
Abstract
Background
Shortening chemotherapy infusion times is associated with improvements in resource use and patient satisfaction, as well as reductions in nursing workload and clinic wait times. Cyclophosphamide package inserts mention that the drug should be injected or infused very slowly, but the exact duration of infusion is not specified. Per literature review, there is heterogeneity in infusion times among regimens for various conditions.
Methods
The aim was to analyze the incidence of documented adverse events (AEs) temporally related to cyclophosphamide when it was administered as either a 60- or 30-minute infusion. We performed a retrospective chart review of records between January 1, 2023, and January 31, 2024, including adult patients (age >= 18 years) who received at least one cyclophosphamide infusion over 60- or 30-minutes within selected chemotherapy regimens for lymphoma (CHOP +/- R; EPOCH +/- R; CHOEP +/- R) or multiple myeloma (MM) (CyBorD or VCD +/- Dara; KCyD +/- Dara) at any inpatient or outpatient site within Mount Sinai Health System (MSHS).
Results
Among 200 consecutive doses evaluated per disease-based group (n = 400 total doses), there were more numerical occurrences of documented AEs in the 60-minute groups compared to 30-minutes groups (n = 4 vs. n = 2), but this finding was not statistically significant (2% vs. 1%; p > 0.05). There were no documented Grade 3 or higher AEs temporally related to cyclophosphamide infusion.
Conclusion
The shortening of cyclophosphamide infusion times for selected chemotherapy regimens was determined to be a safe practice change.
Background
Shortening infusion times improves resource use and patient satisfaction, as well as reduces nursing workload and clinic wait times. 1 Prior studies have explored shortening infusions and found outcomes to be safe and feasible; however, there are no such published experiences evaluating such modifications with cyclophosphamide.2–4
Cyclophosphamide package inserts state that the drug should be injected or infused very slowly, but the exact duration of infusion is not specified. 5 Within Mount Sinai Health System (MSHS), as of July 2023, selected chemotherapy regimens for lymphoma and multiple myeloma (MM) were modified to shorten the cyclophosphamide infusion time to 30 minutes (instead of the default duration of 60 minutes).
Objective
The purpose of this medication use evaluation was to analyze the incidence of documented adverse events (AEs) related to cyclophosphamide when it was administered as either a 60- or 30-minute infusion.
Methods
This was a retrospective chart review that included two disease-based groups of patients: lymphoma and MM. The Institutional Review Board (IRB) approved this study. All adult patients (age ≥18 years) at an inpatient or outpatient MSHS site who received a cyclophosphamide infusion over 60 minutes (6 months pre-implementation: January 1 to June 30, 2023) or over 30 minutes (6 months post-implementation: August 1, 2023 to January 31, 2024) as part of one of the regimens listed in Table 1 were included.
Chemotherapy regimens that were updated to 30-minute infusion times for cyclophosphamide.
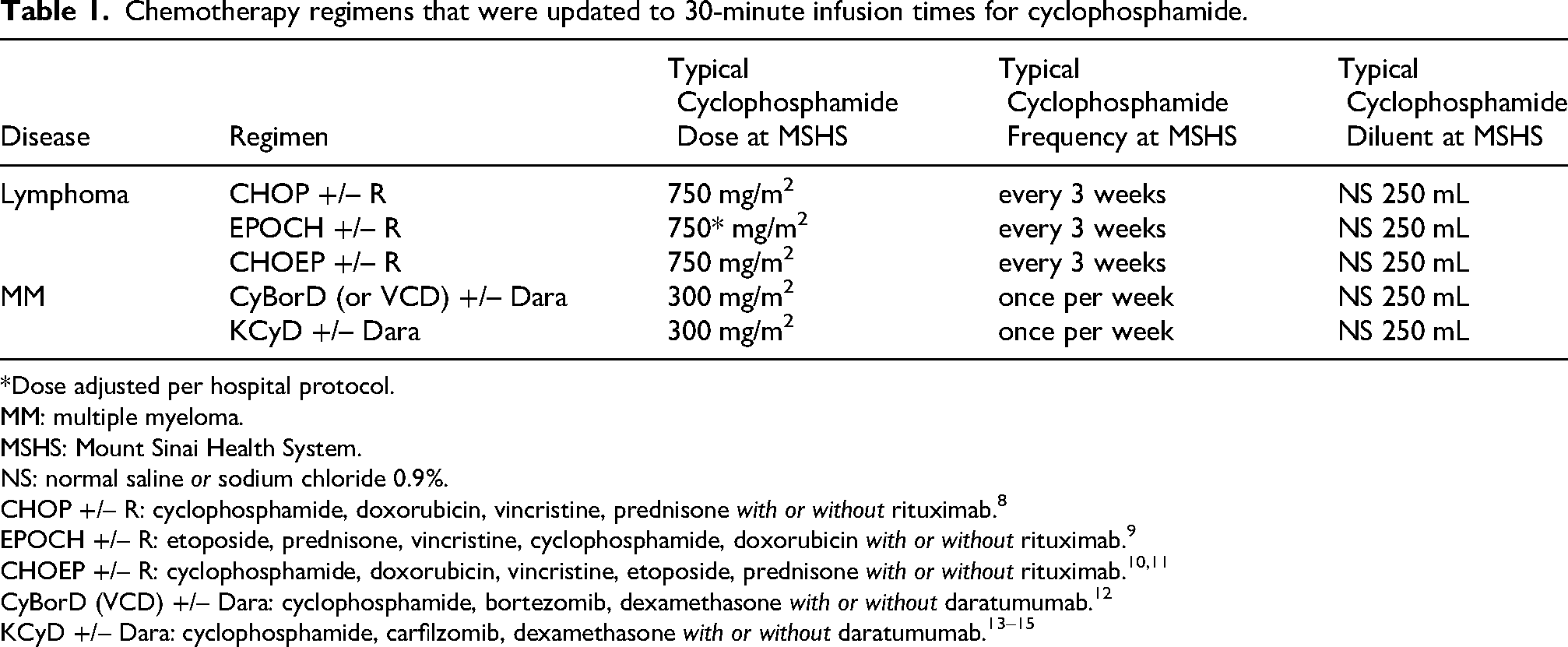
*Dose adjusted per hospital protocol.
MM: multiple myeloma.
MSHS: Mount Sinai Health System.
NS: normal saline or sodium chloride 0.9%.
CHOP +/– R: cyclophosphamide, doxorubicin, vincristine, prednisone with or without rituximab.8
EPOCH +/– R: etoposide, prednisone, vincristine, cyclophosphamide, doxorubicin with or without rituximab.9
CHOEP +/– R: cyclophosphamide, doxorubicin, vincristine, etoposide, prednisone with or without rituximab.10,11
CyBorD (VCD) +/– Dara: cyclophosphamide, bortezomib, dexamethasone with or without daratumumab.12
KCyD +/– Dara: cyclophosphamide, carfilzomib, dexamethasone with or without daratumumab.13–15
As depicted in Figure 1, there was a goal to collect data for 100 doses in each pre- or post-implementation group in each of the disease-based groups, with a total sample size of 400 doses.
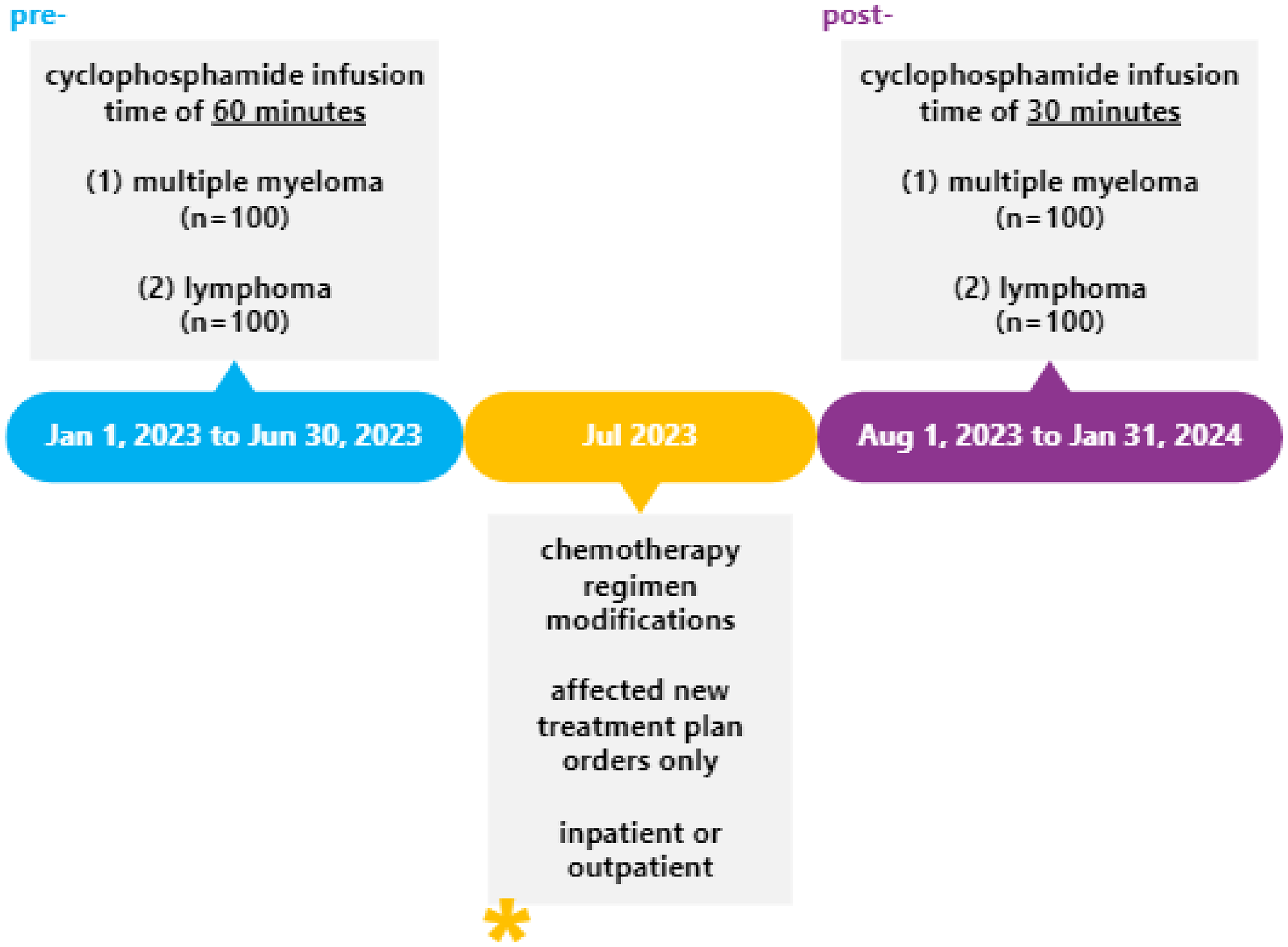
Visual representation of the study design.
The primary outcome was the incidence of any documented AE temporally related to cyclophosphamide within 7 days after drug administration. All AEs were graded per Common Terminology Criteria for Adverse Events (CTCAE v5).6 There was further assessment of the primary outcome via the Adverse Drug Reaction Probability Scale (i.e., Naranjo Algorithm).7
Baseline demographics included age, gender, race, chemotherapy regimen (name, components), cyclophosphamide infusion information (dose, concentration, diluent volume, infusion rate, and pre-dose steroid use), and the location where cyclophosphamide was administered (inpatient versus outpatient).
Other data was collected to evaluate changes in laboratory values (pre-dose to within 7 days after administration), pharmacist intervention (I-vent) documentation, subsequent reversions to 60-minute infusion times, and practice differences among MSHS sites.
Along with descriptive statistics (e.g., measures of central tendency), nominal variables were analyzed via Fisher’s exact test. P-values of < 0.05 indicated statistical significance.
Results
The presented data is from March 20 to December 2, 2023 (excluding July), covering approximately 227 days of inpatient and outpatient care combined.
Per study design, 100 total consecutive doses were collected and evaluated for each of the four groups (400 total doses). There were 34 patients in the lymphoma pre-implementation group, 34 patients in the MM pre-implementation group, 31 patients in the lymphoma post-implementation group, and 18 patients in the MM post-implementation group (117 total patients).
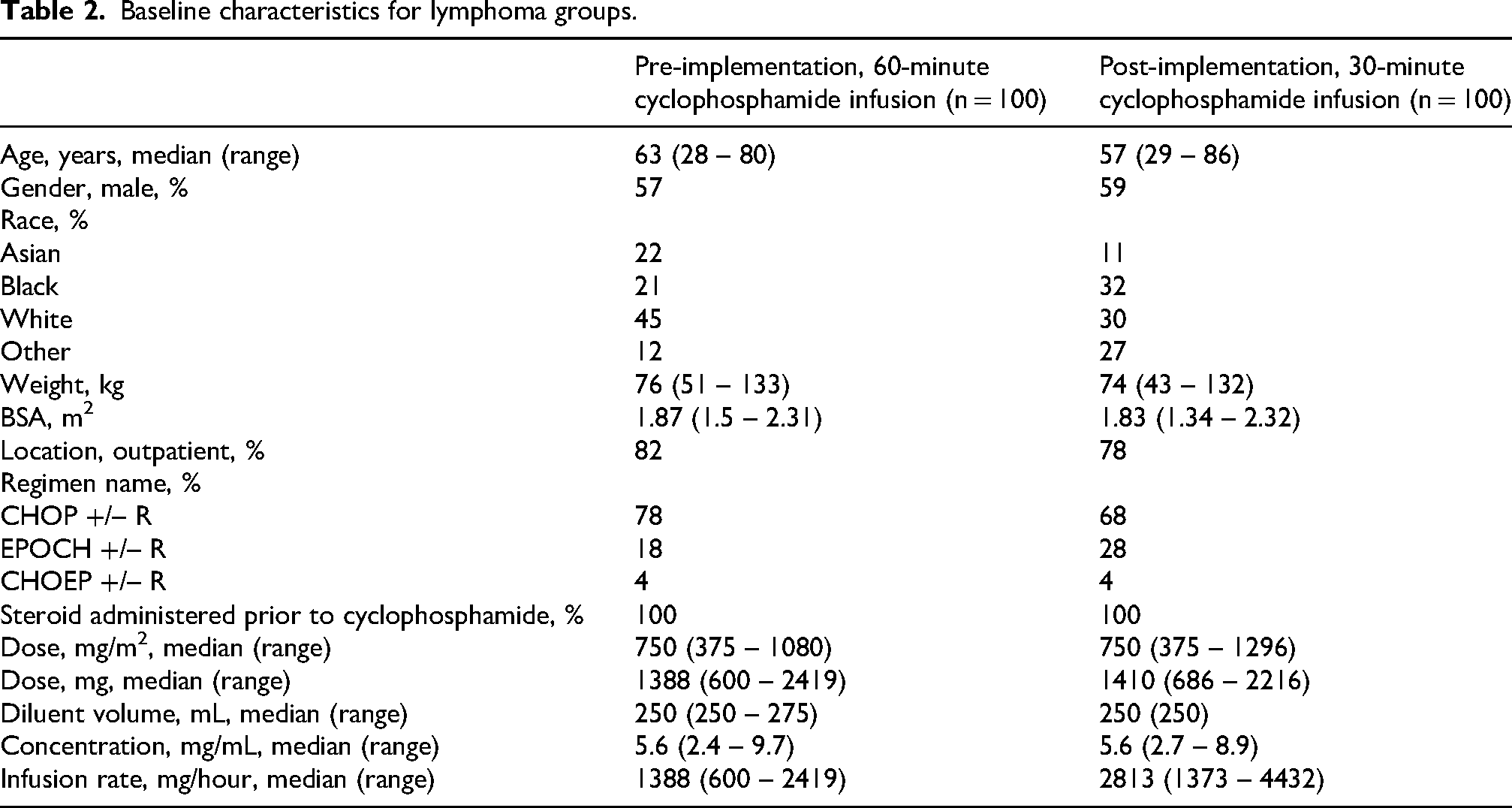
As described in Tables 2 and 3, in the lymphoma groups, the median age of patients was 57 to 63 years, with mostly male gender. Most cyclophosphamide doses were administered in the outpatient setting. The most common regimen was CHOP +/–R. Across all regimens, the median dose of cyclophosphamide was 750 mg/m2, and it was diluted in sodium chloride 0.9% (NS) with a median volume of 250 mL. All patients received a steroid (e.g., dexamethasone, prednisone) as part of the chemotherapy regimen. The maximum tolerated infusion rate in the pre-implementation group was 2,419 mg/hour and in the post-implementation group was 4,432 mg/hour.
Baseline characteristics for lymphoma groups.
Regimen names and pre-medication components for lymphoma groups.
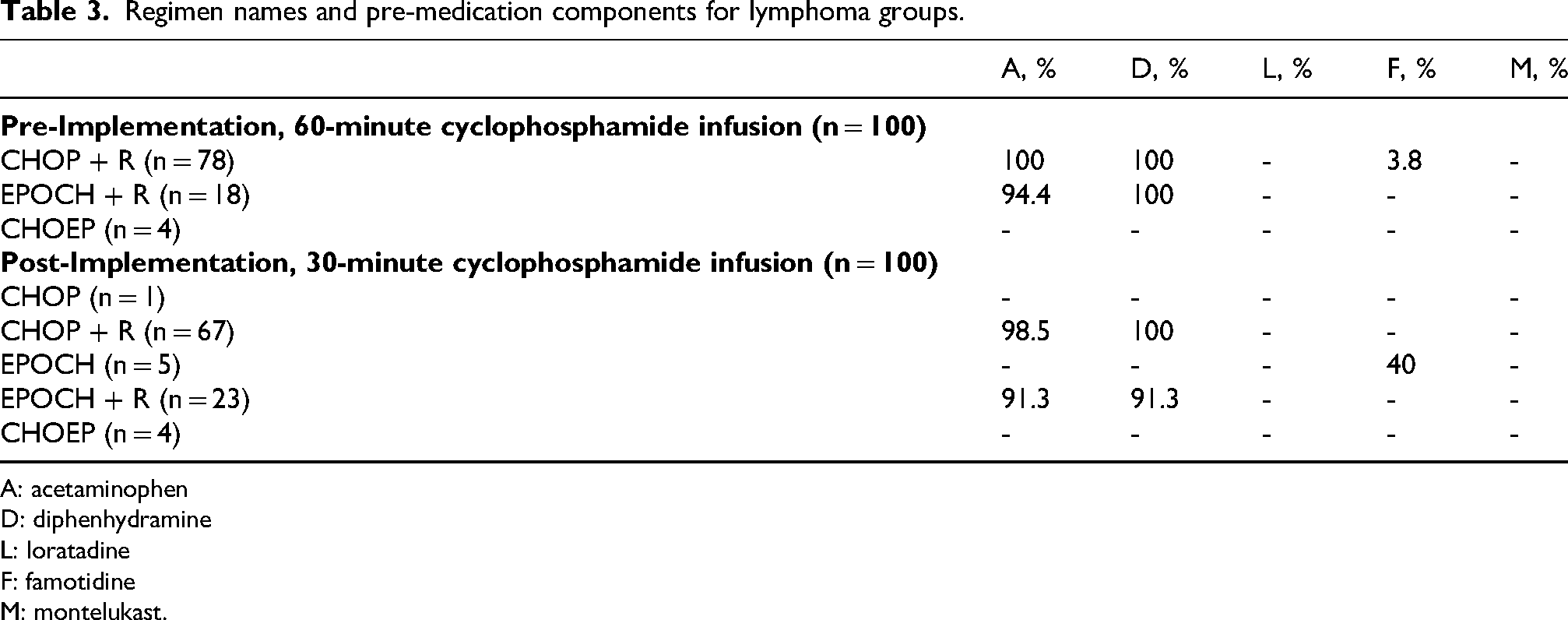
A: acetaminophen
D: diphenhydramine
L: loratadine
F: famotidine
M: montelukast.
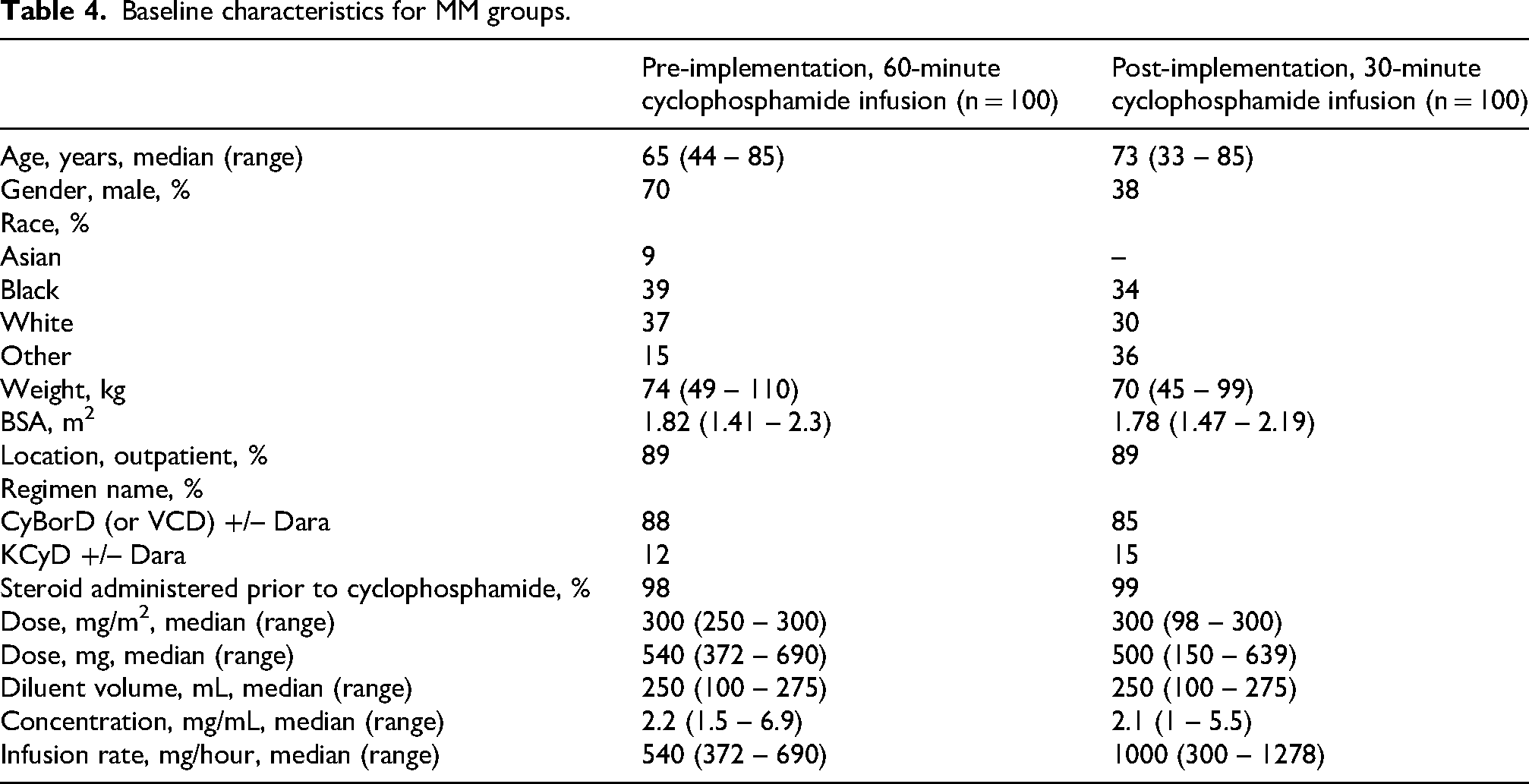
As described in Tables 4 and 5, in the MM groups, the median age of patients was 65 to 73 years, with mostly male gender in the pre-implementation group and mostly female gender in the post-implementation group. Most cyclophosphamide doses were administered in the outpatient setting. The most common regimen was CyBorD (or VCD) +/- Dara. Across all regimens, the median dose of cyclophosphamide was 300 mg/m2 and it was diluted in NS with a median volume of 250 mL. Most patients received a steroid (e.g., dexamethasone, methylprednisolone) as part of the chemotherapy regimen. Of note, 2 doses of cyclophosphamide in the pre-implementation group and 1 dose of cyclophosphamide in the post-implementation group were administered without any steroid in the chemotherapy regimen. The maximum tolerated infusion rate in the pre-implementation group was 690 mg/hour and in the post-implementation group was 1,278 mg/hour.
Baseline characteristics for MM groups.
Regimen names and pre-medication components for MM groups.
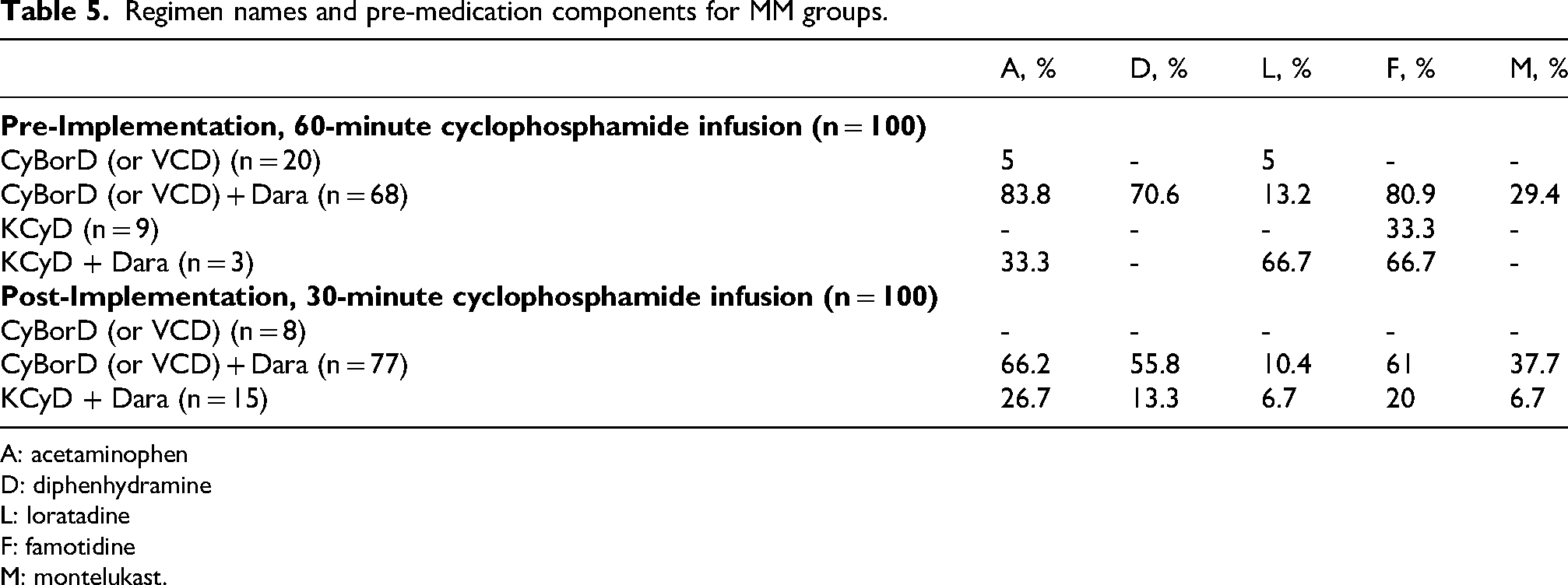
A: acetaminophen
D: diphenhydramine
L: loratadine
F: famotidine
M: montelukast.
As summarized in Table 6, in the pre-implementation period, there were AEs with 3 doses in the lymphoma group and 1 dose in the MM group. In the post-implementation period, there were AEs with 2 doses in the lymphoma group and 0 doses in the MM group. Overall, there were no significant differences (p > 0.05) in infusion-related AE rates among lymphoma or MM patients who received a cyclophosphamide infusion dose administered over 60 or 30 minutes.
Primary outcome of interest: adverse event rate of cyclophosphamide infusion doses.
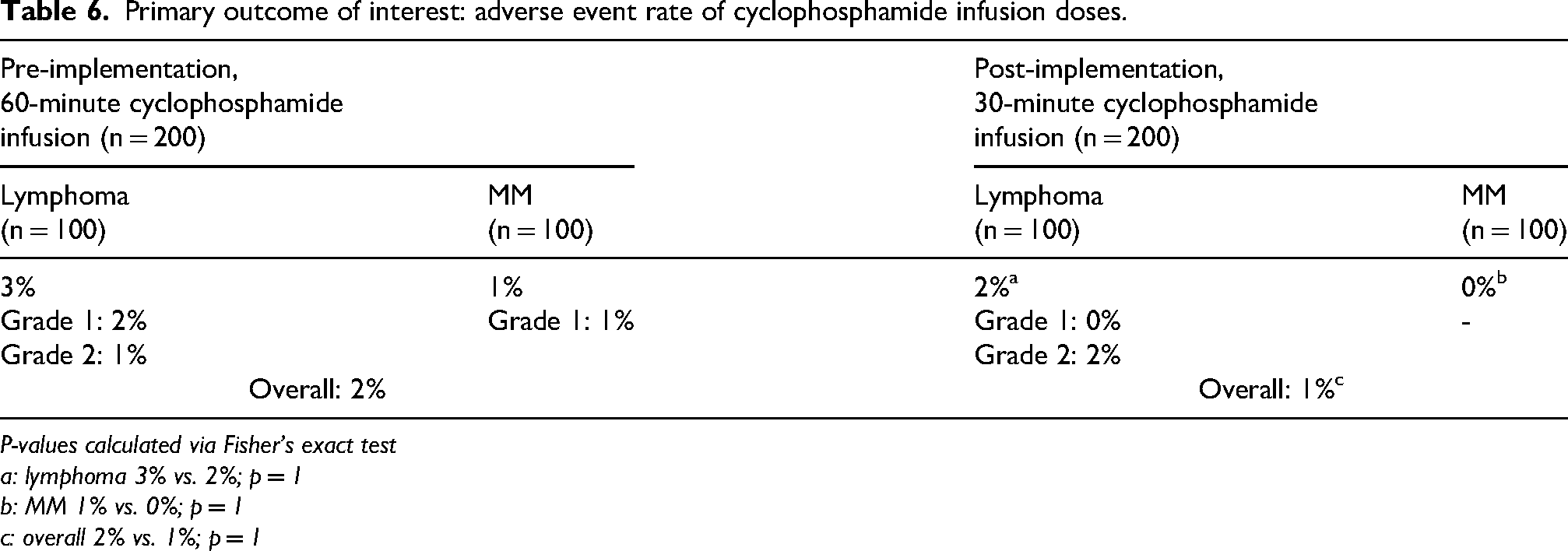
P-values calculated via Fisher’s exact test
a: lymphoma 3% vs. 2%; p = 1
b: MM 1% vs. 0%; p = 1
c: overall 2% vs. 1%; p = 1
The CTCAE v5 definition of a Grade 1 reaction is “Mild transient reaction; infusion interruption not indicated; intervention not indicated” and Grade 2 reaction is “Therapy or infusion interruption indicated but responds promptly to symptomatic treatment (e.g., antihistamines, NSAIDS, narcotics, IV fluids); prophylactic medications indicated for <=24 hours.”6 Details of the AEs are described below.
#1: 34-year-old White female with nodular lymphocyte predominant Hodgkin lymphoma (NLPHL) receiving CHOP + R as an outpatient. On cycle 2 day 1, the patient received cyclophosphamide 750 mg/m2 (1,402 mg) in NS 250 mL over 60 minutes. She reported mild itching and tingling in her nose towards end of infusion, which resolved without interventions after 40 minutes. The infusion was completed without interruption. This was considered a grade 1 infusion-related reaction. This case had a Naranjo algorithm total score of 5 (probable).
#2: The same patient presented on cycle 3 day 1 as an outpatient, and during the infusion, she experienced a tingly sensation on the nose and a cough, leading the team to pause the infusion for 10 minutes. Once restarted at the same infusion rate, the patient did not have any other symptoms. This repeat reaction was considered a grade 2 infusion-related reaction, as the infusion was paused and later resumed. Of note, the patient tolerated a subsequent cyclophosphamide dose without any AEs noted in the chart, as an outpatient. This case had a Naranjo algorithm total score of 7 (probable).
#3: 71-year-old Asian female with high-grade B cell lymphoma receiving EPOCH + R as an inpatient. On cycle 1 day 4, the patient received cyclophosphamide 750 mg/m2 (1,200 mg) in NS 250 mL over 60 minutes. After the infusion, the patient complained of chest pain and was placed on overnight telemetry monitoring. She also experienced nausea and vomiting, which was treated with ondansetron. This was considered a grade 1 infusion-related reaction. After discharge, the patient tolerated 8 subsequent doses of cyclophosphamide administered over 60 minutes without any AEs, as an outpatient. This case had a Naranjo algorithm total score of 2 (possible).
#4: 75-year-old White female with newly diagnosed MM receiving CyBorD + Dara as an outpatient. The patient received cyclophosphamide 300 mg/m2 (552 mg) in NS 250 mL over 60 minutes. The patient became hypertensive after the infusion with a blood pressure reading of 177/85 mmHg, which could have also been related to the sodium chloride content of the bag and/or concurrent dexamethasone administration. This was considered a grade 1 infusion-related reaction. The patient tolerated a subsequent infusion without any adverse events and was switched to oral cyclophosphamide as outpatient, per patient and provider preference. This case had a Naranjo algorithm total score of 2 (possible).
#5: 61-year-old White female with a peripheral T-cell lymphoma (PTCL) with a high tumor burden started CHOEP as an inpatient. On cycle 1 day 1, cyclophosphamide was administered at 750 mg/m2 (1,320 mg) in NS 250 mL over 30 minutes. The team had started NS hydration at 100 mL/hour to mitigate potential tumor lysis syndrome (TLS) due to tumor burden and administered a dose of furosemide 20 mg PO with known peripheral edema. Recent ejection fraction was 67%. The patient also received dexamethasone 4 mg PO (2 doses) and fosaprepitant 150 mg in NS 150 mL (1 dose) prior to the cyclophosphamide infusion. The patient tolerated the cyclophosphamide infusion itself without issues, but with ongoing infusion of NS for about 4.5 hours (i.e., 450 mL), the patient developed transient hypotension (83/47 mmHg to 92/54 mmHg without intervention, which was close to baseline) and hypoxia requiring intervention (baseline 90% on room air; newly 89% on room air and improved to 94% on 2 liters of oxygen via nasal cannula). A chest x-ray confirmed a small right pleural effusion. The team held NS IV fluids, and the patient then received etoposide 100 mg/m2 (176 mg) in NS 500 mL over 120 minutes without any issues. This event was considered a grade 2 infusion-related reaction to cyclophosphamide, as there was a prompt response to intervention (e.g., oxygen, cessation of IV fluids) and short therapy interruption (e.g., chest x-ray for assessment, delay of etoposide administration). After discharge, reassuringly, the patient tolerated 6 doses of cyclophosphamide infused over 30 minutes as an outpatient. This case had a Naranjo algorithm total score of 2 (possible).
#6: 47-year-old Black female with diffuse large B-cell lymphoma (DLBCL) being treated with CHOP + R as an outpatient. On cycle 1 day 1, she received cyclophosphamide 750 mg/m2 (1,275 mg) in NS 250 mL over 30 minutes. After 10 minutes of the infusion, the patient complained of facial tightness and hypertension to 148/93 mmHg. The infusion was paused, and then resumed after 30 minutes. Two minutes after restarting, the patient had the same reaction. The infusion time was then modified to 60 minutes instead. This was considered a grade 2 infusion-related reaction as there was a prompt response to intervention (e.g., cessation of infusion) and short therapy interruption (e.g., delay of re-infusion). Subsequent cyclophosphamide infusions were administered and tolerated over 60 minutes as an outpatient, per patient and provider preference. This case had a Naranjo algorithm total score of 7 (probable).
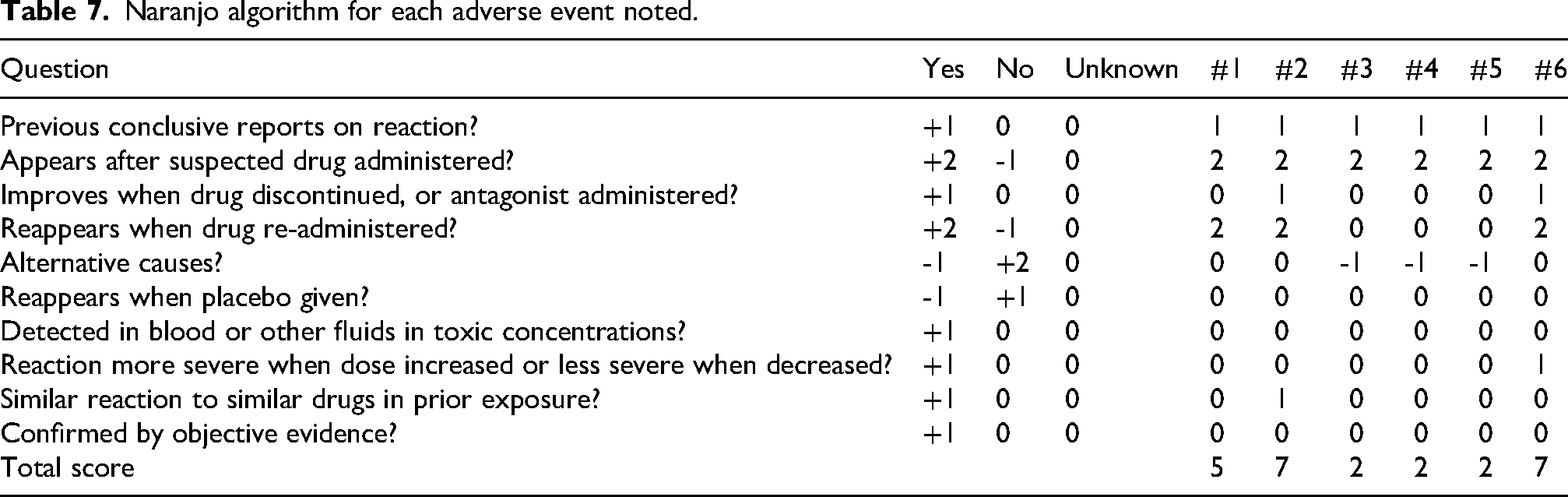
Table 7 summarizes the Naranjo algorithm scoring for each AE noted above.
Naranjo algorithm for each adverse event noted.
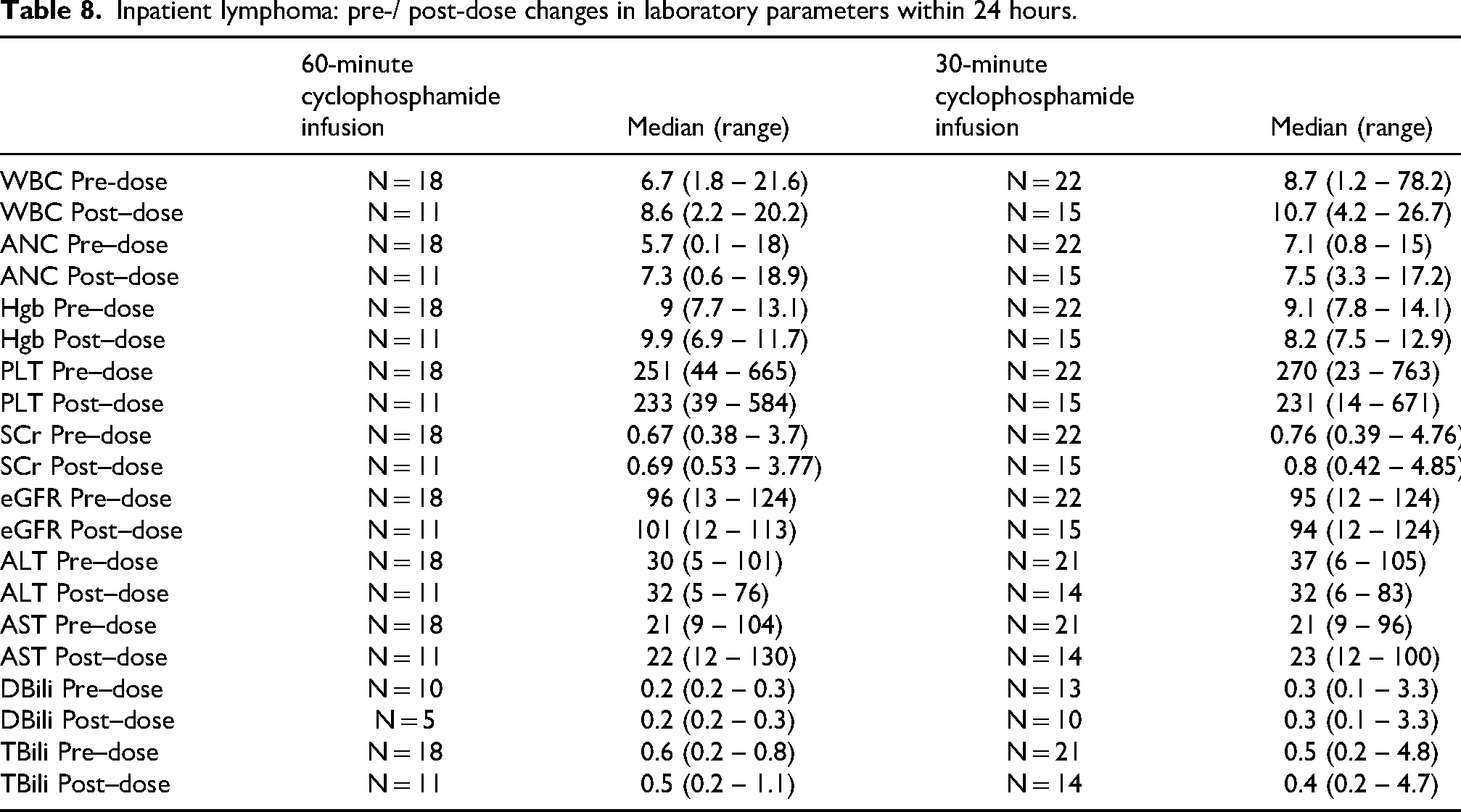
As detailed in Tables 8 and 9, when analyzing post-dose administration trends (specifically within 24 hours) in inpatient pre-/post-implementation lymphoma or MM groups, there were no major laboratory changes (in median WBC, ANC, Hgb, PLT, SCr, eGFR, ALT, AST, DBili, or TBili), with limitations in interpretation due to missing post-dose data (e.g., driven mostly by discharge from hospital after administration of the cyclophosphamide dose). Outpatient laboratory changes were unable to be assessed accurately due to variations in follow-up visits. While interpretations were limited by doses with actual concurrent laboratory data, this was hypothesis-generating for potential future analyses.
Inpatient lymphoma: pre-/ post-dose changes in laboratory parameters within 24 hours.
Inpatient MM: pre-/ post-dose changes in laboratory parameters within 24 hours.
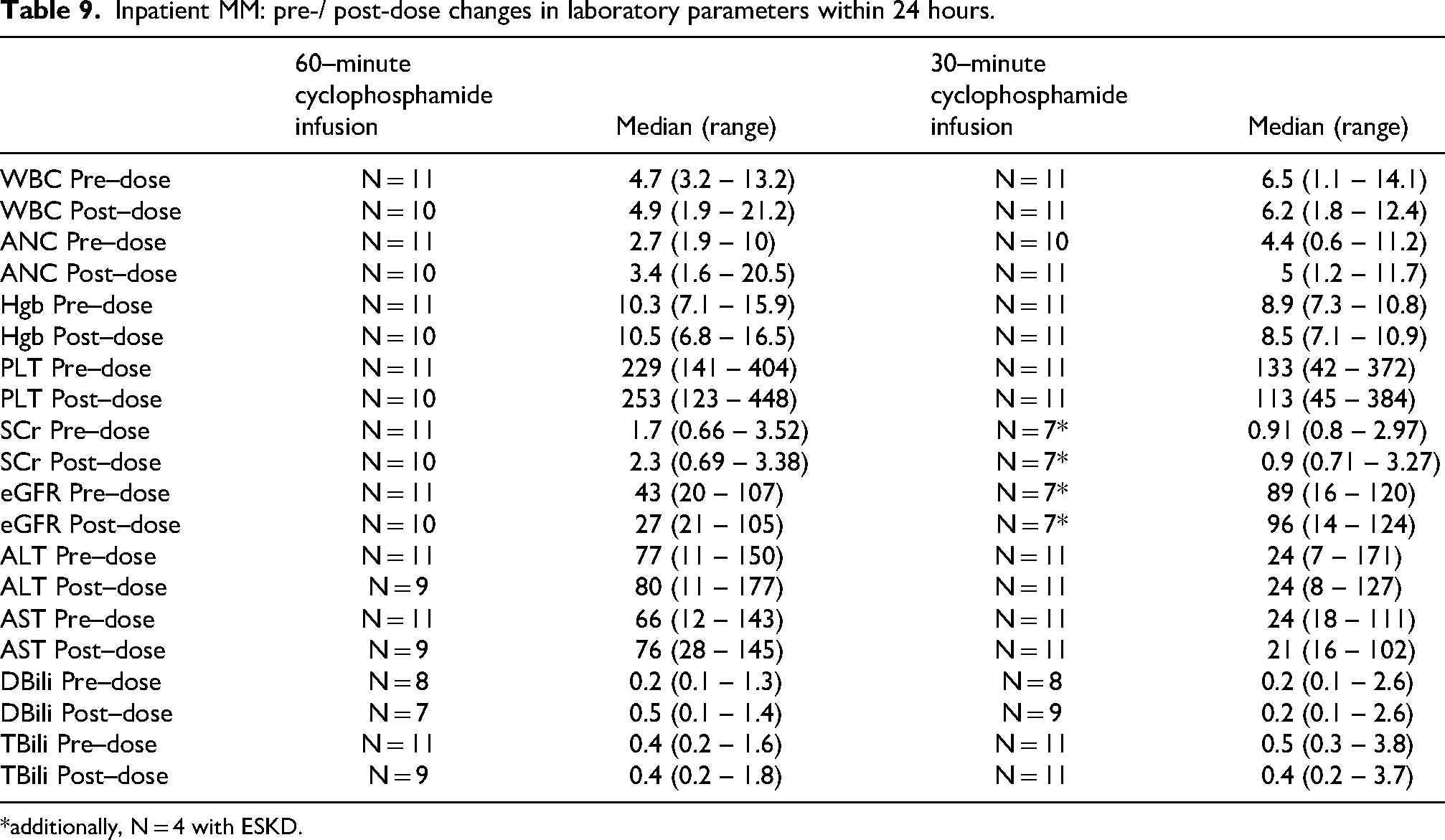
*additionally, N = 4 with ESKD.
Discussion
Within the selected chemotherapy regimens for MM, based on patient and provider preference, there already exists an option to change the route of administration. While this type of intravenous to oral (IV to PO) conversion would affect pill burden (as cyclophosphamide capsules are only commercially available in 25 or 50 mg doses), it wholly mitigates the IV route in the CyBorD (or VCD) +/- Dara regimen.5,12 Daratumumab and bortezomib would be subcutaneous (SC) injections, while cyclophosphamide and dexamethasone would be PO.12 Conversely, within the KCyD +/- Dara regimen, even if the cyclophosphamide were transitioned to PO, the carfilzomib would remain as an IV bolus as there is no alternative route of administration for that drug.5,13–15
Limitations
There were limitations in this study due to its retrospective design. We relied on the documentation within progress notes for the determination of AEs and the description of how patients were treated.
Although results were based on the number of doses (n = 400) rather than the number of patients (n = 117) who received cyclophosphamide, this type of analysis was helpful in the assessment of subsequent dose tolerability.
When comparing the 2 disease-based groups, within the selected chemotherapy regimens for lymphoma, cyclophosphamide was administered at a median 750 mg/m2 once every 3 weeks; and for MM, the drug was administered at a median 300 mg/m2 once per week. Despite differences in dosing, there were no significant changes in laboratory data with inpatient administrations of cyclophosphamide. While limited by group size and co-administration of other drugs within each chemotherapy regimen, these analyses were hypothesis-generating.
A 50% reduction in chair time (from 60 to 30 minutes) is meaningful because cyclophosphamide is frequently utilized in many chemotherapy regimens. While this retrospective chart review did not specifically quantify actual / realized cost savings, such changes could reduce outpatient chair time and permit more infusion visits to be scheduled within the day.
Conclusion
Within selected chemotherapy regimens for lymphoma and MM, the shortening of cyclophosphamide infusion time from 60 to 30 minutes was found to be feasible and safe, with no Grade 3 or higher AEs noted.
Based on these findings, future steps at our institution would include re-evaluating and potentially shortening infusion times in treatment plans that contain cyclophosphamide for other conditions / indications (e.g., stem cell collection, bone marrow transplant, CAR-T lymphodepletion, breast cancer, sarcoma).
Footnotes
Acknowledgments
Not applicable
Ethical approval and informed consent
Study was approved by Institutional Review Board.
Author contributions
SD, CB, and MAR designed the study. SD and MAR collected the data. SD, CB, and MAR performed the analysis and interpreted the results. SD, CB, and MAR drafted the manuscript. All authors reviewed and approved the final version of the manuscript.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Declaration of conflicting interest
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Data availability
Available upon request.
Prior publication
A prior version of this study was presented as an ePoster at the Leukemia, Lymphoma, and Myeloma Congress 2025.