
Abstract
Introduction
Medication complexity is associated with the number of drugs, dosing frequency, dosage form, and additional instructions. Some studies have shown that high medication complexity is associated with several adverse outcomes, including hospitalization, prolonged hospital stay, readmission, and non-compliance with medication, but studies in older cancer patients are quite limited
Methods
This retrospective study included patients with cancer who were hospitalized in the oncology services of the Süleyman Demirel University Research and Practice Hospital between June 2022 and November 2023
Results
The median number of medications used by patients was 6 (IQR, 5-8), and the polypharmacy rate was 79.6%. The median MRCI score was 24 (IQR, 17-31). The total number of medications and age were significant predictors of the MRCI score (p < 0.05). In logistic regression models, the MRCI score was associated with readmission to hospital within 30 and 90 days. (p < 0.05).
Conclusion
In older adult cancer patients, reducing medication complexity as part of medication management may be beneficial in reducing the risk of hospital readmission.
Introduction
Increasing age is a major risk factor for cancer, with most cancer deaths occurring in adults aged 65 and older. 1 Older cancer patients have more comorbidities, frailty, and geriatric syndromes than younger adults. 2 Cancer patients receive chemotherapy regimens and supportive treatments, thus older cancer patients are exposed to polypharmacy. Polypharmacy is associated with drug-drug interactions, adverse drug reactions, increased falls, hospitalizations, and death.3,4 These patients are at a high risk of medication complexity due to polypharmacy. 5
Medication complexity is associated with the number of medications, dosing frequency, dosage form, and additional instructions. 6 The Medication Regimen Complexity Index (MRCI) is a validated tool for assessing medication regimen complexity. 6 The MRCI provides a comprehensive assessment of a patient's medication regimen. 7 Studies have shown that high medication complexity is associated with many adverse outcomes, such as hospitalization, prolonged hospital stay, hospital readmission, and medication non-adherence.8,9 However, some studies have found no relationship between the MRCI score and hospital readmission.10–12
Hospital readmissions are associated with adverse outcomes, such as increased mortality, morbidity, and healthcare costs.13,14 Risk factors for hospital readmission in the general cancer population include advanced cancer, end-of-life status, high incidence of chronic disease, polypharmacy, and abnormal hemoglobin and sodium levels.14,15 Studies assessing medication complexity in older patients with cancer are limited. 16 Therefore, it is important to evaluate the relationship between medication regimen complexity and hospital readmission in older adult patients with cancer.
The primary aim of this study is to determine the association between the Medication Regimen Complexity Index (MRCI) score and readmission to the hospital for any reason within 30 and 90 days. The secondary objective was to identify risk factors associated with the MRCI score.
Materials and methods
Study design
This retrospective study was conducted on patients with cancer who were hospitalized in the oncology services of the Süleyman Demirel University Research and Practice Hospital between June 2022 and November 2023. Patients with cancer aged > 65 years were included in the study. Patients who were hospitalized for less than 24 h and those with insufficient data were excluded. Additionally, patients who could not be followed for 90 days were also excluded from the study. The ethics committee decision was approved by the Süleyman Demirel University Faculty of Medicine Clinical Research Ethics Committee (Approval No: 254, Date: 5.12.2023).
The sample size was calculated using the Raosoft sample size calculator to be at least 130, with a 5% margin of error, 95% confidence, and a 50% distribution ratio. 17
Patient information (sociodemographic, medication, and medical conditions) was obtained from the hospital's electronic medical record system. MRCI and anticholinergic drug scores were calculated and independently assessed by two researchers.
The outcome of this study was to examine the association between MRCI scores and 30- and 90-day readmission rates in older cancer patients. Planned hospital stays are not excluded. Using all patients’ initial hospitalizations during the study period, 30- and 90-day readmission rates were calculated as the time from the index discharge date to the readmission date.
Measures
In this study, polypharmacy was defined as the use of five or more medications.
The MRCI, developed by George et al., 6 was validated in Turkish by Okuyan et al. 18 In this study, the validated Turkish version of the MRCI was used to determine medication regimen complexity with the permission of the authors. The MRCI consists of three sections and 65 items. Section A covers dosage forms, Section B covers dosing frequency, and Section C covers additional directions. The total MRCI score is determined by summing the scores from the three sections. Although the minimum score is 1, there is no specific maximum score. The MRCI score increases as the medication dosage form becomes more complex, the daily dosing frequency increases, and additional directions are added.
The Anticholinergic Cognitive Burden Scale (ACBS) was used to determine anticholinergic medication use. 19 Permission for the scale was obtained from the first author of the study. According to this scale, anticholinergic drugs are classified based on their anticholinergic potency, with scores ranging from 0 to 3. Drugs with in vitro affinity for muscarinic receptors but no clinically significant adverse cognitive effects are assigned a score of 1 (probably anticholinergic). Drugs with blood-brain penetration, clinically significant anticholinergic effects, and a reported association with delirium are assigned a score of 2 or 3. 19 The updated version of the ACBS was used in this study. 20 Furthermore, an ACBS score >1 was considered to indicate anticholinergic medication use.
Statistical analysis
Statistical analyses were performed using the Social Sciences Statistical Package (SPSS) version 20. The Kolmogorov-Smirnov Test was used to determine whether the data were normally distributed. Variables were expressed as mean ± standard deviation, median (interquartile range), and percentage (%). If the data were normally distributed, the Student t-test was used. If the data were not normally distributed, the Mann-Whitney U test was used. The Chi-square test was used to compare categorical variables. The Chi-square test was used to compare categorical variables.
A multiple linear regression model was created to identify characteristics associated with and influencing MRCI. The model was examined for multicollinearity and autocorrelation. Binary logistic regression models were developed to identify prognostic factors associated with 30- and 90-day hospitalizations. In the linear regression model, forward selection was used in the second stage; in the logistic regression model, coefficients for only significant variables were estimated using the forward stepwise likelihood ratio (LR) method. p-values less than 0.05 were considered statistically significant.
Results
A total of 137 patients were included in this study, and thirty-seven point two percent of the patients were female. The median age was 70 years (IQR, 67-76). The median total number of drugs used by patients was 6 (IQR, 5-8), and polypharmacy was 79.6%. The median MRCI score was 24 (IQR, 17-31), and anticholinergic drug use was 25.5%. The patients were mostly diagnosed with lung (16.8%), colorectal (13.1%), breast (8%), pancreatic (8%), or prostate (8%) cancer. Most patients had hypertension (38%) and diabetes (29.9%). Table 1 shows the sociodemographic characteristics of the patients.
Socio-demographic and clinical characteristics of the patients.
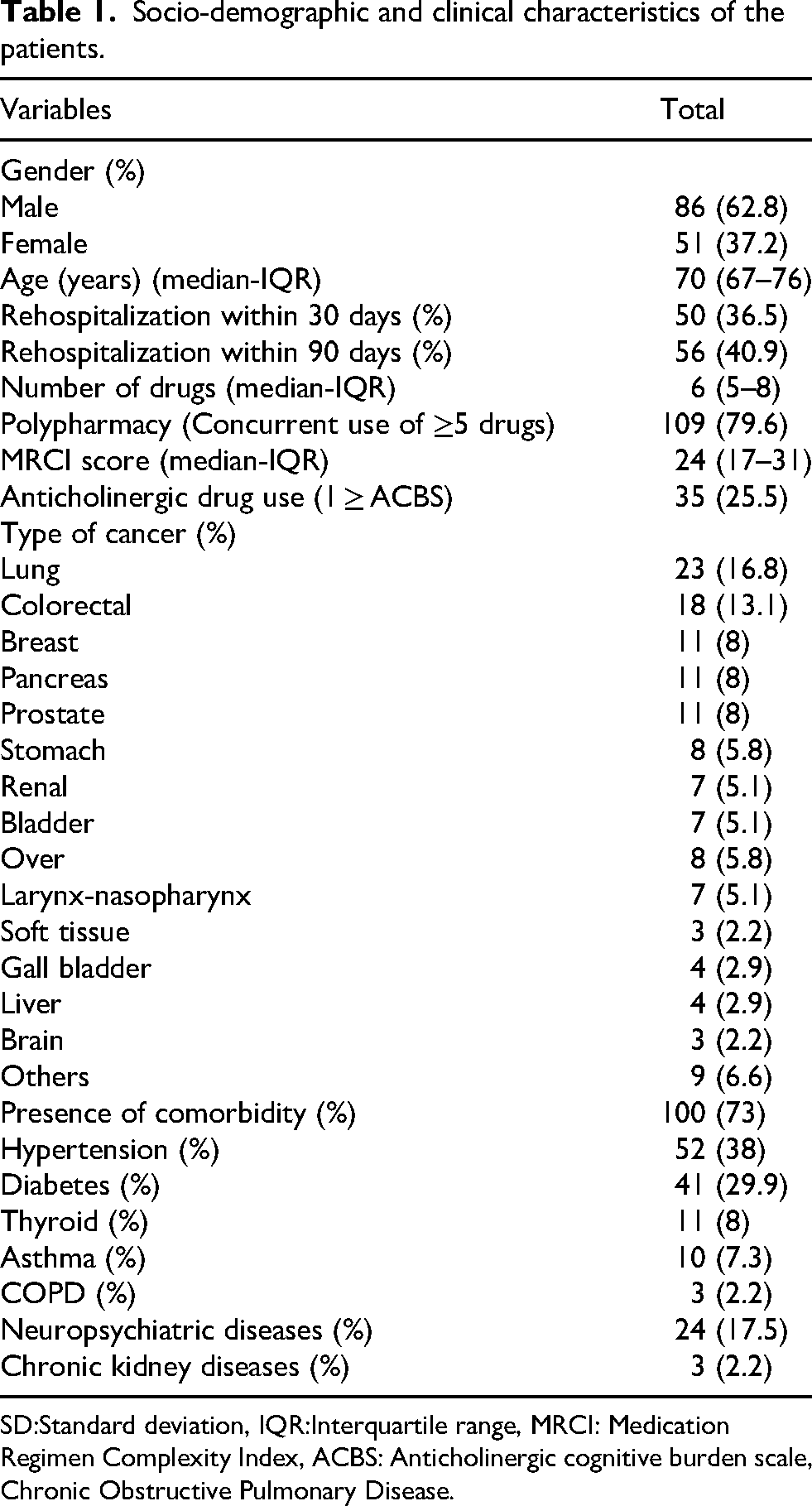
SD:Standard deviation, IQR:Interquartile range, MRCI: Medication Regimen Complexity Index, ACBS: Anticholinergic cognitive burden scale, Chronic Obstructive Pulmonary Disease.
The MRCI score was statistically significantly higher in those with polypharmacy than in those without, and in those using anticholinergic drugs than in those not using (p < 0.05) (Table 2).
The relationship between patient clinical characteristics and MRCI scores.
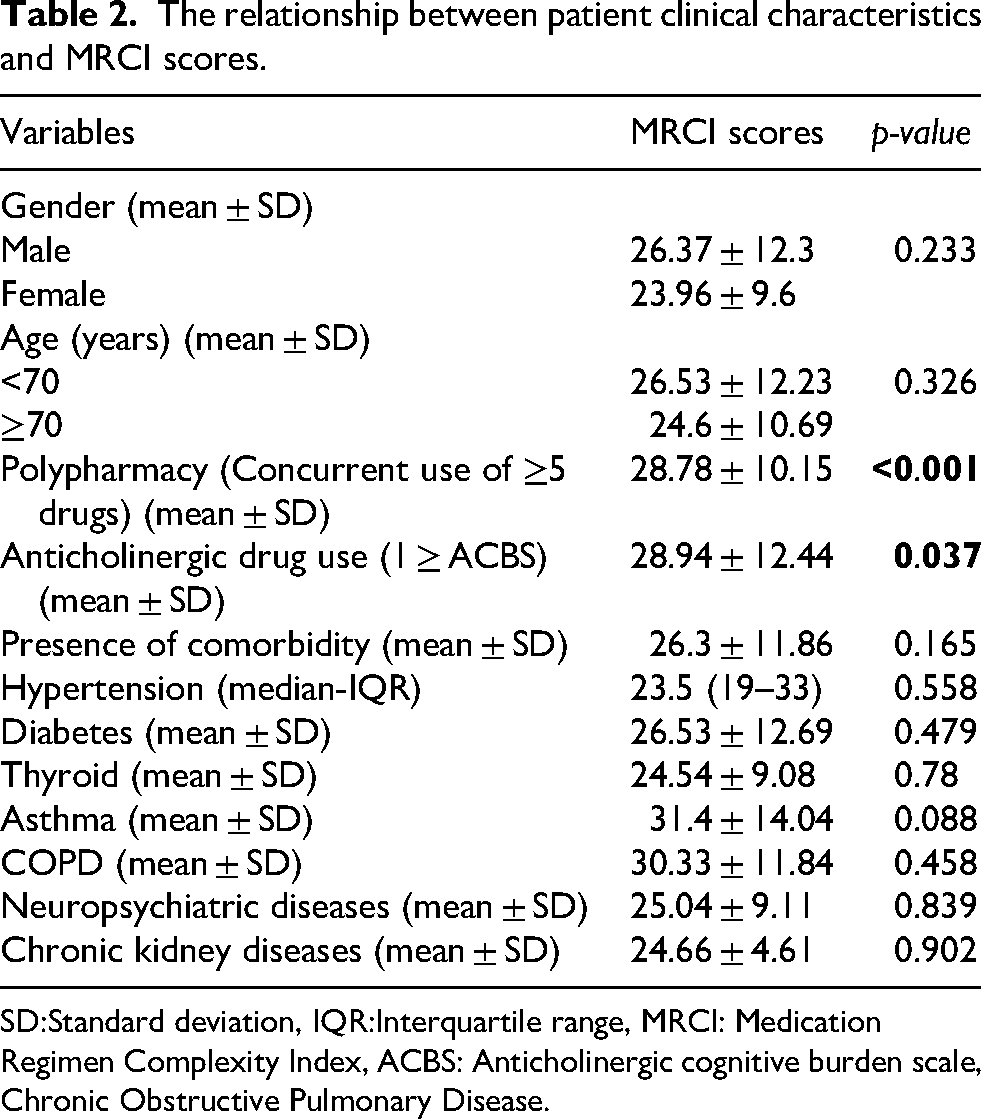
SD:Standard deviation, IQR:Interquartile range, MRCI: Medication Regimen Complexity Index, ACBS: Anticholinergic cognitive burden scale, Chronic Obstructive Pulmonary Disease.
MRCI scores were significantly higher in patients who were readmitted to the hospital within 30 days than in those who were not (p < 0.05) (Table 3).
Relationship between patient clinical characteristics and hospital readmission.
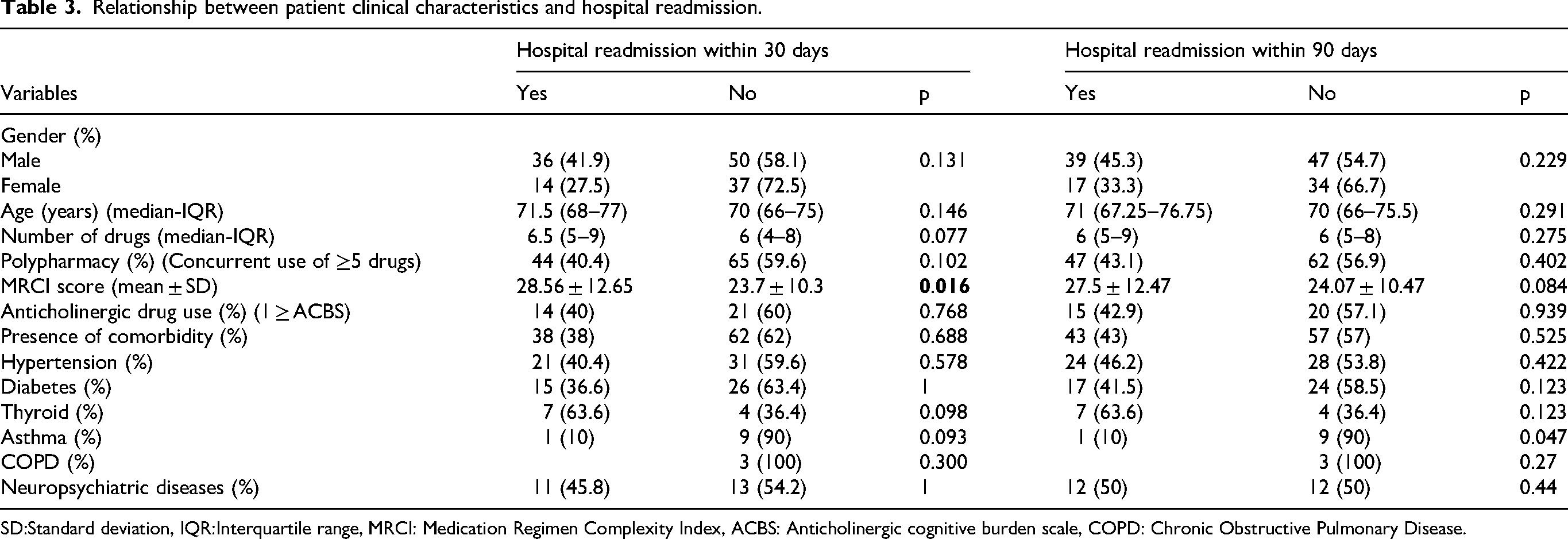
SD:Standard deviation, IQR:Interquartile range, MRCI: Medication Regimen Complexity Index, ACBS: Anticholinergic cognitive burden scale, COPD: Chronic Obstructive Pulmonary Disease.
A multiple linear regression model was developed to identify factors affecting MRCI scores. In univariate analyses, variables such as “hospital readmission within 30 days” and “use of anticholinergic drugs” which showed significant differences in MRCI scores, did not have a significant association with the MRCI score. However, a significant association was found with the total number of drugs (p < 0.001). As a result of the forward selection method, which identified only significant variables, both the total number of medications and the patient's age significantly affected the model. The total number of medications increased the MRCI score, whereas age significantly decreased the MRCI score (p < 0.05) (Table 4).
Factors affecting the MRCI score.
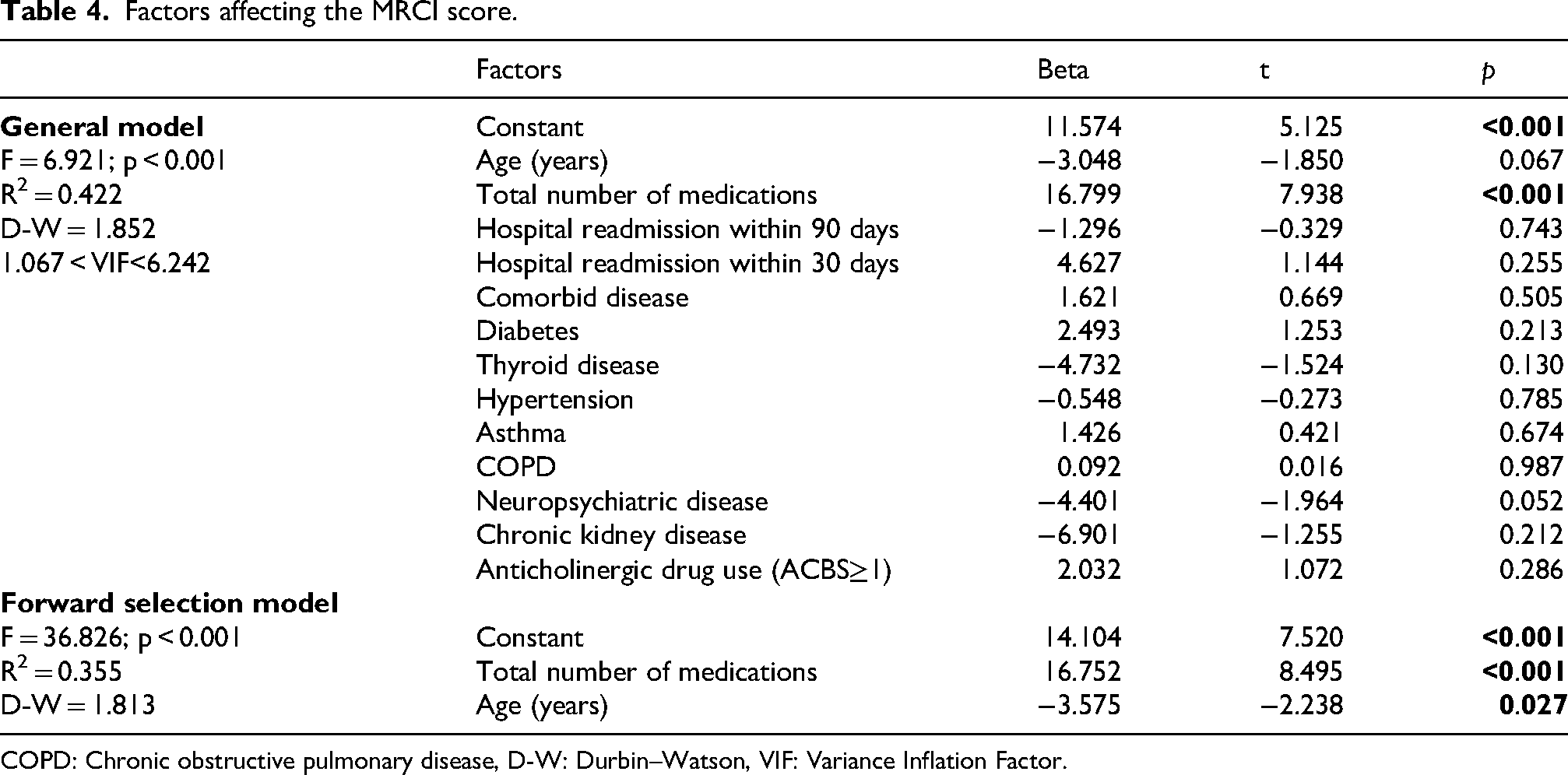
COPD: Chronic obstructive pulmonary disease, D-W: Durbin–Watson, VIF: Variance Inflation Factor.
A logistic regression model was constructed to identify factors associated with 30-day hospital readmission rates; however, none of the variables in the model were significant. In the forward stepwise model (multivariate model), only the MRCI score had a slightly positive effect (OR = 1.039, 95% CI = 1.006-1.072, p = 0.019) (Table 5).
Factors affecting hospital readmission.
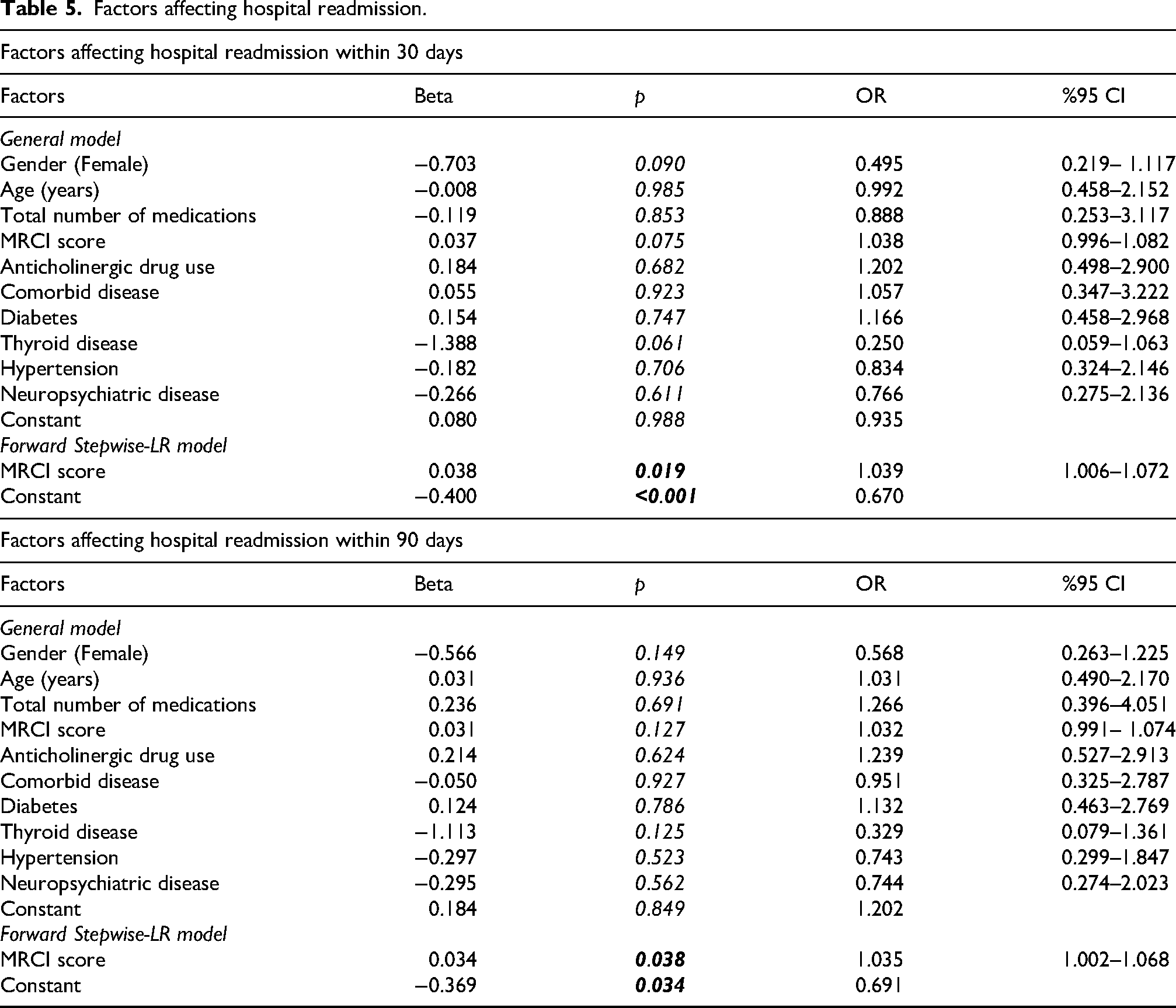
Among the factors significantly associated with 90-day hospital readmission rates, none showed a statistically significant association. However, in the forward stepwise model, only MRCI score has a significant effect (OR = 1.035, 95% CI = 1.002-1.068, p = 0.038). Although statistically significant, the odds ratios for MRCI were close to one, indicating a modest effect size. All models for 30 and 90-day hospital readmission had significant goodness-of-fit results (Table 5).
Discussion
This study evaluated the association between MRCI score and hospital readmission within 30 and 90 days, and examined MRCI risk factors. In this study, the median MRCI score was 24 (IQR, 17-31). In a study by Oliveira et al. of older cancer patients, the mean MRCI score was 27.39 ± 16.67. 16 In another study by Cifci et al., which included not only older patients but also adult cancer patients in general, the median MRCI score was 15 (IQR, 11-22). 21 One of the main reasons for the differences in these MRCI scores may be differences in study design. The MRCI score in Oliveira et al. 16 was similar to that of this study; medication complexity may have been reduced in Cifci et al.'s 21 study due to the involvement of a clinical pharmacist in the oncology service. There is no specific threshold for the MRCI scores. In a study of hemodialysis patients, 22 the mean MRCI value was 27.0 ± 10.9 points; 33.43 ± 15.47 in heart failure patients 11 ; and 27 (IQR, 20-35) in chronic kidney disease patients. 23 In studies conducted in pharmacies in Türkiye, the median MRCI score was 11 (IQR, 7–15) 24 and 12.5 (IQR, 7.0–19.6). 25 In a study conducted in primary care in Brazil, the median MRCI score was 12. 26 Studies conducted in pharmacies or primary care centers with older adults showed lower MRCI scores than those in hospitals. This may be due to hospitalized patients having multiple illnesses, taking more medications, and being frailer.
In this study, we found that the total number of medications was associated with higher MRCI scores, whereas advanced age was associated with lower MRCI scores. It was expected that the total number of medications or polypharmacy would increase the MRCI score. The relationship between age and MRCI is complex. Generally, as age increases, more medication use is expected. 27 However, in this study population, the medication burden may have been reduced in older patients and those with advanced cancer, and simpler treatments may have been preferred over more complex treatments to improve the patient's quality of life. According to a study conducted by Oliveira et al. on older patients with cancer, an increase in the MRCI score was significantly associated with polypharmacy, chronic diseases, and administration of high-risk medications. 16 Most studies found an association between MRCI score and polypharmacy or the total number of medications.25,26,28,29 However, most studies found no association between MRCI and sociodemographic variables such as age and gender.26,28–30
In this study, the MRCI score was associated with readmission to hospital within 30 and 90 days. Although statistically significant, the odds ratios for MRCI were close to 1, suggesting a modest effect size and warranting cautious interpretation. Cifci et al. found that, among adult cancer patients, those who were readmitted to the hospital within 30 days had a statistically significantly higher MRCI score. 21 Studies examining the relationship between MRCI scores and hospital readmissions have yielded varied results. 31 Several studies have examined the relationship between the MRCI score and readmission in patients with heart failure.11,32,33 Some of these studies found no association between MRCI score and hospital readmission,11,32 while others did. 33 Studies that found no association were retrospective and conducted with smaller patient populations,11,32 while the study that found an association was also retrospective but had a larger patient population. 33 Therefore, the association of MRCI can be observed in a larger population. A study of older adults with chronic kidney disease found no association between MRCI and hospital readmission. 12 However, a larger population-based study conducted exclusively in older patients found an association between MRCI and hospital readmission. 34 Differences between these studies may stem from variations in patient population size and characteristics, as well as differences in healthcare systems across countries.
Reducing medication complexity is crucial for preventing drug-related problems such as drug-drug interactions and adverse drug reactions in patients with cancer. 35 In patients with cancer, the deprescription of medications can be performed to reduce medication complexity. Drug deprescription is the systematic process of identifying and discontinuing medications when their harms outweigh their benefits, in the context of the patient's care goals, life expectancy, values, preferences, and purpose of the medication. 36 The National Comprehensive Cancer Network (NCCN) Older Adult Oncology guidelines recommend evaluating patients for potentially inappropriate medications and discontinuing those that are not needed. 37 In addition, to reduce medication complexity, longer-acting drugs can be selected by reducing the frequency of drug dosing, and fixed-dose combinations can be chosen. 12
Clinical pharmacists play a vital role in improving patient safety and treatment effectiveness by collaborating with a multidisciplinary team in oncology departments. Clinical pharmacists contribute to the identification and reduction of drug-related problems. 38 Examples of drug-related problems include unnecessary drug use, drug-drug interactions, drug incompatibilities, and underdosing or overdosing. 39 Numerous studies describe the role of clinical pharmacists in oncology departments.39–41 Clinical pharmacists can also contribute to medication management by reducing polypharmacy and medication complexity. 21 The use of MRCI in daily practice can be useful for predicting patients at risk. However, determining MRCI scores in routine clinical practice may not be straightforward. Therefore, simplifying and automating the MRCI application by integrating it into electronic health records would be beneficial, making it a practical, fast, applicable, and easy-to-use tool for managing drug therapy in a hospital setting. 16 Although studies on this subject exist, widespread integration into clinical information systems has not yet been achieved.42,43
Physician-clinical pharmacist collaboration in modifying medication regimens and educating patients about medications can help reduce medication complexity. As we showed in this study, lowering the MRCI score can reduce hospital readmissions. Poor patient adherence is a contributing factor to hospital readmission. 44 Patient adherence can also be improved through patient education. 21 Furthermore, clinical pharmacists can contribute to deprescribing and reducing medication complexity in older cancer patients by identifying potentially inappropriate medications (PIMs) use using various criteria (e.g., Beers, OncPal).37,45 In a study by McAdam et al., 45 they investigated the prevalence of PIMs among adult cancer patients receiving palliative care, the rate at which physicians implemented pharmacists’ recommendations for medication deprescribing, and the associated cost implications. In conclusion, the study highlights the benefits of pharmacist-led medication deprescribing among palliative care patients receiving inpatient treatment, demonstrating cost savings and a reduction in medication burden.
This study had some limitations. The retrospective, single-center design and limited sample size were the study's most significant limitations. Therefore, these results cannot be generalized. Due to the retrospective nature of the study, some sociodemographic characteristics of the patients, herbal product and OTC use, and medication adherence could not be evaluated. In this study, hospital readmission was defined as any readmission for any reason. Therefore, potentially medication-related readmissions could not be distinguished. Additionally, because the data were collected from a single hospital, transfers of patients to other hospitals within 30 and 90 days were not recorded.
Future studies should be multicenter, large-population, and prospective. By collecting more detailed patient adherence to medication and other clinical data, pre- and post-intervention studies and randomized controlled trials can be conducted to assess and reduce medication complexity.
Conclusion
This study found a significant association between the total number of medications and age, and the MRCI score. The MRCI score was associated with readmission to hospital within 30 and 90 days. Reducing medication complexity as part of medication management may reduce the risk of hospital readmission.
Footnotes
Acknowledgements
The authors would like to thank Assoc. Prof. Dr. Adnan Karaibrahimoğlu for his statistical analysis support.
Author contributions
AA conceived the study, AA and NY designed the study, AA analyzed data. AA and TY collected data and wrote the manuscript. All authors reviewed and approved the final version of the manuscript.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.