
Abstract
Many oral oncolytics inhibit rapidly dividing cells and are teratogenic. However, only a few agents are restricted under a Risk Evaluation and Mitigation Strategies (REMS) program due to embryo-fetal toxicity. The benefit of a REMS program for only select oral oncolytics is unclear.
Prior to 2007, the Food and Drug Administration (FDA) used Risk Minimization Action Plans (RiskMAPs) to minimize the risks for approved drugs. 1 RiskMAPs could provide education for providers, limit the distribution of medications, or implement patient safety programs. RiskMAPs were subsequently replaced by the Risk Evaluation and Mitigation Strategies (REMS) program, which was written into law in 2007. 2 The FDA was statutorily allowed to require manufacturers to establish a REMS program, as opposed to a RiskMAP, which was not written into law.
In 2011, an “Assessment of Risk Evaluation and Mitigation Strategies in Oncology” workshop hosted by the American Society of Clinical Oncology (ASCO) was conducted. Some key unintended consequences of REMS programs in oncology discussed included “REMS elements that do not consider existing, widely practice oncology safety standards, professional training and experiences” and “administrative burdens that divert the health care team from direct patient care activities and, in some cases, could limit patient access to important therapies.” Prior to the REMS strategies in oncology workshop, an ASCO member survey of 1311 respondents was conducted. More than half the respondents voted that “the negative impact of REMS administrative requirements outweigh and potential benefits to patients” and 41% responded that REMS did not add to patient safety. 3 The mandatory tasks for the REMS programs can be completed online though the REMS program portal which is significantly faster than using interactive voice response on the phone and talking to customer care representatives. 4 However, the online portal is sometimes non-functional, leading to an increase in administrative burden.
In June 2025, the FDA eliminated the REMS program for autologous CAR-T cell immunotherapies. The decision was based on the risk of CAR-T therapy not outweighing the benefits. Although CAR-T therapy is vastly different, the argument can be made that CAR-T therapy by far has more safety concerns than oral oncolytics.
Oral oncolytics have different mechanisms of actions at which they exert their effect on cancer cells such as targeting rapidly dividing cells for apoptosis. Due to these mechanisms, oral oncolytics can cause fetal harm by targeting the rapidly dividing cells of embryos leading to disruption of normal embryonic development. While most oral oncolytics do not have a REMS program for embryo-fetal harm, a select few do.
Currently, the only oral oncolytics with a REMS program for embryo-fetal toxicity are lenalidomide, pomalidomide, and thalidomide. All three agents fall into a class of agents called immunomodulatory drugs (IMiDs). The first IMiD, thalidomide, used as an antiemetic and sedative for pregnant women. 5 Thalidomide caused a worldwide scandal in the 1950s and 60s when it was found to cause birth defects. When lenalidomide was approved by the FDA in 2005 for myelodysplastic syndromes, it was required to have a RiskMAP program, which subsequently became a REMS program. 6 Pomalidomide and thalidomide were subsequently approved with similar requirements.
Currently, lenalidomide is FDA approved for multiple myeloma, myelodysplastic syndromes, and mantle cell lymphoma. 7 Off label indications for lenalidomide include chronic lymphocytic leukemia and other lymphomas such as diffuse large B-cell lymphoma, follicular lymphoma and marginal zone lymphoma.8–10 Pomalidomide is approved in multiple myeloma and Kaposi sarcoma. 11 Thalidomide is approved in multiple myeloma and moderate to severe erythema nodosum leprosum. 12
The average age of diagnosis of the cancers that these oral oncolytic agents are indicated for can vary, however many female patients will be diagnosed in the postmenopausal phase of life, with some exception. The median age of diagnosis for multiple myeloma is 69 years old. 13 The median age of diagnosis for Kaposi sarcoma is 74 years old, however for acquired immune deficiency syndrome (AIDS)-related Kaposi sarcoma the average age is 36 years old. 14 The median age of diagnosis for myelodysplastic syndromes and chronic lymphocytic leukemia is 70 years old.15,16 The median age of diagnosis for non-Hodgkin lymphoma and mantle cell lymphoma is 68 years old.17,18 The median age of diagnosis for these cancers exceeds the typical age of female patients with reproductive potential.
There does not appear to be a good rationale for why these three agents need to have a REMS program while other oral oncolytics are excluded, given that many can cause embryo-fetal toxicity. The female patients receiving these agents are more likely to be post-menopausal based on the average age of diagnosis of the given cancer the oral oncolytic is indicated for. Clinicians in oncology clinics should be counseling all oral oncolytic patients on embryo-fetal toxicity regardless of whether the medication has a REMS program. The package insert of every medication has a section specifically for female patients of reproductive potential. REMS programs for embryo-fetal toxicity add an additional administrative and operational burden for prescribers, patients, and pharmacies (Table 1) without providing much value.
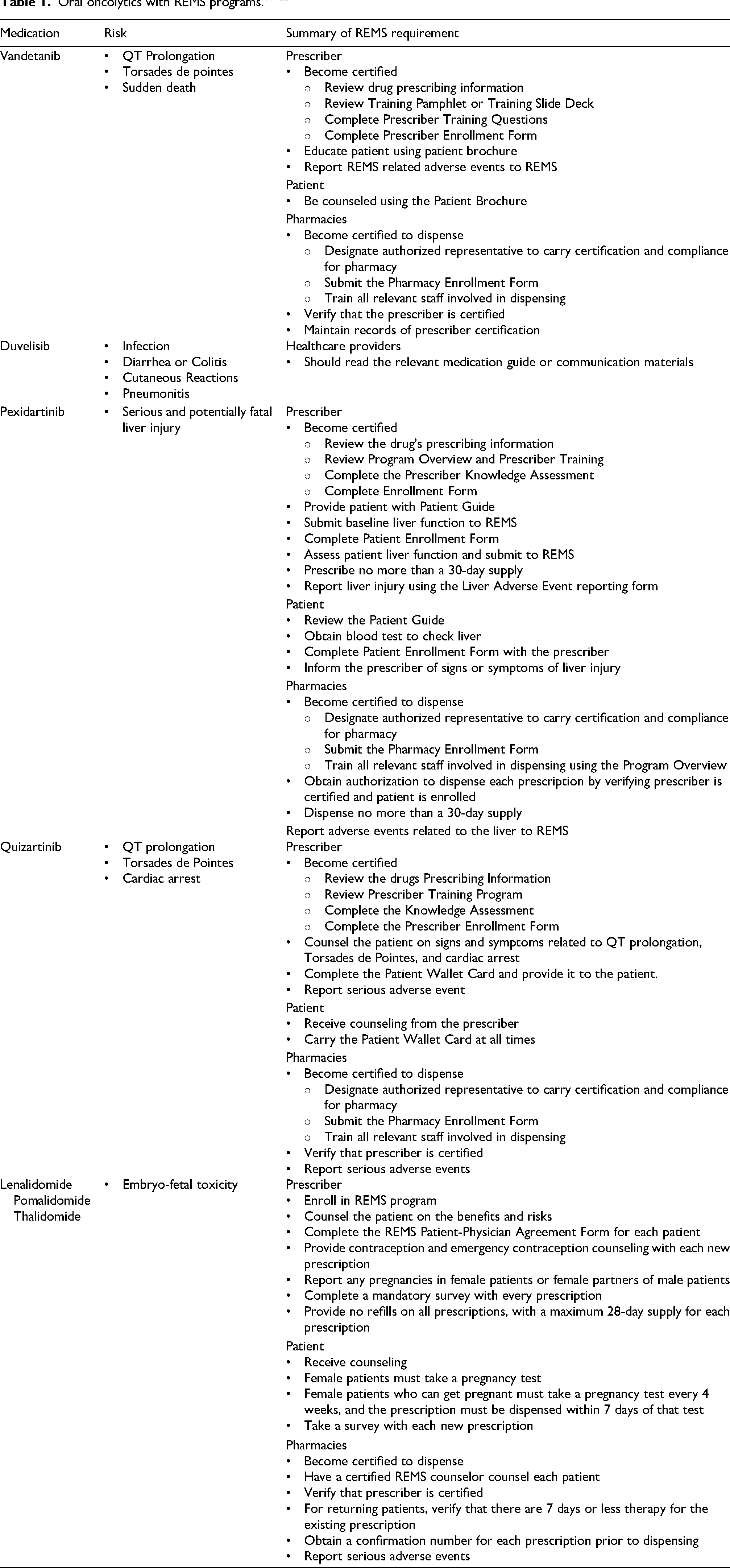
The IMiD REMS program also leads to delays in care. Prescribers must complete mandatory surveys with each new 28-day prescription due to the prohibition of no refills. All patients must complete monthly surveys, excluding females who cannot get pregnant. Prescribers and pharmacies must independently obtain an authorization number for each prescription written. Prescriptions must be dispensed within 7 days of a pregnancy test for female patients of reproductive potential. If a survey is not completed, an authorization number is not obtained, or a pregnancy test is not done at the right time, the medication cannot be dispensed to the patient. Furthermore, because only certain pharmacies are REMS program certified, patients must wait for the medication to be mailed to them, extending the time between diagnosis and treatment.
There has been published data on treatment delays with IMiDs, mostly with lenalidomide, as it is the most prescribed IMiD. A retrospective single-center study from a large safety net hospital found that 10.9% of lenalidomide prescriptions had a delay of >2 weeks from the date the prescription was written to the date it was dispensed. 26 After implementing a standardized workflow, the hospital was able to reduce that percentage to 4.4%. Another single-center study from a large hospital system found one in four newly diagnosed myeloma patients took more than 12 days to fill a lenalidomide prescription. 27 In addition, the number of pregnancy tests required by the IMiD REMS program – weekly for the first four weeks, then every 4 weeks for patients with regular menstrual cycles, or every 2 weeks for patients with irregular menstrual cycles – leads to false positives. A retrospective cohort study found that 2.2% of women of reproductive potential who were receiving lenalidomide reported a false positive pregnancy test. 28 False positive results lead to interruptions or delays in care and causes unnecessary patient stress. 29 Patients already have many barriers delaying their access to IMiDs – insurance authorizations, assistance programs, geographical distance – and the REMS program adds to these barriers.
The FDA should consider removing the REMS program for embryo-fetal exposure for all oral oncolytics. Embryo-fetal toxicity is a known and established side effect. While IMiDs caused a birth defect crisis over half a century ago, our medication practices today are much more robust. There is no public health need for lenalidomide, pomalidomide and thalidomide to have a REMS program, nor is there a need for any future oral oncolytics to have a REMS for embryo-fetal toxicity.
Footnotes
Author contributions
VH and MHT contributed equally to the writing of this manuscript. All authors reviewed and approved the final version of the manuscript.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.