
Abstract
Objective
Hematopoietic stem cell transplant (HSCT) is the only curative option for genetic, immunological, and hematological disorders such as leukemia, lymphoma, and bone marrow failure syndromes. Graft-versus-host disease (GVHD) remains the most frequent post-transplant complication and is commonly managed with cyclosporine. However, recipients of HSCT are at high risk of life-threatening infections despite prophylaxis, and azole antifungals can alter cyclosporine concentrations, predisposing patients to toxicities. This study is the first from Pakistan to evaluate the effect of azole antifungals on cyclosporine levels and associated toxicities.
Material and methods
A retrospective analysis was performed on 150 HLA-matched HSCT recipients at the National Institute of Blood Disease and Bone Marrow Transplantation (NIBD and BMT) who received cyclosporine with either fluconazole or voriconazole between October 2018 and December 2022. Cyclosporine levels and toxicities were assessed on day +14. Primary outcomes included cyclosporine-related adverse effects (hypertension, nephrotoxicity, hepatotoxicity, neurotoxicity, electrolyte imbalance), while the secondary objective was to correlate toxicities with cyclosporine drug concentrations in the presence of triazole antifungals.
Results
The study included 97 males (64.4%) and 53 females (35.3%), with a median age of 11 years (range: 6–20). Beta-thalassemia major was the most common indication (n = 71, 47%). According to NCI-CTCAE criteria, the most frequent Grade 2 toxicity was hypokalemia (20%), and hepatotoxicity (16%) was the most common Grade 3 event. No Grade 4 toxicities were observed. Supratherapeutic cyclosporine levels occurred with both fluconazole and voriconazole.
Conclusion
While dose adjustment is standard with voriconazole, our findings suggest the need for similar consideration with fluconazole. Larger studies are required to confirm this observation.
Keywords
Introduction
Hematopoietic stem cell transplant (HSCT) serves as the only curative treatment for various genetic, immunological, and life-threatening hematological disorders such as leukemia, lymphoma, and bone marrow failure syndromes. Following transplantation, graft-versus-host disease (GVHD) is the most common complication documented, impacting mortality and morbidity by up to 10%. 1 Graft-versus-host disease (GVHD) prophylaxis is commonly achieved using cyclosporine, a calcineurin inhibitor. Its efficacy in reducing GVHD incidence has been well established and is primarily attributed to its ability to inhibit T-cell activation and proliferation. Standard prophylaxis in HLA-matched HSCT often involves combining it with either methotrexate (MTX) or mycophenolate mofetil (MMF). The majority of member centers preferred the cyclosporine and methotrexate regimen for GVHD prevention and treatment following HSCT, while a small proportion of centers used tacrolimus and methotrexate, according to the EBMT 2012 survey.2,3
Transplant recipients are at increased risk of acquiring potentially fatal infections, which can have a major influence on the outcome of transplant. By using antifungal and broad-spectrum antibiotics, this risk has been substantially diminished. The most concerning have been invasive fungal infections, which in the first 30 days after transplantation before neutrophil engraftment, can cause mortality rates ranging from 42% to 54%. Nevertheless, fungal infections have been significantly reduced after the addition of antifungal prophylaxis. 4
In the SEIFEM trial, 72% of allogeneic HSCT patients and 35% of autologous HSCT patients died from invasive fungal infections. Aspergillosis was more prevalent and fatal in allogeneic HSCT than autologous. Mortality and incidence were similar for invasive candida infection.5,6,7 Previous studies have reported that over 60% of hematopoietic stem cell recipients acquired invasive fungal infection during the neutropenic phase. 8 Triazole antifungals (fluconazole and voriconazole) are commonly used for prophylaxis. Azole antifungals, when used concurrently with cyclosporine, disrupt the metabolism of the drug as they are inhibitors of CYP 450, resulting in supratherapeutic cyclosporine levels and potentiating toxicity that may affect laboratory values and clinical parameters. Studies show that voriconazole requires dosage modifications with concurrent use of cyclosporine, although fluconazole does not. L. J. Worth et al. found that low-dose fluconazole enhances the cyclosporine area under the curve by 50%, indicating no need for dose adjustment. However, voriconazole raises the area under the curve for cyclosporine by 70%, requiring a 50% dose reduction.9,10,11,12 Unfortunately, neither of the drugs can be avoided due to their significance in the post-transplant regimen, requiring the practitioners to administer the drugs under strict observation.
After extensive research, we found that no such study on the effect of triazole agents on the cyclosporine pharmacokinetic profile and its influence on the adverse effect profile has been carried out in Pakistan. The study we conducted not only assessed the impact of triazole antifungal on cyclosporine toxicity but also compared the individual effects of both antifungals on cyclosporine levels and adverse effect profiles.
Material and methods
A retrospective analysis was conducted on 150 patients who underwent HLA-matched family donor hematopoietic stem cell transplantation at the National Institute of Blood Disease and Bone Marrow Transplantation (NIBD and BMT) from October 2018 to December 2022. After obtaining approval from the institutional review board with IRB number 188/36-2018, informed consent was obtained from the patients.Patients who received cyclosporine for GvHD prophylaxis and either voriconazole or fluconazole for fungal prophylaxis were included in the study.
All patients with active fungal or bacterial infections, those switching between antifungals, and those with pre-existing deranged liver or kidney function were excluded from the study. Patients with total bilirubin >3 ULN, transaminases >5 ULN, or serum creatinine >2 ULN were excluded. Clinical parameters such as blood pressure, tremors, and seizures, along with laboratory parameters including complete blood count, urea, creatinine, liver function tests, electrolytes, and cyclosporine trough levels, were assessed on day +14 post-transplant. We documented the adverse effects using NCI-CTCAE grading.
Drug dosing and protocol for administration
As per institutional policy, antifungal prophylaxis was initiated on day −4, i.e., four days before the stem cell infusion, and cyclosporine was started at day −2. The choice of antifungal was decided on the basis of the risk of fungal infection. High-risk patients were given voriconazole at 6 mg/kg/dose twice a day in adults and 8 mg/kg/dose twice a day in the pediatric population; however, low-risk patients were given fluconazole at 6 and 12 mg/kg/dose once daily for adult and pediatric groups, respectively. Cyclosporine was administered at 3 mg/kg via continuous infusion diluted in normal saline over 10 h. The dose adjustment as per institutional policy was a 50% dose reduction of cyclosporine with voriconazole and no dose adjustment with fluconazole. Therapeutic levels were categorized into normal, subtherapeutic, and supratherapeutic levels of cyclosporine.
Procedures
The institution utilized an Abbott Architect i1000SR modular chemiluminescent immunoassay analyzer for therapeutic drug monitoring for cyclosporine trough level, and a target range of 200–400 ng/mL was applied and followed.
Data presentation and analysis
Statistical analysis was conducted using SPSS version 25. Categorical variables were summarized in terms of frequencies and percentages. The occurrence of cyclosporine related toxicities including hypertension, nephrotoxicity, neurotoxicity, hepatotoxicity, and electrolyte imbalances were analyzed in relation to therapeutic drug levels and the use of antifungal prophylaxis by applying the Pearson chi-square test.
Results
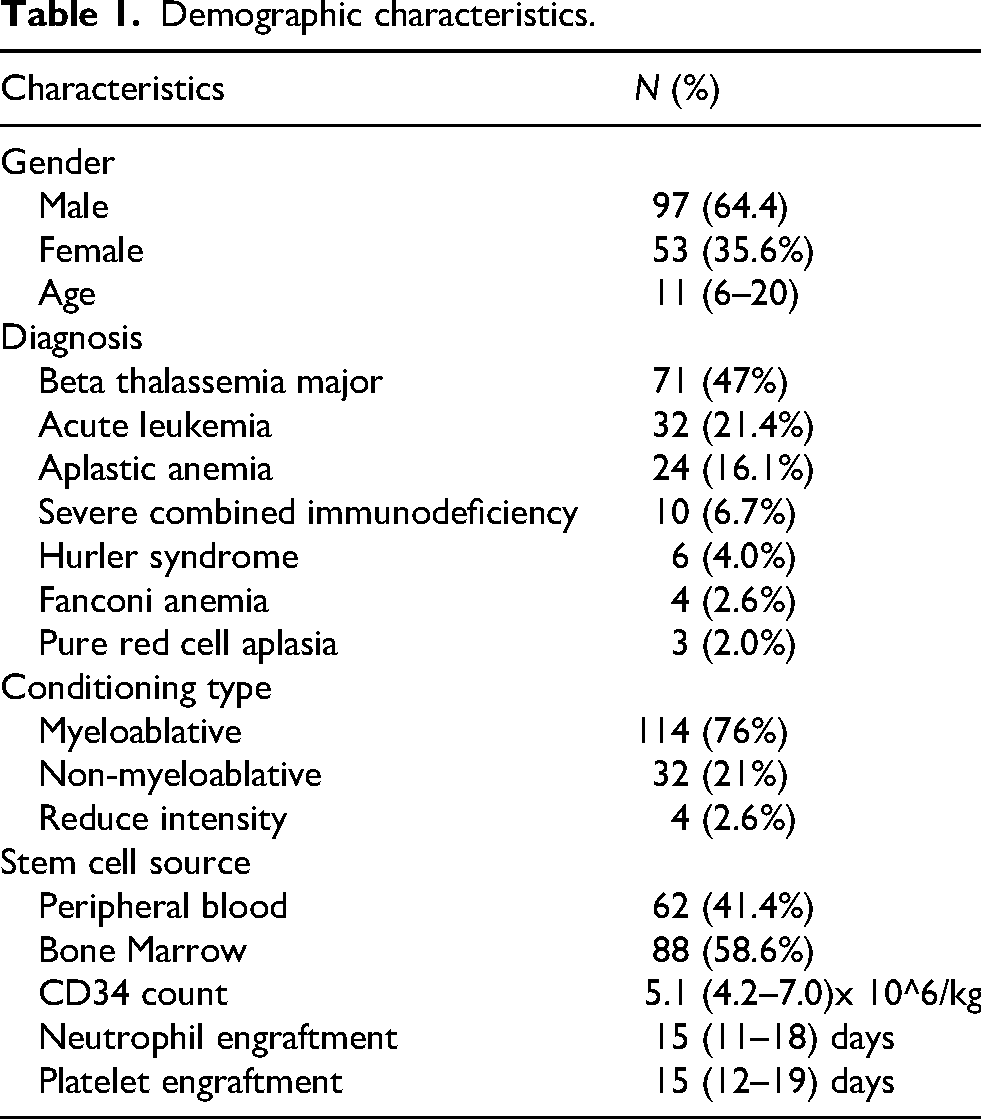
The baseline demographics of 150 patients analyzed are detailed in Table 1. The study included both sexes (n = 97 males, 64.4%, and n = 53 females, 35.6%) with a median age of 11 years (range 6–20 years). Majority of the patients had beta-thalassemia major (n = 71, 47%) followed by acute Leukemia (n = 32, 21.4%), aplastic anemia (n = 24, 16.1%), severe combined immunodeficiency (n = 10, 6.7%), hurler syndrome (n = 6, 4%), Fanconi anemia (n = 4, 2.6%) and pure red cell aplasia (n = 3, 2%). The conditioning regimens offered included: myeloablative (MA) (n = 114, 76%), non-myeloablative (NMA) (n = 32, 21.3%) and reduced intensity (RIC) (n = 4, 2.6%). The source of stem cells was bone marrow in 58.6% and peripheral blood in 41.4% of recipients. The median CD34 count was 5.1 × 10^6/kg (range 4.2 to 7.0). The mean number of days documented for neutrophil and platelet engraftment was 15 for both, with a range of 11–18 days for neutrophil engraftment and 12–19 days for platelet engraftment.
Demographic characteristics.
Only grades 2 and 3 adverse effects were recorded according to the NCI-CTCAE adverse event grading system. No patients demonstrated grade 4 toxicity. Hypokalemia was the most frequently reported toxicity, affecting 20% patients, followed by hypertension reported in 16.6% patients. Grade 2 nephrotoxicity, hepatotoxicity and imbalance of other electrolytes were also noted as depicted in Figure. 1. However, hypertension and hepatotoxicity, were the only side effects graded as grade 3 toxicity, affecting 9.3% and 16% subjects, respectively.
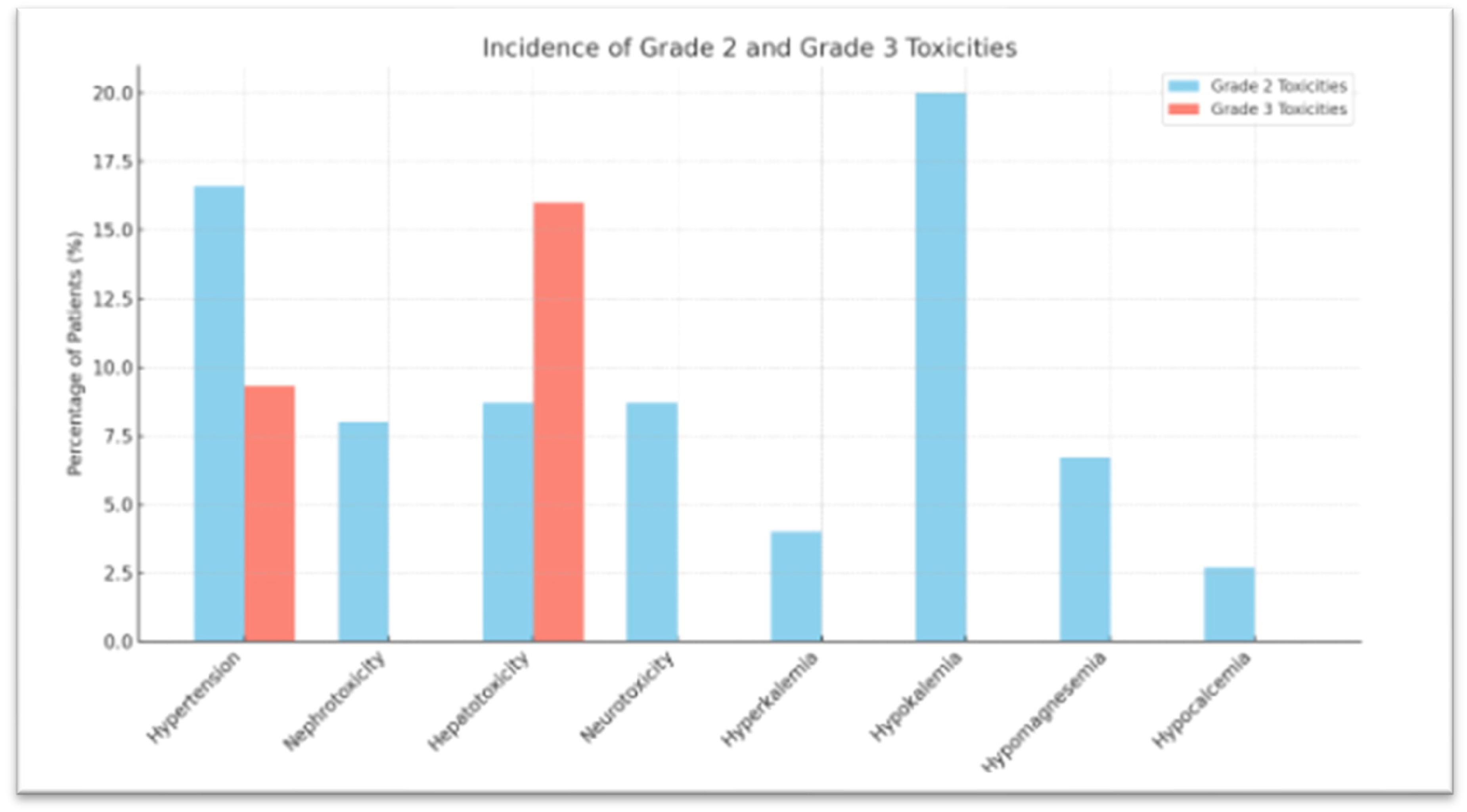
Cyclosporine toxicity at day + 14 according to NCI-CTCAE grading.
The association between cyclosporine levels and specific toxicities namely hypertension, nephrotoxicity, hepatotoxicity, neurotoxicity, and electrolyte imbalance, across two antifungal groups (fluconazole and voriconazole) is summarized in Table 2. In patients receiving fluconazole, supratherapeutic cyclosporine levels were associated with a notably higher incidence of all reported toxicities compared to the normal and subtherapeutic groups. Among these, electrolyte imbalance (p = 0.01), hepatotoxicity (p = 0.01), hypertension (p = 0.01) and neurotoxicity (p = 0.01) showed statistically significant differences between cyclosporine level categories.
Cyclosporine toxicity in relation to fungal prophylaxis and therapeutic levels.
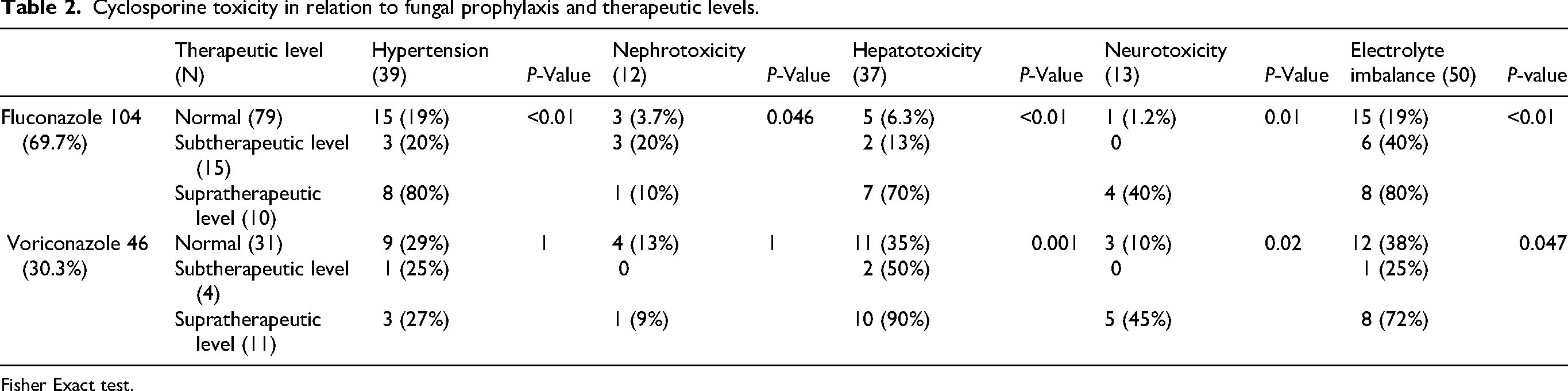
Fisher Exact test.
In contrast, among patients receiving voriconazole, hepatotoxicity, neurotoxicity, and electrolyte imbalance demonstrated statistically significant differences across subtherapeutic, normal, and supratherapeutic groups. Other toxicities, such as hypertension and nephrotoxicity, did not show a significant association with cyclosporine levels in this group.
Discussion
This retrospective study examines antifungal-induced cyclosporine toxicity and therapeutic drug levels. Cyclosporine is a CYP3A4 and P-gp substrate. As a result, their inhibition or activation may have an impact on its metabolism and drug levels.The European Society for Blood and Marrow Transplantation (EBMT) and European LeukemiaNet (ELN) now propose 200–300 ng/mL trough concentration of cyclosporine for GvHD prophylaxis. Regarding side effects, a concentration of up to 500 ng/mL is generally considered safe, although clear evidence to fully support this assumption is lacking. 13 Cyclosporine exposure is significantly increased when co-administered with CYP3A4 inhibitors due to reduced clearance. Current recommendations suggest reducing cyclosporine doses by 25–50% with moderate CYP3A4 inhibitors and by 50–75% with strong inhibitors. 14 Specifically, in the case of azole antifungals, a 20–50% reduction is advised with fluconazole (400 mg) and approximately 50% with voriconazole to minimize the risk of toxicity while maintaining therapeutic levels. 15
Patients undergoing allo-HSCT frequently develop hypertension. 16 One contributing factor is cyclosporine, which is known to induce systemic and renal vasoconstriction, leading to elevated blood pressure early in the post-transplant period. In our analysis, an association was observed between supratherapeutic cyclosporine levels and the development of hypertension in patients receiving antifungal prophylaxis. The majority of affected patients experienced grade 2 or 3 hypertension, as defined by the National Cancer Institute's Common Terminology Criteria for Adverse Events (NCI-CTCAE). Additionally, corticosteroid use, commonly administered as prophylaxis against serum sickness following anti-thymocyte globulin (rabbit) in conditioning regimens, may also contribute to the onset of hypertension in these patient population.
Renal impairment is a common and serious complication observed early after hematopoietic stem cell transplantation (HSCT). Cyclosporine, particularly when administered concomitantly with other nephrotoxic agents such as amphotericin B or aminoglycosides, can exacerbate renal dysfunction. 17 Elizabeth A. de Kort et al. reported that patients receiving high-dose cyclosporine frequently developed renal toxicity, with grade 2 nephrotoxicity, defined as serum creatinine levels 2 to 3 times above baseline, occurring in 49% (63 out of 129) of patients, and grade 3 toxicity in 7.5% (10 out of 129) of cases. 13 In our study, although renal toxicity was reported in both groups there was no significant association between renal toxicity and cyclosporine levels during the first four weeks post-transplant.
Although several studies have demonstrated that azole antifungal such as voriconazole significantly increase cyclosporine levels, 18 and others have reported cyclosporine-induced liver injury (CILI), 19 direct evidence linking azole-induced elevation of cyclosporine levels to hepatotoxicity remains limited. In our study, however, grade 2 and 3 hepatotoxicity were observed predominantly, as defined by standardized toxicity criteria. Notably, a high incidence of hepatotoxicity occurred in patients with supratherapeutic cyclosporine levels, 90% in those receiving voriconazole and 70% in those on fluconazole, highlighting a strong association between elevated drug levels and hepatic toxicity.
A retrospective review of 104 allo-HSCT patients demonstrated that co-administration of cyclosporine with triazole antifungals led to life-threatening complications in 12 patients, despite therapeutic drug monitoring. Among these, 33% developed neurological toxicities, and cyclosporine levels remained supratherapeutic even after dose reduction, highlighting that trough levels may not reliably predict drug exposure or toxicity.20,21 Similarly, our data also revealed a higher incidence of neurotoxicity in patients with supratherapeutic cyclosporine levels co-administered with antifungal agents, whereas no neurotoxicity was observed in those with subtherapeutic levels. Specifically, among the patients with supratherapeutic levels of cyclosporine, neurotoxicity was identified in 40% of patients receiving fluconazole and 45% receiving voriconazole, with both groups showing statistically significant associations (p < 0.05). Posterior reversible encephalopathy syndrome (PRES) was confirmed in 6% of patients through MRI. While no cases of grade 3 or 4 neurotoxicity were detected, symptomatic management, including seizure control and tremor treatment, was required, and in some instances, dose modification or discontinuation of the implicated agents was necessary.
According to the EBMT Handbook on Hematopoietic Cell Transplantation, calcineurin inhibitors such as cyclosporine are associated with renal tubular dysfunction, which can lead to clinically significant electrolyte imbalances, including hyperkalemia, metabolic acidosis, hypomagnesemia, hypophosphatemia, and hypercalciuria, necessitating close monitoring and early intervention to prevent toxicity. 22 Additionally, voriconazole labeling from both the FDA and manufacturers’ product monographs explicitly warns of hypokalemia, hypomagnesemia, and hypocalcemia, recommending correction before and during therapy due to the risk of worsening these imbalances when combined with nephrotoxic agents like cyclosporine. 23 In line with these findings, our study identified statistically significant electrolyte disturbances in both the fluconazole and voriconazole groups (p < 0.05). On Day +14 post-transplant, we observed grade 2 electrolyte abnormalities, including hypomagnesemia in 6.7%, hyperkalemia in 4%, hypokalemia in 20%, and hypocalcemia in 2.7% of patients. However, it is noteworthy that none of these patients exhibited clinical or laboratory evidence of renal tubular dysfunction, suggesting that the electrolyte disturbances may have occurred independently of overt tubular injury, possibly due to pharmacodynamic interactions or subclinical effects of drug combination.
A key strength of this study is its focus on a clinically relevant and underexplored area, the potential link between supratherapeutic cyclosporine levels and antifungal co-administration, particularly with triazoles. The findings provide valuable real-world insights into the incidence of hepatotoxicity in HSCT patients receiving cyclosporine with azole antifungals. However, the study has several limitations. First, as a retrospective observational analysis, it is inherently subject to selection bias and lacks the ability to establish a definitive causal relationship. Second, while the data suggest a strong association between azole use and elevated cyclosporine levels, we were unable to simultaneously monitor both cyclosporine and azole plasma concentrations over time, which is essential for confirming pharmacokinetic interactions. Lastly, the sample size is limited, and larger, prospective studies with serial drug level monitoring are necessary to validate these findings and clarify whether supratherapeutic cyclosporine levels are directly attributable to CYP450 inhibition by azoles such as voriconazole or fluconazole.
Conclusion
In conclusion, our findings suggest that supratherapeutic cyclosporine levels are particularly observed in the context of concomitant antifungal therapy, both with fluconazole and voriconazole. While our current practice already accounts for cyclosporine dose reduction with voriconazole, similar consideration may also be warranted with fluconazole. However, the interpretation of these results is limited by the small sample size, potential selection bias, and the observational nature of the study. Therefore, larger and more controlled studies are needed to validate these findings and to better delineate the contributing factors to these complications.
Footnotes
Ethics approval and consent to participate
This study involves human participants and was approved by institutional review board/ Ethic committee NIBD & BMT with protocol approval #: IRB number 188/36-2018
Authors contributions
RPh. Aisha Rafiq, Dr Uzma Zaidi, Dr Waseem Shahani (Concept development)
Dr Aisha Jamal, Dr Uzma Hayat, Dr Shafaq Abdul Samad (Critical evaluation and review manuscript)
Dr Rabeea Munawar Ali, RPh. Aisha Rafiq (Manuscript writing)
Muhammad Nizamuddin (Statistics/Data Analyst)
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Declaration of conflict of interest
The authors declared the following potential conflicts of interest with respect to the research, authorship, and/or publication of this article: This manuscript has been extracted from my M.Phil thesis work.
Data sharing statement
The clinical trial data of this article will not be shared.
Patient and public involvement
Patients or the public WERE NOT involved in the design, or conduct, or reporting, or dissemination plans of our research.