
Abstract
Introduction
The advent of tyrosine kinase inhibitors (TKI) has revolutionised the treatment of chronic myeloid leukaemia (CML). Nevertheless, no specific tools are currently available to support follow-up and guarantee the adequate management of safety, adherence, and effectiveness altogether of TKI-based regimens. This study aimed to introduce a monitoring instrument tailored to patients undergoing TKI therapy for CML.
Data Source
A structured instrument proposal was developed after conducting an integrative review. The instrument was then evaluated by clinicians and laboratory professionals with expertise in onco-haematology, who assessed clarity, objectivity, practicality, and clinical relevance using a five-point Likert scale.
Data Summary
The model comprised three protocols designed to evaluate adherence, safety, and effectiveness of TKI therapy. During evaluation of the instrument, all assessed parameters achieved mean scores ≥ 3.0. By aligning with international guidelines, the instrument consolidates essential monitoring parameters, thereby enhancing clinical decision-making and supporting patient-centred care in CML.
Conclusion
Instruments of this nature are rare and represent an important challenge for healthcare teams managing CML patients. Considering that adherence and safety are critical determinants of therapeutic success, structured tools such as this have the potential to facilitate improved outcomes.
Introduction
Chronic myeloid leukaemia (CML), described over 170 years ago, is characterised by the presence of the Philadelphia chromosome (Ph1), originating from a reciprocal translocation between chromosomes 9 and 22, leading to the BCR::ABL1 oncogene. This genetic lesion results in uncontrolled cell-cycle progression and premature release of immature myeloid cells into the bloodstream.1,2 Epidemiologically, CML is typically diagnosed between the ages of 40 and 70 years, with a mean age of 56 at diagnosis. Incidence is approximately 0.4 cases per 100,000 inhabitants annually, with a higher prevalence in men (male-to-female ratio 1.2–1.7, rising to 1.75–2.0 in the United States). 2
Treatment has undergone significant evolution with the introduction of tyrosine kinase inhibitors (TKI), such as imatinib, which have markedly improved the life expectancy of patients. Previously, individuals faced a prognosis of approximately five years after diagnosis. With the advent of TKI, however, overall survival (OS) now approaches that of the disease-free population, representing a true revolution in the treatment of this neoplasm.3–6 Given that therapy extends throughout the patient's lifetime, continuous monitoring of its implementation and outcomes is essential, allowing for the early detection of therapeutic failures, their underlying causes (such as resistance), and thus enabling timely treatment adjustments to achieve the expected responses more rapidly. 7 Specialised diagnostic tools and therapeutic protocols are available in some countries.8–10 However, regarding the monitoring and assessment of parameters such as adherence and safety, no instruments have been specifically designed for this purpose, nor is there any tool that integrates and unifies guidance for monitoring safety, adherence, and effectiveness (e.g., CML milestones) altogether.
From the perspective of achieving therapeutic success, the absence of tools for pharmacists to monitor the use of these medicines poses a significant challenge for disease management. Non-adherence to therapy is recognised as a critical factor leading to drug resistance and disease progression. 11 Nonetheless, safety concerns, including adverse reactions (ADR) and drug interactions, strongly influence adherence, particularly given the reliance of TKI on CYP3A4 enzymes for metabolism.12,13 Therefore, the aim of this study was to develop an integrative pharmacotherapeutic monitoring tool to empower pharmacists in optimising TKI management and evaluating their effectiveness, safety, and adherence in CML patients receiving TKI-based therapy.
Data source and evaluation of the instrument
A previous integrative review, conducted between March and December 2023, has already been accepted for publication, and served as the basis for the present study.
Based on the collected data, an integrative tool for pharmacotherapeutic monitoring of TKI use in CML patients was developed, primarily in the form of flowcharts — one for each parameter: effectiveness, adherence, and safety. Canva® was used for this purpose, following the recommendations of the ISO (International Organization for Standardization) 5807:1985 (confirmed in 2019).
The proposed instrument model was submitted for evaluation. Thus, an online form was developed with assessment items organised into three domains (adherence, effectiveness, and safety). Invitations, the instrument, the Informed Consent Form, and the link to complete the form were emailed to each participant.
Twenty healthcare professionals with clinical or laboratory experience in onco-haematology, including pharmacists, physicians, and nurses, were invited. Eligibility criteria required that they currently work, or had previously worked, in the management, diagnosis, and/or clinical-laboratory monitoring of haematological neoplasms for at least three years within the past decade. A multidisciplinary group of professionals was deliberately recruited to reinforce the comprehensive nature of treatment monitoring and to enrich the instrument with diverse perspectives, ensuring that it fully addresses the specificities of TKI use in CML patients.
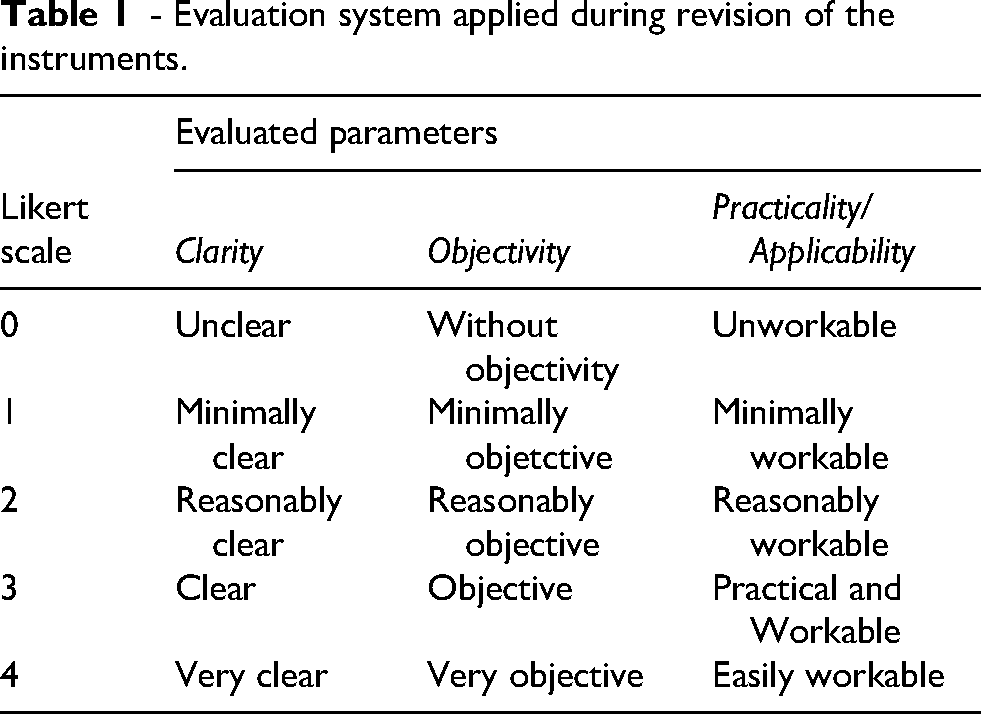
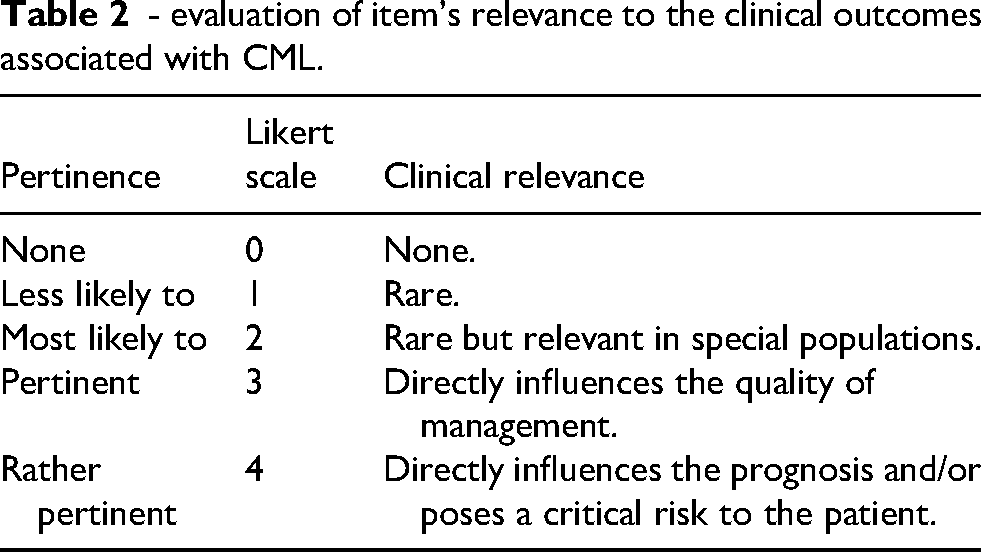
Each participant evaluated the instrument for clarity, objectivity, practicality/applicability, and relevance using a five-point Likert scale (0–4) for each parameter. The relevance of all items was assessed based on the participants’ judgement of their importance to clinical outcomes in CML (Tables 1 and 2).
- Evaluation system applied during revision of the instruments.
- evaluation of item's relevance to the clinical outcomes associated with CML.
Items with a mean score of two or higher were considered approved. A free-text field was provided at the end of the form for additional suggestions. If any of the four parameters failed to reach the minimum threshold for any criterion, the item was revised and resubmitted to participants for re-evaluation. After analysing participants’ feedback, the instrument was further refined. The final version was then prepared and emailed to all participants. This study was approved by the Human Research Ethics Committee of UFSC (CEPSH-UFSC), approval number 74240923.9.0000.0121.
Data summary and the instrument
Effectiveness
Overall, review articles,14,15 international guidelines; mainly European Leukaemia Net (ELN) and National Comprehensive Cancer Network (NCCN); and clinical studies discussed in these reviews indicated that the time to achieve cytogenetic responses ranges from two weeks to one month, and molecular response (MR) is usually achieved within up to three months. Some divergent points were, however, identified with respect to MR.8,9
The German CML IV Experience 16 demonstrated that patients who achieved an early MR (EMR), defined as less than 10% of BCR::ABL1 transcripts within the first three months of treatment, had superior OS compared to those with transcript levels above 10% during the same period. This finding has sparked debate among authors due to the lack of consensus on how to define failure or alert situations in patients who do not achieve EMR, with the discussion extending also to the interpretation of major molecular response (MMR).
The crux of the discussion concerns the appropriate timing for switching TKI. The divergence lies in the fact that, according to the NCCN, MMR may be achieved up to the end of the fifth quarter of treatment without necessarily indicating failure or imminent resistance, as nearly 60% of patients who achieved EMR went on to obtain a MMR by the 15th month of therapy. In this context, the outcome is interpreted merely as a warning signal, prompting investigation of issues such as non-adherence or drug interactions. Conversely, the ELN recommends considering an immediate TKI switch in the absence of MMR within 12 months, considering this as indicative of secondary resistance to the drug in use.8,9,16
According to other guidelines, such as those of European Society of Medical Oncology (ESMO) and the Brazilian therapeutic protocol (PCDT), a BCR::ABL1 value > 0.1% (provided it remains below 1% in the case of ESMO) does not in itself constitute therapeutic failure. Rather, it indicates the need for closer monitoring, without a direct association with secondary resistance. This situation is interpreted as a possible pharmacodynamic or pharmacokinetic peculiarity inherent to a subgroup of patients who are slower to achieve a MMR within the first 12 months of treatment, but who may eventually reach this milestone.10,17
Adherence
Unlike other guidelines, the NCCN also emphasises the role of the patient as an active participant in therapeutic decision-making. This approach is noteworthy from the perspective of treatment persistence, as it positions the patient as a key protagonist in their own care; an aspect increasingly recognised as fundamental to long-term adherence and sustained therapeutic success. 8
Richard, Glasser, and Lussier 18 have demonstrated that active patient participation in treatment decisions enhances understanding of clinical guidelines, which is essential to achieving therapeutic goals. Similarly, Jørgensen and Rendtorff 19 discussed the broader implications of patient involvement in disease management, including the ethical dimension of respecting the patient's autonomy, as well as improving their understanding of both their health condition and treatment. This is particularly relevant given the direct impact on adherence and, consequently, therapeutic success. In this context, Herledan et al. 20 emphasise the pivotal role of the pharmacist in patient education, ensuring appropriate guidance on therapy, providing information on potential ADR, implementing suitable management strategies when necessary, and clarifying the clinical implications of treatment. 21
Despite its recognised importance, few studies specifically address adherence and the range of factors that must be considered in its evaluation or in the development of strategies to overcome related challenges. This highlights a clear gap in the literature that warrants further investigation, particularly given that non-adherence is one of the main causes of loss of response and is closely associated with therapy resistance.11,14
Studies have reported that strategies to improve patient adherence to TKI, especially when it is unintentional, include effective communication, the use of reminder devices and logs, counselling, simplification of the therapeutic regimen, pharmaceutical monitoring programmes, and the implementation of frameworks such as the “4Es.” This strategy applies four principles; education, empowerment, encouragement, and execution; to foster greater patient awareness and autonomy in managing therapy, for example by engaging patients in discussion about the proposed guidelines rather than merely instructing them to take the medication.22,23
This relationship between optimal response and adherence has been consistently demonstrated in the literature. Marin et al. 11 showed that patients with adherence rates below 90% (considered to be suboptimal adherence) had significantly lower probabilities of achieving MMR or complete molecular response (CMR), with no satisfactory MR observed when adherence was ≤ 80%. Similarly, Al-Dewik et al., 24 in a cohort from Qatar, found that adherent patients were far more likely to obtain optimal responses compared with non-adherent ones (95% vs. 14.3%). In a large U.S. cohort, Haque et al. 25 demonstrated that higher adherence combined with regular molecular monitoring was associated with markedly reduced risk of disease progression or mortality.
The monitoring of the parameter must consider its multifactorial nature, including disease-related factors, patient socioeconomic conditions, access to medicines and quality of healthcare services, communication with the healthcare team, and the toxicity profile of the therapeutic regimen. 26 It was also acknowledged that adherence to TKI therapy is usually not measured directly (e.g., laboratory determination), but rather indirectly (e.g., questionnaires, pill counts, or the Medication Possession Ratio (MPR%)). Given its complexity and relevance to therapeutic success, adherence monitoring should ideally be performed using a combination of two or more methods. This approach increases accuracy in identifying problems and supports healthcare professionals in selecting the most appropriate interventions. 21
Recent systematic reviews, such as Tan et al., 7 have highlighted the use of instruments such as the MPR%. However, its application in some countries may face obstacles, as it requires the existence of integrated health systems to verify the amount dispensed over a given period. Another disadvantage of this instrument is its low accuracy in detecting specific deviations, being more appropriate for evaluating treatment persistence. Pill count, in turn, is a practical and objective strategy, but it only measures the quantity of medication taken and does not reveal the underlying causes of non-adherence.27–29 To overcome these gaps, the ARMS (adherence to refills and medications scale) questionnaire represents a versatile strategy that can be integrated with pill counting, providing complementary information that allows professionals to identify the most likely reasons for adherence problems and to design targeted interventions. 30
Even with several tools available for use, however, McCue, Lohr, and Pick 23 highlighted the lack of studies addressing the structuring of methods for proper indirect assessment of adherence in patients with CML. Consequently, monitoring of TKI use may fall below the level required for this clinical condition. 31
Safety
Regarding treatment safety, studies focus primarily on reporting ADRs, without addressing their management. Potential drug interactions are rarely discussed in the literature; a particularly concerning omission, given that TKI are metabolized via CYP3A4. Such interactions can significantly alter TKI plasma levels, leading to toxicity (potentially compromising adherence) or reduced efficacy (potentially compromising therapeutic response and patient survival).
For instance, co-administration with strong CYP3A4 inhibitors such as azole antifungals (e.g., ketoconazole, itraconazole) or macrolide antibiotics (e.g., clarithromycin) can markedly increase TKI plasma concentrations and the risk of adverse events. Conversely, CYP3A4 inducers such as rifampicin, phenytoin, or carbamazepine can substantially reduce TKI exposure, jeopardising therapeutic response. Other clinically relevant interactions include anticoagulants such as warfarin, where altered metabolism may lead to unstable anticoagulation control. These examples illustrate that monitoring for interactions is a critical component of pharmacotherapeutic follow-up and should be systematically integrated into clinical practice.32–38
Closely related to adherence, treatment safety plays a crucial role in medication persistence, particularly during the initial stages of therapy adaptation. The toxicity profile of a drug is the main factor limiting its safe use, although in this clinical context the benefits often far outweigh the risks. Fortunately, TKI-based therapy generally demonstrates a favourable safety profile and is usually well tolerated. The most common ADR are typically moderate and manageable. Nevertheless, it should be noted that some adverse effects may result from drug interactions, which can compromise both the safety and the effectiveness of treatment.
Knowing that the occurrence of ADR during TKI therapy is an important cause of treatment discontinuation or missed doses, as highlighted by Rosti et al., 39 their early identification and management should be a priority. Therefore, periodic safety assessments are recommended. During consultations, when identifying signs and symptoms potentially associated with treatment, the pharmacist should evaluate the causal relationship and, whenever possible, provide guidance on management or refer the patient to the prescribing physician, thereby reducing the likelihood of discontinuation due to intolerance of ADR.
The instrument
The instrument was structured into three sections, incorporating essential and clinically relevant information identified in the previous stage (Figures 1 to 4). The model was evaluated by 10 professionals: seven pharmacists (including clinical pharmacists, generalists, and biochemists) and three haematologists.
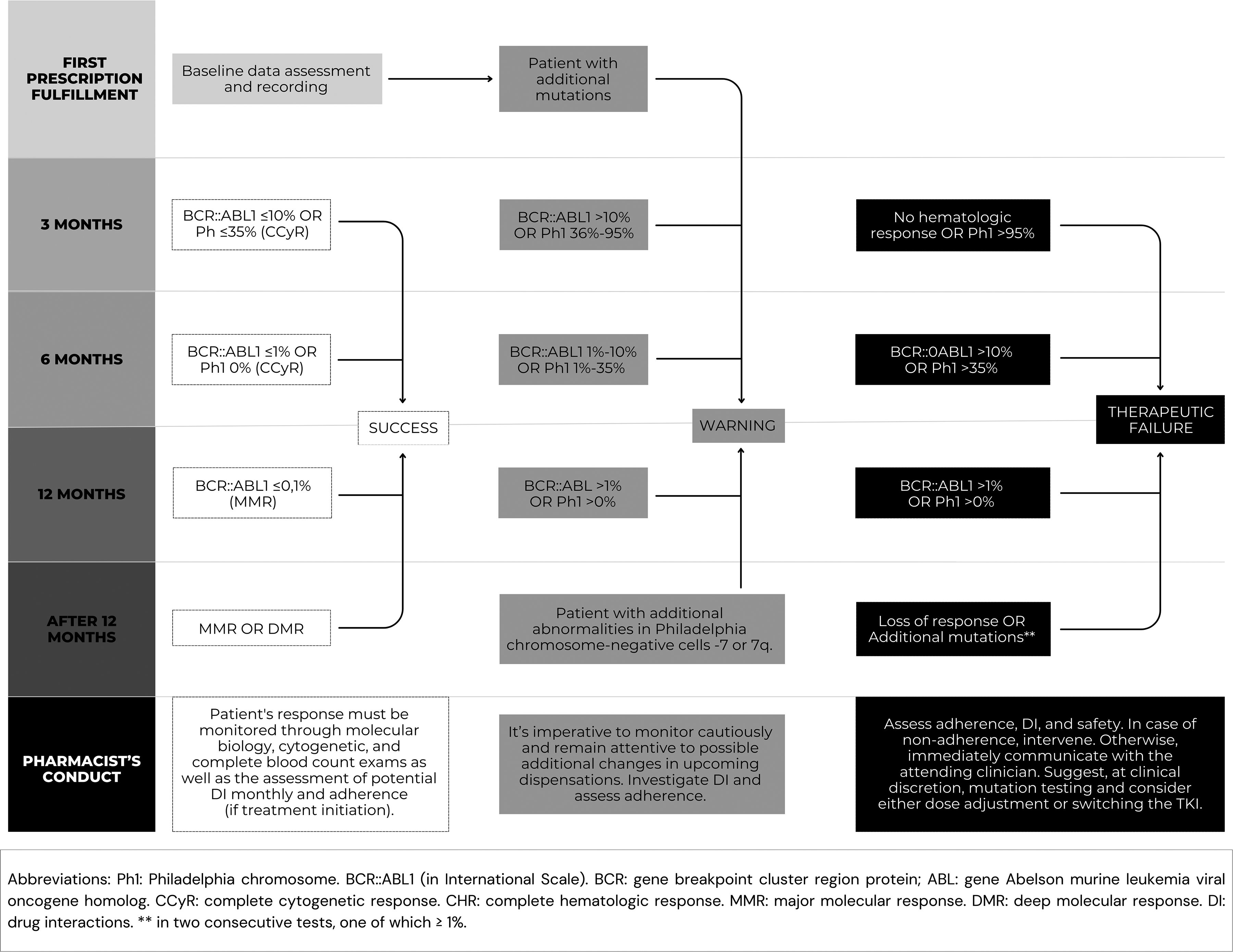
Treatment milestones.
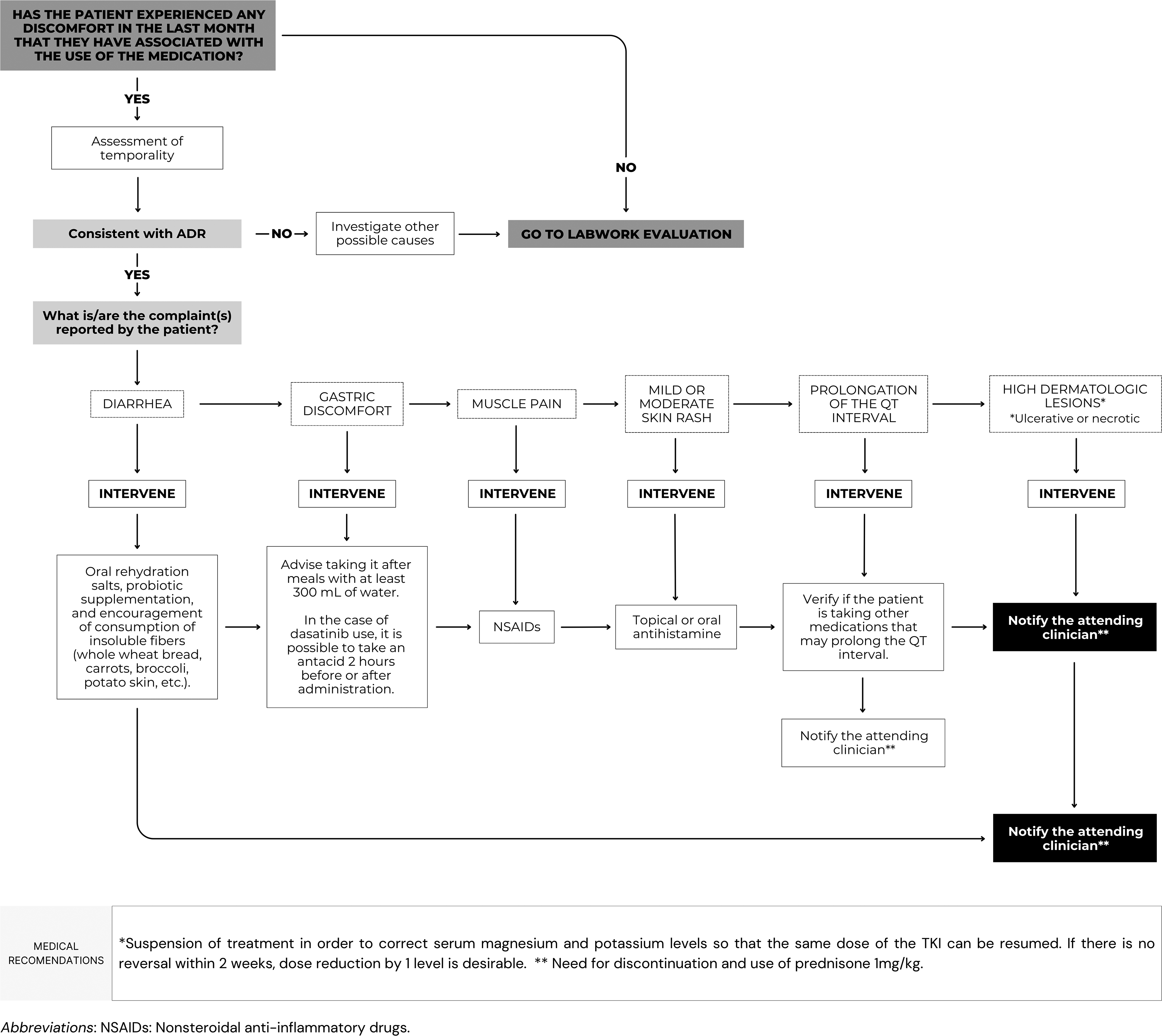
Clinical evaluation of the treatment safety.
Laboratory evaluation of the treatment safety.
Adherence assessment.
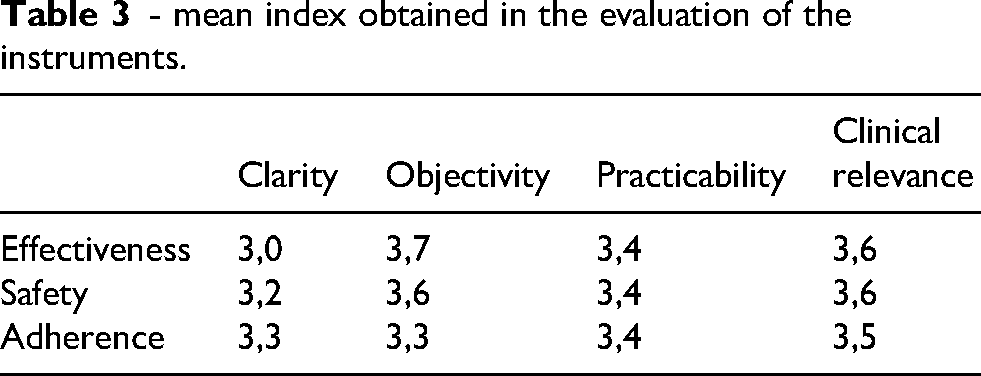
All evaluated parameters achieved an average score above 3 on the Likert scale and were therefore approved (Table 3). Suggestions provided by the professionals for improving the instrument mainly concerned formatting and presentation aspects. Additional recommendations included the incorporation of guidance on missed doses during treatment and on key reported drug interactions. These elements were subsequently added to the instrument to reflect the participants’ contributions.
- mean index obtained in the evaluation of the instruments.
The integrative instrument was organised into flowcharts designed to guide clinical decision-making, making the evaluation process more intuitive and standardised for pharmacists.
The effectiveness section (see Figure 1) establishes clear therapeutic milestones, such as achieving cytogenetic and MR at specific time points (3, 6, and 12 months). At each stage, the pharmacist is instructed to assess the patient's clinical and laboratory data, interpret results, and determine whether the response is optimal, suboptimal, or indicative of therapeutic failure. In cases where warning signs or deviations are identified, the protocol directs the pharmacist to investigate potential causes; including non-adherence, drug interactions, or safety issues; and to either intervene directly within their scope of practice or promptly refer the patient to the physician.
The structured design of this instrument reinforces the pharmacist's role as an active member of the multidisciplinary team, promoting early detection of problems that could compromise MR and, therefore, OS. Moreover, it provides a practical framework that can be applied in outpatient settings, ensuring consistency in monitoring and enhancing the integration of pharmaceutical care into routine clinical practice.
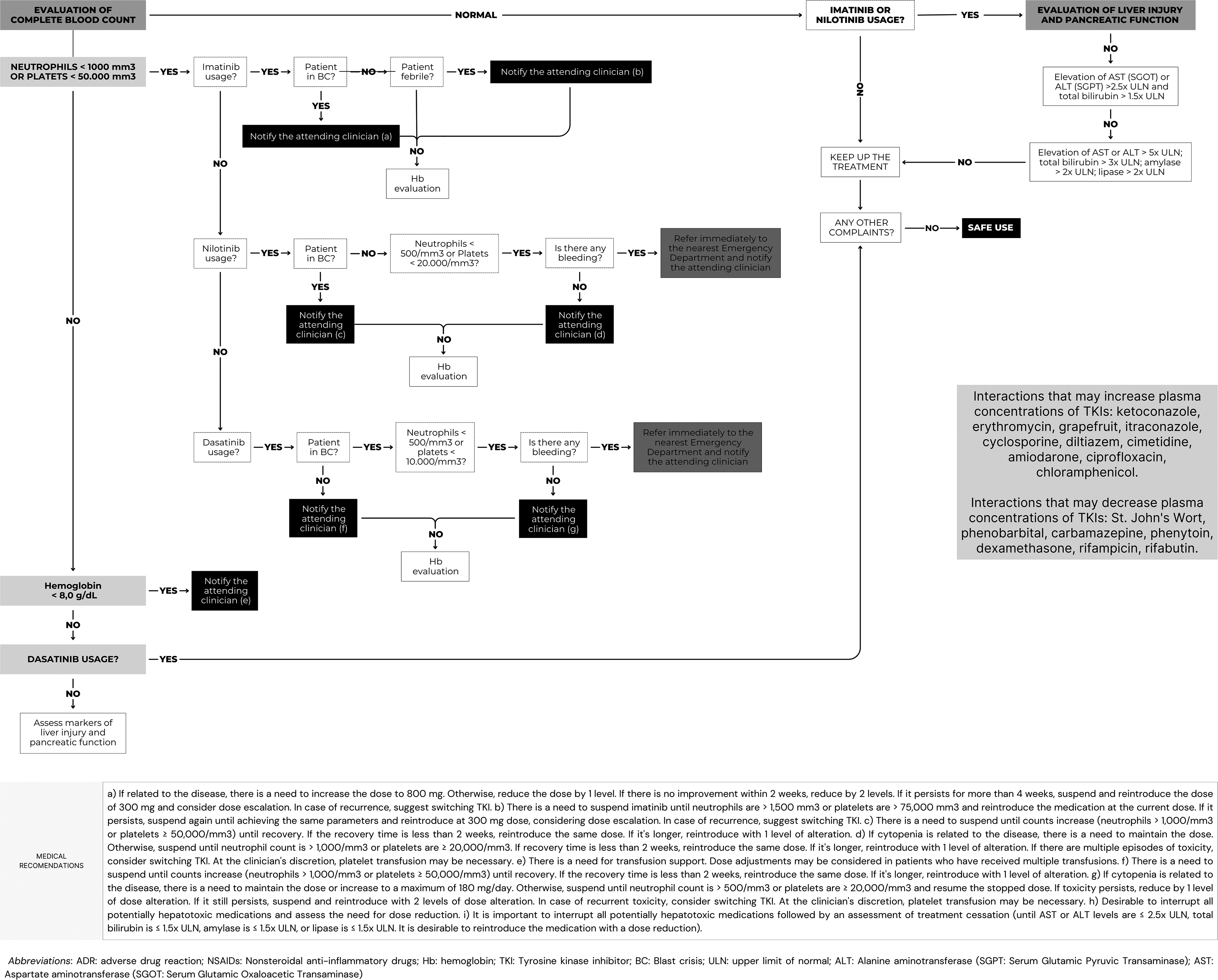
The safety protocol developed aimed to outline the main management strategies, distinguishing those interventions that fall within the pharmacist's scope of practice from those that are the responsibility of the physician. In this way, it facilitates the pharmacist's identification and intervention, while also clarifying the situations that require referral to the physician and the actions recommended in response to the problems that are identified more frequently in clinical practice.
To properly organise this topic, two flowcharts were developed: one for the clinical evaluation of signs and symptoms (see Figure 2), such as diarrhoea and rash, and another for the evaluation of laboratory data (see Figure 3), particularly hepatic transaminases and complete blood count. It is recommended that the instrument be used digitally or printed in larger formats. Incorporating this instrument into navigation applications would represent an advance in clinical practice and patient care for individuals living with CML. The goal is to make these treatments as safe as possible, thereby ensuring both adherence and effectiveness.
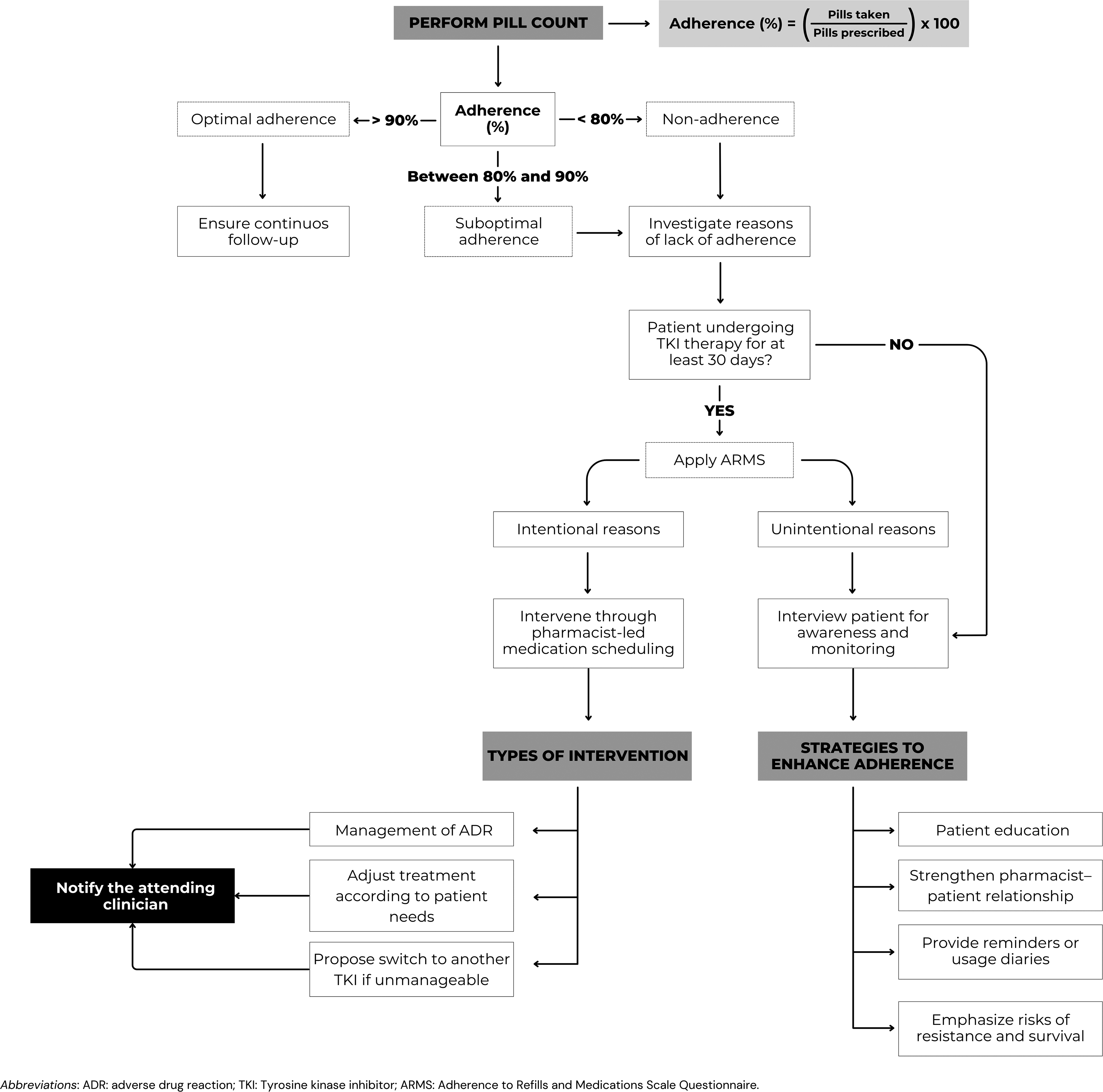
Finally, the adherence assessment protocol (see Figure 4) integrates both objective and subjective methods of adherence assessment. Initially, pill counting is performed to quantify medication use, classifying patients as optimally adherent (≥ 90%), sub optimally adherent (80–90%), or non-adherent (< 80%). This objective measure is complemented by the application of the ARMS questionnaire, which helps identify the most likely causes of non-adherence; whether intentional, such as dose omission or treatment interruption due to ADR, or unintentional, such as forgetfulness or misunderstanding of the regimen.
By combining direct measurement, validated questionnaires, and pharmaceutical counselling, the protocol offers a comprehensive approach to adherence monitoring. It provides pharmacists with a clear framework to identify problems early, propose tailored interventions, and strengthen continuous follow-up. As such, the tool not only presents a proposal of standardization of adherence assessment but also reinforces the pharmacist's role as an active agent in ensuring persistence with TKI therapy and maximising therapeutic success in CML.
By aligning with international guidelines and translating it into an operational tool that considers the various scopes of practice assigned to pharmacists across different countries, this instrument provides a means to standardise follow-up, optimise therapeutic responses, and strengthen patient-centred care in CML.
Conclusion
Without a doubt, the monitoring of these treatments can bring substantial benefits to patients living with CML, as well as to the entire healthcare team involved. They allow early identification of problems related to adherence, effectiveness, and safety that may compromise MR and OS. In general, these instruments will provide support to professionals in carrying out their activities, facilitating their role as active participants in the care of these patients. The instrument construction process, grounded in recent literature, the main guidelines, and expert revision, provides an initial framework to support the monitoring of these therapies.
Nevertheless, as this study was based on an integrative review, the instrument should be interpreted as a starting point rather than a definitive tool. Its value lies in offering practical guidance and highlighting key aspects of pharmaceutical care that can improve patient follow-up. Future research, including systematic reviews and large-scale validations on patients, is needed to consolidate these findings and refine the instrument in accordance with each health service. In this way, the tool developed here contributes to advancing patient-centred monitoring in CML, while also pointing to the need for more rigorous evidence to strengthen future clinical recommendations.
Limitations of the study
This study has limitations. First, it is product of an integrative review of the literature. As such, it did not include a formal risk of bias assessment or evaluation of the quality of evidence of the included studies. Consequently, the findings should be interpreted with caution. Also, the exploratory nature of this work limits its ability to provide definitive recommendations for clinical practice, but rather a clinical guidance. Despite these limitations, this study highlights an underexplored research field and provides an initial framework to guide future investigations aimed at strengthening the evidence base for monitoring TKI therapy in CML patients, reinforcing the role of care as a determinant of therapeutic success.
Footnotes
Acknowledgements
The authors would like to thank the Library team of the Federal University of Santa Catarina for their assistance in conducting the integrative review, a primary step in the development of this protocol.
Ethical considerations
This study was approved by the Human Research Ethics Committee of UFSC (CEPSH-UFSC), approval number 74240923.9.0000.0121.
Consent to participate
Invitations, the instrument, the Informed Consent Form (ICF), and the link to complete the form were electronically sent to each participant by e-mail after approval from the Ethics Committee
Author contributions
GCG: Academic and intellectual conception of the entire project. Structuring of the protocols. Conduction of the integrative review. Writing of the manuscript. JARP: Conducting of the integrative review. VMR: Structuring of the flowcharts. Adjustment of design and format to technical standards. MRMR: Academic and intellectual conception of the project. Structuring of the protocols. Writing of the manuscript.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Data sharing statement
The data supporting the findings of this study are available from the corresponding author upon reasonable request. All relevant datasets have been anonymised to ensure the confidentiality of participants and comply with ethical and legal requirements. No additional unpublished data are available.