
Abstract
Objective
This review discusses current strategies, new advancements and clinical trials for the treatment of bone metastases.
Method
We performed a narrative review using literatures obtained from PubMed and Google Scholar using the terms such as “Prostate cancer”, “bone metastases”, “treatment”. The search included articles between 2000 and 2024. For clinical trial information, we searched www.clincialtrial.gov and included trials of Prostate cancer and bone metastases.
Summary
We go through the mechanisms of action, clinical effectiveness, and limitations of current and emerging therapies, including bisphosphonates, Receptor activator of nuclear factor kappa-Β ligand (RANKL) inhibitors, novel agents and Prostate-Specific Membrane Antigen (PSMA) targeted approaches. By examining recent research and ongoing clinical trials, we seek to inform the development of optimized treatment strategies and guide future research directions. The review discuss about novel agents such as Radium-223 and Lutetium-177. Lutetium-177 is emerging as a promising treatment for metastatic prostate cancer with bone involvement. These treatment options offer significant survival benefits in patients with bone-dominant metastatic prostate cancer. The review also explores combination treatments, where integrating bone-targeted therapies with systemic prostate cancer treatments holding potential for enhanced efficacy. Ongoing clinical trials investigating novel treatment options and advanced drug delivery techniques are highlighted.
Conclusion
The advancements signify a promising direction in the treatment of bone metastases in prostate cancer, highlighting the need for continuous innovation to enhance patient care and outcomes
Introduction
Prostate cancer (PCa) is a leading cause of morbidity and mortality among men globally. It's the second most commonly diagnosed malignancy and the fifth most frequent cause of death in men worldwide. 1 Many patients with PCa develop bone metastases, which are secondary tumors that spread to the bones. Approximately 10% of patients with early PCa and up to 80% of those with advanced disease experience bone metastases. 2 The tendency of prostate cancer cells to colonize bone is due to their interaction with the bone microenvironment, which supports tumor growth and leads to complex bone remodeling. 3
Bone metastases in prostate cancer often result in severe pain, increased risk of fractures, and a significant decline in quality of life. 4 Additionally, the presence of bone metastases is associated with a poorer prognosis and higher healthcare costs, complicating the effective management strategies.4,5
This review aims to provide a comprehensive overview of the most recent pharmacological treatments for prostate cancer bone metastases. We will go through the mechanisms of action, clinical effectiveness, and limitations of current and emerging therapies, including bisphosphonates, Receptor activator of nuclear factor kappa-Β ligand (RANKL) inhibitors, Radium-223, and Prostate-Specific Membrane Antigen (PSMA) targeted approaches. By examining recent research and ongoing clinical trials, this review seeks to inform the development of optimized treatment strategies and guide future research directions.
Methods
We performed a narrative review using literatures obtained from PubMed and Google Scholar using the terms such as “Prostate cancer”, “bone metastases”, “treatment”. The search included articles between 2000 and 2024. Original articles published in English were only included. For clinical trial information, we searched www.clincialtrial.gov and included trials of Prostate cancer and bone metastases.
Pathophysiology of bone metastasis in prostate cancer
PCa often metastasizes to bone, a process influenced by intricate molecular and cellular interactions between cancer cells and the bone microenvironment. The pathophysiology of bone metastases in PCa involves several key mechanisms, including tumor cell adhesion, disruption of bone remodeling, and the creation of a favorable environment for metastatic growth. Prostate cancer cells have a particular affinity for colonizing bone tissue due to interactions between their surface molecules and bone matrix proteins. Integrins play a crucial role in this process, mediating the adhesion of cancer cells to extracellular matrix components like collagen and fibronectin found in bone. 6 Moreover, prostate cancer cells secrete factors such as parathyroid hormone-related peptide (PTHrP) and interleukin-6 (IL-6) that stimulate both osteoblasts and osteoclasts, leading to abnormal bone remodeling.7,8
The bone microenvironment plays a crucial role in promoting the growth and survival of metastatic prostate cancer cells. 9 Tumor cells interact with bone cells through various signaling pathways, including the RANK/RANKL/OPG axis. Prostate cancer cells produce RANKL, which interacts with the RANK receptor on osteoclast precursors, promoting their maturation and activity. This results in increased bone resorption and the release of growth factors from the bone matrix further enhances tumor growth. 10 Osteoblasts, responsible for bone formation, are also impacted by prostate cancer cells. Tumor cells can disrupt normal osteoblast activity by producing bone morphogenetic proteins (BMPs) and other factors that lead to the formation of osteoblastic lesions (Figure 1). 11
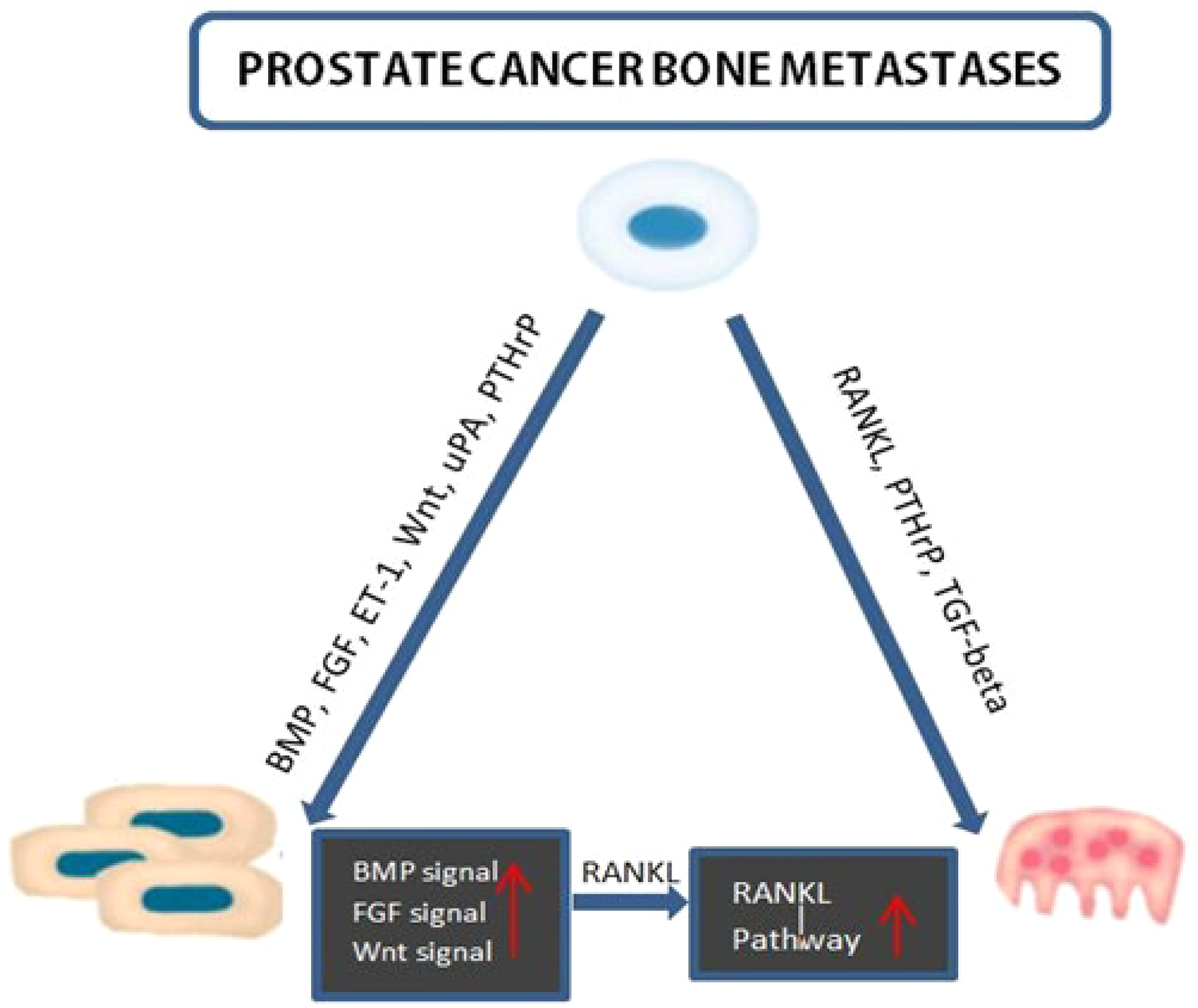
Prostate cancer bone metastases pathway.
Furthermore, the interaction between prostate cancer cells and stromal cells in the bone marrow is crucial for the formation of metastases. Bone marrow stromal cells create a supportive microenvironment rich in cytokines and growth factors, such as vascular endothelial growth factor (VEGF) and fibroblast growth factor (FGF), which promote tumor cell survival and proliferation (Figure 1). 12 Prostate cancer cells can manipulate the bone marrow microenvironment to their advantage by inducing angiogenesis and creating a niche for their growth. This interaction is reciprocal; while prostate cancer cells modify the bone microenvironment to enhance their survival, the altered microenvironment also promotes further cancer cell proliferation and metastasis.
The process of bone metastasis is further complicated by prostate cancer cells’ ability to modify local bone remodeling. Increased osteoclastic activity leads to bone destruction; this paradoxically triggers the release of growth factors, such as transforming growth factor-beta (TGF-β), from the bone matrix. These factors subsequently enhance the survival and proliferation of prostate cancer cells, establishing a vicious cycle of bone resorption and tumor growth. 13 This interplay between osteoblasts and osteoclasts, mediated by various signaling molecules, ensures a continually supportive environment for metastatic tumor cells, making bone metastasis a particularly challenging aspect of prostate cancer management.
Current pharmacological treatments for bone metastasis
Bisphosphonates
Bisphosphonates are a class of medications aimed at inhibiting bone resorption mediated by osteoclasts. Osteoclasts are specialized cells derived from the hematopoietic lineage that are responsible for the breakdown of bone tissue. This process, known as bone resorption, is essential for bone remodeling, but it can become dysregulated in conditions like metastatic cancer Bisphosphonates work by binding to hydroxyapatite crystals in the bone matrix. When osteoclasts attempt to resorb bone, they ingest these hydroxyapatite crystals along with the bisphosphonates. Once inside the osteoclast, bisphosphonates disrupt critical cellular processes, such as ATP production, leading to osteoclast apoptosis. This apoptosis leads to a reduction in osteoclast activity, ultimately resulting in decreased bone resorption. 14 By inhibiting bone resorption, bisphosphonates help to stabilize the bone matrix and prevent pathological fractures.
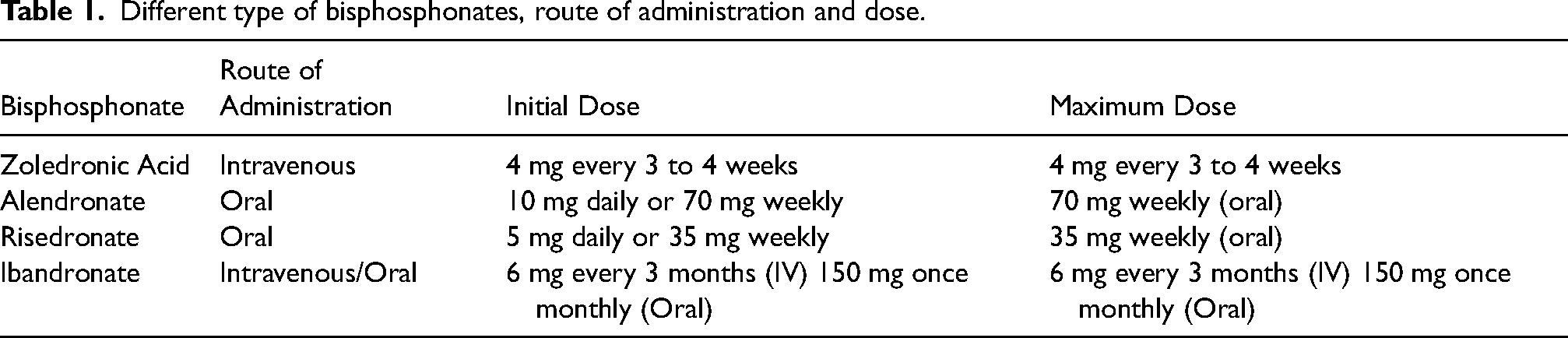
Clinical Efficacy: The clinical efficacy of bisphosphonates in managing prostate cancer bone metastases is well-established. Zoledronic acid (ZA), a potent intravenous bisphosphonate, has been extensively studied and to considerably lower the occurrence of skeletal-related events (SREs). A pivotal study demonstrated that Zoledronic acid decreased the risk of SREs by 36% compared to a placebo in men with hormone-refractory prostate cancer. 15 Additionally, the drug has been linked to a delay in the time to the first SRE, a reduction in bone pain, improved overall survival, and a decreased need for radiation therapy for bone lesions. 16 Pamidronate, while less commonly used today than ZA, has also been effective in reducing SREs. Alendronate and risedronate are oral bisphosphonates beneficial for maintaining bone density and managing bone health, have shown limited efficacy in reducing SREs in metastatic prostate cancer.17,18 Clinical trials have demonstrated that intravenous ibandronate can reduce the risk of SREs and manage bone complications effectively. However, its use in prostate cancer has not been as widely validated or preferred compared to ZA, which remains the more studied and preferred option due to its superior efficacy and dosing convenience. It can be considered an alternative treatment for metastatic prostate cancer when ZA is not suitable.18,19 Doses of each bisphosphonates are discussed in Table 1.
Different type of bisphosphonates, route of administration and dose.
Side Effects: The most frequent side effects of bisphosphonates are flu-like symptoms, including fever and muscle pain, which typically resolve within a few days after infusion. 20 More serious side effects include osteonecrosis of the jaw (ONJ), condition where the jawbone deteriorates, often exacerbated by dental procedures or trauma. While the incidence of ONJ is relatively low (1 in 10,000 to 1 in 100,000), it can be severe when it occurs, necessitating preventive measures such as regular dental evaluations prior to starting bisphosphonate therapy. 21 Alendronate and risedronate can cause gastrointestinal problems, including nausea, abdominal pain, indigestion, and esophageal irritation. This is often due to the irritation of the esophagus and stomach lining. 20
Limitations: While bisphosphonates are effective in reducing SREs, they may not necessarily improve overall survival for all patients. Research has indicated that bisphosphonates are less effective in advanced, hormone refractory cases of prostate cancer. 22
RANK ligand inhibitors (denosumab)
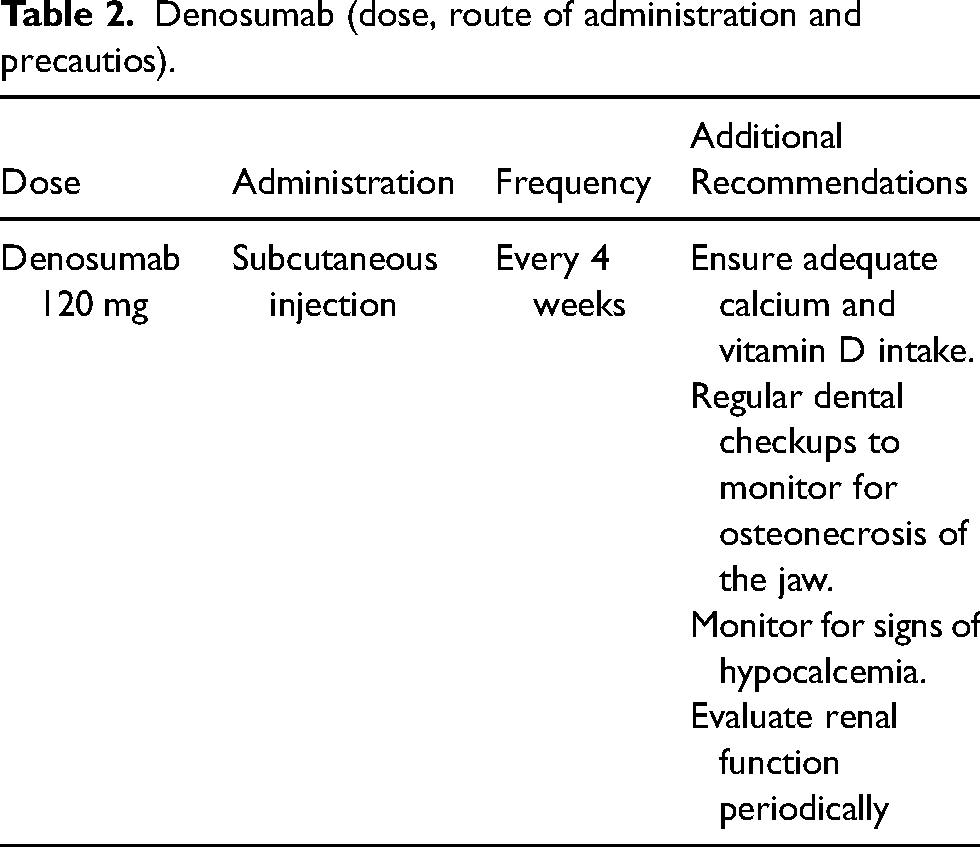
Denosumab is the only RANKL inhibitor approved for treating bone metastases Table 2. A monoclonal antibody that targets the RANKL. Its mechanism of action involves inhibiting the interaction between RANKL and its receptor RANK on osteoclasts and their precursor cells. This is critical for osteoclastogenesis and bone resorption. By preventing this interaction, denosumab effectively reduces the formation, activity, and survival of osteoclasts, leading to decreased bone resorption and a decrease in SREs, including fractures and spinal cord compression. 23
Clinical Efficacy: A pivotal Phase III clinical trial compared denosumab with zoledronic acid, in men with bone metastases from prostate cancer. The study showed that denosumab significantly lowered the risk of SREs by 22% when compared to ZA. Additionally, denosumab extended the time to the first SRE and was well-tolerated, making it an effective alternative for patients who may not tolerate bisphosphonates. 24 Another key study focused on castration-resistant prostate cancer (CRPC), a more advanced form of the disease. This research showed that denosumab was effective in reducing the incidence of SREs and improving bone health in men with CRPC. The results confirmed denosumab's ability to provide durable benefits, making it a valuable treatment option for managing bone complications in advanced prostate cancer. 25 Further investigation into the impact of denosumab on quality of life found that it improved pain management and mobility in patients. By reducing the frequency of SREs and associated complications, denosumab enhanced overall patient well-being and functional status. 26 Ongoing research continues to explore denosumab's role in combination with other treatments and in earlier stages of prostate cancer. Studies are examining whether early use of denosumab can prevent or delay the onset of bone metastases and evaluating its long-term safety and efficacy. A study explored the long term efficacy of denosumab and the result suggest that long term use of denosumab will prevent and postpone SRE, but with ONJ at increased risk. This study would be crucial for optimizing treatment strategies and improving outcomes. 27
Side Effects: The most severe issue is hypocalcemia, which can cause symptoms such as muscle cramps, tingling, and, in severe cases, cardiac complications. Hypocalcemia occurred more frequently in patients receiving denosumab compared to zoledronic acid, with an incidence of 9.6% versus 5.0%, respectively. The FDA has issued a warning about the risk of severe hypocalcemia.23,28,29 In patients with pre-existing hypocalcemia, regular monitoring of serum calcium levels is essential. Denosumab should be used cautiously in individuals with conditions that predispose them to hypocalcemia. An increased risk of being diagnosed with ONJ is associated with longer durations of denosumab exposure. Patients may also experience symptoms including back pain, skin rashes, joint pain, diarrhea, nausea, vomiting, and headaches. Additionally, skin infections at the injection site and potential allergic reactions have been reported but are less common. 23 Overall, while denosumab effectively reduces SRE and improves bone health, awareness and management of these side effects are essential for optimizing patient outcomes and ensuring safe use of the drug.
Limitations: Denosumab may not be suitable for patients with severe renal impairment or those who cannot maintain proper oral health. The requirement for frequent subcutaneous injections may also be a limiting factor for some patients. Additionally, denosumab is often more expensive compared to bisphosphonates like zoledronic acid, which may be a consideration in treatment planning, especially in healthcare systems with budget constraints. 30 While denosumab has proven effective in reducing SREs, long-term data on its safety and efficacy are still being gathered. Studies indicate that long-term use of denosumab may help prevent or delay SREs, but it also carries an increased risk of ONJ. However, most patients who resumed denosumab treatment did not experience a recurrence of ONJ. 27 Understanding the full spectrum of potential adverse effects and the impact on overall survival is crucial. Ongoing monitoring and research are essential to fully understand long-term outcomes.
Denosumab (dose, route of administration and precautios).
Novel anticancer agents
Radium-223 dichloride is a targeted alpha-emitter radiopharmaceutical approved for treating prostate cancer bone metastases. It selectively targets and irradiates bone metastases, mimicking calcium and localizing to areas of high bone turnover. Once incorporated into the bone matrix, it emits alpha particles that deliver potent radiation directly to tumor sites while sparing surrounding healthy tissues. Radium-223 dichloride is primarily used to treat symptomatic bone metastases in patients with CRPC who have extensive bone involvement but no evidence of visceral metastases.31–33 Clinical trials have shown that radium-223 significantly lowers the risk of SREs, such as fractures and spinal cord compression, while also improving overall survival and quality of life. For instance, the ALSYMPCA trial, a pivotal Phase III study, it has been established that radium-223 significantly extends overall survival and delays the time to the first SRE compared to a placebo. 34 Radium-223 is administered via intravenous injection every four weeks for six cycles. Its effectiveness is coupled with a relatively manageable safety profile. Common side effects include peripheral edema, nausea, vomiting, and diarrhea. Common hematological adverse effects include bone marrow suppression, leading to anemia, thrombocytopenia, and leukopenia. Fatigue is another frequently reported issue. 32 Importantly, Radium-223 is contraindicated in patients with visceral metastases, such as liver or lung involvement, as it primarily targets bone lesions and may not be effective or safe in those with widespread disease. Additionally, its use is limited by the necessity for regular intravenous administration and the requirement for careful monitoring of blood counts and renal function.32,33
PSMA-targeted therapies are designed to specifically target and destroy prostate cancer cells while minimizing damage to healthy tissues. They are particularly effective in treating advanced prostate cancer that has spread to the bones. PSMA is a protein found in high concentrations on prostate cancer cells, including those that have metastasized to the bones. There are two main types of PSMA-Targeted Therapies; PSMA-Directed Radioligand Therapy and PSMA-Targeted Monoclonal Antibodies. Lutetium-177-PSMA-617 (Lu-177-PSMA-617) is a example of PSMA-Directed radioligand therapy. This therapy combines a radioactive substance (Lutetium-177) with a PSMA-targeting molecule. The radioligand binds to PSMA on cancer cells, delivering targeted radiation that destroys them. 35 177Lu-PSMA-617 is administered by slow intravenous injection (1–30 min) followed by a ringer or saline solution. The cooling of salivary glands (performed in 11/12 therapy centers) using cool packs started 30 min before injection and was applied until 4 h after injection to avoid salivary toxicity. Further therapy cycles are performed 8–12 week apart. 35 PSMA-ADC (Antibody-Drug Conjugates) is a PSMA-Targeted Monoclonal Antibodies. These antibodies are linked to cytotoxic drugs, delivering the toxic agent directly to cancer cells expressing PSMA. 36 A pivotal study (VISION trial) evaluating Lu-177-PSMA-617 demonstrated significant reductions in tumor burden and improved survival rates in patients with advanced prostate cancer and bone metastases. 37 Ongoing studies continue to assess long-term efficacy, optimal dosing, and safety of PSMA-targeted therapies. Common side effects of PSMA-targeted therapies include fatigue, dry mouth, and nausea. 37 Bone marrow suppression is another potential adverse effect that requires close monitoring. It can cause decreased blood cell counts, leading to risks of infections, bleeding, or anemia.37,38 Regular monitoring of liver and kidney function is also necessary. 39 PSMA-targeted therapies can be expensive. Affordable Lu PSMA Treatment Cost in India starts from INR 5,00,383. 40 Prostate cancer cells may develop resistance to PSMA-targeted therapies over time. Several studies have already pinpointed the PSMA heterogenic expression, defect on DNA repair genes, clonal expansion of PSMA-negative cells and tumor heterogeneity as possible mechanism of resistance. 41
Combination therapies
ADT + bisphosphonates (e.g. zoledronic acid, pamidronate) or RANKL inhibitors (e.g. denosumab)
Androgen deprivation therapy (ADT) for prostate cancer can result in considerable bone density loss and a higher risk of fractures due to decreased testosterone levels, which adversely affect bone health. To counteract these effects, bisphosphonates and RANKL inhibitors are commonly used in combination with ADT. Bisphosphonates work by inhibiting osteoclast activity, which slows bone resorption and helps maintain bone density. ZA, commonly used bisphosphonates are administered intravenously, typically every 6 to 12 months, and have been demonstrated to lower the incidence of SREs in patients undergoing ADT. 42 RANKL inhibitor offers a different approach by blocking RANKL. Denosumab, a RANKL inhibtor effectively reduces bone resorption and improves bone density. In patients experiencing ADT-induced bone loss, 60 mg dose of denosumab every 6 months has been demonstrated to improve bone mineral density and decrease the risk of vertebral fractures. 25 Both therapies have demonstrated efficacy in reducing fracture risk and improving bone health, but the choice between them often depends on patient-specific factors and clinical considerations.
Chemotherapy bone-targeted agents (bisphosphonates or RANKL inhibitors)
Docetaxel is a potent chemotherapeutic agent that can reduce tumor burden but may also lead to bone density loss and increased fracture risk. Combining chemotherapy agents like docetaxel with RANKL inhibitors, is an effective strategy for managing metastatic prostate cancer. An animal study with animals with tumor received 4 doses of Docetaxel (12 mg/kg) in combination with Denosumab (3 mg/kg), both given simultaneous as an IV injection. The result demonstrated that this combination treatment was significantly effective in treating bone metastasis. 43 However, the combination of chemotherapy and bisphosphonates, such as zoledronic acid with docetaxel, did not impact overall patient survival. 44
ADT + radium-223
The combination of abiraterone and radium-223 did not show any improvement in skeletal event-free survival, and instead, it led to a higher incidence of bone fractures. 45 As a result, osteoprotective agents have been recommended. The PEACE III trial evaluated the effectiveness of combining radium-223 with enzalutamide compared to enzalutamide alone in men with early asymptomatic or mildly symptomatic skeletal metastatic CRPC. The results of the PEACE-III trial demonstrated that adding six cycles of radium-223 to enzalutamide as a first-line treatment for metastatic castration-resistant prostate cancer (mCRPC) significantly improved patient outcomes, increasing the median progression-free survival from 16 to 19 months. 46 Studies indicate that better prevention of pathological fractures occurs only when bone-targeting agents are coadministered with combinations of radium-223 and novel hormone therapies. 47
Ongoing clinical trials in prostate cancer bone metastases
NCT05740488 48 : This study aims to assess the efficacy and safety of combining apalutamide with 89Sr (strontium) as neoadjuvant therapy for prostate cancer patients with ≤10 bone metastases. The primary endpoint is progression-free survival (PFS), evaluated up to 2 years following radical prostatectomy. Secondary endpoints include pathological complete response (pCR), evaluated up to 1 year; radiographic progression-free survival (rPFS), monitored up to 3 years; prostate-specific antigen (PSA) response rate, defined as more than a 50% decrease from baseline and assessed up to 3 years; pain score, measured using a Visual Analogue Scale (VAS) at baseline and during follow-up visits over an average of 3 years; and the number and extent of bone metastases, evaluated through bone scans up to 3 years. This comprehensive approach is designed to assess both the therapeutic efficacy and safety of the treatment regimen.
NCT06008483 49 : This is an open-label, unblinded, multi-center, dose-finding study of 153-Sm-DOTMP, a radioconjugate that combines the phosphonic acid chelator DOTMP (1,4,7,10-tetraazacyclododecane-1,4,7,10-tetramethylenephosphonic acid) with the beta- and gamma-emitting radioisotope samarium (Sm 153). When injected, this compound delivers radiation directly to the bone. The study aims to identify the maximum tolerated dose (MTD) of 153-Sm-DOTMP, which will be administered as a pair of doses to subjects with solid tumors detectable on bone scans. The MTD is defined as the dose level at which the dose-limiting toxicity (DLT) rate does not exceed 25%. DLTs are defined as any grade 3 or higher hematologic or nonhematologic toxicity, as outlined by the National Cancer Institute's (NCI) Common Terminology Criteria for Adverse Events (CTCAE), occurring during a 42-day observation period. Clinical response will be determined by either stable disease (SD) or a reduction in tumor size based on radiographic imaging (e.g. CT or MRI), evaluated using Response Evaluation Criteria in Solid Tumors (RECIST) v1.1. The Day 1 dose will remain fixed at 0.5 mCi/kg, while the Day 8 dose will escalate from 0.5 mCi/kg (dose level 1) to 1.0 mCi/kg (dose level 2), then 2.0 mCi/kg (dose level 3), and finally 3.0 mCi/kg (dose level 4).
NCT04754425 50 : This phase II trial evaluates the effects of erdafitinib in treating patients with castration-resistant prostate cancer, a form of the disease that continues to grow and spread despite the surgical removal of the testes or the use of drugs to block androgen production. Erdafitinib may inhibit tumor cell growth by blocking certain enzymes required for cell proliferation. This treatment may help control the disease in patients with castration-resistant prostate cancer. The primary objective is to assess the efficacy of erdafitinib in patients with advanced prostate cancer who have progressed on second-generation androgen receptor (AR)-targeting agents (SART). Secondary objectives include: (i) determining the objective response rate, (ii) measuring Time on Treatment (ToT) as a surrogate for clinical efficacy and PFS, (iii) evaluating PFS, (iv) correlating changes in bone-specific alkaline phosphatase (BAP) with response, ToT, and PFS, (v) correlating changes in PSA with response, ToT, and PFS, (vi) characterizing the safety profile of erdafitinib treatment, (vii) assessing overall survival, and (viii) collecting and storing bone marrow biopsies, aspirates, serum, and plasma samples for future hypothesis-generating analyses.
NCT04549207 51 : Current guidelines recommend bone-modifying agents (BMAs), such as bisphosphonates and denosumab, every 4 to 12 weeks to reduce the incidence and delay the onset of symptomatic skeletal events (SSEs) in patients with bone metastases from breast cancer and CRPC. However, the optimal frequency and duration of BMA treatment after 2 years remain unclear. This is an important clinical question, as the risk of SSEs decreases over time, while the risk of treatment-related toxicities increases. This pragmatic, multicenter, open-label randomized controlled trial (RCT) will involve patients with bone metastases from breast cancer or CRPC who have received at least two years of BMA treatment. Eligible patients who consent will be randomized to either continue the standard BMA schedule (every 4 or 12 weeks) or a de-escalated BMA schedule (every 24 weeks). The co-primary endpoints are the physical functioning subscale of the EORTC-QLQ-C30 and the functional interference subscale of the EORTC-QLQ-BM22. Secondary endpoints include the number of patients with ≥1 SSE, time to first SSE, SSE-free survival, skeletal morbidity rate, EORTC-QLQ-C30 and BM22 scores, BMA-related toxicity, and treatment adherence. Randomization (1:1 ratio) will be stratified by cancer type (breast vs. prostate) and prior treatment schedule (every 4 weeks vs. every 12 weeks). A subgroup analysis will compare patients with 2–3 years of prior BMA treatment to those with more than 3 years of prior treatment.
NCT03395197 52 : PARP-inhibitors (poly-ADP ribose polymerase-inhibitors), when combined with androgen receptor-targeted therapy, have shown promise in the treatment of mCRPC. This article outlines the design and rationale of the multinational, phase III, two-part TALAPRO-2 study, which compares talazoparib plus enzalutamide to placebo plus enzalutamide as a first-line treatment for patients with mCRPC, both with and without DNA damage response (DDR) alterations. The study has two co-primary endpoints: rPFS, assessed by blinded independent clinical review, in all patients (cohort 1) and in those with DDR alterations (cohort 2). TALAPRO-2 aims to determine whether talazoparib plus enzalutamide can significantly enhance the efficacy of enzalutamide in improving rPFS in both molecularly unselected and DDR-deficient mCRPC patients.
Personalized medicine approaches
Personalized medicine in the treatment of bone metastases involves customizing therapies based on a patient's unique tumor characteristics, genetic profile, and overall health. This approach seeks to enhance treatment effectiveness while reducing adverse effects. A key component of personalized medicine is the use of biomarker-driven strategies. By identifying specific genetic mutations or protein expressions in tumors, clinicians can guide the selection of targeted therapies. In prostate cancer, biomarkers like AR-V7 can impact treatment decisions, particularly in determining the use of androgen receptor-targeted agents. 53
Additionally, advanced imaging techniques like PET scans and MRI play a crucial role in evaluating the extent of bone involvement and monitoring the response to treatment, enabling more informed decisions about when to adjust or intensify therapy. 54 For older patients with significant comorbidities, palliative care strategies, including bisphosphonates or RANKL inhibitors, may be more beneficial than aggressive systemic treatments.
Advances in drug delivery systems
Most drugs are poorly distributed to the bone, making them pharmacologically ineffective in treating bone metastases. This is due to the unique physiology of bone, which acts as a blood-bone marrow barrier, preventing large exogenous substances from reaching the bone surface. 55 To efficiently treat bone metastases, the development of drug targeting technologies is essential. Various bone-targeting strategies have been developed for the delivery of drugs to the bone. Among these, drug conjugates with bone-targeting ligands were the first to be introduced in the field of bone drug targeting. Ligands with high affinity for hydroxyapatite (HAP), a key component of the bone matrix, are particularly effective for drug targeting. Ligands such as Tetracycline, 56 BP 57 and carboxylic acid (e.g. aspartic acid) 58 have been identified for their strong affinity for HAP. Additionally, antibodies targeting PSMA are being used for active targeting in bone metastatic prostate cancer, with some PSMA antibody conjugates having been developed and tested in clinical trials. 59 The use of these targeting ligands offers the potential for more efficient bone-targeted drug delivery.
Conclusion
Advancements in the treatment of bone metastases in prostate cancer have significantly improved patient outcomes and quality of life. Innovative therapies, including novel pharmacological agents such as bisphosphonates and denosumab, have demonstrated efficacy in reducing skeletal-related and alleviating symptoms. Additionally, targeted therapies and radionuclide treatments, like radium-223, have shown promise in extending survival. Furthermore, the integration of treatment with biomarkers holds potential for tailoring treatment approaches to individual patient profiles, enhancing therapeutic effectiveness. As research continues to evolve, a multidisciplinary approach combining medical, surgical, and supportive care is essential for optimizing management strategies. Ongoing clinical trials and studies are crucial for deepening our understanding of the mechanisms behind bone metastases and discovering new therapeutic targets. Overall, these advancements signify a promising direction in the treatment of bone metastases in prostate cancer, highlighting the need for continuous innovation to enhance patient care and outcomes.
Footnotes
Acknowledgements
We are grateful to professors from department of Urology in Yenepoya Medical College Hospital, for their invaluable insights and critical feedback of this research project. The expertise of professors and HOD of urology helped in strategies significantly improved the comprehensiveness and focus of the manuscript. Finally, we thank Secretary of the department, senior residents for sharing their valuable knowledge. They enabled us to dedicate time and resources to thoroughly analyze during this review.
Authors’ contributions
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.