
Abstract
To review pharmacology, pharmacokinetics, therapeutic use, product safety/description and perspectives on use of lutetium Lu 177 vipivotide tetraxetan in patients with metastatic castration-resistant prostate cancer (mCRPC).
Keywords
Introduction
Globally, prostate cancer is the second most frequently diagnosed cancer in men, and the incidence is expected to double worldwide by 2040.1,2 Because metastatic disease still lacks a cure, metastatic prostate cancer is the 8th leading cause of cancer-related deaths. 1 The rate of prostate cancer–related deaths is also expected to double in the next 2 decades. 2 Thus understanding new treatment options that are changing the outcomes for patients with metastatic prostate cancer is essential.
The treatment of metastatic prostate cancer can vary depending on whether the disease is castration-sensitive or castration-resistant. 3 Castration-sensitive disease is found in patients who are diagnosed with metastatic disease and have not been treated with long-term androgen deprivation therapy (ADT). Castration-sensitive prostate cancer eventually becomes castration-resistant when it no longer responds to therapies that target androgen suppression and continues to proliferate without androgen signaling. 4 Mechanisms leading to the progression of castration-resistant disease include increased androgen biosynthesis or use of adrenal androgen precursors; alterations of androgen receptor signaling which can be a result of androgen receptor mutations; androgen receptor variants that are constitutively active in absence of ligand, androgen receptor gene amplifications and overexpression, crosstalk with other signaling pathways, or reliance of other pathways.
Several systemic therapies are available for the treatment of metastatic castration-resistant prostate cancer (mCRPC), including chemotherapy (eg, docetaxel), androgen receptor pathway inhibitors (ARPIs; abiraterone, second-generation antiandrogens), targeted therapies (polymerase ADP ribose polymerase [PARP] inhibitors), and radiopharmaceuticals (eg, radium-223). These are selected for an individual patient based on previous treatment, tumor characteristics, and type of disease progression. 3 Although these treatments have been shown to delay disease progression, prolong survival, and improve quality of life, mCRPC is still incurable. Patients are often likely to receive many of these treatments throughout their lifetime.
Radiopharmaceuticals are increasingly used in the treatment of mCRPC and currently include radium-223 and lutetium Lu 177 vipivotide tetraxetan. Radium-223 (radium-223 dichloride) is a radionucleotide therapy that has been used to treat mCRPC since 2013. It delivers alpha, or short-particle length (<100 μm), radiation after it binds to areas of increased bone turnover, such as osteoblastic or osteoclastic metastases. 5 Radium-223 induces double-strand DNA breaks, delivering a highly specific and localized effect in only targeted areas, reducing potential toxic effects to surrounding tissue. The results of a randomized controlled trial comparing radium-223 to placebo, showed that 6 injections of radium-223 produced a longer overall survival (14 vs 11.2 mo), resulting in a 30% reduction in death (hazard ratio [HR] 0.70; 95% confidence interval [CI], 0.55–0.88; p < 0.001). 5 Both a higher quality of life and lower rates of adverse drug reactions occurred in those treated with radium-223 compared with placebo.
Lutetium Lu 177 vipivotide tetraxetan was more recently approved (in 2022) both in the United States and European Union for patients with prostate specific membrane antigen (PSMA)–positive mCRPC who have progressed after receiving docetaxel and ARPIs.6,7 Unlike radium-223, lutetium Lu 177 vipivotide tetraxetan is a beta emitting radiopharmaceutical, that delivers beta radiation to areas of the body that are expressing PSMA. PSMA, a protein that is normally expressed on the epithelium of prostate cells, in addition to other organs and glands, is highly expressed in prostate cells that are malignant, making it a good target for therapies as most metastatic lesions in patients with mCRPC are PSMA–positive.6,8 Metastatic PSMA-positive cells are detected using a PSMA-specific position emission tomography (PET)–computed tomography (CT) scan, which uses a PSMA-specific radioactive imaging agent that binds to highly expressed PSMA proteins and shows up on the scan. Lutetium Lu 177 vipivotide tetraxetan specifically targets malignant PSMA-positive and surrounding cells, causing DNA damage and cell death. 8
The purpose of this review is to provide an overview of lutetium Lu 177 vipivotide tetraxetan's pharmacology, pharmacokinetics, therapeutic use, product safety, product description and perspectives on use to understand the role of lutetium Lu 177 vipivotide tetraxetan in treating patients with mCRPC.
Data selection
A literature search was conducted using PubMed/Dynamed (October 2013 through May 2025). Keywords included Lu-177-PSMA-617, Lu 177 Vipivotide Tetraxetan, Lu 177 Vipivotide Tetraxetan AND cost, Lutetium-177–PSMA-617, Lutetium Lu 177 vipivotide tetraxetan AND mode of action. The search was limited to the English language, humans, clinical trials, case reports, and guidelines.
Pharmacology
Lutetium Lu 177 vipivotide tetraxetan (formerly known as 177Lu-PSMA-617) is a radiopharmaceutical that consists of the beta-emitting radioisotope lutetium Lu-177 linked to a peptide, vipivotide tetraxetan (ie, PSMA-617). 6 Vipivotide tetraxetan, a small molecular inhibitor, binds to the extracellular domain of PSMA expressed on cells, with high affinity. Then the beta emission from lutetium Lu 177 results in cell death of the PSMA-expressing cells and their surrounding environment.6,8 In addition to prostate cells which express PSMA, PSMA is also expressed on epithelium of other benign tissues, including kidney, lacrimal glands, liver, salivary glands, small and large bowel, and the spleen. 6 Thus, the radiation exposure of lutetium Lu 177 vipivotide tetraxetan is not limited to the PSMA-expressing prostate cells but potentially to all PSMA-expressing tissues, and also surrounding tissues and organs adjacent to PSMA-expressing tumors (due to the length of beta-wave radiation), and urinary system due to the urinary excretion of lutetium Lu 177 vipivotide tetraxetan. PSMA-negative tissues, however, are exposed transiently and minimally to lutetium Lu 177 vipivotide tetraxetan because of its rapid elimination. 9
Although the pharmacodynamic response has not been fully characterized, some information is known. Lutetium Lu 177 decays to a stable hafnium-177 in 6.647 days by primarily emitting beta-minus radiation (79%) and photonic radiation or gamma radiation (17.4%). 10 In the phase III VISION study, whole body and organ radiation dosimetry was calculated following 6 doses of 7.4 GBq of lutetium Lu 177 vipivotide tetraxetan. The highest absorbed radiation doses occurred in lacrimal glands (92 Gy), salivary glands (28 Gy), left colon (26 Gy), rectum (25 Gy), right colon (14 Gy), kidneys (19 Gy), and urinary bladder wall (14 Gy). Bone marrow had a 1.5 Gy dose. 8 Limited radiation occurs to surrounding tissue due to maximum penetration of approximately 2 mm, and mean penetration of 0.67 mm. 10
Pharmacokinetics
Following intravenous administration of lutetium Lu 177 vipivotide tetraxetan at the recommended dose of 7.4 GBq (200 mCi), the mean maximum blood concentration is 6.58 ng/mL and mean area under the curve (AUC) is 52.3 ng(h)/mL, which is increased with decreased creatinine clearance (CrCl). 10 The mean volume of distribution is 123 L, with lutetium Lu 177 vipivotide tetraxetan distributing to the bone marrow, gastrointestinal tract, heart, kidney, liver, lungs, and salivary glands within 2.5 h after administration. About 60–70% of the non-radioactive drug binds to plasma proteins.
Excretion of lutetium Lu 177 vipivotide tetraxetan occurs primarily through the kidneys.6,8,10 Concerns about cumulative renal radiation exposure led to an analysis of patients enrolled in the VISION study. 6 A higher incidence of toxicity, dose modifications and discontinuations were observed in those with moderate renal impairment (CrCl 30–59 mL/min) than those with mild impairment or normal renal function. In fact, grade 3 and 4 renal-related adverse drug reactions occurred more commonly in those with moderate renal impairment (14%) compared with mild impairment (2.9%) and normal function (1.4%). No patients with severe renal impairment were enrolled in this study.
Some other evidence exists for the renal safety in patients with compromised renal function and mCRPC. A subset analysis of 22 patients with decreased baseline renal function (estimated glomerular filtration rate (eGFR) < 60 mL/min) enrolled in a prospective patient registry, showed an improvement in renal function after therapy completion (mean GFR 45 [±10.7] to 53 [±16.7] mL/min). 11 Only one patient experienced a decrease in renal function. Additionally, 2 case reports demonstrate the safety in patients with reduced renal function. A 78-year-old patient with a 15-year history of mCRPC was referred to consideration with the use of lutetium Lu 177 vipivotide tetraxetan after progressing on docetaxel (PSA doubling after 1.4 months). 12 This patient demonstrated right renal outflow obstruction secondary to a nodal mass on the ureter, with an eGFR reduced to 16 mL/min/1.73 m2. After 4 cycles of 20% dose-reduced lutetium Lu 177 vipivotide tetraxetan, the patient responded to therapy showing a 97% reduction in PSA and a 61% reduction in tumor volume, an improvement in eGFR to 30 mL/min/1.73 m2, and no evidence of lutetium Lu 177 vipivotide tetraxetan–induced acute or chronic nephrotoxicity. Another case report supports the safety of lutetium Lu 177 vipivotide tetraxetan in a patient with single kidney function.13A 69-year-old patient, diagnosed with mCRPC, also showed left kidney mass but adequate kidney function (GFR > 50 mL/min/1.72 m2). After relapsing on enzalutamide, the patient received lutetium Lu 177 vipivotide tetraxetan with no dose reductions (3 cycles total; cumulative dose 19.5 GBq at 8 weeks) and no changes in renal function were noted. 13
While the effects of renal elimination do not seem to impact kidney function, a higher incidence of adverse drug reactions may occur. Initial dose adjustments are unnecessary for patients with mild to moderate renal impairment (CrCl 30–89 mL/min), but close monitoring is recommended.6,10 Effects of severe renal impairment have not been evaluated. During therapy if renal function significantly changes, a reduced dose is recommended (see Dosing section).
Lutetium Lu 177 vipivotide tetraxetan is not metabolized by the liver or kidney nor is it a cytochrome P450 substrate or transporter of breast cancer resistance protein (BRCP), p-glycoprotein, multidrug and toxin extrusion (MATE)1, MATE2-K, organic anion transporter (OAT)1, OAT3 or OCT2. It has a mean terminal elimination half-life of 41.6 h and clearance of 2.04 L/hour.8,10
Therapeutic uses
Lutetium Lu 177 vipivotide tetraxetan is an intravenous radiopharmaceutical (radioactive ligand), used for the treatment of adult patients with PSMA-positive mCRPC who have been previously treated with ARPI and taxane-based therapy.7,10 In the United States, it may also be used in those whom taxane-based therapy is indicated but can appropriately be delayed. 10 Its approval in the United States and within the European Union was originally based on a phase III, international, open label, randomized-controlled trial, the VISION trial. 14 When added to standard of care, overall survival was prolonged and progression of disease on imaging was delayed with limited adverse drug reactions (Table 1).14–24 A subsequent phase III, international, open-label, randomized-controlled trial (PSMAfore trial) showed that taxane-naïve patients with mCRPC who progressed after ARPIs experienced prolonged disease-free survival with lutetium Lu 177 vipivotide. 15
Phase II and III trials evaluating lutetium Lu 177 vipivotide tetraxetan.
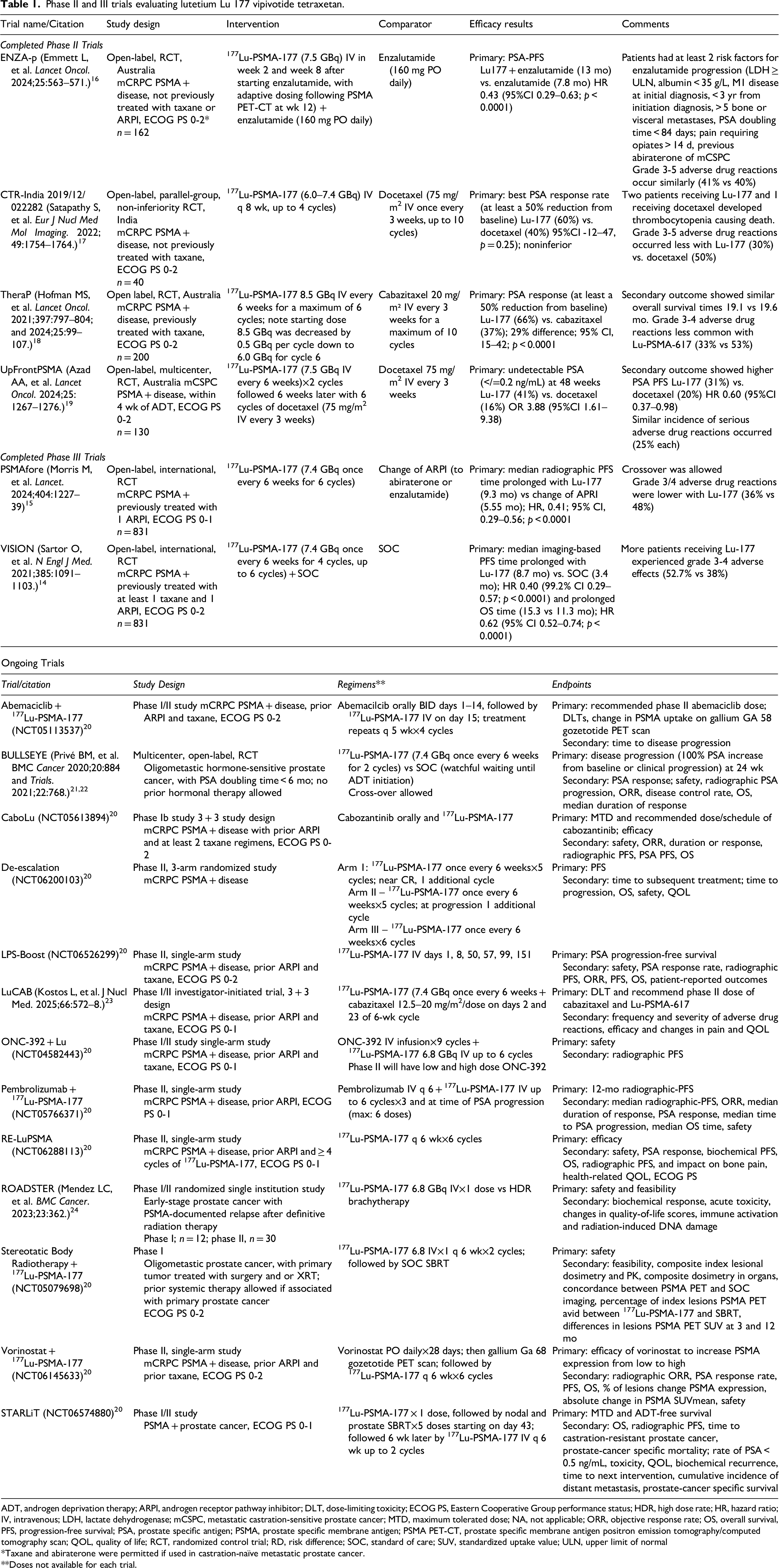
ADT, androgen deprivation therapy; ARPI, androgen receptor pathway inhibitor; DLT, dose-limiting toxicity; ECOG PS, Eastern Cooperative Group performance status; HDR, high dose rate; HR, hazard ratio; IV, intravenous; LDH, lactate dehydrogenase; mCSPC, metastatic castration-sensitive prostate cancer; MTD, maximum tolerated dose; NA, not applicable; ORR, objective response rate; OS, overall survival, PFS, progression-free survival; PSA, prostate specific antigen; PSMA, prostate specific membrane antigen; PSMA PET-CT, prostate specific membrane antigen positron emission tomography/computed tomography scan; QOL, quality of life; RCT, randomized control trial; RD, risk difference; SOC, standard of care; SUV, standardized uptake value; ULN, upper limit of normal
*Taxane and abiraterone were permitted if used in castration-naïve metastatic prostate cancer.
**Doses not available for each trial.
Vision trial
Within the VISION trial, eligible patients were required to be castrate-resistant, have at least 1 metastatic lesion confirmed through imaging (CT, MRI or bone scan) and disease progression following at least 1 ARPI and one taxane-based therapy. 14 Once deemed eligible, then patients underwent a 68Gallium (G8Ga)-PSMA-11 PET-CT (positron emission tomography-computed tomography) scan to identify areas with PSMA-expressing cells. Patients were excluded if presenting with no PSMA-positive lesion or more than or equal to 1 exclusionary PSMA-negative lesion, had previous PSMA-targeted radioligand treatment, any systemic anticancer therapy or investigational agent within the past 28 days prior to randomization, transfusion within the past 30 days, central nervous system metastases instability or other malignancy that would alter life expectancy. Patients with serious comorbidities, including New York Heart Association class III or IV congestive heart failure, were not included.
Of the 1179 patients assessed for eligibility, 1003 underwent 68Ga-PSMA-11 PET-CT, and 831 patients underwent treatment randomization. 14 Of those randomized, 551 patients were assigned to receive lutetium Lu 177 vipivotide tetraxetan 7.4 GBq (200 mCi) intravenously once every 6 weeks for 4 cycles (with 2 additional cycles permitted) plus standard of care, and 280 patients were assigned to receive standard of care alone. Standard of care therapy was determined prior to initiation and did not include cytotoxic chemotherapy, systemic radioisotopes (eg, radium-233), immunotherapy, or investigational drugs during the time of trial (eg, olaparib), but did include hormonal treatments, such as abiraterone and enzalutamide. Supportive care, including radiation therapy, bisphosphonates, denosumab, and corticosteroids, was permitted.
The most common site of metastases included bone (∼90%), followed by lymph node (∼50%), liver (∼12%), and lung (∼10%). 14 About 40% of patients that underwent randomization had a previous prostatectomy. Most patients had received one or 2 previous ARPIs, almost all patients had received docetaxel (∼97%), and about 40% also received cabazitaxel. The imaging-based progression free survival was 8.7 months in the patients treated with lutetium Lu 177 vipivotide tetraxetan compared to 3.4 months in the comparator group (HR 0.40; 99.2CI, 0.29–0.57; p < 0.001). Overall survival was prolonged (15.3 vs 11.3 mo; HR, 0.62; 95% CI, 0.52–0.74; p < 0.001). Secondary outcomes, including median time to first skeletal event, objective response, and disease control also were improved with lutetium Lu 177 vipivotide tetraxetan.
PSMAFore trial
In the PSMAFore trial, eligible patients had PSMA-positive, mCRPC with disease progression on abiraterone, apalutamide, darolutamide, or enzalutamide (see Table 1). 15 If the patient had received chemotherapy for castration-resistant or castration-naïve prostate cancer, they were ineligible, unless they had received as adjuvant or neoadjuvant therapy ≥ 12 months before randomization. Other ineligible criteria included immunotherapy other than sipuleucel-T, systemic radiation therapy < 6 months prior to randomization, or the presence of actionable genetic mutations for which approved therapies were available. Criteria for PSMA positive lesions were similar to VISION trial with the exception that intraprostatic lesions had to be PSMA positive in the PSMAFore trial.
Five hundred and eighty-five patients were assessed for eligibility, and 547 underwent 68Ga-PSMA-11 PET-CT, with 468 patients randomized. 15 Of those randomized, 234 patients were randomized to receive lutetium Lu 177 vipivotide tetraxetan 7.4 GBq (200 mCi) ± 10% intravenously once every 6 weeks for 6 cycles, and 234 patients were randomized to receive abiraterone or enzalutamide (standard dosing). Crossover to lutetium Lu 177 vipivotide tetraxetan was allowed upon meeting eligibility criteria.
The most common site of metastases included bone (∼88%), followed by lymph node (∼30%), lung (∼10%), and liver (6%). 15 About 50% of patients received 2 previous anticancer regimens, with approximately 50% of patients having received abiraterone and 35–40% of patients receiving enzalutamide previously. The median radiographic progression-free survival was 9.3 months in the patients treated with lutetium Lu 177 vipivotide tetraxetan compared to 5.5 months in ARPI group (HR 0.41; 99.2CI, 0.29–0.56; p < 0.0001). 15 An updated analysis at 24 months, showed continued improvement in radiographic progression-free survival (11.6 vs 5.59 mo; HR, 0.49; 95% CI, 0.39–0.61). Overall survival, the secondary outcome, was similar; 23.66 months versus 23.85 months with lutetium Lu 177 vipivotide tetraxetan and ARPI, respectively. Similar to the VISION study, lutetium Lu 177 vipivotide tetraxetan improved additional endpoints, such as time to symptomatic skeletal events, radiograph and PSA response rates and second progression-free survival on the next line of therapy.
Phase II trials
Several phase II trials have also been completed; 3 in patients with mCRPC and one trial in patients with metastatic castration-sensitive prostate cancer (see Table 1). The TheraP trial compared lutetium Lu 177 vipivotide tetraxetan to cabazitaxel in patients for whom cabazitaxel was considered to be the next appropriate standard treatment after receiving docetaxel previously. 18 Compared with cabazitaxel, lutetium Lu 177 vipivotide tetraxetan provided a higher PSA-response rate, defined by a reduction in PSA by 50% from baseline (66% vs 37%; p < 0.0001). A study conducted in India by Satapathy and colleagues, compared the efficacy and safety of lutetium Lu 177 vipivotide tetraxetan and docetaxel in chemotherapy-naïve mCRPC patients. 17 This study demonstrated noninferiority of lutetium Lu 177 vipivotide tetraxetan to docetaxel with an improved higher 50% reduction in PSA (60% vs 40%; p = .025). The ENZA-p trial evaluated the combination of enzalutamide and adaptive-dosing lutetium Lu 177 vipivotide tetraxetan compared with enzalutamide alone in patients with clinical risk factors for early progression on enzalutamide monotherapy. 16 In this study the combination improved PSA progression-free survival times (13 mo vs 7.8 mo; p < 0.0001).
The UpFRONTPSMA trial evaluated lutetium Lu 177 vipivotide tetraxetan followed by docetaxel compared to docetaxel treatment alone in men with castration-sensitive prostate cancer with PMSA-positive disease who had initiated androgen deprivation therapy within 4 weeks before randomization. 19 The combination improved the likelihood of an undetectable PSA level at 48 weeks compared with docetaxel alone (41% vs 16%).
Several other ongoing phase I and II trials are evaluating lutetium Lu 177 vipivotide tetraxetan combined with other agents, including abemacicilb, cabozantinib, cabazitaxel, ONC-392, a novel, target-preserving anti cytotoxic T-cell antigen 4 (CTLA-4) inhibitor, pembrolizumab, and vorinostat in patients with mCRPC after progression following ARPI and/- taxane therapy (see Table 1).20,23 Other studies are evaluating lutetium Lu 177 vipivotide tetraxetan combined with radiation therapy in early-stage prostate cancer, or alone in patients with oligometastatic disease.21–24 Finally, 3 ongoing trials are evaluating different dosing strategies including, intensified dosing (days 1, 8, 50, 57, 99, 141) de-escalation, and retreatment. 20 More details of these studies can be found in Table 1.
Dosing
The recommended dose for lutetium Lu 177 vipivotide tetraxetan is 7.4 GBq (200 mCi) intravenously every 6 weeks for up to 6 doses. 10 Before and after administration of lutetium Lu 177 vipivotide tetraxetan, the amount of radioactivity of the vial or prefilled syringe should be confirmed with an appropriate dose calibrator. Doses used in completed phase II studies ranged from 6–8.5 GBq and ongoing studies are evaluating a variety of dosing strategies (see Table 1).
Lutetium Lu 177 vipivotide tetraxetan may be administered by slow intravenous push, using a syringe, or by infusion, using gravity or peristaltic pump. 10 All administration is done within the nuclear medicine department (not by nursing staff) due to radioactivity. Full directions for each administration method can be found in the prescribing information, but special differences are highlighted here. When administering lutetium Lu 177 vipivotide tetraxetan with a syringe, it is slowly pushed over 1 to 10 min, through an intravenous catheter that is primed with 0.9% sodium chloride. Using the gravity method, lutetium Lu 177 vipivotide tetraxetan is administered by intravenous catheter (primed with 0.9% sodium chloride), using a clamp or infusion pump to regulate the flow. The dose should be administered within approximately 30 min. When using the peristaltic infusion pump, lutetium Lu 177 vipivotide tetraxetan is administered at approximately 25 mL/h. With each administration, the catheter should be flushed with 0.9% sodium chloride.
Based on the drug's prescribing information, a reduced dose is recommended in patients who experience significant changes in renal function during therapy as a result of an adverse event while on therapy. 10 The dose would be reduced to 5.9 GBq/160 mCi in patients with at least a 40% confirmed increase in serum creatinine from baseline and at least a confirmed 40% decrease in CrCl (calculated using the Cockcroft-Gault equation with actual body weight) from baseline.
Lutetium Lu 177 vipivotide tetraxetan has also been effective and proven safe use in older adults. Both in the VISION and PSMAfore studies, more than 70% of patients were 65 years and older, and nearly 30% of patients were 75 years or older.14,15 Efficacy and toxicity were similar, regardless of age.
Product handling
Lutetium Lu 177 vipivotide tetraxetan is available as a 1000 MBq/mL (27 mCi/mL) single dose vial for injection and a prefilled syringe, either 10 mL or 20 mL, each with total of 7.4 GBq (200 mCi ± 10%). 10 Drug handling should be consistent with good institutional radiation safety practices; radiation exposure to patients, medical personnel and household contacts should be minimized. Best practices are that healthcare providers who are qualified and trained for safe use and handling of radiopharmaceuticals are involved in the preparation and administration of this product. 25 Typically, government or regulatory agencies will authorize the license of radiopharmaceuticals within an institution. The application process will vary depending on the local regulations. Often an internal institutional radiation safety board will need to approve the addition of a radiopharmaceutical to its formulary, which can take weeks to months.
Medical personnel should use waterproof gloves and effective radiation shielding, safety glasses, a lab coat, and use tongs when handling lutetium Lu 177 vipivotide tetraxetan. 10 Minimal time spent near the radioactive product is recommended. Inspection for particulate matter prior to administration under shielded screen should be completed; discard if present. Radioactivity should be measured with a radiation detection device on all personnel who handled the product before leaving the administration area.
Lutetium Lu 177 vipivotide tetraxetan vials must be stored below 30 degrees Celsius, in the original package to protect from ionizing radiation. 10 The shelf life is 120 h (5 days) from calibrated date/time. Any unused product or waste needs to be stored to allow time for decay and then disposed of in accordance with the local and federal regulations/laws.
Safety
Based on phase III trial data, the most common adverse drug reactions are asthenia/fatigue (23–43%), dry mouth (39–58%), nausea (32–35%), and anemia (27–32%).14,15 However, severe (grade 3 and 4) adverse drug reactions are uncommon. In the VISION trial, with more heavily pretreated patients, the most common grade 3 and 4 adverse drug reactions included anemia in 12.9%, thrombocytopenia in 7.9%, lymphopenia in 7.8%, and fatigue in 5.9% of patients. 14 In the PSMAfore trial, with patients who had not had previous chemotherapy, the most common grade 3 or higher adverse drug reaction was anemia, occurring in 6% of patients. 15 Few patients required interruption or discontinuation of treatment; 12% of patients experienced an adverse drug reaction that led to treatment interruption, and 6–12% of patients discontinued therapy because of an adverse drug reaction.14,15
Because of the small risk of myelosuppression, including anemia, thrombocytopenia, leukopenia, or neutropenia, with the administration of lutetium Lu 177 vipivotide tetraxetan, complete blood counts should be performed before starting therapy and before each dose. 10 Lutetium Lu 177 vipivotide tetraxetan administration should be held if grade 2 or higher myelosuppression occurs until improvement to grade 1 or to baseline. A 20% dose reduction of lutetium Lu 177 vipivotide tetraxetan to 5.9 GBq should occur in those experiencing grade 3 or higher myelosuppression. If recurrent grade 3 or higher myelosuppression occurs after one dose reduction, permanent discontinuation of lutetium Lu 177 vipivotide tetraxetan is recommended.
Acute kidney injury was rare in phase III studies (1.3–3.4%), but with the potential for vomiting and diarrhea as well, it is important to monitor renal function regularly before and during treatment.10,14,15 Additionally, patients should be advised to remain well hydrated and urinate frequently before and after lutetium Lu 177 vipivotide tetraxetan administration. 10
In patients who are experiencing dry mouth, the use of a sodium bicarbonate mouthwash during the first 3 days following treatment can be helpful. 26 A commercial formulation can be used, or the patient could mix ½ teaspoonful of baking soda in 1 cup of warm water. Encouraging good oral hydration is also very important. The use of a saliva gel to stimulate salivary flow may be useful or hard candy, gum, or xylitol can be used.
No contraindications exist. Radiation exposure risk, embryo-fetal toxicity and infertility, however, are a potential concern. 10 Lutetium Lu 177 vipivotide tetraxetan does contribute to the cumulative radiation exposure, which is a known risk factor for the development of cancer. The risk, however, is quite low and is comparable to that of diagnostic X-ray imaging. 26 This risk can be minimized with proper institutional safety practices and appropriate instructions for patients (Table 2).6,10,26 Bladder radiation exposure can be minimized by ensuring the patient increases oral fluid intake and frequent voiding following administration. Additionally, the patient should limit close contact (defined as less than 3 feet) with others for 2 days and with children and pregnant women for 7 days following treatment administration. Additionally, sexual activity should be refrained for 7 days, and patients should sleep in a separate bedroom from others, children, and pregnant women for 3, 7, and 15 days, respectively. After each administration, the patient should also be given a radiation safety card that details the treatment, including radioactivity amount. 26 This can be useful when traveling or when the patient has to see other medical personnel (eg, primary care). Disposal precautions must be used. During the first week, any items that cannot be flushed, such as incontinence or sanitary pads, and bandages, should be placed in a specific plastic trash bag and can be thrown into the usual household waste after 70 days.
Recommendations for patients following lutetium Lu 177 vipivotide tetraxetan administration. 26
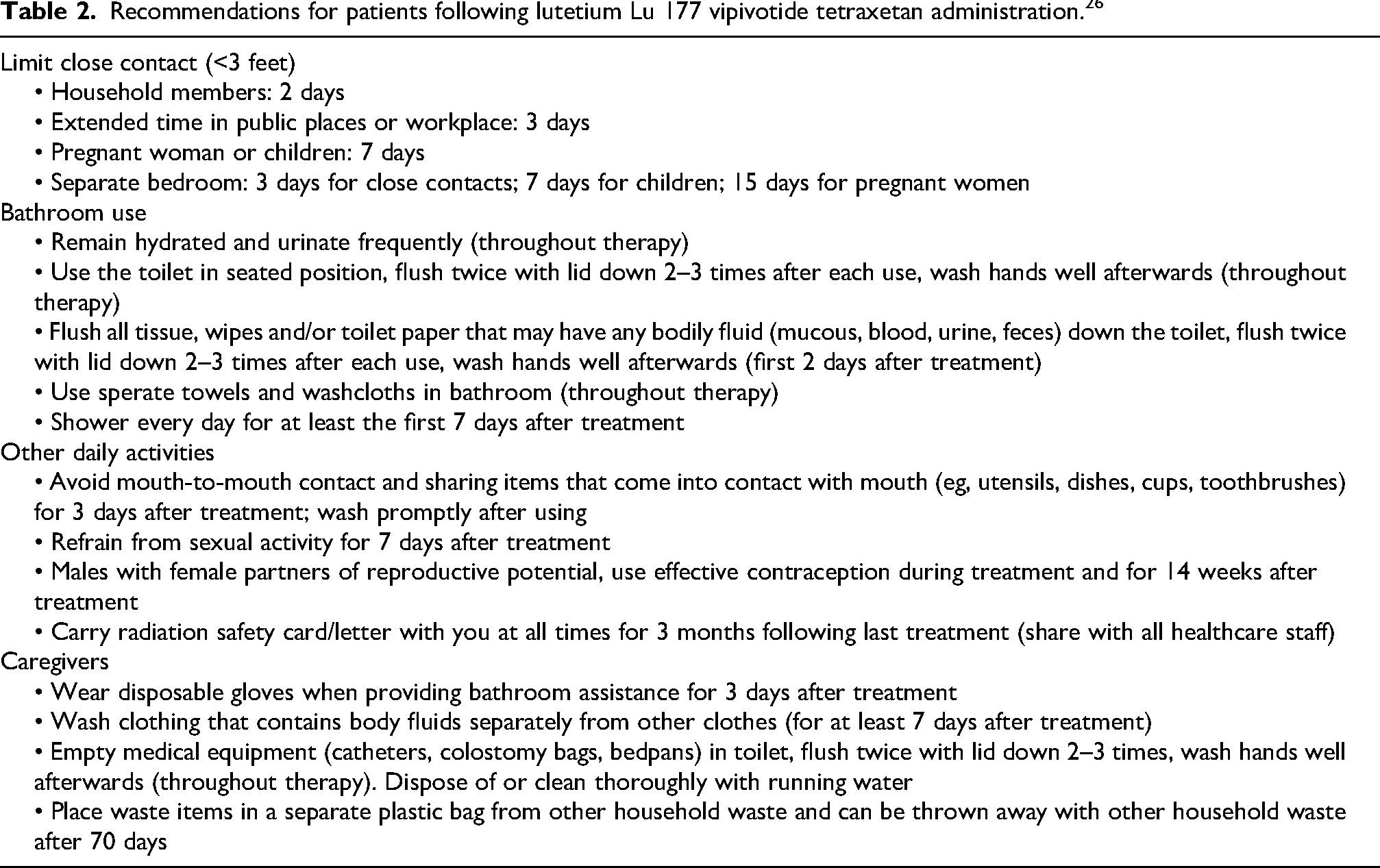
For patients with urinary incontinence, the risk of radiopharmaceutical exposure is higher. In these patients, it is recommended that they use incontinence pads that are changed frequently to avoid exposure and radiation burns from urinary leakage. 26 Similarly, those with nephrostomy bags or Foley catheters, will require specific equipment and proper handling by healthcare professionals.
Because of the risk of fetal harm, male patients with female partners of reproductive potential are recommended to use effective contraception during and for at least 14 weeks following the last dose of lutetium Lu 177 vipivotide tetraxetan. 10 Additionally, lutetium Lu 177 vipivotide tetraxetan may cause temporary or permanent infertility in males.
No known drug interactions have been reported with lutetium Lu 177 vipivotide tetraxetan. In vitro studies showed no induction or inhibition of common cytochrome P450 enzymes. Additionally, vipivotide tetraxetan is not a substrate of cytochrome P450 enzymes and transporters. A theoretical risk of added immunosuppression or myelosuppression could occur with drugs that suppress the immune system, but none have been reported.
Perspectives on use
According to the National Comprehensive Cancer Network (NCCN) guidelines for the treatment of prostate cancer, lutetium Lu 177 vipivotide tetraxetan is an appropriate treatment for patients with mCRPC and PSMA-positive metastases after progressing on either an ARPI or both an ARPI and docetaxel therapy, based on the VISION and PSAMFore trials. 3 These recommendations are category 2A, meaning they are based on lower-level evidence but uniform NCCN consensus, defined as 85% or more of panelist agree intervention is appropriate in select populations. The European Society of Medical Oncology (ESMO) guidelines for prostate cancer recommend lutetium Lu 177 vipivotide tetraxetan as an appropriate treatment for patients with mCRPC and PSMA-positive metastases after progressing on both an ARPI and docetaxel therapy, based on the VISION trial. 27 This recommendation is category IA, meaning it is based on evidence from at least 1 large randomized, controlled trial of good methodology with strong evidence for efficacy by providing a substantial clinical benefit. The ESMO guideline did not include use after progression with an ARPI because the guideline was created before the PSMAFore trial was published.
The options for patients with mCRPC are many even after progression on an ARPI and/or docetaxel, including PARP inhibitors for patients with homologous recombinant repair gene mutations (primarily BRCA mutations), pembrolizumab for patients with high microsatellite instability/deficiency in mismatch repair genes or high tumor mutation burden, sipuleucel-T, taxanes (cabazitaxel or docetaxel rechallenge), radium-223, and mitoxantrone. Most of these options, however, were not evaluated in patients with PSMA-positive disease, as this is a diagnostic method that is relatively new, approved by the U.S. Food and Drug Administration (FDA) in 2020 for more accurate detection of prostate cancer. Additionally, the optimal sequencing of these agents is unknown. It seems reasonable based on current evidence to consider lutetium Lu 177 vipivotide tetraxetan in patients who have progressed on at least on one ARPI and for those who do not have BRCA mutation, for which high quality evidence exists for use of a PARP inhibitor in those patients.3,27
When selecting a second- or subsequent-line therapy regimen, it is always important to consider all aspects of the therapy. Overall, lutetium Lu 177 vipivotide tetraxetan was well tolerated in the VISION and PSMAFore trials.14,15 Most patients had low-grade adverse drug reactions, manageable with appropriate monitoring and supportive care. The toxicity profile of lutetium Lu 177 vipivotide tetraxetan may be desirable when comparing with other treatment options, such as taxanes. Furthermore, it has a limited number of administrations (6) as opposed to ongoing therapy with many of the other options (mitoxantrone PARP inhibitors, pembrolizumab, taxanes) which continue until disease progression.
It is also important to note the high costs of lutetium Lu 177 vipivotide tetraxetan. Its average wholesale price for one dose of 7.4 GBq is approximately $52,000 US dollars; or $312,000 for treatment. A cost-effectiveness analysis was performed using data from the VISION trial and setting the willingness-to-pay threshold at $50,000, $100,000, and $200,000 per quality adjusted life years and a lifetime horizon of 60 months. 28 Patients treated with lutetium Lu 177 vipivotide tetraxetan were estimated to gain 0.42 incremental quality-adjusted life years, with a cost-effective ratio of $200,708 per quality-adjusted life years. Whether this benefit will be seen when lutetium Lu 177 vipivotide tetraxetan is used after progression on ARPIs alone or as the drug is on the market longer is unknown.
Despite the benefits of lutetium Lu 177 vipivotide tetraxetan, this may not be available to all patients as it does require the institution to have qualified and trained personnel and safe radiation procedures in place for storage, delivery, and administration. 26 In fact, multidisciplinary collaboration is crucial for safe use. Furthermore, the patient must be able to follow safe practices following administration, such as keeping distance from family members, appropriate bathroom use (see Table 2). This may be difficult or even impossible for some patients, such as those in a long-term care facility. Thus, careful consideration to all aspects of lutetium Lu 177 vipivotide tetraxetan are needed when considering this treatment option.
Summary
Lutetium Lu 177 vipivotide tetraxetan is an option for treatment of patients with mCRPC and PSMA-positive metastases after progressing on an ARPI ± docetaxel. Trials have demonstrated that 6 cycles of lutetium Lu 177 vipivotide tetraxetan improves median radiographic progression-free survival and prolong overall survival times compared with standard of care or taxane therapy.14,15 It is generally well tolerated, with asthenia/fatigue, dry mouth, mild nausea and low-grade anemia most commonly occurring. Because lutetium Lu 177 vipivotide tetraxetan is a radiopharmaceutical it should only be administered by trained personnel in a designated clinical setting in nuclear medicine with existing radiation safety protocols in place. Further studies are ongoing to determine safety and efficacy in earlier stages of the disease and with different dosing strategies, which will better define the role of this therapy in the treatment of prostate cancer.
Footnotes
Acknowledgments
None
Author contributions
Both authors contributed to all aspects of the manuscript, including: Conception and design; Collection and assembly of information; Information analysis and interpretation; Manuscript writing; and Final approval of manuscript. Both authors are accountable for all aspects of the work.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Data sharing statement
Data sharing not applicable to this article as no datasets were generated or analyzed during the current study