
Abstract
Acute erythroid leukemia treatment is associated with poor survival. The most common treatments are intensive chemotherapy regimens and hypomethylating agents. Choice of preferred therapy is complex, and data are conflicting on the optimal regimen. The definition of AEL has also shifted with time but the impacts of these changes on survival reporting are largely unknown.
We designed a single-center, retrospective review of patients meeting the 2001 World Health Organization definition of acute erythroid leukemia. Patients were treated with an intensive chemotherapy or a hypomethylating agent regimen. The primary outcome was overall survival.
Most patients were older with complex karyotypes. Median overall survival did not differ between treatment groups. When survival was stratified by WHO 2022 diagnosis, patients meeting MDS criteria had notably increased survival outcomes while patients still meeting the definition of AEL did poorly regardless of induction regimen.
Treatment of acute erythroid leukemia remains complex with poor survival outcomes.
Introduction
Acute erythroid leukemia (AEL) is a rare subtype of acute myeloid leukemia (AML) that accounts for less than 1% of AML cases. 1 Historically, the French-American-British (FAB) Group classified AEL as AML-M6, requiring erythroid cell predominance among total cells and at least 30% myeloid blasts among non-erythroid cells. 2 The World Health Organization (WHO) developed criteria of their own in 2001 and established subclassifications of pure erythroid leukemia (PEL) and erythroid/myeloid AEL. 2 This definition mirrored the original FAB criteria but required a lower threshold of 20% myeloid blasts among non-erythroid cells. 2 Subsequent updates saw the removal of the erythroid/myeloid subtype and led to many cases being reclassified to either myelodysplastic syndrome (MDS) or AML, not otherwise specified (AML-NOS).3,4,5 The 5th edition of the WHO definitions classifies AEL, now interchangeably referred to as PEL in this edition, as a distinct type of AML and removes the AML-NOS classification in favor of AML, defined by differentiation which includes AEL. 2 AEL is characterized by erythroid predominance with more than 80% of bone marrow elements (of which at least 30% are proerythroblasts) and high rates of biallelic TP53 alterations.2,6,7 By contrast, the 2022 International Consensus Classification (ICC) includes PEL under a broader category of AML with mutated TP53. 8 For consistency, we used PEL to refer to patients meeting the definition of pure erythroid leukemia based upon the WHO 2001 criteria and AEL will refer to patients meeting the WHO 2022 criteria for AEL. For patients that were classified as an AEL in 2001 that were since reclassified, these are noted to be an AEL based upon the 2001 criteria only.
AEL has traditionally been associated with poor outcomes overall and no standard therapy has been established.9–15 The data regarding the optimal treatment strategy have been mixed, due to differences in patient characteristics, response definitions, and AEL diagnostic criteria changing over time. Several studies have suggested more favorable outcomes associated with the use of a hypomethylating agent (HMA) compared to traditional intensive chemotherapy. An initial retrospective review from our center found favorable outcomes for patients receiving decitabine based treatment for AEL. 10 Another multinational retrospective study found improved response rates and longer survival time for patients receiving HMA therapy. 11 While the role of HMA therapy seems promising overall, there are data to suggest limited benefit as well, which complicates their place in therapy.12,13 Given the mixed literature to date, which may be impacted by differences in AEL diagnostic criteria, we sought to assess the impact of HMA-based therapy and disease classification on outcomes in patients diagnosed with AEL.
Methods
We conducted a single-center, retrospective cohort study. Patients were included if they were 18 years of age or older, met 2001 WHO criteria for a diagnosis of AEL—erythroid/myeloid or PEL, and received induction therapy at our institution between January 1st, 2001 and December 31st, 2022. Patients were excluded if they received therapy with an investigational agent or if therapy was initiated outside of the institution. Patients were separated into two cohorts based upon the regimen they received. The hypomethylating agent cohort consisted of patients who received induction therapy containing either azacitidine or decitabine. The intensive chemotherapy (IC) group consistent of patients who received an induction regimen utilizing high-intensity chemotherapy, such as high-dose cytarabine (e.g., fludarabine, cytarabine, granulocyte colony stimulating factor (FLAG)) or anthracycline containing regimens (e.g., daunorubicin and cytarabine in traditional “3 + 7” fashion).
Patient data were collected via manual chart review of the electronic health record (EHR). Baseline characteristics included age, gender, bone marrow or peripheral blast % at diagnosis, cytogenetics, molecular mutations, the presence of TP53 alterations, and induction regimen.
The primary endpoint of the study was the difference in median overall survival (OS) between patients treated with HMAs compared to IC, when defining AEL using the most recent, WHO 2022 criteria. Secondary outcomes included progression-free survival, overall response rate (ORR), classification of disease based on WHO definitions from 2001 and 2022, and the impact of the revision of the classification on treatment outcomes. The Kaplan-Meier method was employed to estimate overall survival and progression-free survival, with a log-rank test to compare the two groups. ORR was defined as the complete response (CR) rate plus complete response with incomplete count recovery (CRi), as defined by Cheson criteria. Continuous data were compared utilizing either an independent t-test or Mann-Whitney test depending on the normality of the data. Nominal data were compared utilizing the chi-square test or Fischer's exact test as appropriate.
Results
A total of 146 patients diagnosed with AEL between January 2001 and December 2022 were identified. After excluding 115 patients (Figure 1) a final cohort of 31 patients with an AEL based on the WHO 2001 criteria were included in the study. Of the 18 patients included in the HMA cohort, only 2 received venetoclax as part of their induction regimen.
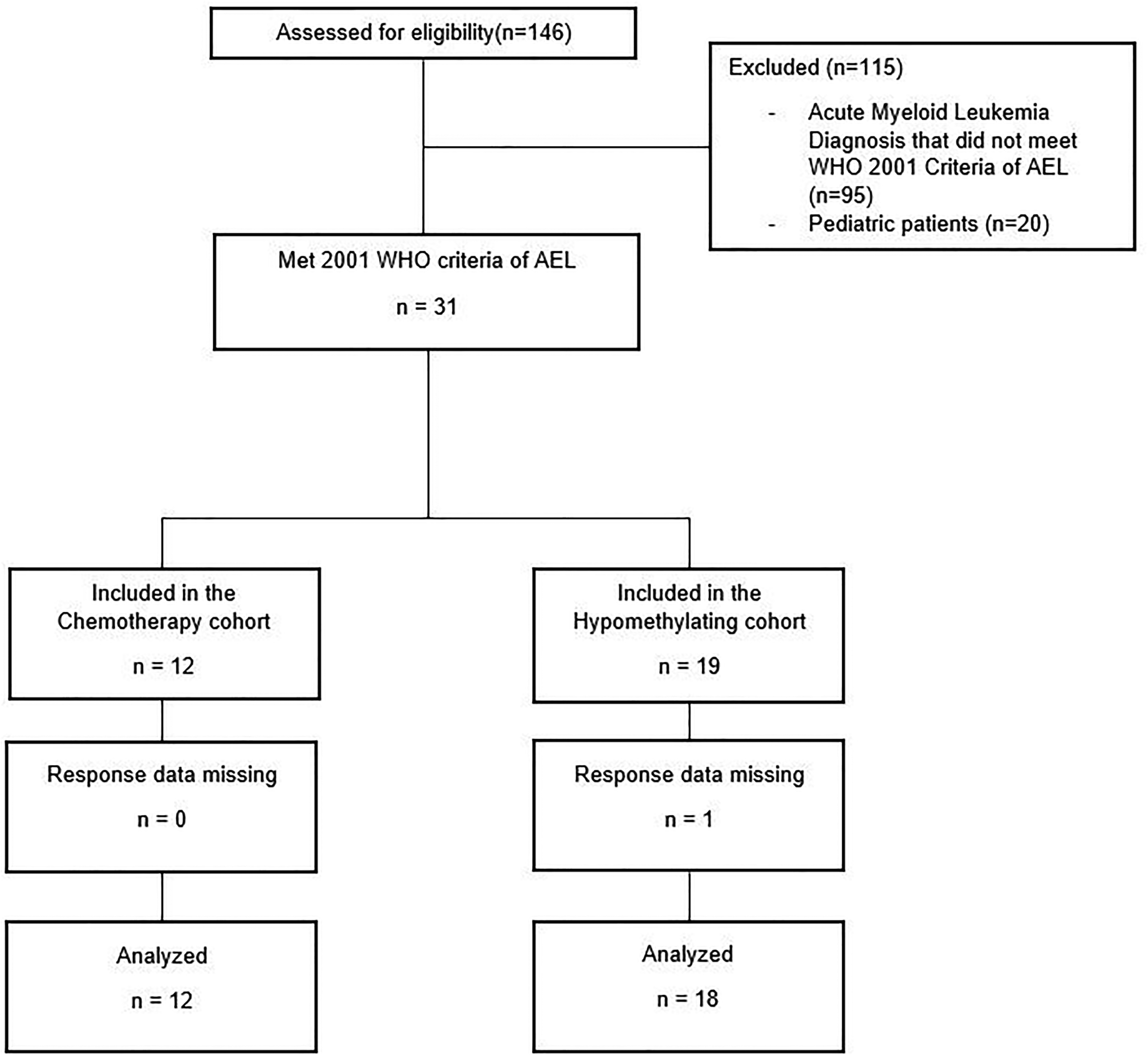
Consort diagram of eligible patients and how patients were categorized once included in the study. WHO = World Health Organization, AEL = Acute Erythroid Leukemia.
According to the 2016 criteria, most patients were reclassified as having MDS. By utilizing the updated 2022 WHO criteria, 4 patients were classified as having AML, 10 patients met the criteria for AEL, and the remaining 16 patients were classified as having MDS (Figure 2). Baseline characteristics of the two cohorts did not exhibit significant differences, as shown in Table 1.
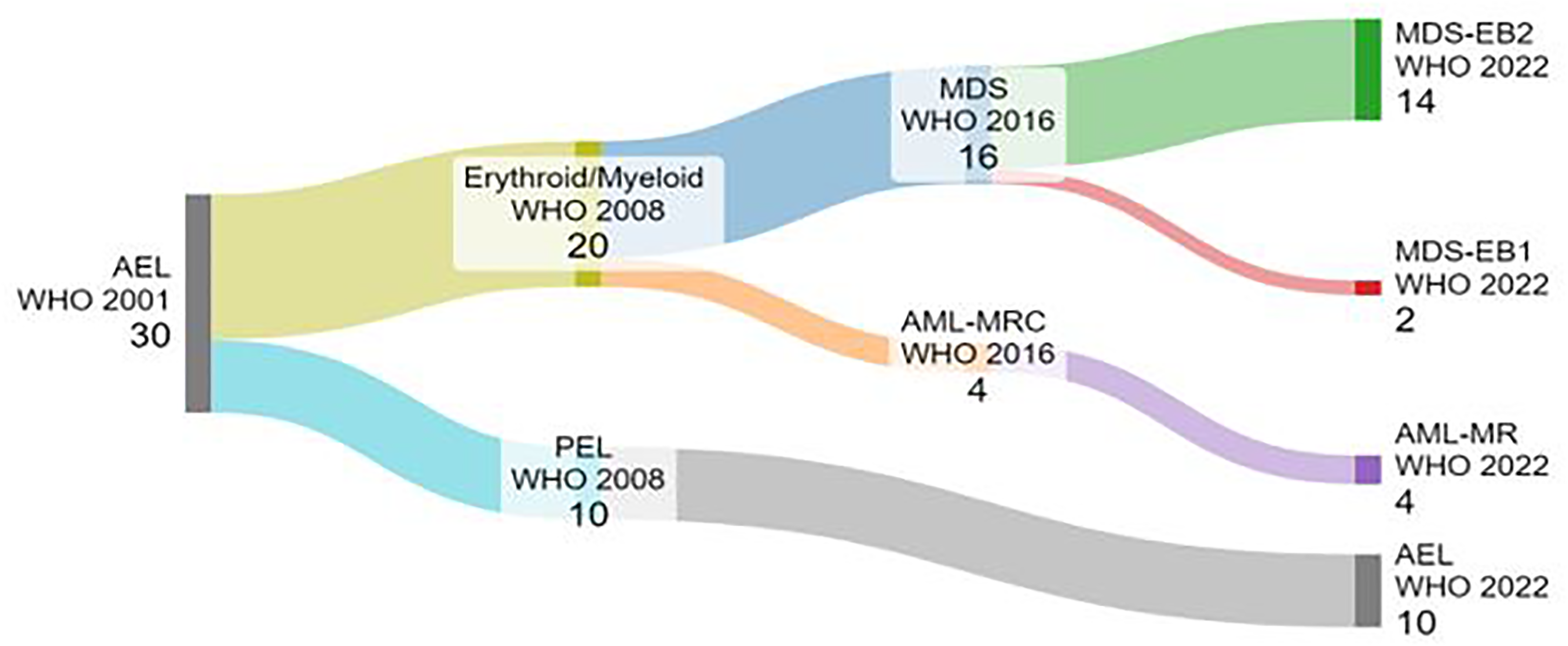
(Color): Sankey diagram illustrating the classification of patients through the various definition changes of acute erythroid leukemia by the World Health Organization (WHO). AEL = Acute Erythroid Leukemia, PEL = Pure Erythroid Leukemia, MDS = Myelodysplastic Syndrome, AML-MRC = Acute Myeloid Leukemia with Myelodysplastic Changes, AML-MR = AML myelodysplasia-related, MDS-EB1 = Myelodysplastic Neoplasms with Elevated Blasts 1, MDS-EB2 = Myelodysplastic Neoplasms with Elevated Blasts 2. Made at SankeyMATIC.com.
Baseline characteristics.
The primary endpoint, median overall survival (Figure 3A) showed no statistically significant difference between HMA and IC induction regimens (HMA 12.5 months [95% CI 0.00–30.233] vs. IC 6.2 months [95%CI 2.81–9.60, p = 0.289]). Similarly, progression-free survival (Figure 3B
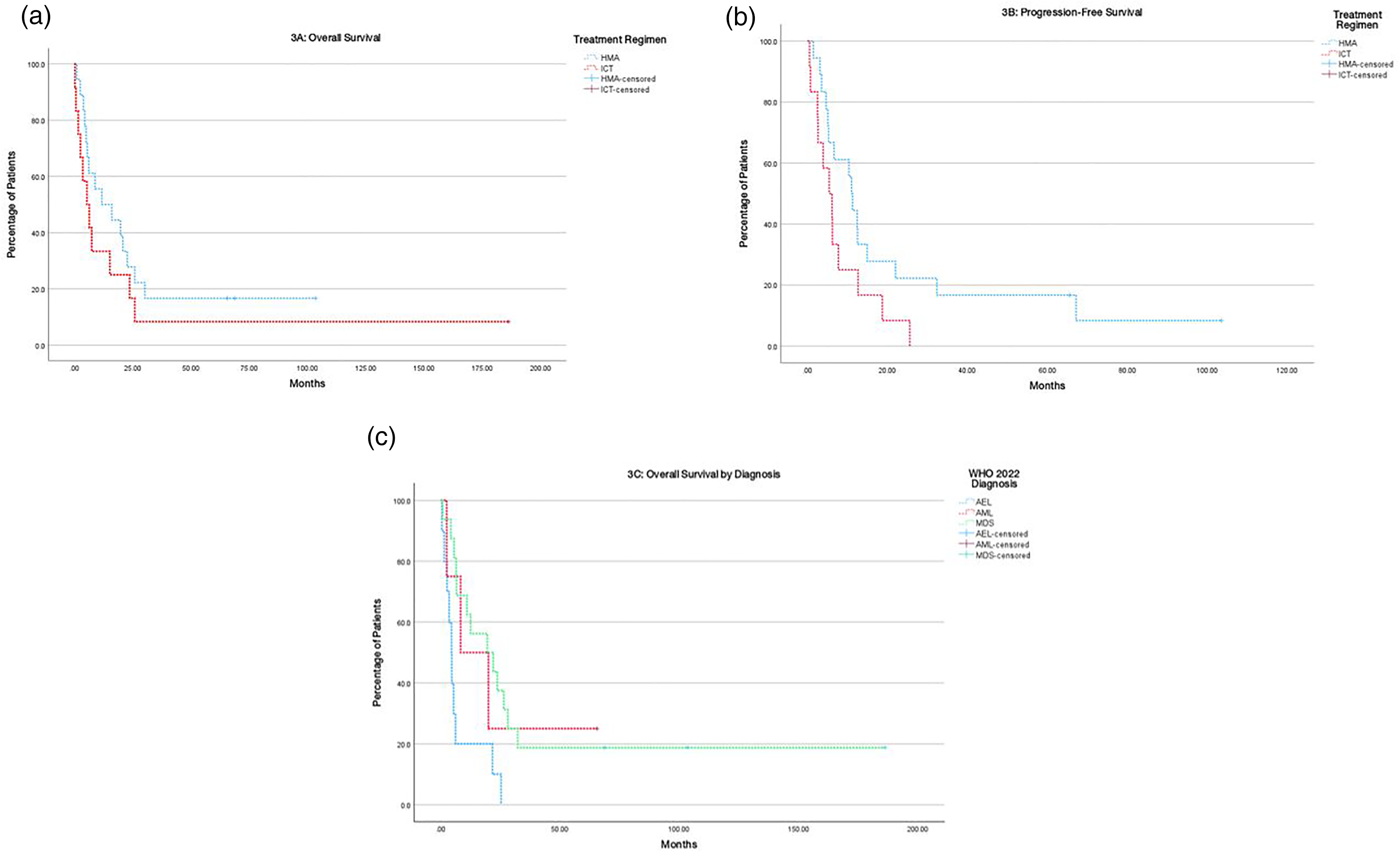
(A): Overall survival for patients treated with a hypomethylating agent based regimen compared to patients treated with intensive chemotherapy regimens. Hypomethylating agent (HMA). Intensive chemotherapy (ICT). (B): Progression-free survival for patients treated with a hypomethylating agent based regimen compared to patients treated with intensive chemotherapy regimens. Hypomethylating agent (HMA). Intensive chemotherapy (ICT). (C): Overall survival for patients based upon their updated WHO 2022 classification. Hypomethylating agent (HMA). Intensive chemotherapy (ICT).
OS was analyzed according to reclassification by WHO 2022 criteria, and a significant difference was noted between the three diagnostic categories (Figure 3C). Patients classified as having AML had a median overall survival of 8.37 months (95% CI 0.00–25.49), while those with AEL had a median overall survival of 4.5 months (95% CI 2.75–6.25), and MDS had a median overall survival of 19.53 months (95% CI 0.85–38.21, p = 0.015). 16 patients were classified as having MDS, 11 of which were treated with a hypomethylating agent (68.75%). Median overall survival of patients classified as having MDS and treated with an HMA was 19.53 months compared to 22.03 months for patients treated with IC and meeting the definition of MDS. 10 patients met the definition of AEL with half the subgroup treated with HMA based therapy and the other half IC based regimens. Overall survival for this subpopulation was 4.63 months for the HMA cohort and 4.5 months for those treated with IC. 60-day mortality rate was 10% for the overall study population. When comparing cohorts, 60-day mortality rates were 16.67% for patients treated with IC induction compared to 5.56% for patients receiving HMA based induction treatment.
Overall response rates (ORR) were similar between the two treatment groups. In patients treated with a hypomethylating agent, the ORR was 67.7%, while it was 58.3% for those that received intensive induction therapy. Complete response occurred in 27.8% of the HMA cohort vs. 25% of the IC group (CR/CRi 50% vs. 50%). When stratifying the results by disease response, it was observed that patients who achieved a CR exhibited the longest median overall survival of 26.43 months compared to patients with a CRi who had a median overall survival of 21.67 months. However, partial responders and individuals with resistant disease had much worse prognosis with median survival times of 5.4 months and 4.63 months, respectively. Patients that proceeded to allo-HCT had a 64.29% CR/CRi rate and an ORR of 71.43% prior to transplant while patients that did not receive a transplant had a 42.86% CR/CRi rate and an ORR of 64.29%. Notably, two patients in the no transplant cohort had incomplete response data and were not included in the calculation of response rate for this group.
Discussion
In our study, the use of HMAs for the treatment of an AEL (based on the WHO 2001 criteria) resulted in a numerical but not statistically significant improvement in OS in comparison to patients receiving IC regimens. Due to the rarity of AEL as a disease and updated/changing definitions, it is unlikely for a study to truly be adequately powered to detect a difference in survival outcomes. It was determined to achieve a power of 80% with an alpha of 0.05 and a beta of 0.2, 64 subjects would have been needed in each group for a total of 128 patients. Our data suggesting possibly improved outcomes with HMA over IC is in concordance with the study by Almeida et al.; however, there may be additional factors at play. 11 First, the possible disparity in baseline characteristics and potential selection bias between HMA-treated and IC-treated patients could have influenced the results. In general, IC is selected for younger, healthier patients with a better baseline prognosis who may also be candidates for additional therapies such as allo-HCT. Second, and most importantly, the evolving definition of AEL may have had an impact on both our findings and the interpretations of past literature.
Patients initially diagnosed with PEL based on WHO 2001 were later reclassified as having Myelodysplastic Syndromes (MDS) using the WHO criteria from 2022 were more likely to receive HMA-based therapy. As MDS typically has a better prognosis than PEL, this could skew results when comparing HMA and IC regimens.13,14 This is an important distinction as these patients may have had less aggressive disease which may have led to the numerical difference seen in median overall survival between the two cohorts. CR/Cri rates were slightly higher in the HMA cohort compared to the CR/Cri rate reported by Almeida et al.. 11 This difference may be due to our organization's practice of using 10-day decitabine in therapy vs. the traditional 5-day decitabine regimens or 7-day azacytidine. Exposing these patients to an extended treatment timeline with decitabine may have led to numerically improved CR/CRi rates. 60-day mortality rates appeared to numerically favor HMA induction but our population's small sample size, difference in baseline disease, and genetic variability likely had an impact on this variable as well.
Receipt of a transplant was not significantly associated with enhanced survival outcomes but had a large numerical difference favoring transplant which is similar to the outcomes reported by Badar, et. Al. 14 This is likely explained by the small study population as there was a notable numerical difference between patients that did and did not go to transplant. It must be noted that these patients tend to be in a CR following induction, are generally younger at baseline, and tend to be a fitter patient population. Similarly, our patient population that proceeded to transplant had a higher rate of CR/CRi after induction. The inherent selection bias in choosing candidates for allo-HCT, both in our study and in previous literature, precludes drawing definitive conclusions regarding whether allo-HCT improves outcomes for patients with AEL.
The classification of AEL has recently become more complex with revisions to the WHO's myeloid disease definitions. As of 2022, the definition of AEL has evolved to closely mirror what was traditionally classified as PEL. Many patients formerly diagnosed as having AEL—erythroid/myeloid subtype based on the 2001 or 2008 WHO criteria have since been reclassified into MDS, AML, Not Otherwise Specified (AML-NOS), or AML, defined by differentiation depending on the classification system applied. There is a distinct difference in survival outcomes between these disease states and previously reported survival metrics could be altered significantly if these new criteria were applied to historical cohorts. Patients in our cohort who met the definition of MDS had relatively better outcomes, and treatment with an HMA remains a viable option. Future classifications may need to incorporate more robust genetics in their inclusion criteria, as suggested by more recent publications.16,17
Patients that meet the most recent definition of AEL (historically termed PEL) tend to have a high rate of TP53 abnormalities, complex karyotype, and poor prognosis overall. PEL has historically accounted for only 10% of AEL meeting FAB criteria; however, we observed a significantly higher rate of 33.3% in our study population.1–11 This could be because of the unique population we see at our institution as a referral center. Otherwise, our patient population is similar to the characteristics identified by Reichard et al. with a male predominance, high incidence of complex karyotype, and a median age greater than 65. 13 Consistent with previous literature, our study found that those classified under the 2022 WHO criteria for AEL had significantly worse survival outcomes. Notably, only 2 patients received concurrent venetoclax in our study. This likely can be attributed to the time period of the study, with the majority of patients collected prior to venetoclax's approval in 2016. These patient outcomes did not differ significantly from the other patients included in the HMA cohort with similar rates of response and survival. Historically, venetoclax has performed poorly in TP53 mutated AML and we anticipate that we could see similar poor outcomes with AEL given the predominance of TP53 mutated disease.18,19 Future treatments should focus on novel target pathways, like the anti-CD47 monoclonal antibody magrolimab, or mechanisms designed to circumvent TP53 abnormalities as this appears to be a large driver in the poor outcomes seen with AEL.20–22
This study is not without limitations. First, we are limited by the retrospective nature of this study and sample size of our population. Additionally, we are limited to pathology reports at the time which appeared to shift in focus on what was described in the reports. Earlier reports appeared to focus on “erythroid precursors” as WHO criteria was less specific in the type of erythroid cell required for diagnosis. As WHO criteria evolved, so too did the reporting in our pathology department with more descriptive measures of proerythroblasts specifically. Because of this limitation, applying WHO 2022 and 2016 criteria to patients treated prior to 2016 was difficult. We decided to include patients in the PEL cohort if their reported marrow components were at least 80% erythroid precursors as this was the best estimate available for patients that did not have proerythroblasts highlighted in their marrow reports. While this was noted as a limitation, patients classified as PEL in our study still had significantly worse outcomes which is consistent with previous literature.
Conclusion
Treatment of AEL remains an area for improvement and further clinical investigation with many patients having poor outcomes regardless of choice of intensive chemotherapy or reduced intensity regimens such as hypomethylating agents. Historical outcomes with AEL may have benefited from including patients that have since been reclassified as having MDS as these patients tend to have better outcomes than patients that meet the updated definition of modern AEL.
Footnotes
Author contribution statement
TG assisted with the design the research study, collected and analyzed data, and drafted the manuscript.
BM generated the research idea, designed the research study, analyzed data, and reviewed and edited the paper. KM analyzed data and reviewed and edited the paper. LB designed the research study and reviewed and edited the paper. MF designed the research study and reviewed and edited the paper. DB reviewed and edited the paper. KP reviewed and edited the paper. PB reviewed and edited the paper. AP generated the research idea, designed the research study, analyzed data, and reviewed and edited the paper.
Data availability statement
All data generated or analyzed during this study are included in this manuscript [and its supplementary information files].
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Ethical approval
The study was conducted in accordance with the Declaration of Helsinki and was approved by the Ethics Committee of University of Michigan Health—Michigan Medicine (HUM00226999) on November 29, 2022 with the need for written informed consent waived.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.