
Abstract
Daratumumab is a human IgG1κ monoclonal antibody targeting CD38, with infusion-related reactions occurring in 45–48% of patients. Among these, 5–10% are severe, requiring treatment discontinuation in 1% of cases. The incidence of hypersensitivity reactions (HSRs) to daratumumab is unknown. We describe a 37-year-old male diagnosed with POEMS syndrome and treated with autologous hematopoietic stem cell transplantation and chemotherapy. Presenting a relapse of the disease, intravenous daratumumab was initiated. Ten minutes after starting the first infusion, he presented with generalized rash, abdominal pain, vomiting, pharyngeal pruritus, throat tightness, dyspnea, decreased oxygen saturation, tachycardia and diaphoresis (Brown III). Due to the refractory disease and lack of alternatives, a desensitization protocol for daratumumab 1000 mg was implemented using a (3 bag-12 step) over 5.67 h. Eight successful desensitizations were performed without hypersensitivity reactions, enabling safe drug reintroduction. Currently, only one successful daratumumab desensitization protocol has been published, involving a 4-bag, 14-step procedure over 5.2 h, as reported by Carrón-Herrero et al. Prior to desensitization, the patient experienced flushing, pharyngeal pruritus, bronchospasm, dyspnea, desaturation, bradycardia, and hypotension. Both case reports were associated with severe anaphylaxis, ultimately enabling the safe reintroduction of the drug.
Introduction
Daratumumab, the first human IgG1κ monoclonal antibody directed against CD38-expressing cells inducing apoptosis, has been approved for use in the treatment of relapsed/refractory multiple myeloma (MM), light chain amyloidosis (LA) and other plasma cell dyscrasias. The use of daratumumab has shown significant improvement in progression-free survival and overall survival in these diseases. 1
POEMS syndrome is an acronym for polyradiculoneuropathy, organomegaly, endocrinopathy, monoclonal plasma cell disorder and skin changes. Also known as Takatsuki syndrome or Crow-Fukase syndrome, it is a rare and potentially fatal multisystemic disease affecting mostly middle-aged men. The prevalence remains uncertain; however, a national survey conducted in Japan in 2003 estimated it to be approximately 0.3 cases per 100,000 individuals. 2
Diagnostic criteria include two mandatory criteria: polyneuropathy (demyelinating) and monoclonal proliferative plasma cell disorder; major criteria: sclerotic bone lesions, Castleman's disease, elevated VEGF; and minor criteria: organomegaly, extravascular volume overload, endocrinopathy, skin changes, papilledema, thrombocytosis/polycythemia. 3 A diagnosis of POEMS syndrome requires the presence of two mandatory, one major and one minor criteria. 4
The treatment of localized disease (isolated bone lesion) is radiotherapy. Due to the rarity of the disease, there are no standardized guidelines for the treatment of disseminated disease. 4 MM therapeutic programs are implemented including chemotherapy with proteasome inhibitors and the use of monoclonal antibodies such as daratumumab. 2
The prevalence of HSRs to daratumumab have not been reported, however, severe infusion-related reactions (IRRs) have an incidence of 5–10%. 5 Desensitization is the procedure of inducting immunological tolerance to the drug in HSR to maintain the indicated therapy by gradually increasing doses. 6
Case description
We describe a 37-year-old male patient with a history of HIV, asthma, allergic rhinitis currently without allergy treatment, diagnosed with POEMS syndrome treated with autologous hematopoietic cell transplant and chemotherapy based on cyclophosphamide, bortezomib and dexamethasone, presenting a relapse of the disease for which daratumumab was started. In preparation for the first cycle with daratumumab IV the
Management & outcomes
Due to the refractoriness of the disease, it was decided to perform a desensitization protocol with daratumumab 1000 mg intravenous, with 3 bags – 12 steps in 5.67 h (Table 1), before starting the protocol the patient
3 bag −12 step desensitization protocol to Daratumumab.

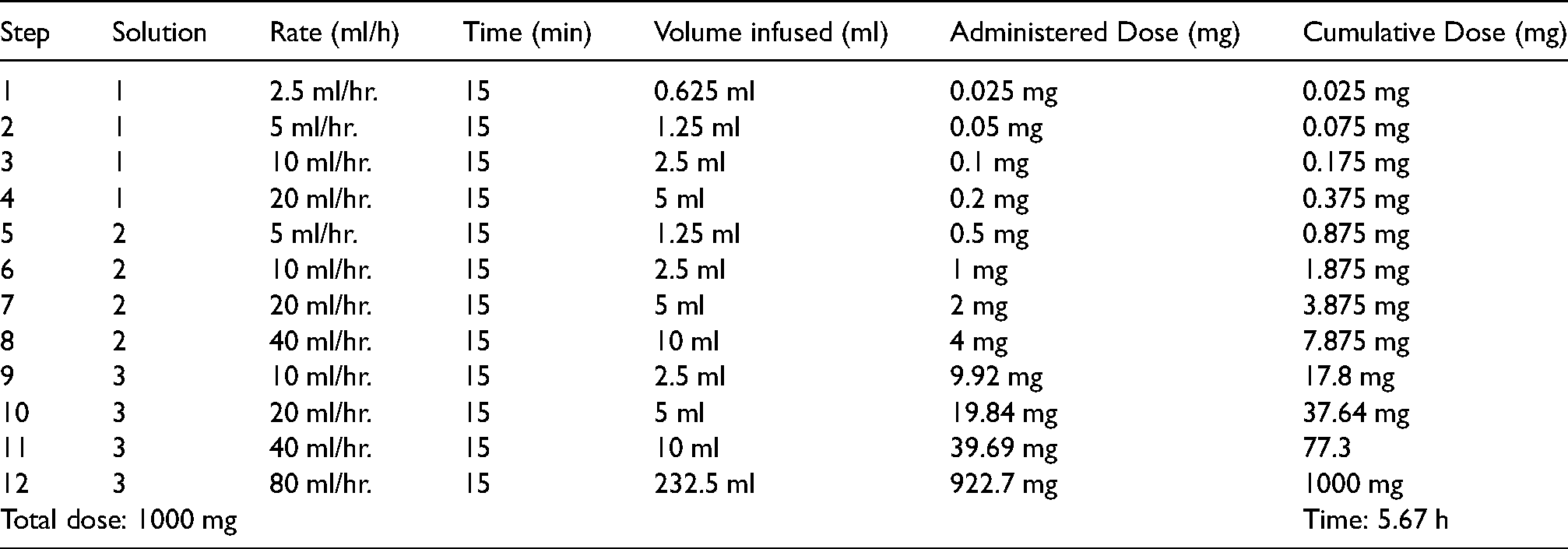
Eight successful desensitizations were performed in this patient, with no HSR. Treatment with daratumumab was used as conditioning treatment for autologous hematopoietic stem cell transplantation. To date, the patient
Discussion
Monoclonal antibody-induced hypersensitivity reactions (HSRs) occur mostly with an immediate IgE-mediated phenotype, non-IgE-mediated, cytokine-released, and mixed; and in few case reports as delayed hypersensitivity reactions type IV and type III vasculitis. 7 About 45–48% of patients treated with daratumumab intravenous have IRRs, 90% were limited to the first infusion, 1% required discontinuation of treatment. IRRs can range from mild to severe: nasal congestion, throat irritation, cough, chills, nausea and vomiting; and severe symptoms such as bronchospasm, dyspnea, hypoxia, hypertension, laryngeal and pulmonary edema. 8
The actual prevalence of HSR to daratumumab has not been reported, however, severe IRRs are known to have an incidence of 5–10%. 5 IRR and cytokine release syndrome (CRPS) usually occur at the first infusion, the main difference between these is the self-limitation of IRR on repeated exposures and adequate response to premedication. 9
Patient-related factors have been identified as possible risk factors for daratumumab-induced HSR such as previous exposure to monoclonal antibodies like bortezomib (risk of cross-reactivity) or concurrent medication and factors related to current treatment such as infusion rate and cumulative dose.5,10
Premedication is usually administered one hour before each infusion to prevent the development of IRR. Drugs used in premedication include long-acting corticosteroid administered intravenously
A report of desensitization to daratumumab using 4 solutions and 14 steps is described in the literature. 6 In our patient, a rapid desensitization protocol with 3 solutions – 12 steps was implemented allowing continuation of first-line treatment.
No type I hypersensitivity reactions to daratumumab have been documented to date, and in this case skin testing demonstrated the absence of an IgE-mediated hypersensitivity response. Due to the clinical characteristics presented, it is suspected that the underlying mechanism of HSR in this patient corresponds to a cytokine release syndrome, so due to the refractoriness of the disease and not having a therapeutic alternative, the patient benefits from a rapid desensitization protocol to daratumumab to achieve the reintroduction of the drug
Footnotes
Abbreviations
Author's contributions
RVG design of the work. RVG, NFG and DCG analysis and interpretation of data. RVG, NFG, DCG, AGL, RPR and OVG drafting, performed critical analysis and review.
Consent for publication
Written and informed consent for publication was obtained from the patient. The patient was informed that de-identified data would be used in scientific research and publications.
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.