
Abstract
Introduction
Lenalidomide is dispensed through a limited distribution network, leading to longer prescription fill times. Acquiring lenalidomide involves navigating the risk evaluation and mitigation strategies (REMS) program, insurance prior authorization, and financial assistance for out-of-pocket costs. Health disparities, including socioeconomic status, health literacy, language barriers, and geography, can further delay access. This study aimed to identify and analyze factors contributing to delays in access to lenalidomide.
Methods
This retrospective study used electronic health records within the Brown University Health system to identify adults newly diagnosed with hematologic malignancies between June 1, 2019 and June 1, 2024, with a lenalidomide prescription. A stepwise multiple linear regression evaluated factors affecting dispensation time. The primary endpoint was to identify factors contributing to delays in lenalidomide acquisition from a health equity perspective. The secondary endpoint was to determine the median time from prescription generation to dispensation.
Results
We included 328 patients with a mean age of 71 years; 53% were male and 80% were White. Comorbidities included cardiovascular disease (53%), diabetes (15%), obesity (21%), respiratory disease (8%), and chronic kidney disease (7%). Eighteen percent of patients required transportation assistance. The primary endpoint revealed 54% required financial assistance, which was associated with delayed lenalidomide dispensation (P < 0.05). The secondary endpoint showed a median time of 8 days (IQR, 5–14) to dispense the prescription.
Conclusion
This study found that lenalidomide prescriptions took a median of 8 days to fill, with those requiring financial assistance experiencing longer delays. These findings suggest that insurance processes and health disparities hinder timely access.
Introduction
Lenalidomide, an oral anti-cancer medication, has improved survival outcomes for patients with multiple myeloma (MM) and other hematologic malignancies.1,2 Most oral anti-cancer medications are categorized as specialty medications and are associated with complex treatment regimens, higher costs, and special handling and administration requirements. Manufacturers often adopt limited distribution networks to ensure safe drug delivery and optimal patient outcomes through high-touch support. 3
The restricted distribution and teratogenic risk of lenalidomide necessitates adherence to the risk evaluation and mitigation strategy (REMS) program, which limits prescriptions to a four-week supply with no refills. Additionally, it restricts dispensing to contracted specialty pharmacies only, resulting in longer prescription fulfillment times.4,5 Furthermore, oral anti-cancer medications like lenalidomide commonly require prior authorization by insurance companies. Patients without health insurance or those with high copays require financial assistance to cover out-of-pocket costs, presenting additional barriers to treatment initiation. 6
Beyond operational challenges, health disparities persist among various patient populations, exacerbated by factors such as socioeconomic status, health literacy, language barriers, and geographic location. The American Society of Clinical Oncology (ASCO) has urged action to promote health equity across all patient demographics, highlighting the need to address disparities related to race, ethnicity, geography, and other sociodemographic factors. 7 The impact of these health equity factors on timely access to medications within limited distribution networks remains underexplored. 8 This study aimed to identify and analyze health equity factors that contribute to delays in acquiring lenalidomide within limited distribution networks.
Brown University Health (BUH) has developed and implemented an in-house medication workflow to streamline the dispensing process for lenalidomide (Figure 1). The process begins when the provider orders the lenalidomide prescription through the electronic health record (EHR) and notifies both the nurse navigator and pharmacy liaison about the new prescription. The nurse navigator obtains the necessary Celgene authorization number and records it in the patient's chart. Simultaneously, the pharmacy liaison initiates the process by working on prior authorization (PA) requirements and providing financial assistance, if necessary. If the PA is denied, providers may appeal. If the appeal is denied, providers may pursue access through the manufacturer assistance program. Once the PA, funding, or provider's appeal is approved, a dose check is sent to the BUH pharmacy clinical specialist to review the prescription for clinical appropriateness. The prescription is then routed by the pharmacy liaison to the provider for signature, with the dispensing pharmacy attached. The pharmacy liaison verifies start date and receipt of prescription with the patient and confirms delivery date with the pharmacy.
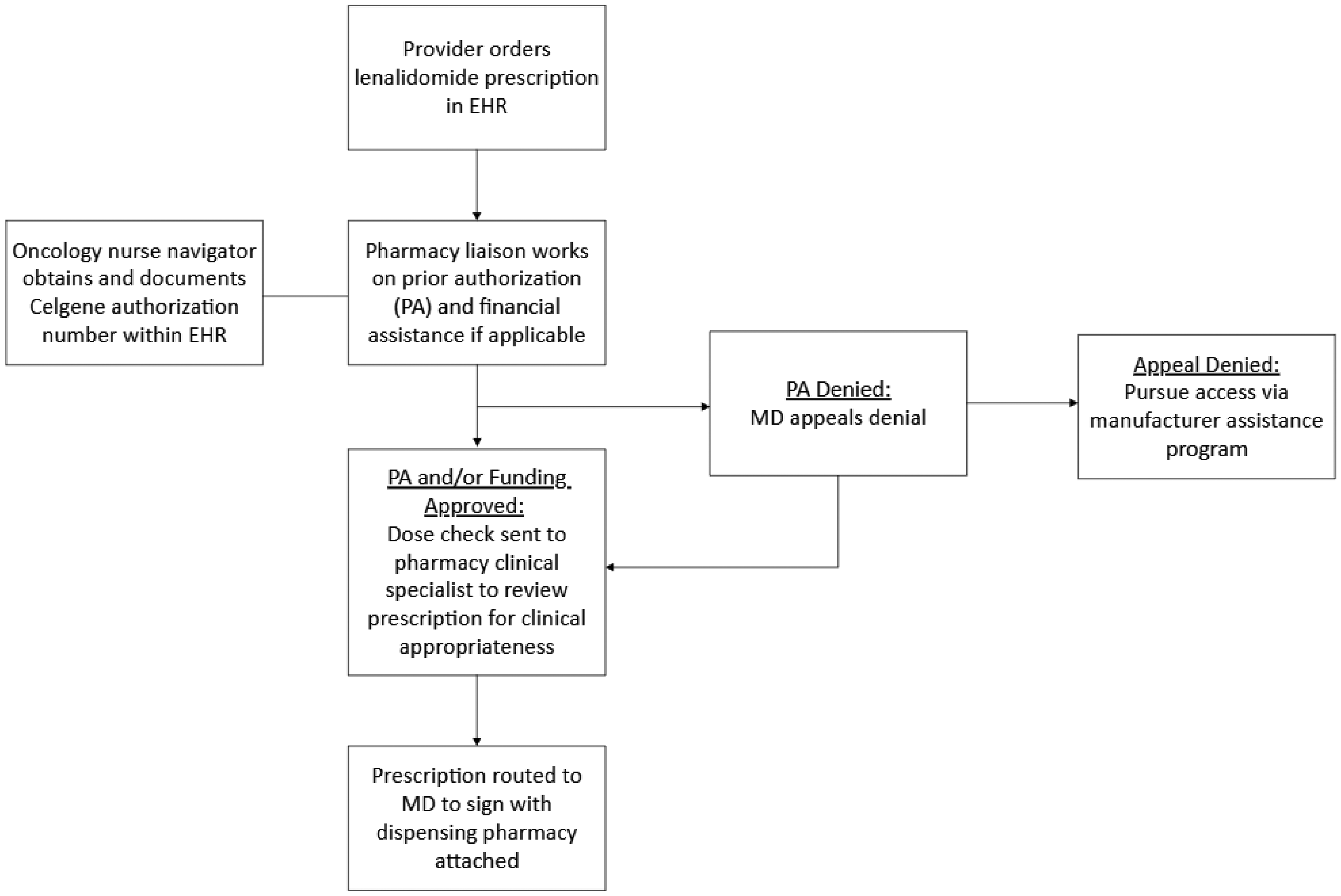
Lenalidomide acquisition process at Brown University Health.
Since the BUH specialty pharmacy is not certified with the lenalidomide REMS program, prescriptions are sent to a REMS-certified external pharmacy for dispensing. Upon receipt, the external pharmacy verifies the Celgene authorization number and obtains a pharmacy authorization number before proceeding with dispensing. The external pharmacy will call the patient to arrange delivery and provide counseling about lenalidomide.
Methods
This IRB-approved, retrospective study took place at the Brown University Health system. The study was conducted in accordance with the Declaration of Helsinki and was approved by the institutional review boards of BUH with an exemption for informed consent.
The study included adult patients with newly diagnosed MM, follicular lymphoma, marginal zone lymphoma, mantle cell lymphoma, myelodysplastic syndromes, or other hematologic malignancies between June 1, 2019 and June 1, 2024, who had a lenalidomide prescription written by a BUH provider. Patients were excluded if they were younger than 18 years of age, prescribed lenalidomide by an outside provider, did not initiate treatment after receiving the medication, or were enrolled in an investigational trial.
Comprehensive data was collected for each patient, including age, sex assigned at birth, sexual orientation, gender identity, and race. Additionally, relevant comorbidities were recorded, including cardiovascular disease (defined as heart failure, hypertension, hyperlipidemia, coronary artery disease, and stroke), type 1 and type 2 diabetes mellitus, obesity, respiratory diseases (chronic obstruction pulmonary disease, asthma), and chronic kidney disease. Socioeconomic factors such as education level, marital status, employment status, primary language, need for an interpreter, transport requirements, and financial assistance requirements were also captured. Lenalidomide prescriptions were fulfilled through a contracted specialty pharmacy within the limited distribution network or directly from the drug manufacturer via a patient assistance program (PAP). All information was retrieved from our institution's EHR application. Prescription refill information was also cross-referenced with the patient's medication chart to resolve any discrepancies in dispensing records.
The primary endpoint was to identify factors contributing to delays in lenalidomide acquisition. The secondary endpoint of this study was to determine the median time from lenalidomide prescription generation to dispensation. A stepwise multiple linear regression model was completed to evaluate the effects of health equity factors on time to dispensation.
Results
Patients
Between June 1, 2019 and June 1, 2024, a total of 810 patients prescribed lenalidomide were identified. Of these, 328 met the inclusion criteria while the remaining 482 were excluded due to initiation of treatment from an outside provider, failure to initiate treatment following medication dispensation, or enrollment in a clinical trial. The population was majority male (53%), White (80%), and English-speaking (88%). With respect to sex assigned at birth, 19% were male, 16% were female, and 65% did not report. In terms of sexual orientation, 21% identified as straight, 1% as gay, and 78% did not report. As for gender identity, 15% identified as female, 20% as male, and 65% did not report. Regarding the population's socioeconomic status, the majority were married (58%), 96% did not report their education level, and 67% were retired. Additionally, 18% of patients required transportation assistance for clinic visits. Comorbidities associated with health disparities included cardiovascular disease (53%), diabetes mellitus (15%), obesity (21%), respiratory disease (8%), and chronic kidney disease (7%). Financial assistance was utilized by 54% of patients. Further demographic characteristics are detailed in Table 1.
Patient baseline characteristics (N = 328).
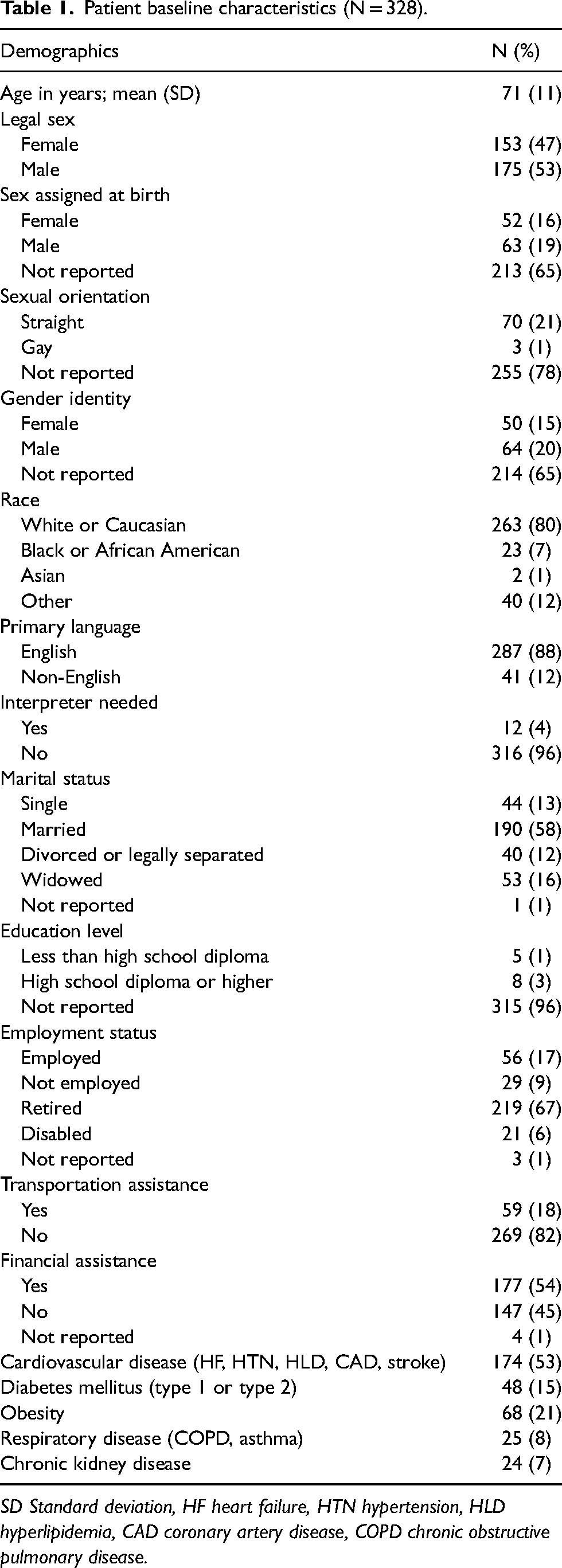
SD Standard deviation, HF heart failure, HTN hypertension, HLD hyperlipidemia, CAD coronary artery disease, COPD chronic obstructive pulmonary disease.
Health equity factors
Table 2 presents the results of a multiple linear regression analysis evaluating the association between health equity factors and the time to lenalidomide dispensation. The beta coefficients indicate the direction of the relationship with dispensation time, with a residual standard error (SE) of 10.8.
Multiple linear regression model of health equity factors related to lenalidomide dispensation time.
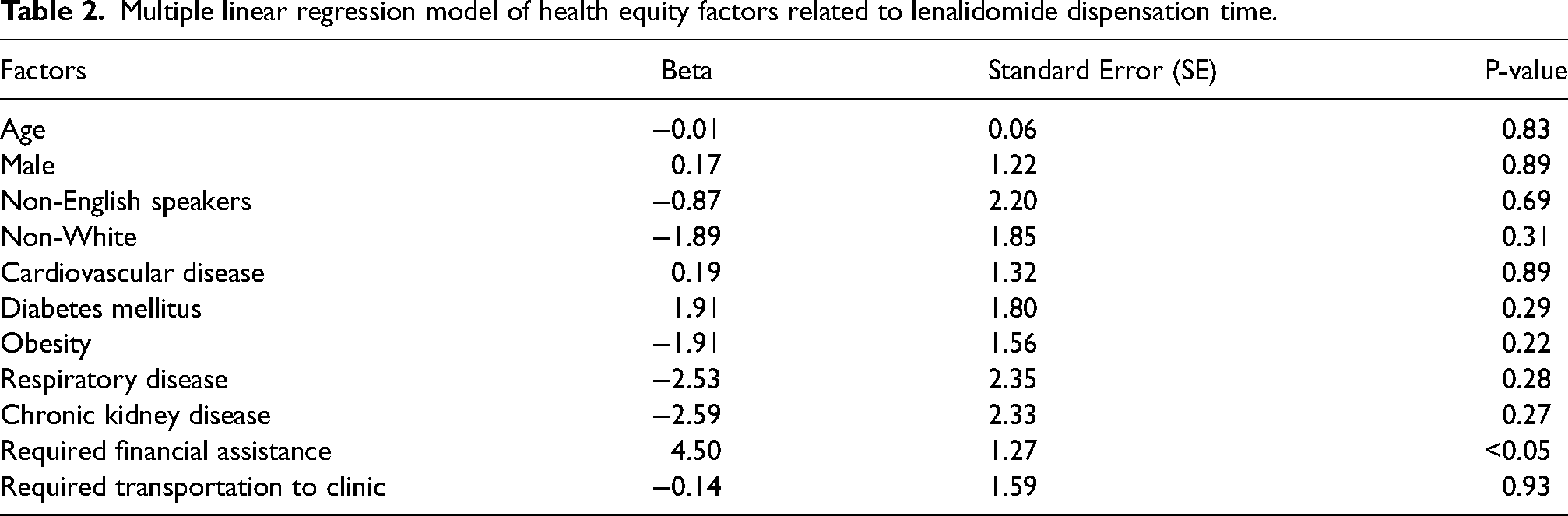
Age was associated with a minimal decrease in dispensation time, showing a reduction of 0.01 days (SE 0.06, P = 0.83). Male sex at birth was linked to a slightly longer dispensation time of 0.17 days (SE 1.22, P = 0.89). Non-English-speaking patients demonstrated a small reduction of 0.87 days (SE 2.20, P = 0.69), while non-white patients showed a 1.89-day reduction (SE 1.85, P = 0.31), suggesting that these factors have a marginally favorable impact on dispensation time.
Comorbidities such as cardiovascular disease, diabetes mellitus, obesity, respiratory disease, and chronic kidney disease were associated with either a slight increase or a slight reduction in dispensation time. Cardiovascular disease was associated with a slight increase in dispensation time of 0.19 days (SE 1.32, P = 0.89), while diabetes mellitus was associated with a longer dispensation time of 1.91 days (SE 1.80, P = 0.29). Obesity was linked to a reduction of 1.91 days (SE 1.56, P = 0.22), respiratory disease to a reduction of 2.53 days (SE 2.35, P = 0.28), and chronic kidney disease to a reduction of 2.59 days (SE 2.33, P = 0.27).
Patients requiring transportation assistance to clinic visits had a slight reduction in dispensation time of 0.14 days (SE 1.59, P = 0.93). Most notably, patients who required financial assistance had a statistically significant longer dispensation time, with an average increase of 4.5 days (SE 1.27, P < 0.05), highlighting the importance of addressing financial barriers to ensure timely access to lenalidomide.
Additionally, the median time from lenalidomide order to dispensation was approximately 8 days (interquartile range [IQR], 5–14).
Discussion
Health disparities have long been recognized as a barrier to timely treatment initiation, particularly in oral anti-cancer therapy. This study evaluated health equity factors previously shown to influence patient outcomes and explored their impact on lenalidomide dispensation times. While our findings revealed minimal changes in dispensation times associated with health equity factors, these factors have been reported in previous studies to affect adherence and initiation to treatment. Ononogbu et al. demonstrated that racial and ethnic disparities significantly affected adherence to immunomodulatory therapies in MM patients at a county hospital (P = 0.048), with the disparities primarily represented by African American and Hispanic patients. 9 A systematic review by Gasoyan et al. reinforced these findings, revealing significant disparities in MM care patterns related to patient race, ethnicity, and insurance coverage. 10 Additionally, Bouwman et al. identified younger age, higher education levels, and fatigue as significant predictors of non-adherence (P < 0.10), 11 while Mian et al. reported that increasing age (adjusted Odds Ratio 1.03 per year, 95% confidence interval [CI] 1.00–1.05, P = 0.024) was linked to poor adherence. 12 These studies underscore the multifaceted nature of age-related factors in influencing treatment outcomes.
Our analysis revealed that financial assistance programs significantly delayed the dispensation of lenalidomide. Geynisman et al. further emphasized that more than half of oral anti-cancer prescriptions utilized financial assistance, and these prescriptions involved significantly more phone calls by clinic staff (P = 0.0001) to get approval for their patients. 13 These challenges highlight that insurance barriers remain a significant obstacle to accessing oral anti-cancer medications, requiring patients and healthcare providers to navigate co-pay assistance to obtain the necessary treatments.
Our study demonstrated several key strengths. Firstly, our institution developed and implemented an in-house process for oral anti-cancer medications to facilitate prior authorizations and financial assistance applications for patients with high co-pays or those who are uninsured (Figure 1). This streamlined approach resulted in a median dispensation time of 8 days (IQR, 5–14) from the lenalidomide order to dispensation, which is notably shorter than the 12-day median reported by Geynisman et al., where some patients waited weeks for treatment initiation. 13 This finding suggests that institutions without the resources for an in-house process may experience longer dispensation times. Therefore, we recommend adopting similar processes to enhance dispensation efficiency. Secondly, while our in-house prescription process allows patients to access lenalidomide more quickly than at other institutions, the dispensation times in general could be further reduced if the REMS program contracted with more specialty pharmacies. Lastly, our health system emphasized equitable treatment, ensuring that health equity factors did not influence treatment initiation. This approach provided timely access to medication for all patients, ultimately improving their health outcomes.
However, our study had several limitations. Black and African American patients, who are at a higher risk of developing MM, were underrepresented in our study. Furthermore, due to the single-center design, our findings may not be generalizable to other healthcare institutions. The relatively small sample size and the absence of a comparator arm further limit the ability to draw definitive conclusions. Additionally, retrospective data collection posed challenges. Key socio-demographic data points that would have aided in identifying health disparities, such as education level, primary insurance type, and urbanicity of their primary residence, were not reported for the majority of patients or were unable to be accurately categorized. These limitations affected the ability to assess the significance of these health equity factors in influencing the time to lenalidomide dispensation.
Conclusion
This study highlighted the critical role of health equity factors in influencing initiation of oral anti-cancer medications, specifically lenalidomide. While our findings demonstrated the effectiveness of institutional processes in mitigating delays, barriers related to financial assistance programs and other health equity factors remain pervasive challenges. Addressing these inequities will require ongoing efforts to improve transparency in financial assistance programs, reduce insurance-related barriers, and implement tailored interventions to support vulnerable populations. Future research should focus on developing and evaluating interventions aimed at improving access to lenalidomide and other limited-distribution medications for underserved populations.
Footnotes
Author contributions
Ngan Nguyen, Justin Huynh, Jenna Wu, Hannah Kisla, and Britny Brown researched literature for this project and developed study protocol. Annabel La and Jamie Read collected data from patients and Darlene Tat performed data analysis. Ngan Nguyen drafted the first version of the manuscript. All authors reviewed and approved the final version of the manuscript.
Consent to participate
Brown University Health IRB waived the need for ethics approval and patient consent for the collection, analysis and publication of the retrospectively obtained and anonymized data for this non-interventional study.
Data availability statement
The datasets generated and analyzed during the current study are not publicly available since they were collected via our electronic health record. They were analyzed in a confidential manner but are available from the corresponding author on reasonable request.
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Ethical considerations
The study was conducted in accordance with the Declaration of Helsinki and was approved by Brown University Health IRB (approval #009424) on July 15, 2024, with the need for written informed consent waived.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.