
Abstract
Background
Standard treatment for bone metastases is based on bisphosphonates such as zoledronic acid. The objective of this study was to evaluate the incidence of acute renal failure during treatment with Zoledronate and to analyze its correlated factors.
Materials and methods
This is a retrospective study carried out at the medical oncology department of Habib Bourguiba University Hospital in Sfax, between January 2022 and March 2022. The creatinine dosage was carried out using the Jaffe-type colorimetric method. Acute renal failure was defined by the Kidney disease Improving Global Outcomes criteria.
Results
48 patients were included. The average age was 56.9 ± 10.7 years with a sex ratio (M/F) equal to 0.5. The average weight of the patients was equal to 68.5 ± 16.4 kg. 62.5% of patients were followed for breast cancer, 12.5% had lung cancer and 12.5% had prostate adenocarcinoma. The mean serum creatinine before the start of treatment was equal to 74.3 ± 34.3 µmol/l 50.84 ± 0.11 mg/dl). The mean pre-therapeutic clearance was 94.1 ± 40.2 ml/min with 4 cases of moderate renal impairment (8.3%). Acute renal failure according to KDIGO during treatment with Zoledronic acid was observed in 9 cases (18.8%), thus requiring a dose reduction. Acute renal failure was significantly associated initial clearance <60 ml/min and low weight of 53.44 kg (p = 0.003 and p = 0.01 respectively), in multivariate analysis.
Conclusion
Our study concluded that factors associated with acute renal failure were low weight and clearance less than 60 ml/min.
Introduction
Since their discovery more than 5 decades ago, bisphosphonates have been used in the treatment of Paget's disease, malignant hypercalcemia, bone metastases and osteoporosis.1,2 These drugs have a primary role in maintaining bone density and contribute to serum calcium homeostasis in these pathological situations.2,3,4 They are incorporated into the bone matrix and absorbed by osteoclasts at resorption sites. They inhibit osteoclast activity and bone remodeling, increase bone mineral density and reduce bone mass loss and the risk of vertebral and non-vertebral fractures. 5 Currently, the standard treatment for bone metastases is based on intravenous bisphosphonates, including zoledronic acid. 6 Renal tolerance of zoledronic acid is a problem linked to its intrinsic toxicity and the cancer patient. 7 zoledronate more frequently induces tubular toxicity. The incidence of renal failure during Zoledronate varies between studies from 10 to 24%. 8 The objective of our study was to evaluate the incidence of acute renal failure during Zoledronate and to analyze the correlated factors.
Materials and methods
Study population
This is a retrospective study carried out at the medical oncology department of Habib Bourguiba University Hospital in Sfax, between January and March 2022.
All procedures performed in studies involving human participants were in accordance with the ethical standards of the institutional and the national research committee of Habib Bourguiba hospital and with the 1964 Helsinki Declaration and its later amendments or comparable ethical standards.
We included in this study patients with cancer confirmed by histological study who received treatment with zoledronate. We excluded from the study those whose medical records could not be used and patients who had not received treatment with zoledronate.
Data collection was done from patients’ medical records. Creatinine determination was carried out using the Jaffe colorimetric method. Estimation of glomerular filtration was made by calculating creatinine clearance using the MDRD (Modification of Diet in Renal Disease) formula. Acute renal failure was defined by the KDIGO (Kidney Disease Improving Global Outcomes) criteria as well as its severity. Acute renal failure is defined by an increase in creatinine of ≥1.5 times the baseline value.
Statistical study
The objective of our study was to evaluate the incidence of acute renal failure during Zoledronate and to analyze the correlated factors. We calculated the number of necessary subjects using the BiostaTGV software. We concluded that we need at least 45 patients to do adequate analysis.
The statistical study of the data was carried out using the SPSS software (Statistical Package for Social Science) in its 20th version of Windows. Quantitative variables were expressed as means plus or minus standard deviation (SD), and qualitative variables as numbers and percentages. The relationship between qualitative variables was evaluated by the Chi-square test (Chi2) and that between quantitative variables was studied by the Student test (t). The threshold of 0.05 was used to judge the significance of each test. We performed the logistic regression in the multivariate analysis to identify the factors associated with acute renal failure during Zoledronate administration. Therefore, we used the descending Wald method.
Results
Patient characteristics
48 patients were included. The average age of the patients was 56.9 ± 10.7 years with extremes ranging from 30 to 82 years. Patients aged less than 60 years represented 56.7% of cases (n = 27). Female patients represented 66.7% of cases (n = 32), the sex ratio was equal to 0.5. Four patients were hypertensive (8.3%) and two patients were diabetic (4.2%). The average weight of the patients was equal to 68.5 ± 16.4 kg with extremes ranging from 40 to 115 kg. 30 patients. 30 patients were followed for breast cancer, 6 had lung cancer and 6 had prostate adenocarcinoma. Forty-six patients had bone metastases. 2 patients received Zoledronic acid as an adjuvant in combination with Letrozole given the presence of osteoporosis. 41 of patients (85.5%) were treated with chemotherapy. Trastuzumab was indicated in 14.6% of cases. 16.7% of patients had received hormonal therapy.
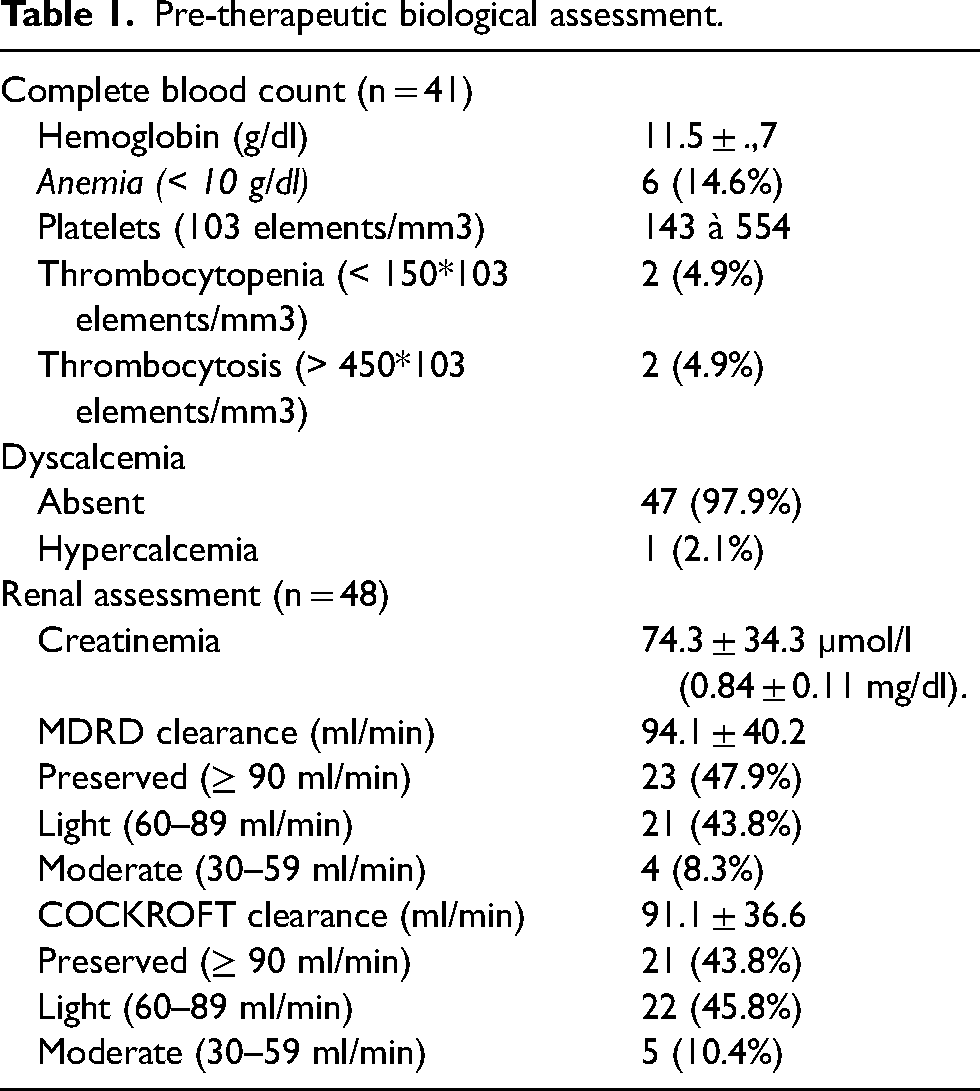
The mean hemoglobin value before the start of treatment was equal to 11.5 ± 1.7 g/dl with extremes ranging from 6 to 15.1 g/dl. The mean value of platelets before the start of treatment was equal to 276.48 ± 93.3 *103 elements/mm3 with extremes ranging from 143 to 554 *103 elements/mm3. One patient had hypercalcemia. The mean serum creatinine before the start of treatment was equal to 74.3 ± 34.3 µmol/l (0.84 ± 0.11 mg/dl). The mean pre-therapeutic MDRD clearance was equal to 94.1 ± 40.2 ml/min with 5 cases of moderate renal insufficiency (10.5%). Table 1 summarizes the pre-therapeutic biological assessment.
Pre-therapeutic biological assessment.
Zoledronate and acute renal failure
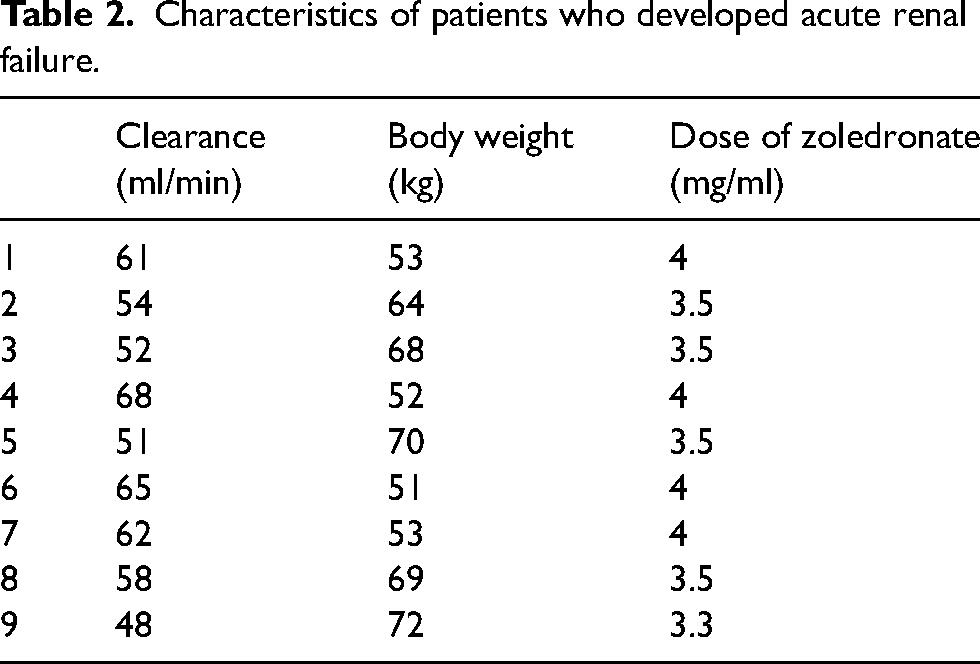
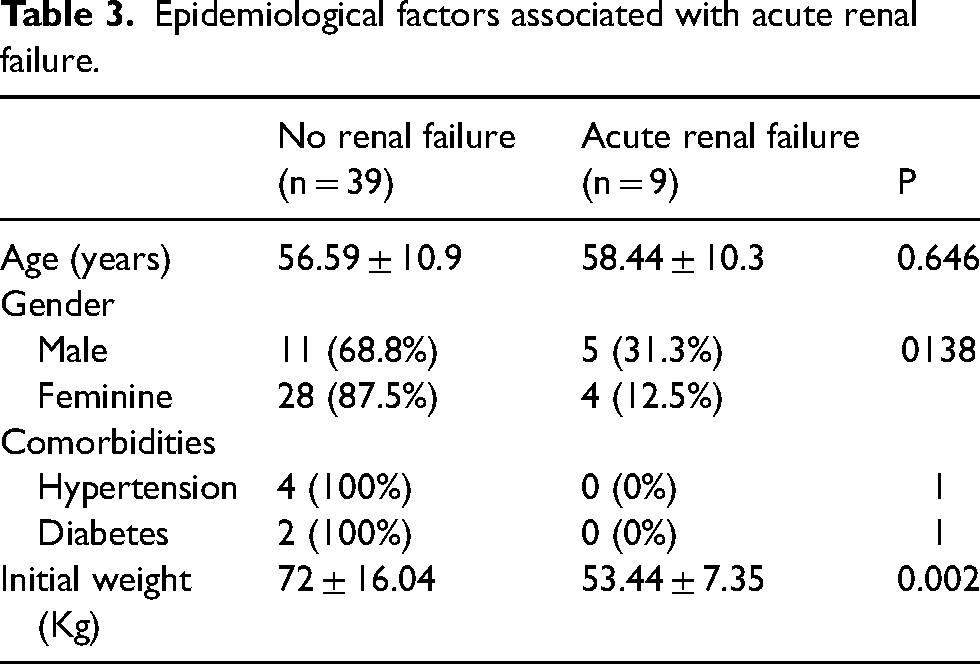
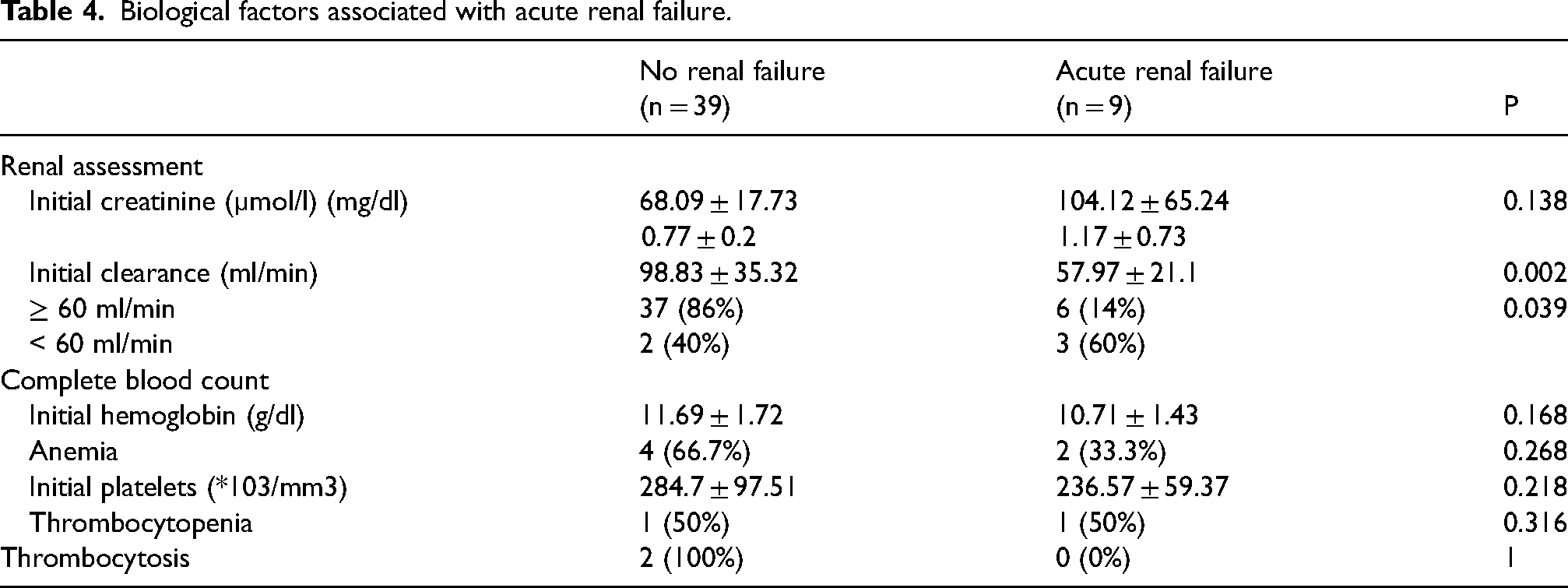
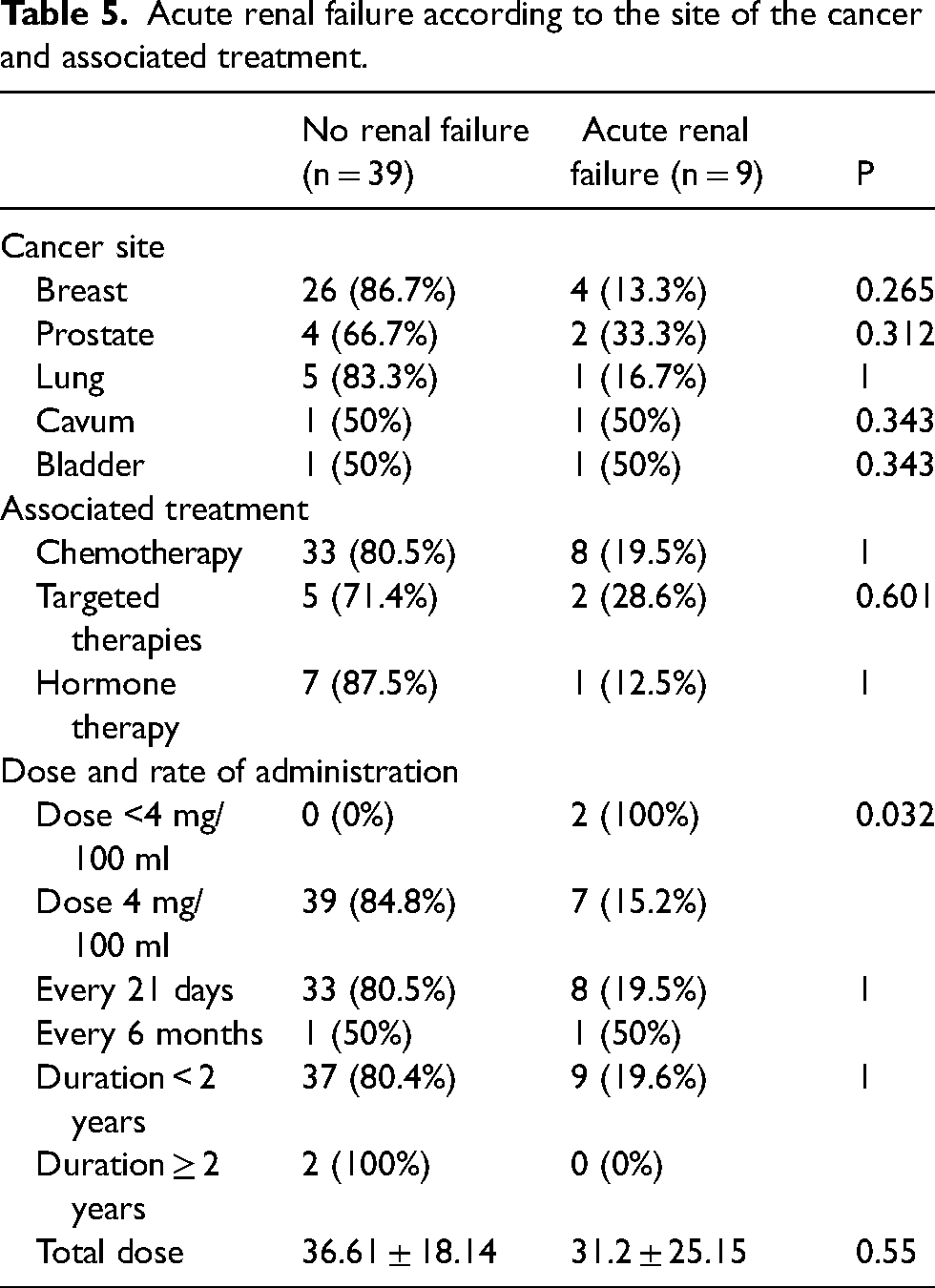
Five patients were treated with a dose of less than 4 mg/100 ml of Zoledronate (10.5%). The others were treated with a dose of 4 mg/100 ml (89.5%). The median cumulative dose was 30 mg (IQR = [24–48 mg]). Acute renal failure during Zoledronic acid was observed in 9 cases (18.8%) (Table 2), thus requiring a dose reduction. No cases of nephrotic syndrome or acute interstitial or tubulointerstitial nephropathy were observed. A single case of evolution to chronic renal failure was noted in a patient receiving Gemcitabine-Carboplatin-based chemotherapy for metastatic bladder cancer. Acute renal failure varied significantly depending on weight (p = 0.002), it was associated with a lower patient weight of 53.44 kg ± 7.35, initial clearance <60 ml/min (p = 0.002) and a dose of Zoledronate < 4 mg/100 ml (p = 0.032) (Table 3, 4, 5). In multivariate analysis, initial clearance <60 ml/min and lower weight were associated significantly with acute renal failure (p = 0.003 and p = 0.01 respectively).
Characteristics of patients who developed acute renal failure.
Epidemiological factors associated with acute renal failure.
Biological factors associated with acute renal failure.
Acute renal failure according to the site of the cancer and associated treatment.
Discussion
To the best of our knowledge, this is the first study of acute renal failure during zoledronate in Africa. Furthermore, there is no prospective data studying this entity in the overall literature. Our study concluded that the incidence of acute renal failure during zoledronate was 18.8%. Factors associated with this side effect were low weight and clearance less than 60 ml/min. In multivariate analysis we didn’t find the dose <4 mg/100 ml. This may be explained by a chance finding based on confounding by association of creatinine clearance < 60 mL/min being a risk factor for acute renal failure.
The incidence of renal failure during Zoledronate varies between studies from 10 to 24%. 8 In a recent published study, 9 the authors analyzed data from 3340 North American breast cancer patients and determined the frequency of occurrence of renal failure, defined as a decrease of 25% of the glomerular filtration rate estimated by the MDRD formula. This study included 3 groups: a group of patients treated with zoledronate (n = 312), a group of patients receiving pamidronate (n = 166), and a group of patients not treated with bisphosphonate (n = 2862). Patients in the zoledronate and pamidronate groups had comparable characteristics at inclusion and the frequency of occurrence of acute renal failure in these two groups was not statistically different: 24% and 27%, respectively. In the group of patients not receiving bisphosphonates, renal failure accounted for 14%.
In multivariate analysis, the risk of developing renal failure in patients with breast cancer receiving zoledronate or pamidronate was twice as high as for patients not receiving bisphosphonates.
In our series, acute renal failure according to KDIGO during treatment with Zoledronic acid (18.8%) required a dose reduction.
The individual risk of developing renal failure during treatment with Zoledronate depends on several patient-related factors 10 such as age over 65 years, the presence of diabetes or high blood pressure, the association with other nephrotoxic drugs, dehydration and pre-existing renal failure.
The treatment-related risk factors 11 are the total dose delivered, the duration of infusion and the number of infusions.
Although the risk is reduced by administering the dose of zoledronic acid over 15 min, impairment of renal function may occur. 11 Renal impairment, progression of renal failure and cases of dialysis have been reported in patients after an initial dose or a single dose of 4 mg Zoledronic acid. In a retrospective analysis of 3115 patients with myeloma and bone metastases from solid tumors who received Zoledronate, McDermott et al. reported worsening of renal function in 9.4% of patients. 12 Predictors of the development of renal deterioration included patient age > 60 years, number of doses administered > 4, current or previous use of cisplatin, and myeloma or renal cancer. In multivariate analysis, the cumulative dose of Zoledronate was an independent predictive factor for developing renal failure. 12 In our study, acute renal failure varied significantly depending on weight (p = 0.002), it was associated with a lower weight of patients 53.44 kg ± 7.35. It also varied significantly depending on initial clearance (p = 0.002). It was significantly more observed in cases of values lower than 60 ml/min (60% vs 14%; p = 0.039). Interestingly, we observed renal failure in the 5 patients treated at a dose < 4 mg/100 ml (p = 0.032). The result of this study shows different indications for zoledronic acid treatment (osteoporosis and bone metastasis). Zoledronate is administrated every 6 months in case of osteoporosis and every 21 days in case of bone metastasis. We didn’t find difference according indications. This may be explained by the low number of patients with osteoporosis included in our study. Our study has some limitations. On one hand, this is a retrospective study and on the other hand the number is limited. Prospective trials are necessary to confirm these results.
Footnotes
Acknowledgement
We acknowledge patients who participated in the study.
Author contribution
W. B K. idea, conception, analysis, M.B.A. data collection, A. K. supervision, revision.
All the authors reviewed the manuscript.
Competing interests
None.
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Ethics approval
All procedures performed in studies involving human participants were in accordance with the ethical standards of the institutional and the national research committee of Habib Bourguiba hospital and with the 1964 Helsinki Declaration and its later amendments or comparable ethical standards.
Funding
The authors have not declared a specific grant for this research from any funding agency in the public, commercial or not-for-profit sectors.
Patient consent for publication
Consent obtained directly from patient(s).
Provenance and peer review
Not commissioned; internally peer reviewed.