
Abstract
Introduction
The increasing cardiovascular events in cancer patients underscore the importance of identifying preexisting risk factors as predictors of heart disease outcomes. This study aimed to assess the predictive risk factors associated with cancer therapy-related cardiac dysfunction (CTRCD) in female patients with breast cancer undergoing treatment with anthracyclines and/or anti-HER-2 therapies.
Methods
A cohort study was conducted at a university hospital outpatient clinic from 2019 to 2024. CTRCD was defined according to the European Society of Cardiology criteria as an absolute LVEF reduction of >10 percentage points to <50% during treatment.
Results
A total of 161 female patients were analyzed (mean age: 51.2 ± 11.6 years), with most being white/Caucasian (83.8%). The most prevalent cardiovascular risk factors were hypertension (47.2%), obesity (31.7%), smoking (31.0%), dyslipidemia (14.3%), and type 2 diabetes mellitus (12.4%). CTRCD occurred in 18 patients (11.1%), with a markedly higher prevalence (27.3%) in those with four or more cardiovascular risk factors. The median time (IQR) from the initiation of chemotherapy to CTRCD was 395 (248–674) days. Multivariable analysis identified the Charlson comorbidity index (HR 1.2; 95% CI: 1.0–1.4), chemotherapy duration (HR 1.0; 95%CI: 1.0–1.0) and LVEF before (HR 0.8; 95%CI: 0.7–0.9) and after chemotherapy (HR 0.8; 95%CI: 0.8–0.9) as independent factors for CTRCD. Breast cancer patients had a 17.7% risk of developing CTRCD within the first two years of antineoplastic treatment.
Conclusion
Hypertension, obesity, and smoking were the most prevalent cardiovascular risk factors. Independent predictors of CTRCD included the Charlson comorbidity index, chemotherapy duration, and LVEF before and after treatment.
Introduction
The incidence of cardiovascular events in patients diagnosed with cancer has become an increasingly evident finding. An analysis of the ASPREE trial revealed that older adults diagnosed with cancer exhibited a cardiovascular disease (CVD) incidence rate of 20.8 events per 1000 person-years. This rate was substantially higher compared to the incidence observed in individuals without cancer, which was 10.3 events per 1000 person-years. 1 With the advancement of drug therapy, along with a better understanding of disease mechanisms, cancer patients currently experience an increase in survival rates and an improvement in overall well-being. 2 However, there is a greater exposure to risk factors and clinically unfavorable outcomes, such as cardiac injury or cardiovascular toxicity. 3
In order to establish connections between CVD complications and cancer therapy, there is evidence highlighting, in addition to structural changes and the consequent reduction in left ventricular ejection fraction (LVEF), the importance of identifying pre-existing cardiovascular risk factors as predictors of outcomes in the development of heart disease after antineoplastic treatment.4,5 Therefore, a comprehensive assessment with an appropriate risk reduction strategy, controlling and managing cardiovascular risk factors, reduces the probability of developing cardiac complications and/or cancer-related diseases. 6
A significant portion of this intersection between CVD and breast cancer is related to the similarity in predictive risk factors, such as age, smoking, obesity, sedentary lifestyle, dyslipidemia, and arterial hypertension. 7 From the perspective of anticancer therapy (especially treatment with anthracyclines and anti-HER-2 therapies), evaluating the type, cumulative dose, duration, and combination of antineoplastic agents similarly gains significant importance in predicting future outcomes. 5
Indeed, several publications have established interfaces between CVD and cancer.8,9 Researching and acknowledging these biological mechanistic connections and pushing the boundaries of knowledge with innovative studies expands the understanding and management of factors potentially related to the development of cancer therapy-related cardiac dysfunction (CTRCD). 10 The sequential or concurrent administration of two distinct agents, anthracyclines and anti-HER-2 therapies (e.g., trastuzumab), may elevate the risk of myocardial injury and cardiac dysfunction associated with cancer therapy. This heightened risk often stems from the cumulative adverse effects of both therapies in breast cancer patients. 11
Nevertheless, the association between cardiovascular risk factors and clinical characteristics of such patients remains unclear. Therefore, this study aimed to assess the predictive risk factors associated with CTRCD in female patients with breast cancer undergoing treatment with anthracyclines and/or anti-HER-2 therapies.
Methods
We conducted a retrospective cohort study of female and adults (≥ 18 years old) patients diagnosed with breast cancer who underwent treatment with anthracyclines and/or anti-HER-2 therapies. Eligible patients were identified through queries in the system of the university hospital, filtered by antineoplastic treatment class. These patients were consecutively enrolled in the cardio-oncology, oncology, haemato-oncology, and heart failure outpatient clinics at a university hospital between January 2019 and March 2024. Following automated selection, detailed reviews of electronic medical records were conducted to extract sociodemographic, clinical, oncological, and cardiological variables. The HCPA is a teaching hospital, university-affiliated, tertiary-level center located in southern Brazil, primarily serving a low-income population.
Patients were excluded if they had a pre-existing diagnosis of left ventricular dysfunction with LVEF <55%, experienced an acute myocardial infarction after the start of antineoplastic treatment/during follow-up, who did not use anthracyclines or anti-HER2 drugs, diagnosed with another type of cancer or had missing information, restricted access, no permission to collect data in the medical records that could compromise the data collection and analysis. This study was approved by the Research Ethics Committee (protocol number 2021/0587). All data verified in the study followed the principles of the Declaration of Helsinki and the Nuremberg Code and respected the Research Standards Involving Human Beings (Resolution No. 466/2012) of the National Health Council. The selection of variables was based on previously published studies demonstrating their association with CTRCD and cardiovascular outcomes in cancer patients.5,10,12 The data collection was based on a specific instrument developed by the researchers, which included: (1) sociodemographic variables (age, race); (2) clinical variables (pre-existing conditions, cardiovascular risk factors); (3) laboratory tests (BNP/NT-proBNP and troponin); (4) imaging tests (electrocardiogram and echocardiogram); and (5) medication therapy (e.g., betablockers, angiotensin receptor blockers, and angiotensin-converting enzyme inhibitors). We also collected information on referrals to antineoplastic treatment (type and duration of therapy, cumulative dose, combination therapy, therapy phase, and progression after treatment).
CTRCD was defined as the adverse effects of cancer treatment on the heart, encompassing both subclinical and clinical manifestations: (1) subclinical cardiotoxicity was detected using cardiac imaging, such as echocardiography and cardiac magnetic resonance imaging (MRI), and included reductions in LVEF, alterations in systolic and diastolic function, changes in myocardial strain or strain rate, increase of biomarkers as troponin T or brain natriuretic peptide, signals and symptoms of heart failure 13 ; (2) clinical cardiotoxicity was defined using the definition of the European Society of Cardiology: a decrease in LVEF of > 10% from baseline to < 50%. 14
The tool developed by the nominated Cardio-Oncology Study Group, the HFA-ICOS Score, 15 aims to stratify the risk of cancer patients previously exposed to antineoplastic therapies known to cause cardiac toxicity. There is a score for each antineoplastic therapy with the potential to cause cardiotoxicity. For this study, the scores for anthracycline and anti-HER2 chemotherapy were used.
This assessment stratifies patients into low, medium, high and very high risk of cardiovascular complications and includes various aspects such as previous CVD, cardiac biomarkers, previous use of anthracycline or anti-HER2 chemotherapy and radiotherapy, kidney disease, diabetes mellitus, hypertension, age, smoking and obesity. Each condition is scored with different scoring weights, and the sum of the points generates the risk level. 15
A sample size of 154 subjects was determined to investigate potential differences in percentages between groups with and without CTRCD. The calculation considered a power of 80%, a significance level of 5%, a percentage of 16%, and an odds ratio of 3.11, as indicated by Meral Gunaldi et al. 16 This calculation was carried out using the online version of the PSS Health tool. 17 Although the study design was retrospective, the sample size calculation was performed a priori to ensure statistical power for detecting clinically significant associations, following recommendations for observational analytical studies.
Continuous variables included age, body mass index (BMI), Charlson comorbidity index (CCI), chemotherapy duration, and LVEF measured before and after chemotherapy. Categorical variables comprised hypertension, diabetes mellitus, dyslipidemia, smoking status, breast cancer histological subtype, tumor stage, molecular profile, and HER-2 receptor status. Continuous variables were maintained in their original form to preserve statistical power and allow for more precise estimation of effects, while categorical variables were included as binary or ordinal predictors, depending on their clinical relevance and distribution in the cohort.
Categorical variables were reported as absolute and relative frequencies, and continuous variables were summarized as mean ± standard deviation (SD) or median and interquartile range (IQR), as appropriate. The normality of distribution of each variable was evaluated using the Shapiro-Wilk test. Categorical variables were compared by the chi-square or Fisher's exact test when indicated. Quantitative variables were compared by Student's t-test if normally distributed or Mann-Whitney U test if not normally distributed. Cox regression models were applied to obtain hazard ratio (HR) estimates, which were used for univariate and multivariable analyses adjusted for confounding variables. The Cox regression model was chosen because it accounts for both the occurrence and the timing of cardiotoxicity events, allowing the inclusion of censored data and providing more accurate risk estimates in this retrospective cohort. We utilized the criteria for multivariable analysis, where statistical significance was considered if the p-value was <0.10. In the survival analysis, a Kaplan-Meier curve was utilized to estimate the probability of outcomes over time, from the time from the initiation of chemotherapy treatment to the development of CTRCD. The collected information was added to the Research Electronic Data Capture (REDCap) database. Missing data were handled by excluding records with incomplete information on primary outcomes to avoid introducing bias. SPSS Statistics Software (version 25.0; IBM, Armonk, New York, USA) was used for data analysis. P-values <0.05 were considered statistically significant.
Results
The flowchart in Figure 1 illustrates the eligibility assessment for all patients (n = 449). Of these, 287 patients were excluded, and 161 patients were included in the analysis. Among these, 18 (11.1%) were diagnosed with clinical and subclinical CTRCD.
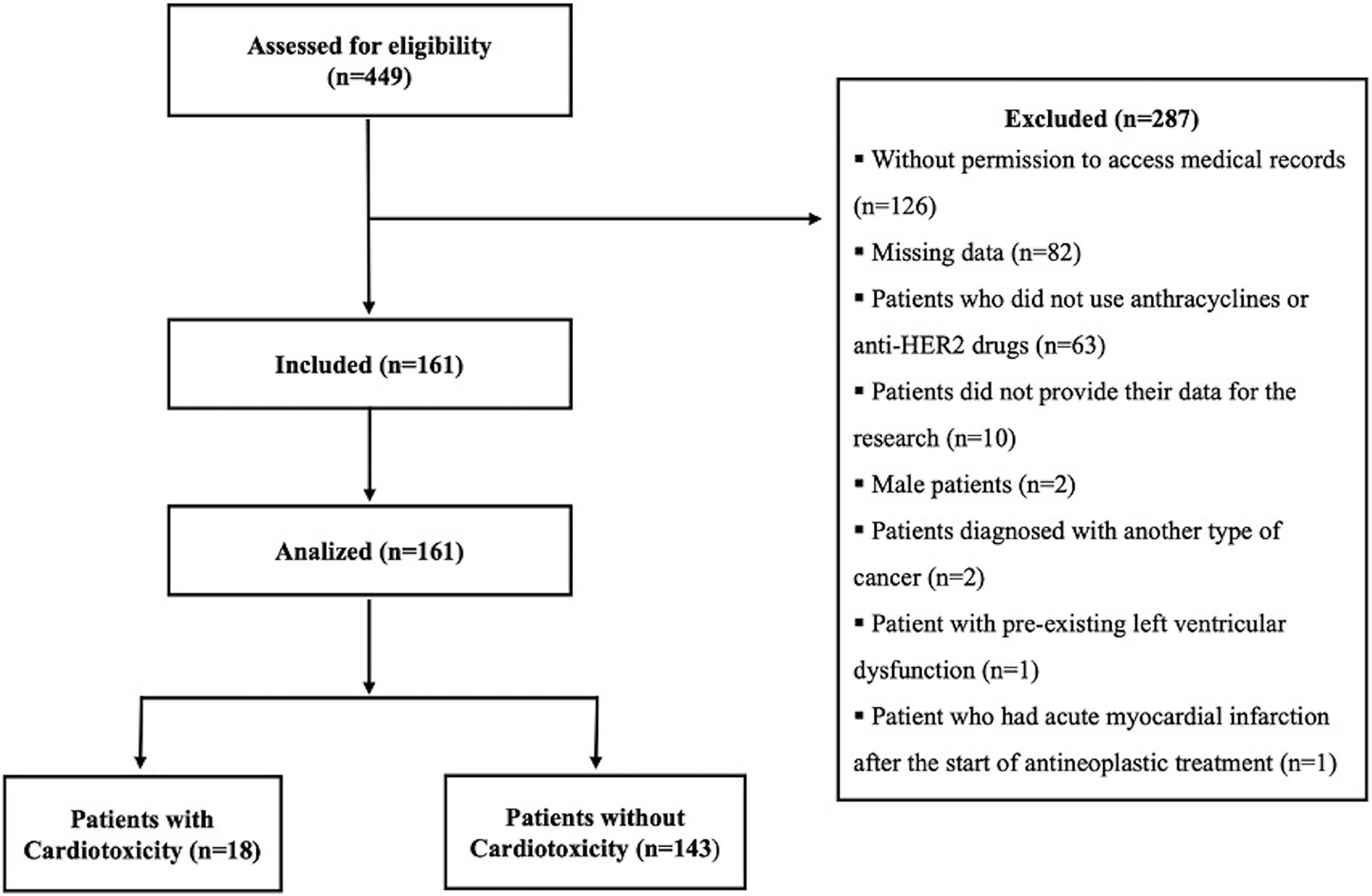
Flowchart of study population.
The mean (±SD) age of patients was 51.2 ± 11.6 years, with 135 patients (83.8% of whom were white/Caucasian). The median (IQR) CCI was 2(2–6) points. Hypertension (47.2%), obesity (31.7%), and smoking (31%) were the most common cardiovascular risk factors, and the mean (±SD) of BMI was 30 ± 5.7 kg/m2. The HFA-ICOS cardiovascular toxicity risk score was applied to patients and classified as low-risk (46.6%), medium-risk (47.2%), high-risk (4.9%), or very high-risk (1.2%). Thiazide diuretics (24.8%), angiotensin-converting enzyme inhibitors (21.1%), and angiotensin receptor blockers (18%) were the most common cardiovascular medications used by the patients prior to cancer diagnosis (Table 1).
Demographic and clinical characteristics of the patients (N = 161).
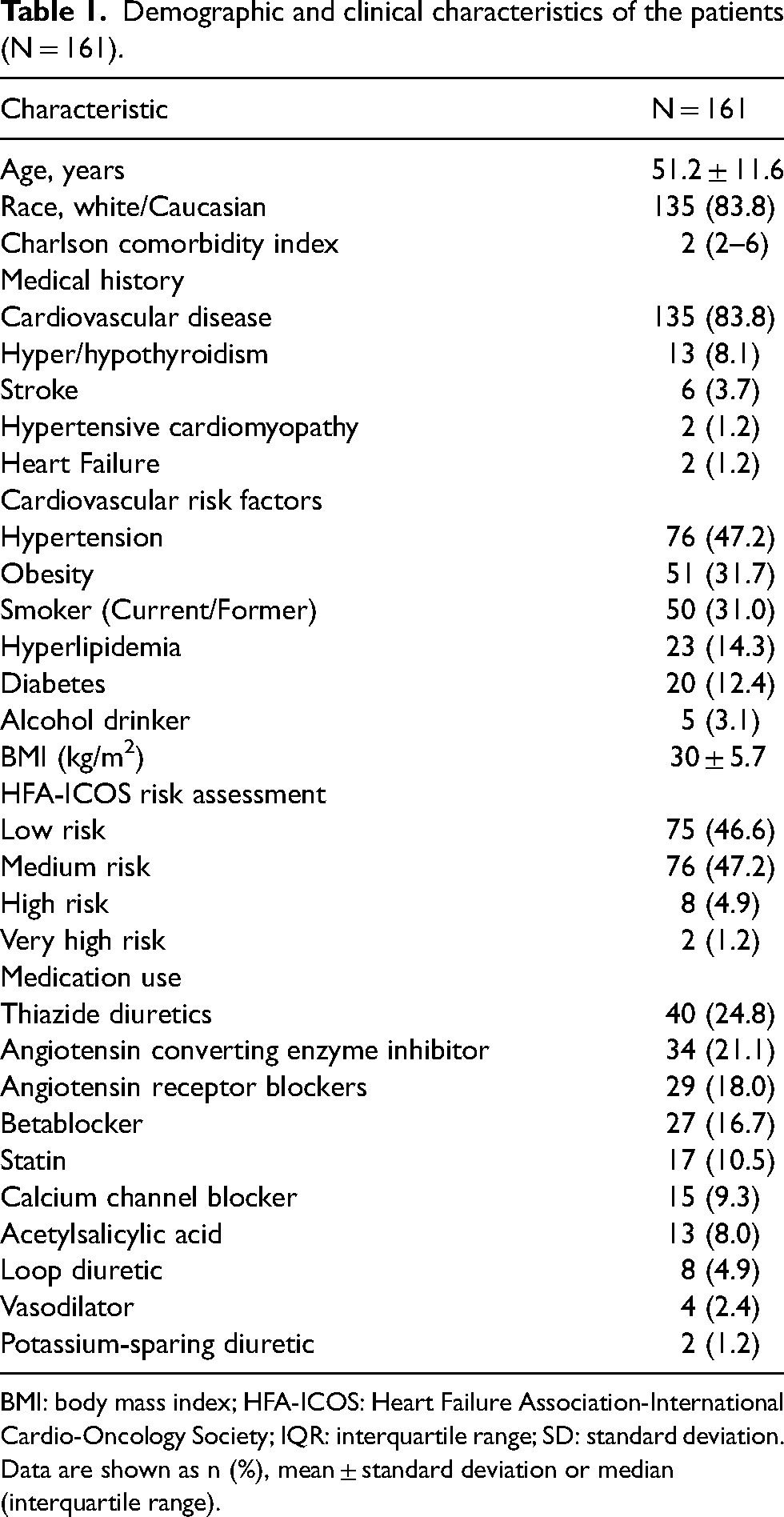
BMI: body mass index; HFA-ICOS: Heart Failure Association-International Cardio-Oncology Society; IQR: interquartile range; SD: standard deviation. Data are shown as n (%), mean ± standard deviation or median (interquartile range).
Regarding the oncological data, 6.2% of the patients had a history of solid-type cancer, and 5.6% underwent prior chemotherapy. Concerning the types of treatment, the patients performed neoadjuvant (n = 81, 50.3%), adjuvant (n = 76, 47.2%) or palliative care (n = 4, 2.4%). Among these patients, 153(96.8%) underwent breast surgery. The types of adjuvant curative treatment as radiotherapy (55.9%) and surgery (52.2%) adjuvants, proved to be the most prevalent. With respect to the additional risk factors studied, late menopause (after 55 years old) (n = 74, 46.0%) and oral contraceptive use (n = 58, 36%) were the most prevalent conditions. The complete data are shown in Table S1 (Supplementary data).
When observing antineoplastic treatment, anthracycline (doxorubicin) and anti-HER-2 therapy (trastuzumab) were the therapies of choice in most patients (81.9% and 40.9%, respectively). The most used antineoplastic protocols were dose-dense AC-T (anthracycline [doxorubicin] + cyclophosphamide + taxane [paclitaxel]) (n = 86, 53.4%) and AC-TH (anthracycline [doxorubicin] + cyclophosphamide + taxane [paclitaxel] + HerceptinTM [trastuzumab]) (n = 39, 24.2%). The mean (±SD) total cumulative dose of doxorubicin at the end of treatment was 418 ± 70 mg/m2, and 68.1% of patients received 17 cycles of trastuzumab (Table 2).
Antineoplastic protocols (N = 161).
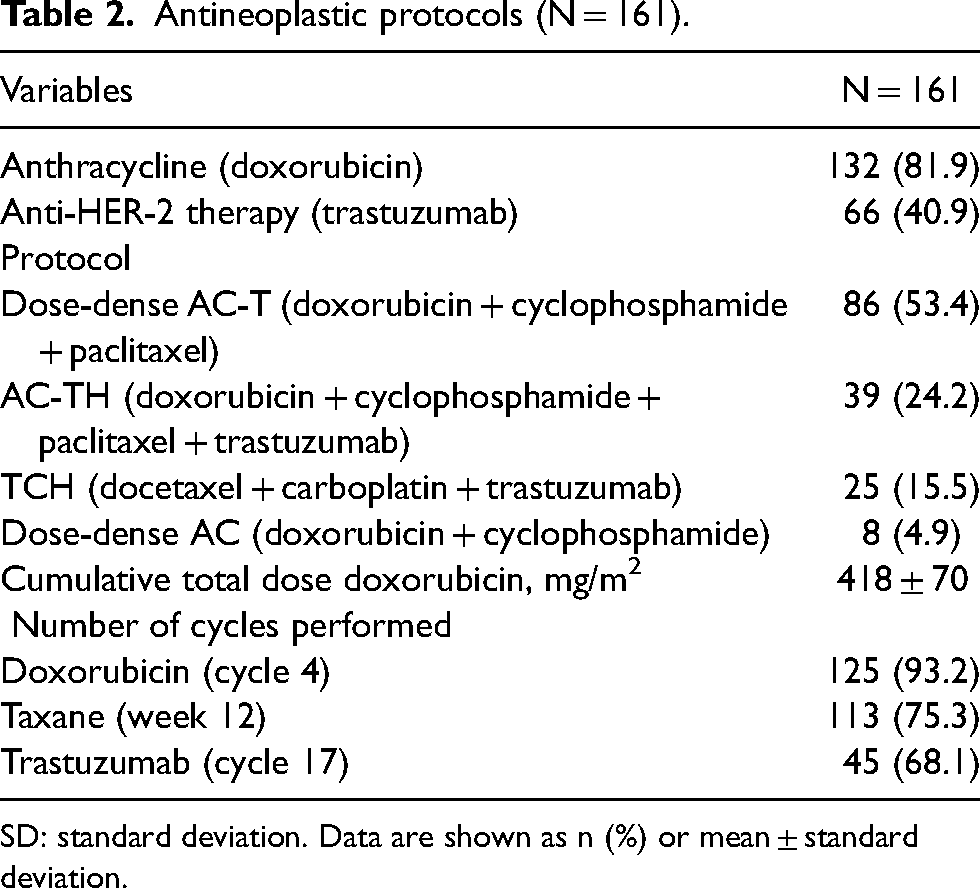
SD: standard deviation. Data are shown as n (%) or mean ± standard deviation.
The duration of chemotherapy for the studied antineoplastic drugs was 133 days (IQR: 47–352). A total of 130 patients (80.7%) underwent radiotherapy. Radiotherapy occurred concomitantly with chemotherapy in 41 patients (25.5%). The diagnosis of clinical 10(6.1%) and subclinical 8(5%) CTRCD was confirmed in 18 patients (11.1%). The mortality rate over follow-up period was 3.1% (n = 5), and of the total number of deaths, 3(61.3%) were attributed to progression disease and 1(38.7%) to infectious cause.
In patients diagnosed with clinical and subclinical CTRCD, the analysis of risk factor grouping (hypertension, diabetes, dyslipidemia, smoking, and obesity) revealed a higher prevalence (27.3%) in those with four or more risk factors (Figure 2).
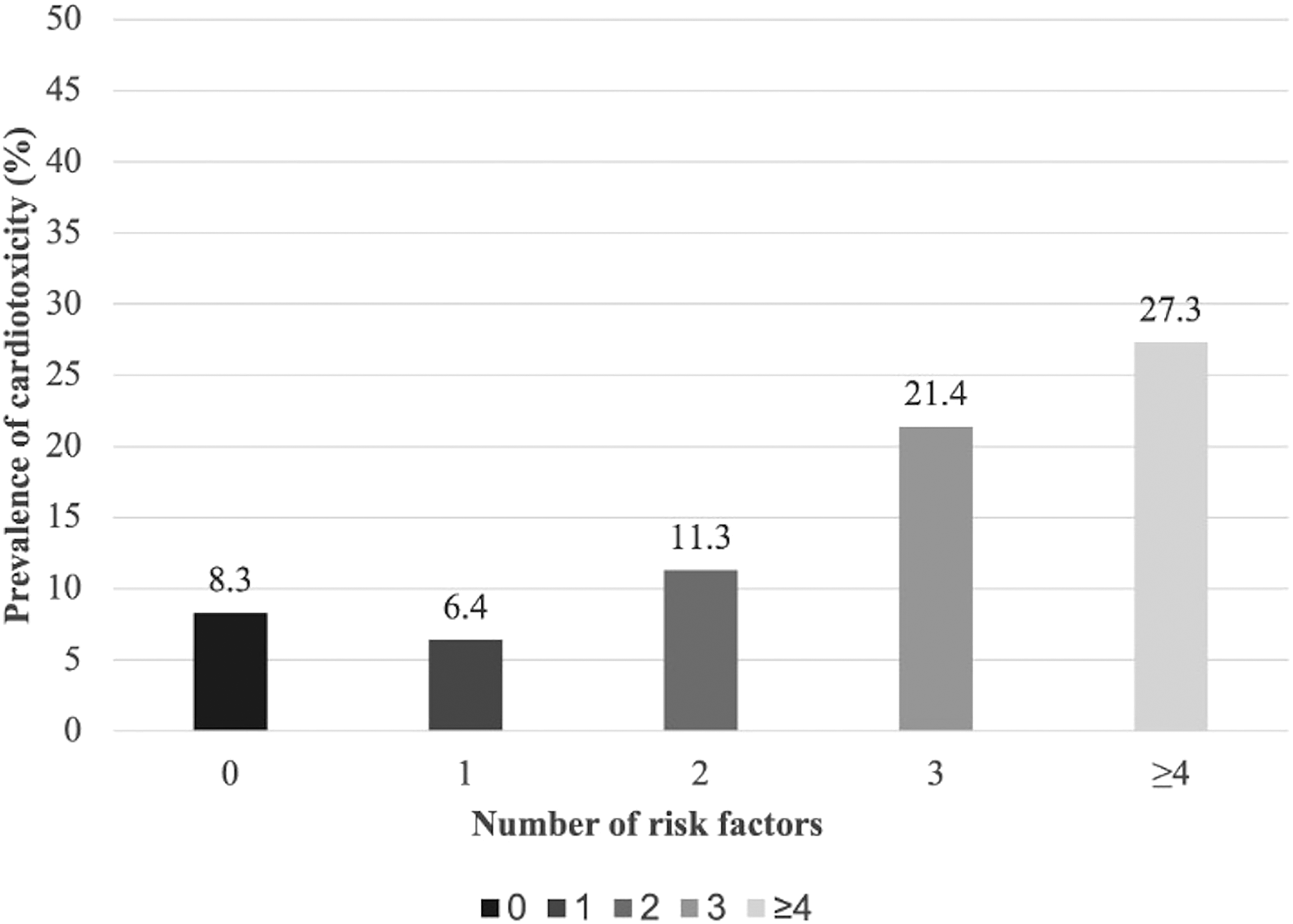
Prevalence of cardiotoxicity according to grouping of cardiovascular risk factors (n = 18).
Table 3 shows the association of cardiovascular risk factors and clinical characteristics with CTRCD. After a bivariate analysis, age (HR 1.0; 95%CI: 1.0–1.1), hypertension (HR 3.2; 95%CI: 1.1–9.2), diabetes (HR 2.6; 95%CI: 0.9–7.4), CCI (HR 1.1; 95%CI: 0.9–1.2), chemotherapy time (period that the patient performed chemotherapy in days) (HR 1.0; 95%CI: 0.9–1.0), LVEF before chemotherapy (HR 0.8; 95%CI: 0.7–0.9) and LVEF after chemotherapy (HR 0.8; 95%CI: 0.8–0.9), had strong, statistically significant effect on the cardiotoxicity of patients diagnosed with breast cancer who underwent treatment with anthracyclines and/or anti-HER-2 therapy.
Association of cardiovascular risk factors and clinical characteristics with cardiotoxicity (N = 161).
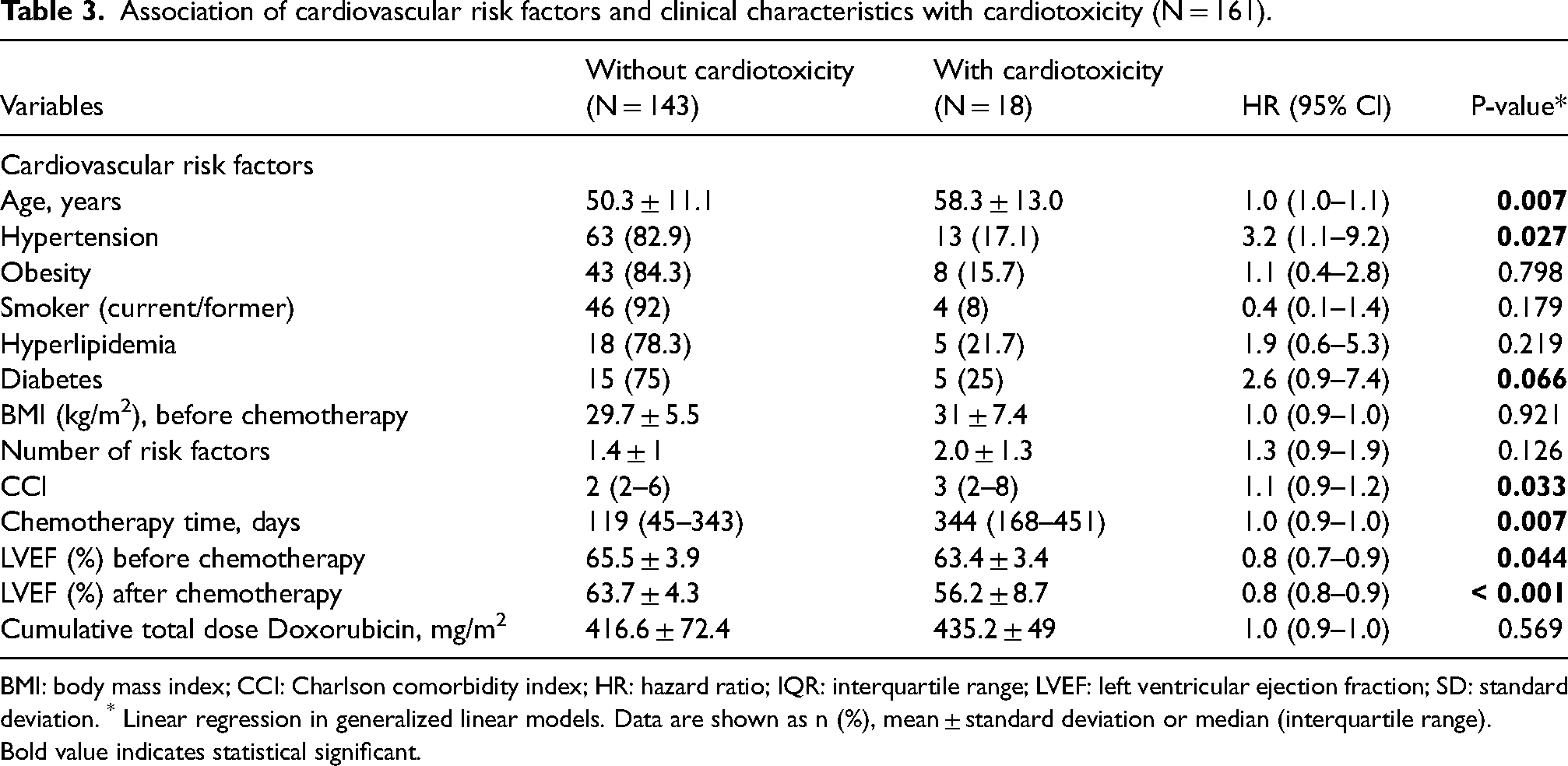
BMI: body mass index; CCI: Charlson comorbidity index; HR: hazard ratio; IQR: interquartile range; LVEF: left ventricular ejection fraction; SD: standard deviation. * Linear regression in generalized linear models. Data are shown as n (%), mean ± standard deviation or median (interquartile range). Bold value indicates statistical significant.
Among the seven variables that emerged as being significantly associated with CTRCD, considering P < 0.10, the results of multivariable analysis revealed four factors that maintained a significant association with cardiotoxicity even after adjusting for other variables: CCI (HR 1.2; 95% CI: 1.0–1.4; P = 0.002), chemotherapy time (HR 1.0; 95% CI: 1.0–1.0; P < 0.001), LVEF before chemotherapy (HR 0.8; 95% CI: 0.7–0.9; P < 0.001), and LVEF after chemotherapy (HR 0.8; 95% CI: 0.8–0.9; P < 0.001) (Table 4).
Multivariable analysis of cardiovascular risk factors and clinical characteristics in patients with breast cancer (N = 161).
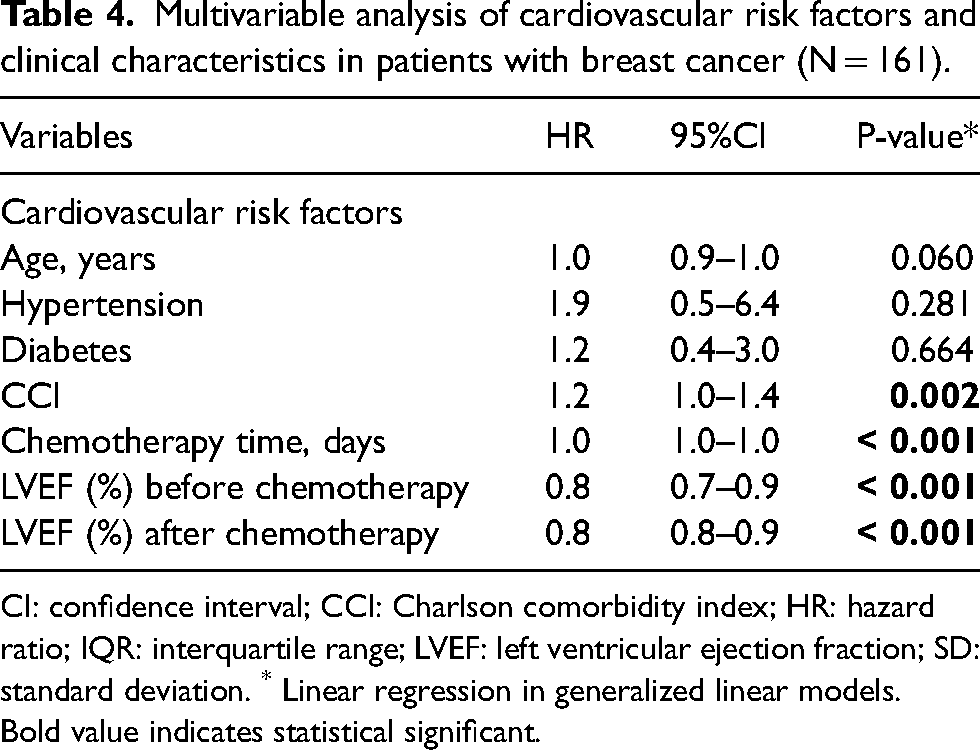
CI: confidence interval; CCI: Charlson comorbidity index; HR: hazard ratio; IQR: interquartile range; LVEF: left ventricular ejection fraction; SD: standard deviation. * Linear regression in generalized linear models. Bold value indicates statistical significant.
The median (IQR) time that elapsed between the start of chemotherapy treatment and the development of CTRCD was 395 (248–674) days. The likelihood of patients developing CTRCD was 17.7% in the first two years after starting antineoplastic treatment. Of a total of 18 cases of CTRCD, in 15 (83.3%) patients, this outcome occurred in the first two years of follow-up (Figure 3).
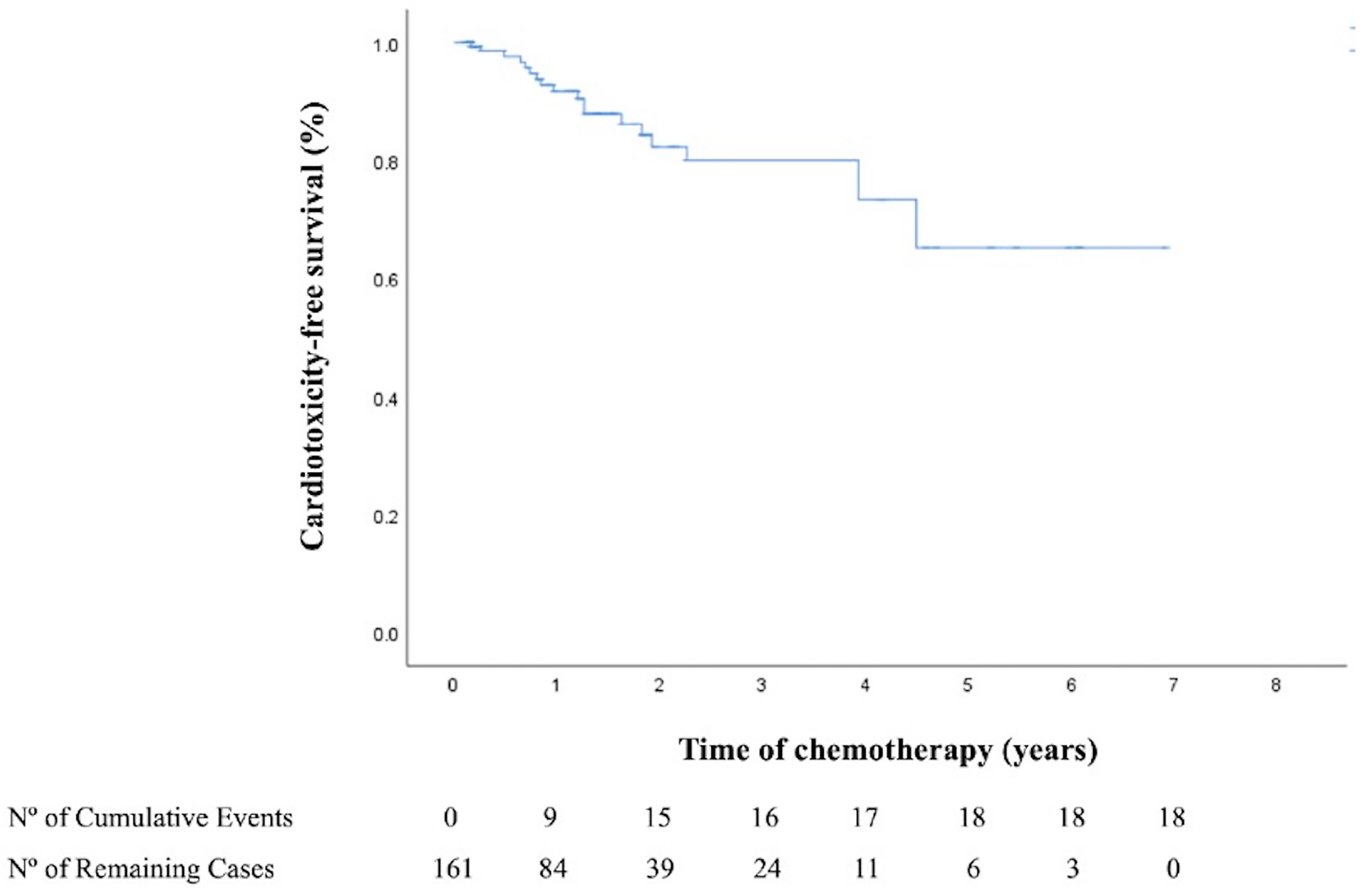
Kaplan–Meier curve showing cardiotoxicity-free survival according to the time of chemotherapy.
Discussion
In this study, CTRCD was observed in 11.1% of patients with breast cancer undergoing treatment with anthracyclines and/or anti-HER-2 therapies, with a particularly notable prevalence of 27.3% among those who exhibited four or more cardiovascular risk factors. This cohort comprised a heterogeneous population, including patients with various histological subtypes of breast cancer, predominantly invasive ductal carcinoma, as well as invasive lobular and tubular carcinomas. Most patients presented with stage II and III disease. The inclusion of different histological types and clinical stages reflects real-world clinical practice, ensuring greater external validity. 3 Importantly, current evidence suggests that the risk of developing CTRCD is primarily driven by the type of cancer therapy and preexisting cardiovascular risk factors, rather than tumor histology or stage alone. 5
Our research aligns with a previous study that examined 86 individuals diagnosed with breast cancer, all of whom maintained a preserved LVEF and underwent treatment with anthracyclines, trastuzumab, or a combination of both. The relative reduction in LVEF following chemotherapy was notably greater for patients with more than four risk factors compared to those without (−9.3 ± 10.8% vs. −2.2 ± 10.2%; P = 0.02). Furthermore, individuals with more than four risk factors exhibited a tendency towards a higher incidence of chemotherapy-induced cardiotoxicity compared to those without (14.3% vs. 2.8%; P = 0.12). 11
The predominant cardiovascular risk factors observed in our study were hypertension, obesity, and smoking. We also found that the CCI, chemotherapy duration, and LVEF before and after chemotherapy were independent risk factors for cardiac dysfunction. In a retrospective study, investigators observed a significant association between postmenopausal status, hypertension, obesity, prior coronary artery disease, and smoking with an elevated risk of cardiac dysfunction in women undergoing trastuzumab treatment. 16 These findings underscore the importance of closely monitoring cardiac health during breast cancer treatment, allowing tailoring of treatment plans based on individual patient risk profiles to minimize potential cardiac complications. 18
Several risk factors have been linked to cardiac dysfunction, including clinical and treatment-related factors. Clinical risk factors include age, pre-existing left ventricular dysfunction, hypertension, diabetes, and coronary artery disease. 19 Based on this information, a systematic review and meta-analysis aimed to establish a correlation between cardiovascular risk factors and the onset of trastuzumab-induced cardiotoxicity, and found that age (OR 0.7; 95%CI: 0.318–1.09), hypertension (OR 0.69; 95%CI: 0.26–1.12), smoking (OR 0.35; 95%CI: 0.01–0.69), diabetes (OR 0.44; 95%CI: 0.24–0.68), and a familial history of coronary artery disease (OR 5.51, 95%CI: 1.76–17.25), were significantly associated with increased susceptibility to cardiotoxicity. 12 We found in our study after a bivariate analysis, age (HR 1.0; 95%CI: 1.0–1.1), hypertension (HR 3.2; 95%CI: 1.1–9.2) and diabetes (HR 2.6; 95%CI: 0.9–7.4), had statistically significant effect on the CTRCD. However, the multivariable analysis revealed that they were not statistically associated with the outcome. These differences may be explained by the characteristics of the studies, populations, and treatments identified in the results of the systematic reviews and meta-analyses.
In addition to our main findings, we found that the median (IQR) duration from the initiation of chemotherapy to the onset of cardiotoxicity was 395 (248–674) days. Furthermore, the probability of patients experiencing cardiotoxicity within the first two years following treatment was 17.7%. This information offers valuable insights into the timeline during which the cardiotoxic effects may manifest in patients undergoing breast cancer therapy. Therefore, a group of researchers evaluated the incidence, timing, and response to heart failure therapy in patients receiving anthracycline-containing therapy. The study found that most cardiotoxicity cases occurred within the first year and were associated with anthracycline dose and LVEF at the end of treatment. 20 This emphasizes the significance of vigilant cardiac monitoring, particularly during the early phases of treatment. It is crucial for the recovery of cardiac function and reducing the risk of adverse cardiac.5,20
Our study has several limitations. First, being an observational study, it could establish associations, but not causation. Second, the inclusion of a population from a single center may restrict the generalizability of the findings. Third, the retrospective design and reliance on electronic medical records for variable collection could potentially introduce inaccuracies into the results. Fourth, alternative characteristics and risk factors for detecting cardiac dysfunction, such as serum biomarkers (brain natriuretic peptide and troponin) and electrocardiographic results, were not comprehensively recorded in electronic medical records, thereby limiting the scope of our analysis.
Conclusion
The predominant cardiovascular risk factors are hypertension, obesity, and smoking. Our study identified the CCI, duration of chemotherapy, and LVEF both before and after chemotherapy as pivotal independent factors influencing the likelihood of cardiac dysfunction in patients with breast cancer undergoing treatment with anthracyclines and/or anti-HER-2 therapies. These findings underscore the significance of considering a comprehensive array of variables to assess and understand the complex interplay between factors contributing to the risk of CTRCD in the studied population. Moreover, future studies would be welcome to determine whether optimization of modifiable risk factors prior to treatment can reduce the risk of CTRCD.
Supplemental Material
sj-docx-1-opp-10.1177_10781552251358183 - Supplemental material for Predictive risk factors associated with cancer therapy-related cardiac dysfunction: A retrospective cohort study
Supplemental material, sj-docx-1-opp-10.1177_10781552251358183 for Predictive risk factors associated with cancer therapy-related cardiac dysfunction: A retrospective cohort study by Bruna Brito Machado, Andreia Biolo, Fernando Pivatto Júnior, Alana de Quadros Schroeder and Marco Aurélio Lumertz Saffi in Journal of Oncology Pharmacy Practice
Footnotes
Author contributors
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
This study was partially funded by Hospital de Clínicas de Porto Alegre (Fundo de Incentivo à Pesquisa e Eventos; FIPE/HCPA), number 2021/0587.
ORCID iDs
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.