
Abstract
Introduction
National guidelines for breast cancer support substitution with nab-paclitaxel for paclitaxel or docetaxel due to medical necessity. 1 This study aimed to assess for correlation between weekly nab-paclitaxel dose and relative dose intensity (RDI) amongst early breast cancer patients.
Methods
This single-center, retrospective cohort study included adult patients with early breast cancer who switched from weekly paclitaxel to nab-paclitaxel after hypersensitivity reaction. The primary outcome of RDI was assessed in patients receiving nab-paclitaxel 80 mg/m2 (NB80) or 100 mg/m2 (NB100) intravenously (IV) weekly. Secondary outcomes included adverse effects, incidence of nab-paclitaxel alterations, and growth factor (GCSF) administration for secondary prophylaxis.
Results
Amongst 26 patients, the median age was 43 years (range 33 to 71), with the majority (54%) having stage II or later disease. Median RDI with NB80 was 91% (range 69 to 100%) versus 86% (55 to 100%) with NB100. Fifty percent of all patients underwent dose reductions. Dose delays occurred in a higher proportion of patients on 50% with NB80 vs 33% with NB100. Early nab-paclitaxel discontinuations occurred more on NB100 (33% vs 10%). Incidence of chemotherapy-induced peripheral neuropathy (CIPN) was 80% vs 83% with NB80 and NB100, respectively, while grade 2 CIPN was more common on NB100 (50% vs 35%). A lower rate of neutropenia resulted from NB80 (60 vs 67% with NB100).
Conclusion
Nab-paclitaxel dosed at 80 mg/m2 IV weekly, after switching due to paclitaxel hypersensitivity, may promote improved RDI and safety compared to nab-paclitaxel 100 mg/m2 weekly amongst early breast cancer patients.
Background
Taxanes are key backbone agents in nearly all systemic chemotherapy regimens for early breast cancer. Paclitaxel and docetaxel are associated with hypersensitivity reaction rates of up to 10% (including severe reactions) despite appropriate pre-medication use.2,3 Current NCCN Guidelines® for breast cancer allow for substitution with nab-paclitaxel due to medical necessity, namely after a hypersensitivity reaction (HSR) secondary to paclitaxel or docetaxel. 1 Dosing recommendations for nab-paclitaxel are limited to a proposed maximum weekly dose of 125 mg/m2. 1 At Fred Hutchinson Cancer Center (FHCC), weekly nab-paclitaxel is dosed at 80 mg/m2 or 100 mg/m2 depending on multiple factors, including stage of disease, treatment intent, concomitant chemotherapy agents, adverse effects from prior treatments, additional comorbidities, and provider preference. Because of the lack of specific guidance from guidelines and literature, there is no standardization of nab-paclitaxel dosing amongst patients with breast cancer.
Nab-paclitaxel is most often substituted for paclitaxel, as lower efficacy and increased adverse effects from the weekly docetaxel arm of the ECOG1199 trial have led to the rarity of its use. 4 As one must consider the actual exposure to a planned course of treatment when evaluating its efficacy, relative dose intensity (RDI) is an emerging value for the quantification of this comparison. 5 RDI is defined as the ratio of the delivered dose intensity (dose per unit body surface area per unit time) to the planned dose intensity of a chemotherapy regimen, and studies have shown it is positively correlated with survival outcomes in solid tumor patients. 6
There are currently no published trials comparing different strategies for switching to weekly nab-paclitaxel in the neoadjuvant or adjuvant treatment of early breast cancer. This study aimed to assess for a correlation between nab-paclitaxel dose, relative dose intensity, and adverse effect incidence amongst patients with early breast cancer. It was hypothesized that using nab-paclitaxel 100 mg/m2 weekly would result in a lower RDI than nab-paclitaxel 80 mg/m2 weekly due to increased incidence of adverse effects.
Methods
Study design
This IRB-approved single-center, retrospective cohort study was conducted via chart review of the electronic health record (EHR) system. The study period of interest was April 1, 2021, to August 1, 2024. Outcomes were compared between patients who received nab-paclitaxel 80 mg/m2 weekly (NB80) versus nab-paclitaxel 100 mg/m2 weekly (NB100) for early stage breast cancer.
Patients
Patients were included if they were 18 years or older with early stage breast cancer. Included patients were planned to receive a fixed-duration weekly paclitaxel regimen before switching to nab-paclitaxel due to a hypersensitivity reaction during Cycle 1 Day 1 or Cycle 1 Day 8 only. Patients were included regardless of chemotherapy agents being given concurrently with weekly paclitaxel. Patients were excluded if paclitaxel dose was reduced at baseline, treatment was initiated with nab-paclitaxel, they were pregnant, or there was a significant alteration in their treatment course due to a non-taxane adverse effect. Pertinent baseline characteristics, such as age, ethnicity, body mass index, diagnosis of diabetes, performance status, cancer stage, and intended chemotherapy regimen, were collected.
Outcomes
The primary outcome was the relative dose intensity of weekly nab-paclitaxel therapy—calculated as:
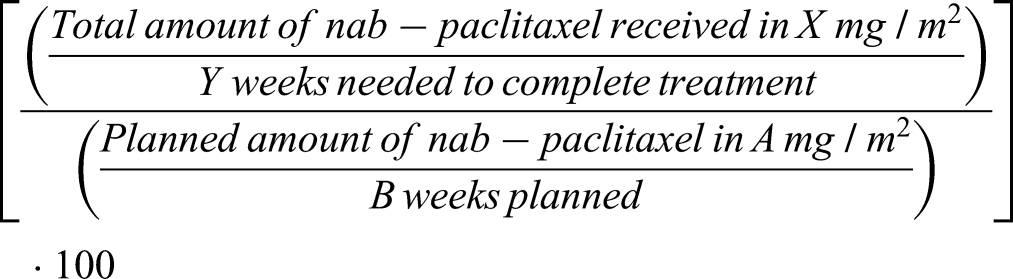
Secondary outcomes included: the incidence of adverse events; the incidence, amount, and reason for nab-paclitaxel dose reductions, delays, or discontinuations; administration of granulocyte colony stimulating factor (GCSF) for secondary prophylaxis; persistence of nab-paclitaxel-related adverse events beyond 6 months from the last administered dose; and total nab-paclitaxel received. Retrospective grading of all adverse events was performed based on the Common Terminology Criteria for Adverse Events (CTCAE) v5.0. 7
Statistical analysis
Descriptive statistics were used to characterize the study population and outcomes.
Results
Of the 51 patients screened, 26 subjects were identified and included in the main analysis comparing nab-paclitaxel 80 mg/m2 weekly to nab-paclitaxel 100 mg/m2 weekly (n = 20 and n = 6, respectively), as seen in Figure 1. Most patients were excluded due to having switched to nab-paclitaxel after C1D8 of paclitaxel; the reason for switching was rash in 17 of those 21 patients (Figure 1). Patient demographics and characteristics are presented in Table 1. All patients were female, and a majority (77%) were Caucasian. Median age was similar between groups; however, 45% of the NB80 arm were greater than 50 years old compared to no patients older than the age of 50 in the NB100 arm. Performance status was similar between groups (70% on NB80 and 66% on NB100 ECOG Score of 0), while 65% of patients on NB80 had stage II or greater disease at diagnosis compared to 17% on NB100 (83% stage I). More patients on NB80 received 2 or more cytotoxic chemotherapy agents in addition to nab-paclitaxel compared to NB100 (60 vs 34%).
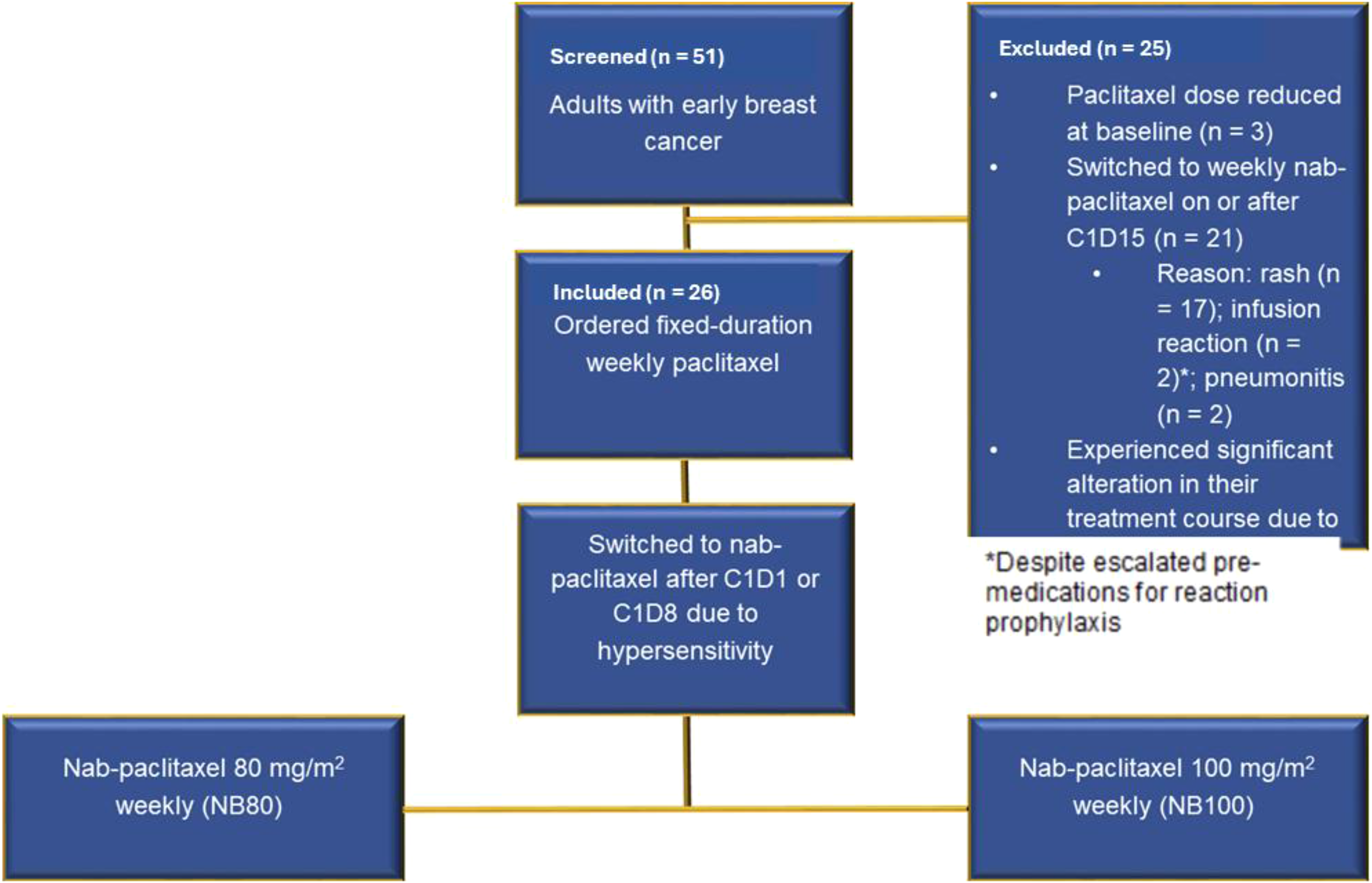
Patient selection and exclusion.
Baseline characteristics.
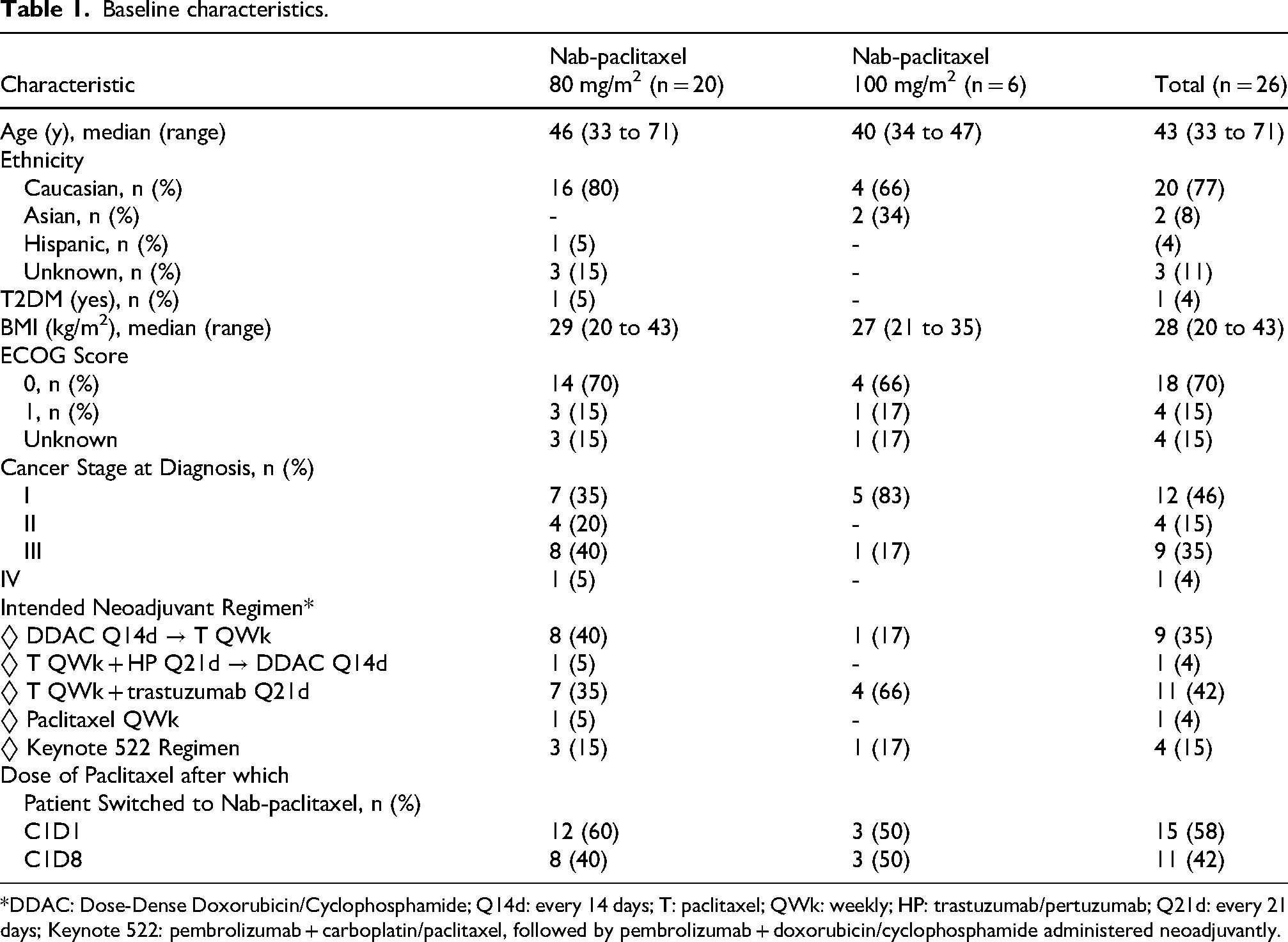
*DDAC: Dose-Dense Doxorubicin/Cyclophosphamide; Q14d: every 14 days; T: paclitaxel; QWk: weekly; HP: trastuzumab/pertuzumab; Q21d: every 21 days; Keynote 522: pembrolizumab + carboplatin/paclitaxel, followed by pembrolizumab + doxorubicin/cyclophosphamide administered neoadjuvantly.
Relative dose intensity achieved with NB80 vs NB100 is presented in Figure 2. Median RDI with NB80 was 91% (range 69 to 100%) versus 86% (range 55 to 100%) with NB100. Further characterization of the RDI with each dosing regimen is presented through the incidence of nab-paclitaxel alterations in Table 2. The same proportion of patients underwent dose reductions in both groups (50%). Median (range) percent reduction for the first dose reduction occurrence was 20% (10 to 25%) with NB80 and 20% (10 to 36%) with NB100 (Table 2). Fewer patients required a second dose reduction when initially on 80 mg/m2 compared to 100 mg/m2 (10 vs 17%). CIPN was the main reason for dose reduction overall and within the NB80 arm (54%). Dose delays occurred in a higher percentage of patients on NB80 (50% vs 33% with 100 mg/m2); however, 6 of 10 dose-delays with NB80 and 1 of 3 with NB100 were deemed unrelated to nab-paclitaxel (Table 2). When correcting for unrelated delays, median RDI achieved with NB80 weekly increased by 6%, while there was no change in median on NB100 [median (range) 97% (69 to 100%) vs 86% (59 to 100%)]. Nab-paclitaxel discontinuation occurred in a higher proportion of patients on NB100 (33 vs 10%). Total nab-paclitaxel received was comparable between groups [median (range) 800 mg/m2 (680 to 960 mg/m2) with NB80 vs 880 mg/m2 (764 to 1110 mg/m2) with NB100]
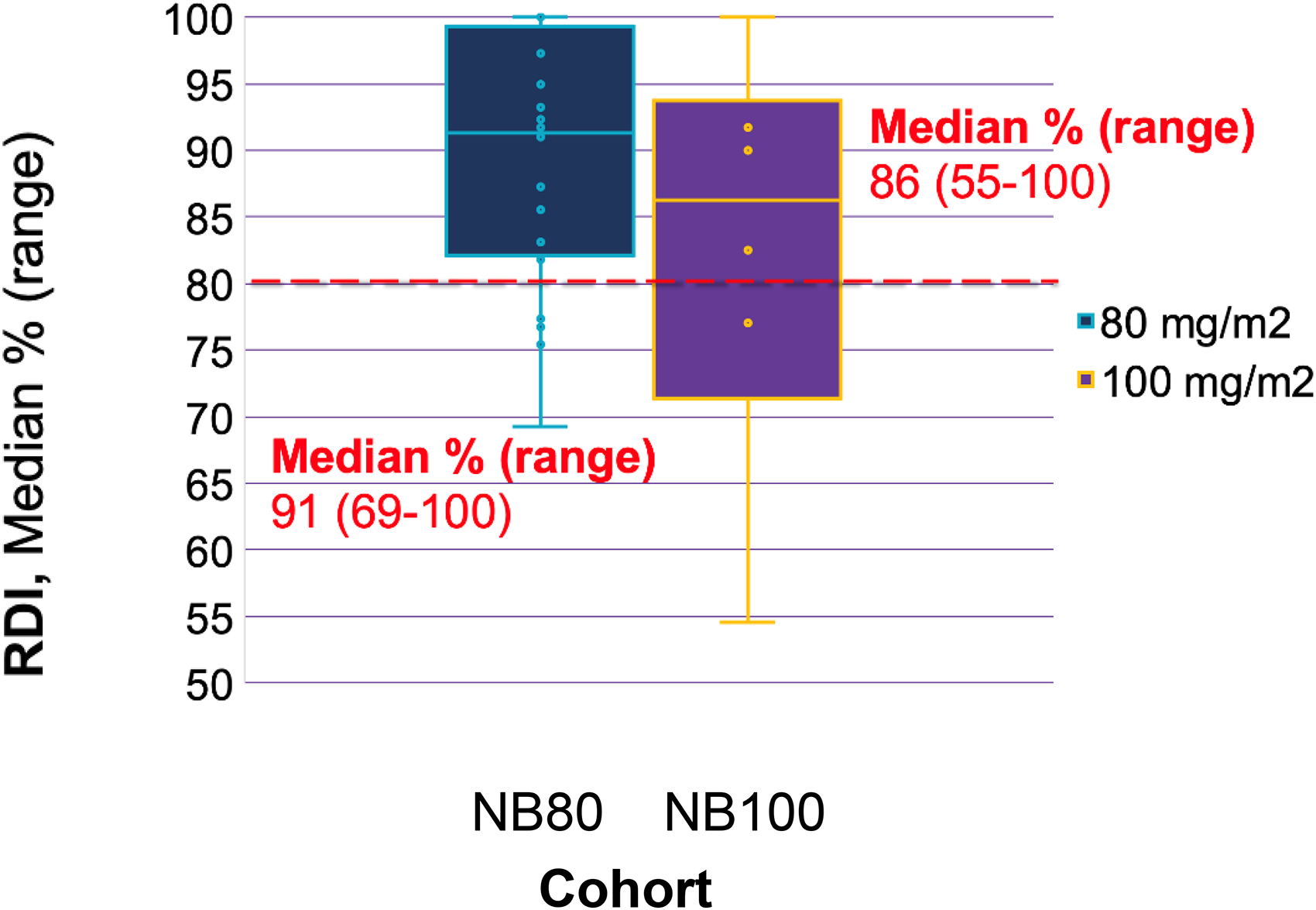
Relative dose intensity of nab-paclitaxel.
Incidence of nab-paclitaxel alterations.
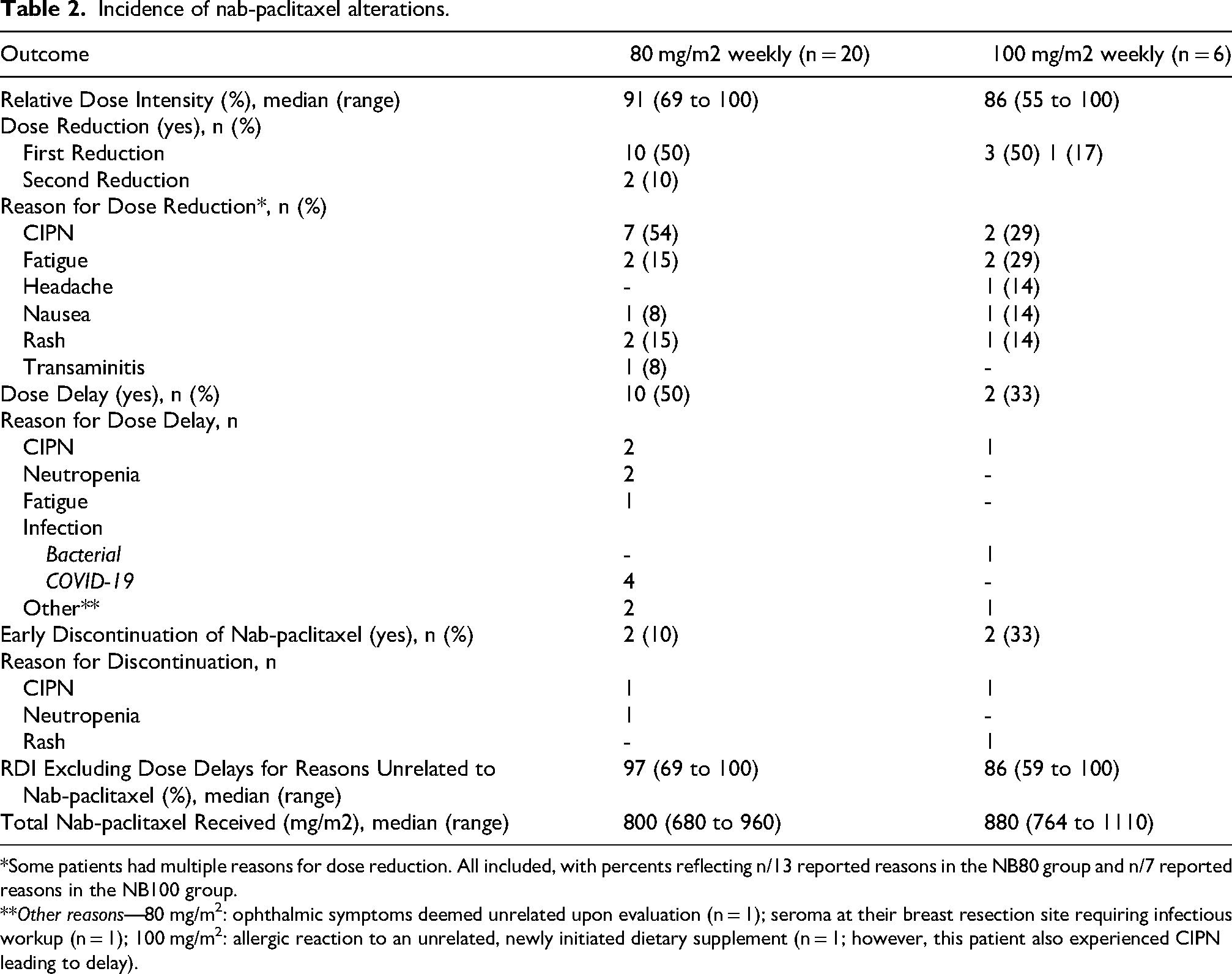
*Some patients had multiple reasons for dose reduction. All included, with percents reflecting n/13 reported reasons in the NB80 group and n/7 reported reasons in the NB100 group.
**Other reasons—80 mg/m2: ophthalmic symptoms deemed unrelated upon evaluation (n = 1); seroma at their breast resection site requiring infectious workup (n = 1); 100 mg/m2: allergic reaction to an unrelated, newly initiated dietary supplement (n = 1; however, this patient also experienced CIPN leading to delay).
Characterizations of adverse effects in both nab-paclitaxel dosing groups are presented in Table 3. Incidence of any CIPN were 80% vs 83% with NB80 and NB100, respectively. The incidence of grade 2 CIPN was higher with NB100 (50% vs 35%). A lower incidence of all grade neutropenia resulted from NB80 (60 vs 67% with 100 mg/m2); however, two patients experienced grade 3 neutropenia with NB80 versus zero patients with NB100. These outcomes occurred in the setting of more GCSF administration for secondary prophylaxis in the NB100 arm (67% vs 40% with NB80). Similar proportions of patients experienced continued nab-paclitaxel-related adverse effects 6 or more months after completion of nab-paclitaxel administration (15% on NB80 versus 17% on NB100). No patients were hospitalized during nab-paclitaxel treatment or died during the study period.
Adverse effects by weekly nab-paclitaxel dose.
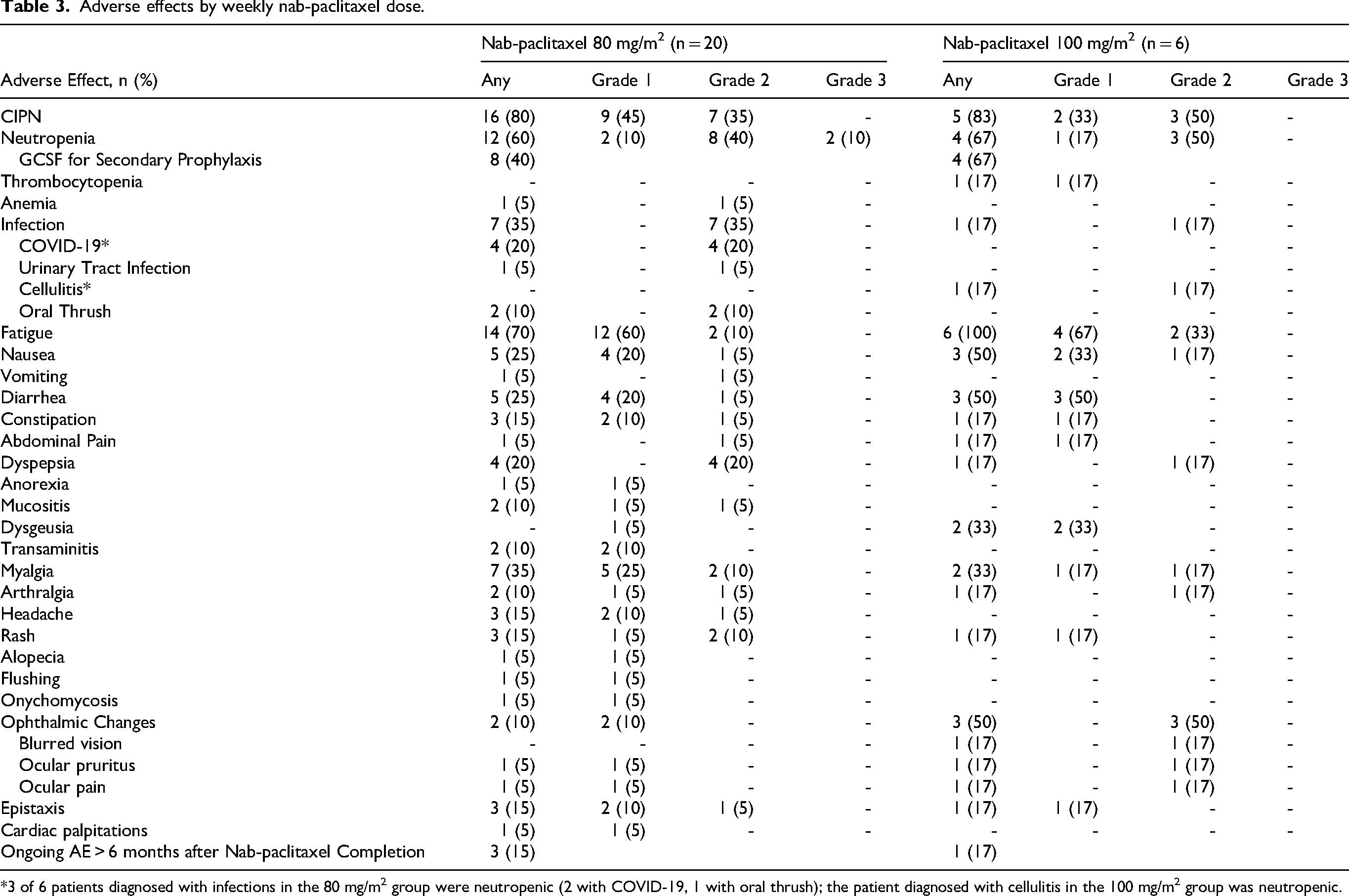
*3 of 6 patients diagnosed with infections in the 80 mg/m2 group were neutropenic (2 with COVID-19, 1 with oral thrush); the patient diagnosed with cellulitis in the 100 mg/m2 group was neutropenic.
Discussion
This retrospective review suggests that nab-paclitaxel dosed at 80 mg/m2 IV weekly may promote increased relative dose intensity compared to 100 mg/m2 IV weekly in patients with early breast cancer switching from paclitaxel due to a hypersensitivity reaction.
The EFFECT trial is one of the few prior studies to directly compare nab-paclitaxel dosing in patients with breast cancer. 8 Nab-paclitaxel 100 mg/m2 versus 125 mg/m2 weekly, 3 weeks on followed by 1 week off, was assessed in patients 65 years or older with advance disease. The results showed no difference in survival outcomes but increased adverse effects in the 125 mg/m2 group, primarily chemotherapy-induced peripheral neuropathy (CIPN), that led to dose reductions with the 125 mg/m2 dosing regimen. 8
The findings of the EFFECT trial relate to the concept of RDI. A meta-analysis by Nielsen et al. evaluated the impact of RDI on survival in adult patients with solid tumor cancers on non-adjuvant chemotherapy regimens. 6 The results indicated significantly shorter overall survival (OS) at RDI <80% versus ≥80% and <85% versus ≥85% in four taxane-based studies for breast, non-small cell lung, or ovarian cancers (HR 1.17; 95% CI: 1.07–1.27). Evaluation of RDI in the neoadjuvant management of breast cancer has also been specifically conducted. 9 The JONIE1 trial assessed RDI in patients receiving FEC followed by 12 cycles of weekly solvent-based paclitaxel at 80 mg/m2. Results showed a 5-year overall survival rate of 91.2% and 76.3%, when RDI ≥85% and <85%, respectively (p = 0.015). An exploratory subgroup analysis associated low RDI with low overall survival in patients with obesity, T1/2 disease, and lymph node metastases. 9
Current NCCN Guideline© recommendations on nab-paclitaxel dosing are limited to the guidance that the weekly dose of nab-paclitaxel should not exceed 125 mg/m2 IV. 1 Given the EFFECT trial suggests nab-paclitaxel 125 mg/m2 IV weekly may be intolerable amongst breast cancer patients, further investigation was necessary. 8 Studies separately incorporating NB80 or NB100 weekly have been conducted amongst breast cancer patients undergoing neoadjuvant treatment; outcomes of these prior trials are summarized in Table 4. Greater incidence of dose-reductions/discontinuations and associated adverse events with NB100 in these trials align with the findings of this study. To our knowledge, this is the first published study to compare different dosing strategies for switching to weekly nab-paclitaxel in the neoadjuvant or adjuvant treatment of breast cancer patients who experienced a hypersensitivity reaction to paclitaxel. A numerically larger proportion of patients NB80 achieved RDI > 80% and >85% compared to NB100 (Figure 2). These findings may be used to guide best practices in dosing weekly nab-paclitaxel after switching from paclitaxel due to a hypersensitivity reaction, as it could promote improved efficacy and safety.6,9
Nab-paclitaxel dosing and outcomes across breast cancer populations.
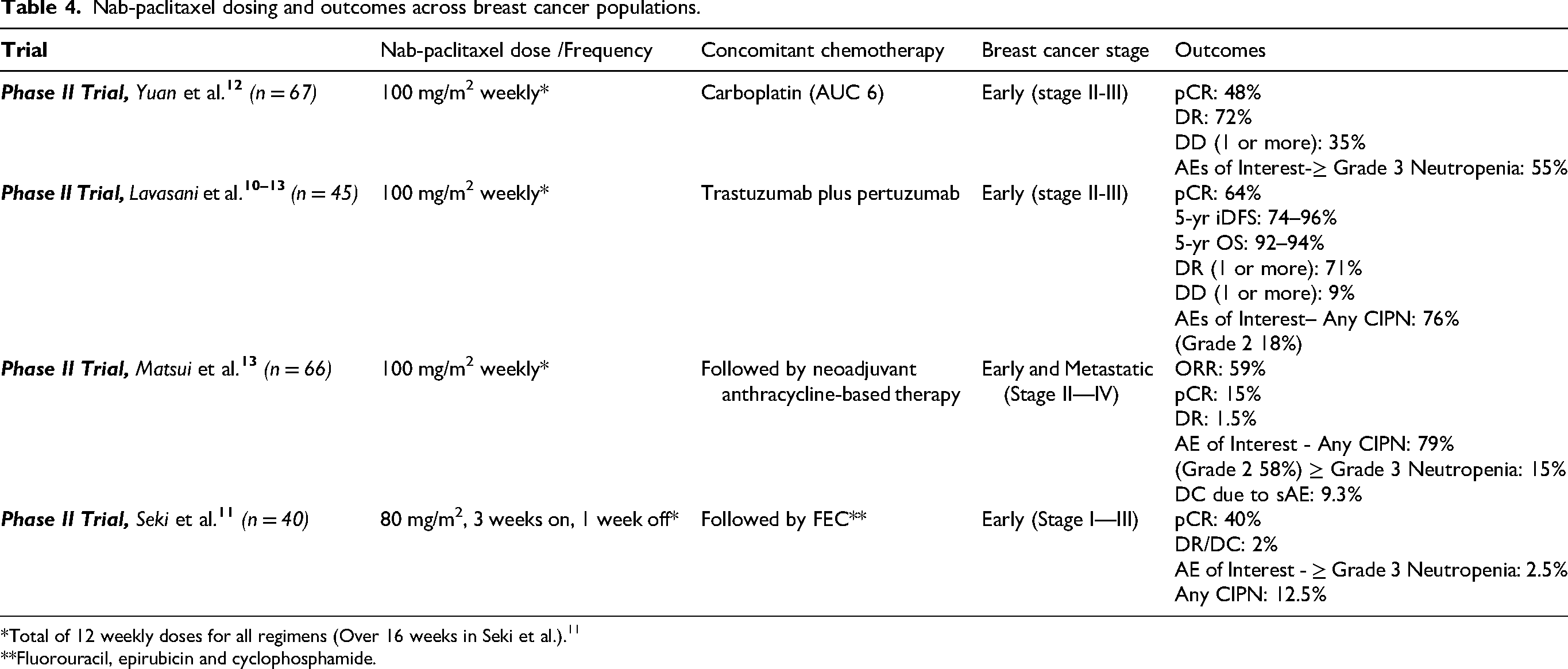
*Total of 12 weekly doses for all regimens (Over 16 weeks in Seki et al.). 11
**Fluorouracil, epirubicin and cyclophosphamide.
There are several limitations to this study. Due to the retrospective design, there is potential for confounding of heterogeneous patient characteristics and information bias due to limitations of data collection through chart review. However, this study design did represent outcomes of patients in real-world practice. The small sample size and unbalanced representation of each dosing schema precluded the ability to conduct statistical analysis of differences in outcomes. Limiting the study period to include patients whose treatment course was completely conducted in our institution's current EHR likely limited the sample population. Furthermore, RDI was used as a surrogate marker for the impact of nab-paclitaxel dose on survival outcomes. This was chosen due to the lack of feasibility in determining relapse-free survival rates amongst other survival outcomes, given breast cancer progression and recurrence often occurs in the span of years. However, as previously stated, it has been validated in its association with survival differences. Grading of adverse events was completed through retrospective review of charts that may have held inaccurate or incomplete reports and assessment by CTCAE v.5 criteria. 7 The subjective nature of this grading tool imposes the possibility of detection bias but remains widely accepted and utilized.
Outcomes from this study warrant further investigation across institutions with expanded timelines and sample sizes, as this would provide power to directly assess survival outcomes and statistical significance of differences. Additionally, a cost-effectiveness analysis might provide better characterization of our finding of reduced GCSF administration for secondary prophylaxis during nab-paclitaxel treatment dosed at 80 mg/m2 weekly. The high rate of patients who were excluded due to switching to nab-paclitaxel later in their treatment course for paclitaxel-induced rash was a unique trend in this study (Figure 1). Future research is indicated to assess the appropriateness of this practice, as it is not proven to be effective in resolving rash. Additionally, early exposure to nab-paclitaxel may limit future treatment options for patients who progress, as data has shown improved efficacy with nab-paclitaxel compared to paclitaxel in metastatic breast cancer treatment. 14
Conclusion
Our data suggest dosing nab-paclitaxel at 80 mg/m2 IV weekly may promote improved RDI and safety compared to 100 mg/m2 IV weekly in patients with early breast cancer switching from paclitaxel due to a hypersensitivity reaction. More patients on nab-paclitaxel 80 mg/m2 weekly achieved an RDI above thresholds shown to be associated with improved survival in prior studies. Nab-paclitaxel 80 mg/m2 weekly may be preferred for patients regardless of age, disease stage, or concomitant chemotherapy agents, with the potential to reduce taxane-related adverse effects and supportive care costs through lower rates of GCSF administration for secondary prophylaxis. Further studies are warranted to confirm these findings.
Footnotes
Ethical considerations
This was study was approved by the University of Washington Institutional Review Board.
Consent to participate
This was waived by the Institutional review board.
Authors' contribution
AI, AD, and JY contributed to project conception and KG research the literature for the study. All authors were involved in protocol development and gaining ethical approval. KG conducted data extraction and analysis, and KG was the primary author on the manuscript. All authors reviewed and edited the manuscript and approved the final manuscript version.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Data availability
The authors confirm that the data supporting the findings of this study are available within the article and the data that support the findings of this study are available from the corresponding author, AI, upon reasonable request.