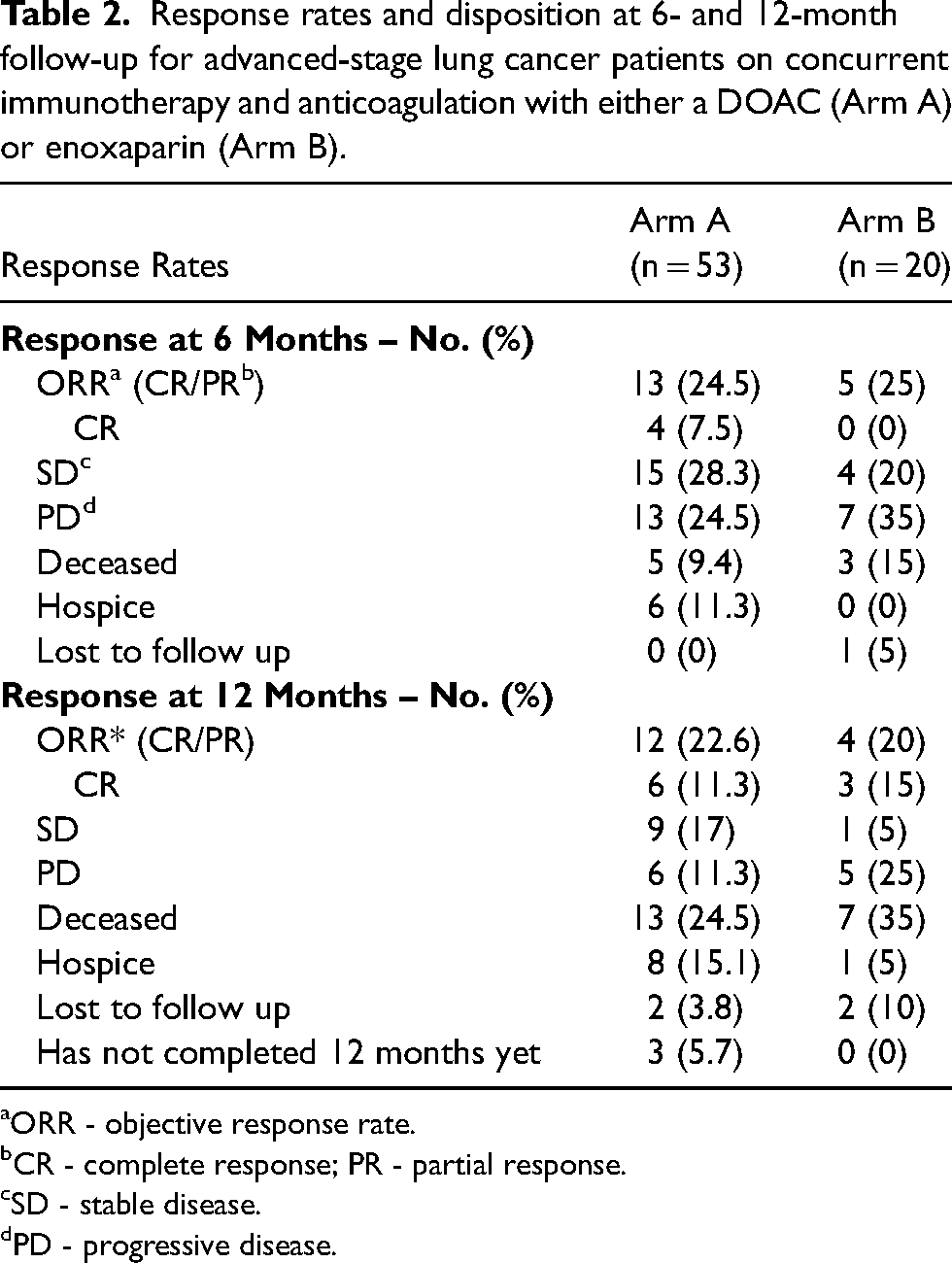
ORR was assessed by reviewing imaging studies (computer tomography chest or chest, abdomen, and pelvis, positron emission tomography scan, and/or magnetic resonance imaging scans) and physician interpretations. ORR at 6 months according to the RECIST 1.1 and iRECIST guidelines was not clinically different between the two treatment arms (24.5% in Arm A versus 25% in Arm B); however, the rates of CR were clinically different between the groups (7.5% in Arm A versus 0% in Arm B). A higher percentage of patients had SD at 6 months in Arm A (28.3%) versus Arm B (20%). A lower percentage of patients had PD in Arm A (24.5%) versus Arm B (35%). At 6-month follow up, 9.4% and 15% of patients in Arm A and Arm B had passed away, respectively. At 6-month follow up, six patients in Arm A had transitioned to hospice, and one patient in Arm B was lost to follow up. Additionally, data regarding ORR at 12 months including rates of CR, PD, and SD for patients that had available data were collected and summarized in Table 2. PFS at 6 months accounting for both patients with ORR and SD was 54.7% in Arm A as compared to 45% in Arm B, correlating with OS at 6 months of 91% and 85% in Arm A and B, respectively (Figure 2).
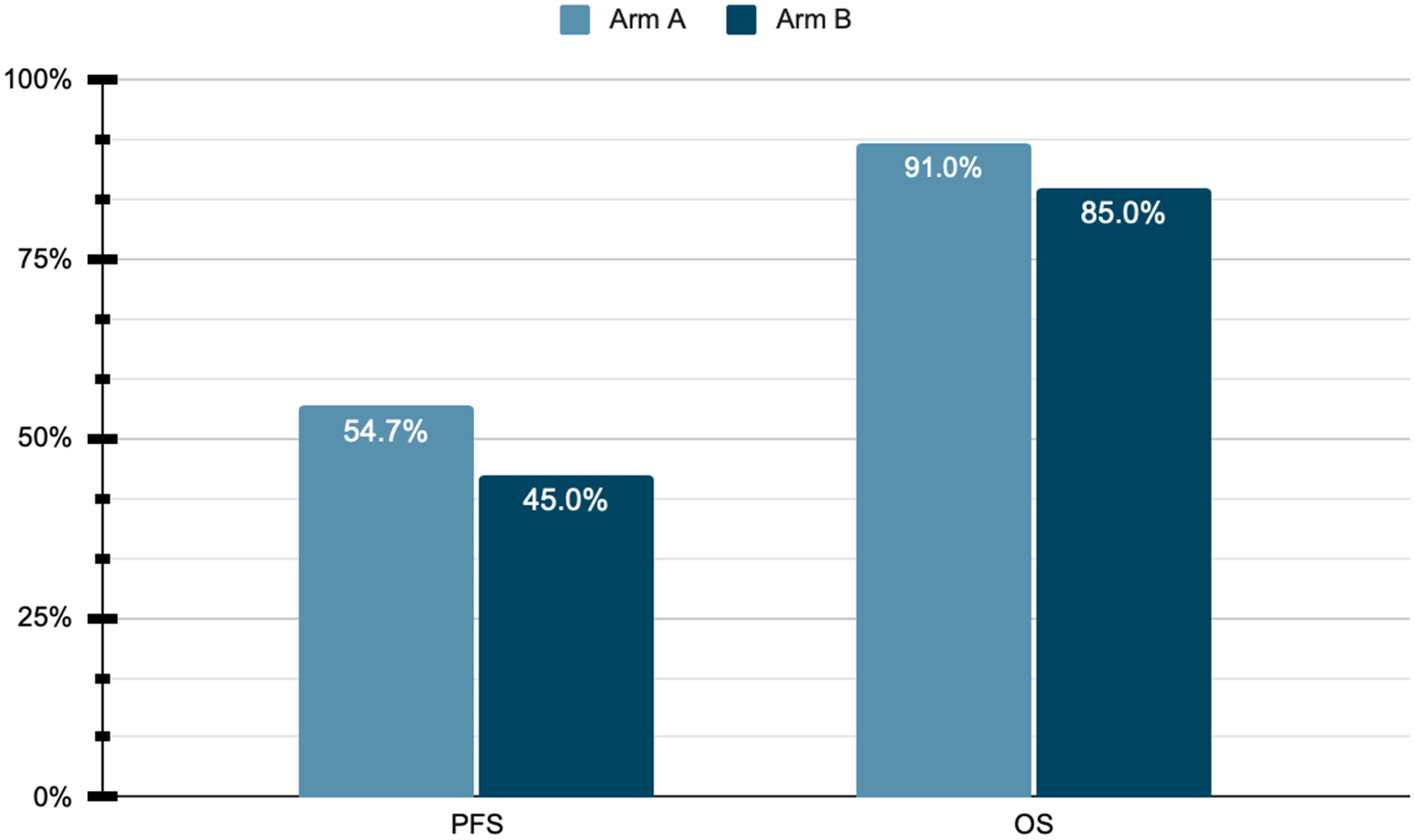
Progression free survival (PFS) and overall survival (OS) at 6 months.
Response rates and disposition at 6- and 12-month follow-up for advanced-stage lung cancer patients on concurrent immunotherapy and anticoagulation with either a DOAC (Arm A) or enoxaparin (Arm B).
ORR - objective response rate.
CR - complete response; PR - partial response.
SD - stable disease.
PD - progressive disease.
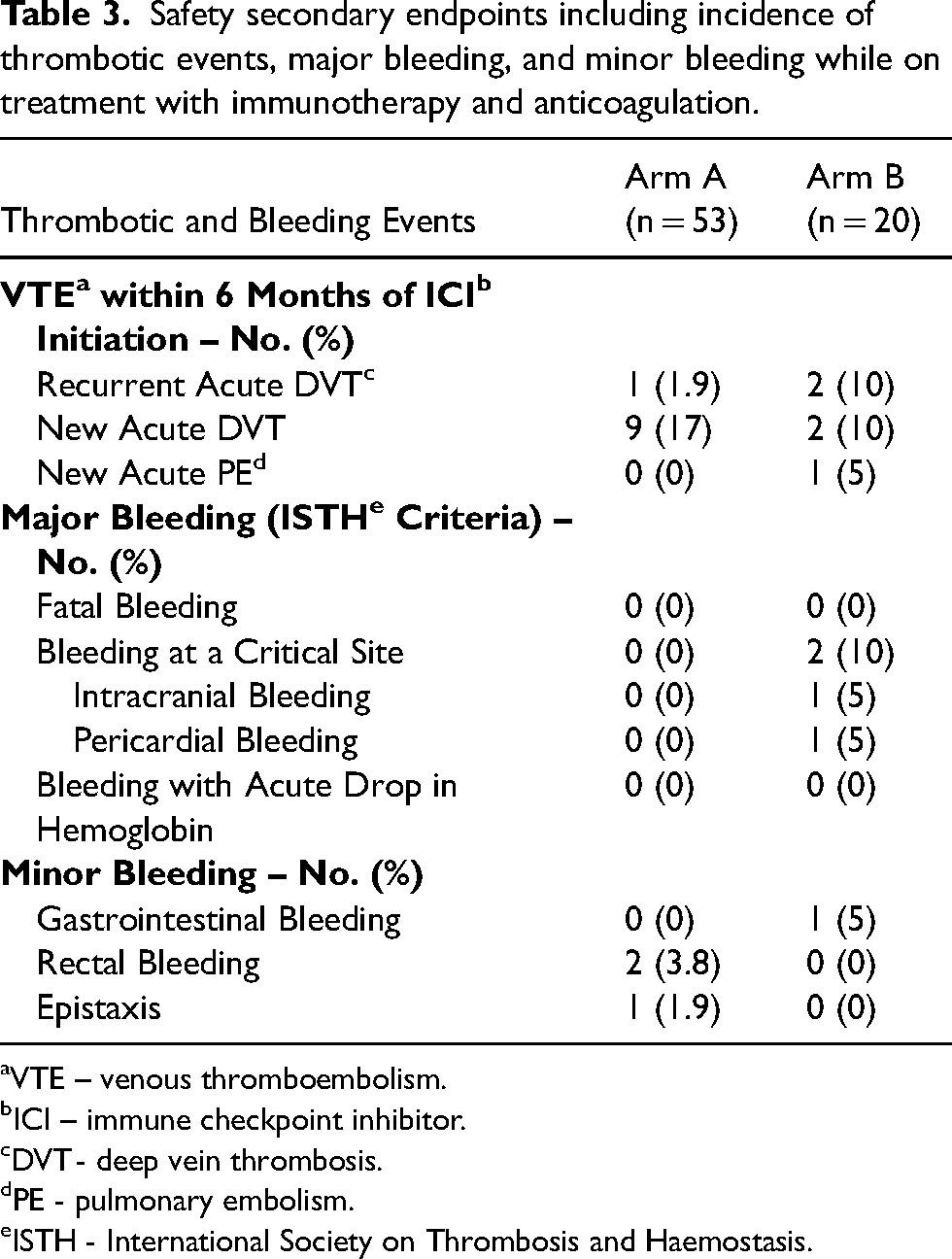
Safety data including rates of thromboembolic events and both minor and major bleeding according to ISTH Criteria were assessed at 6 months. One patient (1.9%) experienced recurrent DVT in Arm A while two patients (10%) experienced recurrent DVT in Arm B. In addition, 12 (16.4%) new thrombotic events occurred in patients who were initiated on ICI therapy without any prophylactic anticoagulation. A total of 11 (15%) patients in the entire population who were initiated on ICI therapy without any anticoagulation experienced a new acute DVT and were ultimately initiated on therapeutic anticoagulation; nine were initiated on a DOAC and two were initiated on enoxaparin. One (1.4%) patient who had been on ICI therapy without any anticoagulation experienced a new acute pulmonary embolism and was ultimately initiated on enoxaparin. There was no observed major bleeding according to the ISTH Criteria in Arm A as compared to two (10%) major bleeding events in a critical site which were observed in Arm B. Both major bleeding events, intracranial and pericardial bleeding, occurred in the same patient. Three patients (5.7%) in Arm A experienced minor bleeding which consisted of two rectal bleeding events and one incidence of epistaxis. One patient (5%) in Arm B experienced minor gastrointestinal bleeding. Thrombotic and bleeding events are summarized in Table 3.
Safety secondary endpoints including incidence of thrombotic events, major bleeding, and minor bleeding while on treatment with immunotherapy and anticoagulation.
VTE – venous thromboembolism.
ICI – immune checkpoint inhibitor.
DVT - deep vein thrombosis.
PE - pulmonary embolism.
ISTH - International Society on Thrombosis and Haemostasis.
Discussion
Lung cancer is the primary cause of cancer death in the United States and around the globe. 19 Although different anti-cancer modalities are available for the management of lung cancer including surgery, chemotherapy, radiation therapy, and combination approaches, they have shown limited OS in locally advanced and metastatic settings. 19 Early detection increases the likelihood of good prognosis, tumor resection, treatment, and durable response; however, lack of robust screening tools, genetic heterogeneity, and advanced stage at diagnosis make it a challenging and fatal cancer. 19 Recent studies have expanded and refined our understanding of the immune system's reaction to cancer and how we could best utilize this mechanism to our advantage leading to improvements in cancer immunotherapy.
Immunotherapy yields robust response rates in lung cancer and possesses efficacy irrespective of histology subtype, leading to sustained remission. Despite remarkable response rates, resistance to ICI therapy has risen and has become an area of active clinical research. Recent studies suggest that coagulation factors may play a pivotal role in tumor progression and resistance to ICI therapy.1–4 In light of this discovery, there is growing research in identifying the role of coagulation factors in response rates to immunotherapy. In this study, we examined a real-world cohort of 73 patients (53 patients in Arm A and 20 patients in Arm B) with stage IV lung cancer who received ICI therapy and stratified their ORR and PFS based on the choice of anticoagulant class that they received. To our knowledge, this is the first study to examine the correlation between ICI response and DOACs or enoxaparin in highly thrombotic advanced stage lung cancer. A smaller study showed that prophylactic or therapeutic anticoagulation with low molecular weight heparin was not associated with better PFS or OS in 47 patients with NSCLC treated with PD-1 or PD-L1 blockade. 20 However, the sample size was smaller, and no study to date has assessed the effect of DOACs in comparison to enoxaparin on ICI response.
While ORR at 6 months in the two anticoagulation arms (24.5% in Arm A versus 25% in Arm B) were similar, the rates of CR were clinically different between the groups (7.5% in Arm A versus 0% in Arm B). It is not unusual to see low but durable responses to ICIs, and it is suggested that non-responders may have an inhibitory tumor environment, potentially through FXa independent pathways. 21 A retrospective study including 322 patients with advanced cancer treated with ICI found that CR was independently associated with improved OS regardless of disease state, ICI agent or line of therapy. 22 Given the higher percentage of patients that had SD at 6 months in Arm A (28.3%) relative to Arm B (20%), PFS was higher at 6 months in Arm A (54.7%) versus Arm B (45%), correlating with OS at 6 months of 91% and 85% in Arm A and B respectively. Predictors of response to ICI in NSCLC include performance status, smoking status, PD-L1 status, and histology type.23–25 Arm A did have a higher percentage of patients with high PD-L1 status (28.3% versus 15%, respectively) and a higher percentage of patients with good performance status (71.7% vs 65%, respectively) compared to Arm B. On the other hand, Arm B had a higher percentage of patients with squamous NSCLC (35% versus 13.2%, respectively), which derive greater PFS and OS benefit from ICI as compared to non-squamous NSCLC. 25 Similarly, there was a higher proportion of KRAS mutant NSCLC in Arm B compared to Arm A (25% versus 15.1%, respectively) and a lower proportion of ALK/EGFR mutant NSCLC in Arm B compared to Arm A (5% versus 13.2%, respectively). It has been shown that KRAS mutant NSCLC (higher proportion in Arm B) predicts a superior response to immunotherapy while ALK/EGFR mutant NSCLC (higher proportion in Arm A) does not, yet PFS was still improved in Arm A. 26
In a recent systematic review and meta-analysis, data from 60 randomized controlled trials with 74 experimental ICI arms and more than 17,000 patients were utilized to validate 6-month PFS and ORR as estimators of 12-month OS. 27 They concluded that ORR was a poor predictor of 12-month OS when ICI combination studies were included; however, they validated that 6-month PFS reliably predicted 12-month OS. Their pooled analysis consisted of a heterogeneous population testing 7 different ICI agents (pembrolizumab, nivolumab, ipilimumab, durvalumab, tremelimumab, atezolizumab, and avelumab), from first- to fourth-line treatment, and in 12 different tumor types including NSCLC (36%). 27 This association between PFS and OS in ICI therapy was previously also reported by another group which showed a high correlation between PFS hazard ratio and OS hazard ratio compared to moderate correlations between ORR and OS in patients treated with durvalumab. 28 Given the implications of the meta-analysis and systematic review, it is reasonable to assume a higher 12-month OS in the DOAC population compared to the enoxaparin population within our current study. To further assess this, we analyzed data for up to 12 months after ICI initiation for all but three patients that had not yet completed 12-months of follow up during our study period. At 12-months of follow-up, 24.5% of the population in Arm A had passed away compared to 35% of the population in Arm B. Similar ORRs were observed in both populations at 12-month follow up.
Of note, clinical data have not reliably demonstrated the association between FXa and thrombin inhibition and enhanced ICI response. A 2021 single-center cohort study did not find a significant difference in ORR between patients receiving concomitant anticoagulation with ICI and those not. 29 The cohort included mostly melanoma patients; almost 50% of patients received DOACs. 29 Multivariable analysis showed that patients on enoxaparin had significantly worse PFS, but PFS was similar for patients on warfarin, direct thrombin inhibitors, and FXA inhibitors. 29 In another retrospective study, 27 patients with melanoma receiving concomitant treatment with FXa inhibition during initial ICI therapy showed a significantly improved ORR and PFS as compared to patients not receiving anticoagulation or patients treated with other anticoagulants, such as heparins or vitamin K antagonists. 11 Our study results add to the growing literature on the role of anticoagulation in augmenting ICIs response rates.
The findings within this study did not identify new safety signals in terms of bleeding in either population; however, the rates of recurrent DVT within 6 months of ICI initiation while on concurrent anticoagulation was numerically higher in Arm B (10%) versus Arm A (1.9%). Eleven (15%) patients in the entire population who were initiated on ICI therapy without any prior anticoagulation experienced a new acute DVT and were ultimately initiated on therapeutic anticoagulation. There were no major bleeding events as defined by the ISTH criteria in Arm A while there were two bleeding episodes at a critical site in Arm B both occurring in the same patient. The incidence of minor bleeding was similar between the two arms at 5.7% in Arm A compared to 5% in Arm B. While randomized trials have demonstrated that the use of a DOAC compared with a LMWH resulted in a noninferior risk of recurrent VTE and similar rates of major bleeding,30,31 real-world analyses have shown that DOACs are associated with a lower risk of VTE recurrence, major bleeding, and mortality. 32 Improved safety and easier route of administration further support the use of DOACs over LMWH in patients treated with ICI.
This study demonstrates that there is a potential pathophysiological role for the coagulation pathway in cancer progression and tumor evasion by the immune system. However, it does have limitations that might narrow its scope. As a retrospective study, it was limited by documentation in the chart and physicians’ impressions of response rates. The study exclusively included patients with stage IV lung cancer; therefore, its generalizability to other cancers that utilize immunotherapy such as melanoma is uncertain. We acknowledge the selection bias introduced within the cohort due to the retrospective and single-center design of the study. In addition, we are not certain to what degree the variability in schedules of concomitant anticoagulation and ICI utilization for lung cancer might have impacted the results observed. The sample size was smaller than anticipated in the enoxaparin population because the hospital system primarily utilizes DOACs for management of and prophylaxis against thromboembolism in alignment with guidelines for cancer-associated VTE. The study was also not powered to detect a clinically significant difference in rates of 6-month PFS and OS given the small sample size. Nevertheless, improved PFS at 6 months has been shown to correlate with 12-month OS benefit in ICI clinical trials. 27 Lastly, the indications for anticoagulation were not balanced among the two treatment arms. A higher proportion of patients in Arm B received anticoagulation for VTE, which is associated with higher mortality, and this could have impacted PFS and OS. 33 However, we posit that our results would be hypothesis generating and relevant for future explorations in malignancies with higher incidences of thrombosis such as gastric and pancreatic cancer. Currently, larger, adequately powered, prospective trials are needed to assess the role of anticoagulation and in particular DOACs in augmenting ICI response and potentially overcoming resistance to therapy. Furthermore, future directions could examine other malignancies with high risk for thrombosis and evaluate the true difference in terms of ORR and PFS in cancer patients treated with concurrent ICI therapy and DOACs. Confirmation of an existent synergy between DOACs and ICI could reinforce the practice of prophylactic anticoagulation in solid tumors according to the Khorana predictive model. 13
Conclusion
In this retrospective cohort review of patients with advanced stage lung cancer who were on concurrent ICI therapy, the addition of a DOAC as compared to enoxaparin improved 6-month PFS with no additional safety concerns. To further elucidate the role of anticoagulants in augmenting immunotherapy response and improving PFS, larger, prospective trials with adequate power are needed.
Footnotes
Author contributions
KA established and supervised the project. SK, KA, and GU were involved in designing the project. SK collected the data, performed the analysis, and drafted the first draft of the manuscript. SK, KA, GU, and EHB discussed the results, interpretation of data, and approved the final version of the manuscript.
Consent to participate
The study was conducted in accordance with the Declaration of Helsinki and was approved by the Institutional Review Board of our institution (PRO00036412) on 9/19/2022, with the need for written informed consent waived.
Consent for publication
Not applicable.
Data availability
The datasets generated during and/or analyzed during the current study are not publicly available due to reasons of sensitivity but are available from the corresponding author on reasonable request and with permission from the Houston Methodist Hospital Institutional Review Board.
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Ethical considerations and informed consent statements
The study was conducted in accordance with the Declaration of Helsinki and was approved by the Institutional Review Board of Houston Methodist Hospital (PRO00036412) on 9/19/2022, with the need for written informed consent waived.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.