
Abstract
Introduction
This study evaluated the real-world effectiveness and safety of biosimilar trastuzumab-anns to the reference trastuzumab in a United States (U.S.) population.
Methods
This observational, multicenter, non-inferiority cohort study used electronic medical records from an integrated U.S. healthcare system. Eligible patients were HER2 + breast cancer patients treated with trastuzumab-anns (August 2019-December 2020) or trastuzumab (March 2017-July 2018). Patients were stratified by treatment setting (curative or palliative) and followed for up to 12 months, death, or end of membership, whichever occurred first. The effectiveness outcome was treatment failure, a composite of all-cause mortality or treatment change. The NI margin was set with an upper limit of 5% and multivariate Cox proportional hazards models were used. The safety was assessed by the incidence of cardiomyopathy and neutropenia. Sensitivity analysis was conducted using stabilized inverse probability of treatment weighting.
Results
Of the 4,111 patients eligible, 1,784 met the inclusion criteria with 893 patients in the trastuzumab-anns group and 891 in the reference trastuzumab group. For the composite of treatment failure, trastuzumab-anns was non-inferior to trastuzumab at 7.7% and 5.6%, respectively (90% CI: 0.0% to 4.0%; p < 0.01). A two-way analysis with Cox proportional hazard models showed no significant difference in the risk of treatment failure (adjusted hazards ratio 0.88, 95% CI: 0.6 to 1.3; p = 0.52). Rates of cardiomyopathy and neutropenia were comparable between groups.
Conclusion
In this real-world U.S. population, trastuzumab-anns was non-inferior to reference trastuzumab in the treatment of HER2 + breast cancer.
Introduction:
Approximately 20% of newly diagnosed breast cancer patients have tumors that overexpress the human epidermal growth factor receptor 2 (HER2). Since its Food and Drug Administration (FDA) approval in 1998, the HER2-targeted monoclonal antibody, trastuzumab, has improved clinical outcomes in both early-stage and metastatic HER2-positive (HER2+) breast cancer. Despite the changing landscape of HER2+ breast cancer with the approval of multiple novel HER2-targeted therapies, trastuzumab remains a cornerstone of treatment.1,2
In the United States (U.S.), trastuzumab has an estimated annual cost of $70,000. 2 Due to its widespread use, it has consistently ranked within the top 20 drugs for sales revenue, reaching a total of $2.46 billion in 2021. 3 As a result, trastuzumab has substantiall financial impact to U.S. healthcare systems and may also affect patients’ out-of-pocket costs. 1
Biosimilars have been approved based on data demonstrating they are highly similar to the FDA-approved reference product with no clinically meaningful differences.2,4–6 In 2019, trastuzumab-anns became the first trastuzumab biosimilar approved in the U.S. 1 The pivotal Phase III LILAC trial demonstrated non-inferiority (NI) of trastuzumab-anns compared to the reference product (RP) trastuzumab for the treatment of HER2 + early-stage breast cancer, supported by pharmacokinetic equivalence data.1,5,6 Similarly, other FDA-approved trastuzumab biosimilars (i.e., trastuzumab-dkst, trastuzumab-dttb, trastuzumab-pkrb, trastuzumab-qyyp, trastuzumab-strf) have their own respective Phase III clinical trials that demonstrate no clinically meaningful differences in treatment outcomes for HER2 + breast cancer compared to the RP trastuzumab. However, these studies, including LILAC, were primarily conducted outside of the U.S, and evidence for these biosimilars in the U.S. setting remains limited.7–13
Although biosimilars are generally associated with cost savings compared to the reference product, concerns about limited evidence may hinder adoption. For trastuzumab biosimilars, most of the real-world data focus on cost rather than safety and effectiveness. 14 Therefore, this study aims to evaluate the effectiveness and safety of trastuzumab-anns compared to RP trastuzumab in patients with HER2 + early or metastatic breast cancer in a non-inferiority study. Findings from this study will provide real-world evidence to support the clinical use of biosimilar trastuzumab-anns in the U.S.
Methods
Setting
Kaiser Permanente (KP) is a not-for-profit integrated healthcare system that serves over 12.6 million members across eight geographic regions in the U.S. This study was conducted using patient data from KP Northern California (KPNC) and KP Southern California (KPSC) regions, which serve over nine million members combined. Data was obtained through the electronic medical record (EMR) which allows access to diagnostic information, clinical encounters, and therapies received by patients. This study was reviewed and approved by the Institutional Review Board (IRB) in the KPNC and KPSC regions. Informed consent was waived due to the observational nature of the study.
Study design and population
This was an observational, multi-center, non-inferiority, cohort study comparing the effectiveness and safety of the biosimilar trastuzumab-anns to RP trastuzumab in patients diagnosed with HER2 + breast cancer within KPNC and KPSC. Data was extracted from the EMR. Patients were included if they were newly initiated on trastuzumab-anns or RP trastuzumab, aged ≥18 years, and had a diagnosis of HER2 + breast cancer within 24 months prior to the index date. Index date was defined as the first date of receiving trastuzumab-anns or RP trastuzumab. Patients were in the trastuzumab-anns group if they received the initial dose of trastuzumab-anns between August 1, 2019 through December 31, 2020, and patients were in the RP trastuzumab group if they received the initial dose of RP trastuzumab between March 1, 2017 through July 31, 2018. This cohort was followed for 12 months from index date, death, or end of membership, whichever occurred first. Patients were excluded if they did not have continuous health plan membership for 12 months prior to index date or received another trastuzumab biosimilar product or the antibody-drug conjugate (ADC) ado-trastuzumab emtansine (T-DM1) within six months prior to index date.
Patients were also stratified by treatment setting (curative or palliative) which was extrapolated from the EMR based on the diagnosis selected by the prescriber on the index date. Data regarding patient age, race, region, Charlson Comorbidity Index (CCI) which includes baseline congestive heart failure, treatment setting, and baseline treatment regimens were covariables that were collected for both groups. 15
Outcomes
There were two primary outcomes in this study: 1) effectiveness, assessed by the composite endpoint of treatment failure, and 2) safety, assessed by the incidence of cardiomyopathy and neutropenia.
Treatment failure. Treatment failure was defined as a composite endpoint composed of all-cause mortality or any treatment change in a patient's regimen due to any cause, including disease progression. 16 Treatment change was defined as the initiation or change to one of the following treatments during the follow-up period: capecitabine, eribulin, fam-trastuzumab deruxtecan (T-DXd), gemcitabine, lapatinib, margetuximab-cmkb, neratinib (for palliative setting only), olaparib (for palliative setting only), pembrolizumab, tucatinib, or vinorelbine, regardless of whether trastuzumab-anns or RP trastuzumab was continued.
Notably, T-DM1 was excluded from the list. Following the KATHERINE trial, adjuvant T-DM1 became the standard of care for patients with residual disease following neoadjuvant therapy, replacing the previous practice of continuing trastuzumab. Consequently, increased switches to T-DM1 during the trastuzumab-anns period were expected representing treatment optimization rather than failure. Therefore, excluding T-DM1 was done to minimize confounding related to the evolving treatment practice across the two time periods. 17
Safety. Safety outcomes were assessed as the incidence of hospitalization or emergency room visits with a primary diagnosis of cardiomyopathy or neutropenia, which are adverse events that have been associated with all trastuzumab products.6,18 Diagnoses were identified based on the International Classification of Diseases, Tenth Revision, Clinical Modification (cardiomyopathy ICD-10-CM I13.2, I41, I42.x, I43, I50.x, and R57; neutropenia, ICD-10-CM D70.3 D70.4, D70.8, and D70.9). This was assessed from index date up to 28 days after the last trastuzumab-anns or RP trastuzumab dose.
Treatment duration. Treatment duration was as an exploratory outcome. The average duration of therapy was assessed and measured the average time from index date to the date of last trastuzumab-anns or RP trastuzumab dose.
Statistical analysis
The approval of trastuzumab-anns was based on the pivotal LILAC trial, the randomized Phase III study in HER2 + early-stage breast cancer designed to demonstrate equivalence to the reference trastuzumab using pathologic complete response (pCR) as the primary endpoint. 5 In other words, the outcomes observed in LILAC served as the regulatory benchmark for trastuzumab-anns, the specific biosimilar evaluated for this retrospective review. Although real-world data exist with trastuzumab biosimilars, the available data specific to trastuzumab-anns focus primarily on biosimilar uptake and utilization patterns rather than clinical outcomes.14,19,20 Therefore, the regulatory benchmark pCR outcome from LILAC – not real-world estimates - was used as the basis for the sample size justification.
In LILAC, the observed pCR rate for patients receiving reference trastuzumab was 41%. 5 Based on these results, a sample size of 283 patients per group would be required to achieve 90% power at a one-sided alpha of 0.05 to meet a non-inferiority with an upper margin of 5%.
If non-inferiority was met, Cox proportional hazards models adjusted for age, race, baseline chemotherapy, CCI, history of congestive heart failure or chronic obstructive pulmonary disease (COPD), treatment setting, were used to determine any differences in treatment effect between trastuzumab-anns and RP trastuzumab for the composite outcome of treatment failure.
Descriptive statistics were performed to evaluate baseline characteristics and safety outcomes. This included Student's t-test for continuous variables and Chi-Square test for categorical variables. As a sensitivity analysis, stabilized inverse probability of treatment weighting (sITPW) would be used to balance the differences between the two groups. The weight would be applied and repeated on the analysis on both the effectiveness and safety outcomes. Results were considered statistically significant with p-values <0.05 for two-way analyses. The SAS statistical package (version 9.4) was utilized to perform all analyses (SAS Institute, Cary, NC).
Results
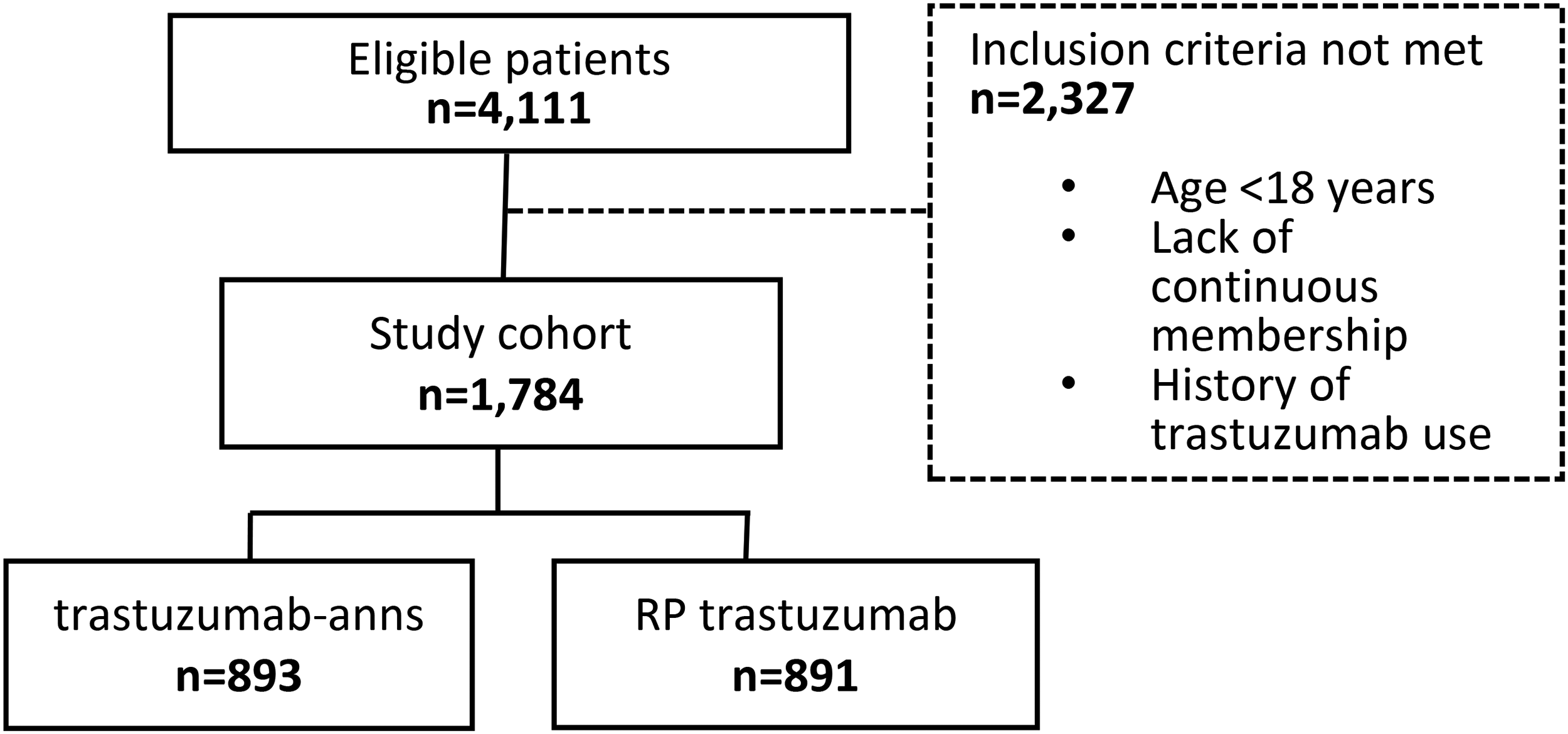
A total of 4,111 eligible patients were diagnosed with breast cancer and received trastuzumab-anns or RP trastuzumab during the cohort identification periods. There were 2,327 patients who did not meet the inclusion criteria either due to age <18 years on index date, lack of consecutive health plan membership 12 months prior to index date, or received prior treatment with a trastuzumab-based regimen within six months prior to index date. From the initial cohort of eligible patients, 1,784 met the inclusion criteria. Of these, 893 were in the trastuzumab-anns group, with 734 (82.2%) treated in the curative setting and 159 (17.8%) in the palliative setting. The remaining 891 were in the RP trastuzumab group, where 794 (89.1%) were treated in the curative setting and 97 (10.9%) were in the palliative setting (Figure 1, Table 1). In total, 1,528 patients were treated in the curative setting and 256 in the palliative setting.
Cohort identification.
Baseline characteristics.
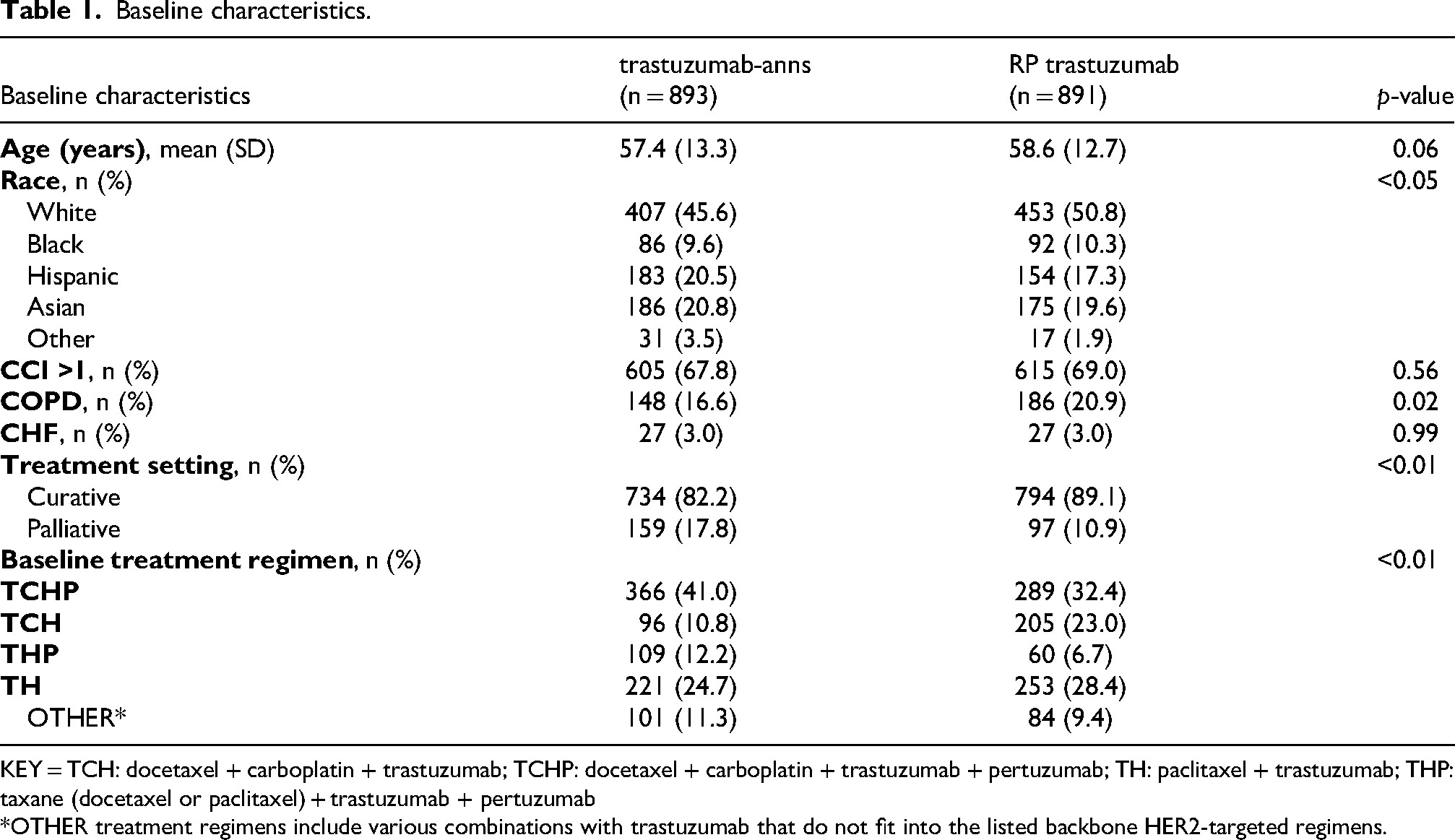
KEY = TCH: docetaxel + carboplatin + trastuzumab; TCHP: docetaxel + carboplatin + trastuzumab + pertuzumab; TH: paclitaxel + trastuzumab; THP: taxane (docetaxel or paclitaxel) + trastuzumab + pertuzumab
*OTHER treatment regimens include various combinations with trastuzumab that do not fit into the listed backbone HER2-targeted regimens.
There were no differences between the trastuzumab-anns and RP trastuzumab groups in terms of age (p = 0.06), comorbidities, defined as having a CCI score of greater than 1 (p = 0.56), and baseline CHF (p = 0.99) (Table 1). The mean age (years ± SD) of patients who received trastuzumab-anns and trastuzumab were 57.4 ± 13.3 and 58.6 ± 12.7 years old, respectively (p = 0.06).
However, there were significant differences in terms of race, COPD, treatment setting, and baseline treatment regimens between the trastuzumab-anns and RP trastuzumab groups. Fewer patients in the trastuzumab-anns group were White compared to the trastuzumab group (45.6% vs 50.8%). In addition, there were fewer patients in the trastuzumab-anns group that had COPD at baseline compared to the trastuzumab group (16.6% vs 20.9%, p = 0.02). More patients in the trastuzumab-anns group were in the palliative setting compared to the trastuzumab group (17.8% vs 10.9%, p < 0.01). Lastly, more patients in the trastuzumab-anns group were given pertuzumab compared to those who were given trastuzumab (p < 0.01) (Table 1). A sITPW was created to balance these differences between the two groups and used to analyze the outcomes.
Outcomes
Composite of treatment failure. Trastuzumab-anns was non-inferior compared to RP trastuzumab on the composite outcome of treatment failure in the total cohort. In the trastuzumab-anns group, 7.7% of patients reached this outcome compared to 5.6% in the RP trastuzumab group (absolute rate difference 2.12%, 90% confidence interval (CI) 0.00% to 4.06%; p < 0.01; sIPTW weighted rate difference −0.01%, 90% CI −1.96% to 1.94%, P < 0.01), falling within the 5% non-inferiority upper-margin and meeting the p-value for statistical significance (Table 2, Figure 2).
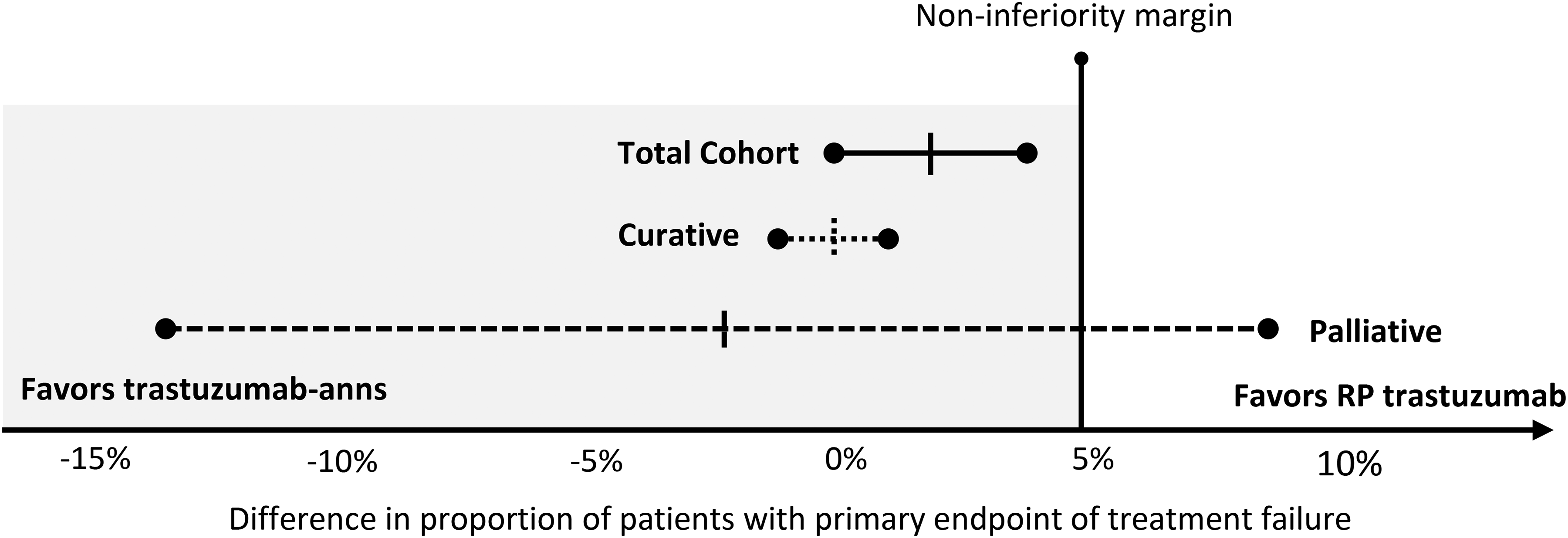
Non-inferiority of treatment failure in patients treated with trastuzumab-anns versus reference trastuzumab.
Treatment failure in the total cohort, curative setting, and palliative setting.
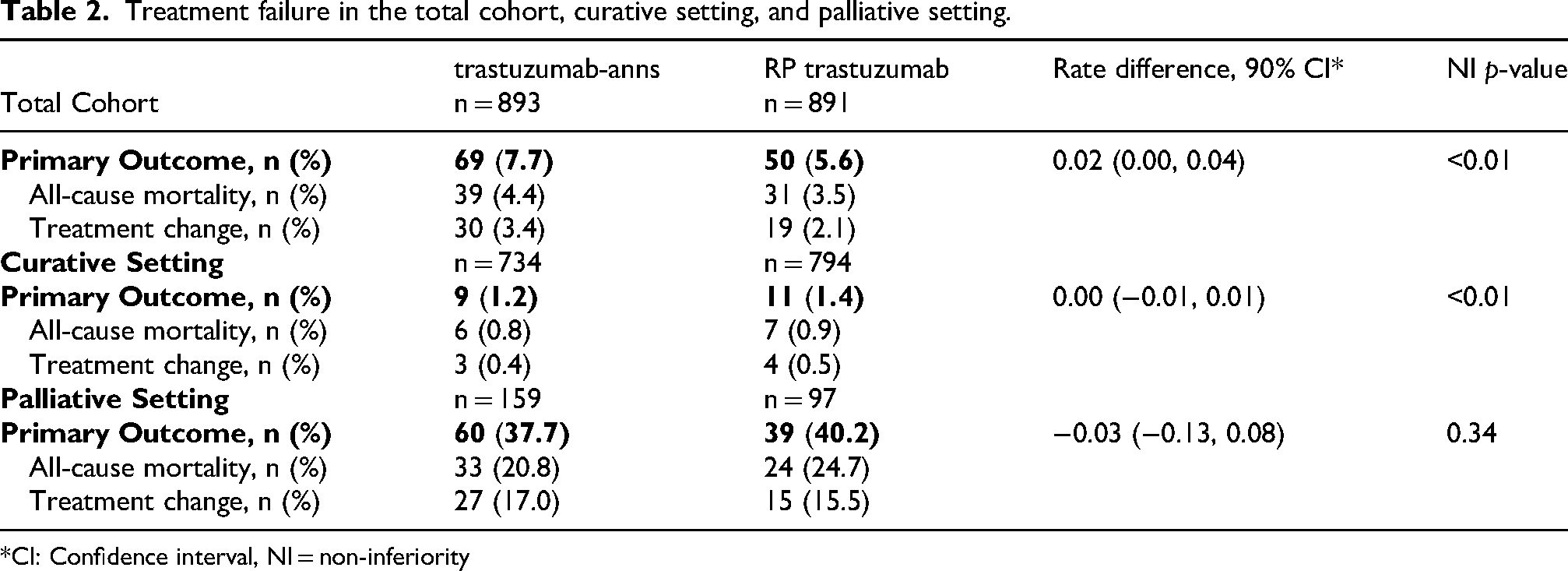
*CI: Confidence interval, NI = non-inferiority
In the curative setting, non-inferiority was also reached; 1.2% and 1.4% of patients in the trastuzumab-anns and RP trastuzumab groups, respectively, met the composite outcome of treatment failure (absolute rate difference 0.2%, 90% CI −1.0% to 1.0%; p < 0.01; sIPTW rate difference 0.01%, 90% CI −0.99% to 0.97%, p < 0.01). This is also within the 5% non-inferiority upper margin and met the p-value for statistical significance (Table 2, Figure 2). However, non-inferiority was not met in the palliative setting. There were 37.7% and 40.2% of patients in the trastuzumab-anns and RP trastuzumab groups, respectively, who met the composite outcome of treatment failure (rate difference −2.47%, 90% CI −12.82% to 7.88%; p = 0.34 sIPTW rate difference −5.51%, 90% CI −15.90% to 4.88%, p = 0.53) (Table 2, Figure 2).
In the two-way analyses with Cox proportional hazard models, there was no significant difference in the risk of treatment failure between patients treated with trastuzumab-anns and those treated with RP trastuzumab (adjusted hazards ratio (HR) 0.88, 95% CI 0.60 to 1.30; p = 0.52; sIPTW adjusted HR 0.86, 95% CI 0.59–1.26). This finding supports trastuzumab-anns was non-inferior to RP trastuzumab for the treatment of HER2+ breast cancer.
Two positive predictors of treatment failure included having a CCI score ≥ 1 (adjusted HR 4.74, 95% CI 1.44 to 15.67; p = 0.01; sIPTW adjusted HR 5.77, 95% CI 1.59–20.92 p < 0.01) and treatment in the palliative setting (adjusted HR 23.89, 95% CI 11.99 to 47.61; p < 0.01; sIPTW adjusted HR 21.73, 95% CI 11.05–42.71 p < 0.01), irrespective of the trastuzumab product used (Table 3).
Multivariate Cox proportional hazards model analysis on the outcome of treatment failure.
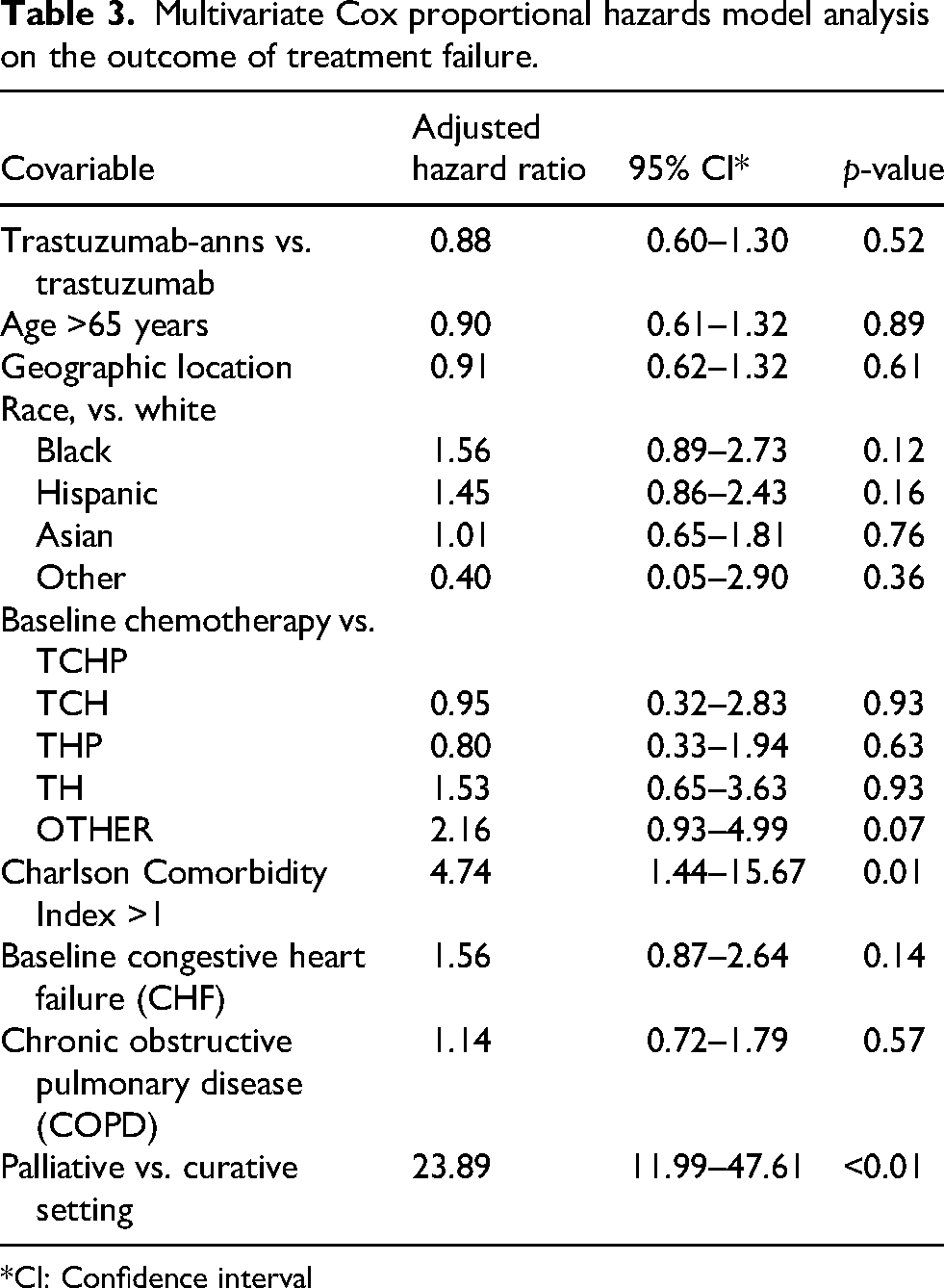
*CI: Confidence interval
Safety outcome. In the overall population, the safety outcomes between the trastuzumab-anns and RP trastuzumab groups were not significantly different. The incidence of cardiomyopathy was 1.3% vs 2.1% (p = 0.2; sIPTW p = 0.62), and the incidence of neutropenia was 2.9% vs 4.3% (p = 0.12; sIPTW p = 0.07), in the trastuzumab-anns and RP trastuzumab groups, respectively. (Figure 3).
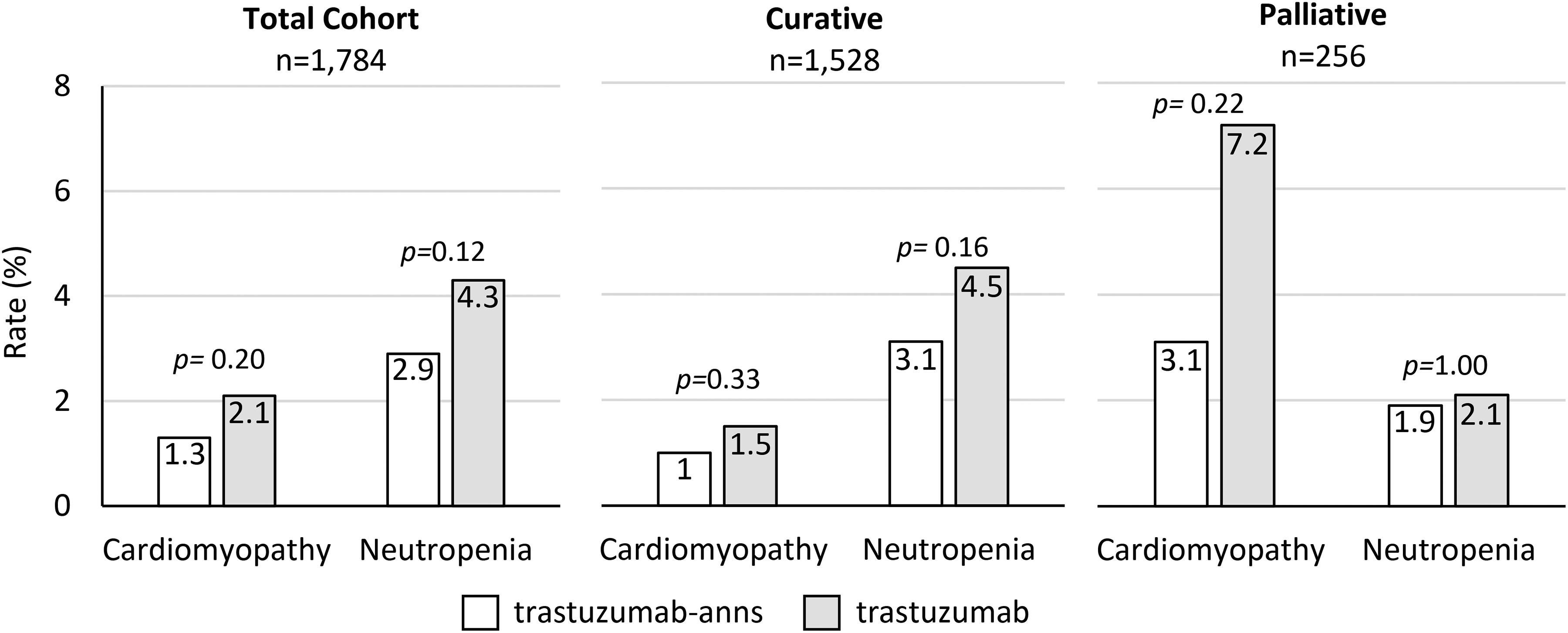
Incidence of cardiomyopathy and neutropenia in patients who received trastuzumab-anns and reference trastuzumab.
There was also no difference in safety outcomes when stratified by treatment setting. In the curative setting, the incidence of cardiomyopathy was 1.0% vs 1.5% (p = 0.33; sIPTW p = 0.66), and the incidence of neutropenia was 3.1% vs 4.5% (p = 0.16; sIPTW p = 0.08), in the trastuzumab-anns and RP trastuzumab groups, respectively. In the palliative setting, the rate of cardiomyopathy was 3.1% vs 7.2% (p = 0.22; sIPTW p = 0.46) and the rate of neutropenia was 1.9% vs 2.1% (p = 1.00; sIPTW p = 0.99), in the trastuzumab-anns and RP trastuzumab groups, respectively (Figure 3).
Moreover, all outcomes analysis were directionally consistent with or without sIPTW. This supports the robustness of our findings.
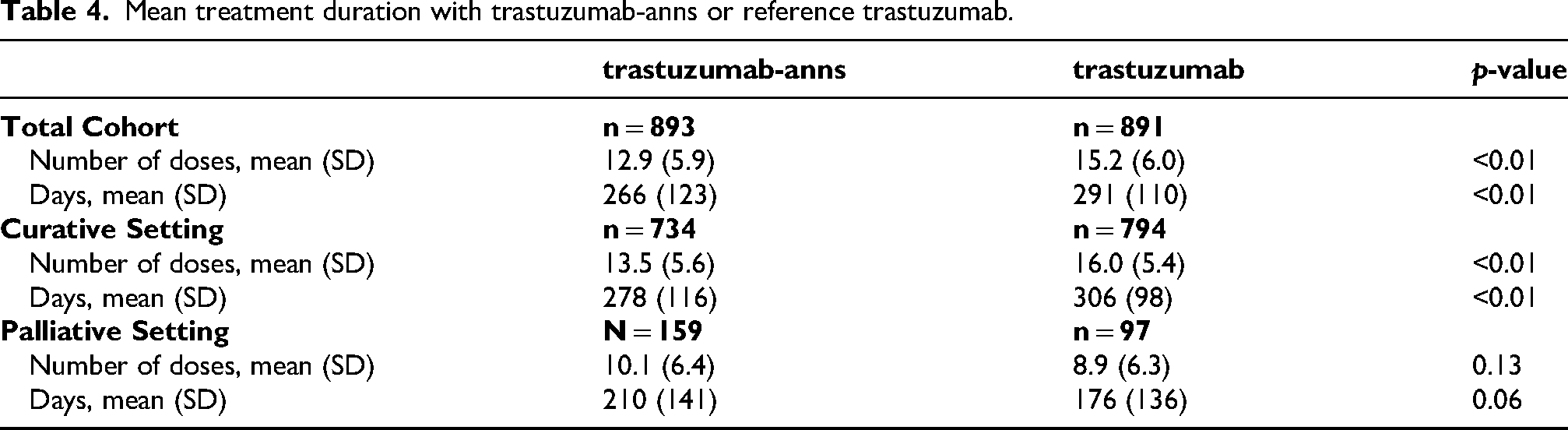
Treatment duration. The duration of treatment with trastuzumab-anns was significantly shorter than RP trastuzumab in the total cohort. Analysis of the total cohort showed that the average number of cycles (mean ± SD) was 12.9 ± 5.9 in the trastuzumab-anns group compared to 15.2 ± 6.0 in the RP trastuzumab group (p < 0.01).
The shorter treatment duration was also seen in the curative setting. Patients in the trastuzumab-anns group received an average of 13.5 ± 5.6 treatment cycles compared to 16.0 ± 5.4 in the trastuzumab group (p < 0.01). However, treatment duration was not significantly different between trastuzumab-anns and RP trastuzumab in the palliative setting with an average of 10.1 ± 6.4 vs 8.9 ± 6.3 cycles, respectively (p = 0.13) (Table 4).
Mean treatment duration with trastuzumab-anns or reference trastuzumab.
Discussion
In this retrospective, non-inferiority study, we evaluated the real-world effectiveness and safety of the biosimilar trastuzumab-anns to reference trastuzumab. Unlike other studies that have evaluated treatment outcomes of various trastuzumab biosimilars in either early or metastatic breast cancer, this study included both treatment settings and compared treatment duration between the two groups.5,8–13
Non-inferiority of trastuzumab-anns in terms of treatment failure was demonstrated for the overall population and curative setting. However, non-inferiority was not met in the palliative cohort. Although the palliative subgroup showed a lower rate of treatment failure in the trastuzumab-anns compared to reference trastuzumab, this finding should be interpreted with caution. Notably, the palliative cohort was substantially smaller than the curative cohort (256 versus 1528 patients) resulting in limited statistical power. Moreover, the wide confidence interval for the palliative cohort crossed both harm and benefit, indicating uncertainty. Therefore, these results do not support non-inferiority or equivalence in the palliative setting. The overall non-inferiority findings are likely driven by outcomes in the curative setting, and further studies are warranted to confirm non-inferiority in the palliative setting.
The safety outcomes were consistent with the known profile of trastuzumab products, which carry warnings for cardiomyopathy and exacerbation of chemotherapy-induced neutropenia. Incidences for both adverse events did not differ significantly between trastuzumab-anns and RP trastuzumab, supporting comparable safety profile.
To our knowledge, this is the first large-scale study in the U.S. evaluating non-inferiority of a biosimilar trastuzumab compared to the RP trastuzumab in HER2 + breast cancer patients in the curative and palliative setting. The study reflects the real-world practice in a large integrated health care system with a racially diverse population reflective of the U.S. Most trastuzumab biosimilars, including trastuzumab-anns, were studied primarily in Europe. Therefore, our study builds on the results from the LILAC trial, which supported the FDA approval of trastuzumab-anns as clinically equivalent to the reference product, by providing evidence in a U.S. population.
Limitations
The study has several limitations, notably those inherent to its retrospective design. For example, his affected our ability to determine the underlying reason for treatment changes. While progression due to treatment failure was one possibility, patients could have also been changed due to toxicity or treatment optimization to improve long-term outcomes. Although chart review could better inform the reason, the large sample size of our study made comprehensive review difficult to complete.
Another limitation was the inability to directly compare patients treated during the same period. Due to the rapid uptake of trastuzumab-anns within the institution, few patients received reference trastuzumab after biosimilar launch. As a result, we were unable to conduct a balanced parallel study and instead compared two different treatment periods in which trastuzumab-anns and RP trastuzumab were administered. This design introduces time-period bias, which is particularly relevant given the constantly evolving HER2+ breast cancer treatment landscape. Consequently, differences in treatment duration between cohorts are likely related to clinical practice factors rather than differences between the drugs themselves. Although trastuzumab has long been the cornerstone of treatment for HER2+ breast cancer, the treatment landscape evolved substantially between the two periods. For example, increased adoption of HER2-directed ADCs led to practice changes affecting sequencing and treatment duration. 21
As previously mentioned, adjuvant switches to T-DM1 following the KATHERINE trial reflected treatment optimization rather than treatment failure. 17 To minimize confounding, T-DM1 was excluded from our analysis. Another example was the shift from T-DM1 to T-DXd in the second-line setting. During the trastuzumab period, T-DM1 was considered the standard of care, but it had limited evidence of CNS penetration and was associated with increased risk of radiation necrosis.22–25 However, during the trastuzumab-anns period, emerging DESTINY-Breast03 data demonstrated superior efficacy of T-DXd compared with T-DM1 in the later-line setting, including patients with brain metastases.26,27 The positive efficacy signal from the study led to guideline changes recommending T-DXd, which has since become widely used across HER2+ breast cancer treatment.
Moreover, the trastuzumab-anns period also overlapped with the COVID-19 pandemic, when treatment schedules were disrupted by restrictions and efforts to reduce patient exposure. These modified schedules resulted in shorter observed treatment duration independent of drug-related performance. Taken together, these time-period factors indicate that the shorter treatment duration observed in the trastuzumab-anns cohort likely reflects contextual differences rather than any difference in effectiveness of the biosimilar.
The rapidly evolving HER2 + breast cancer treatment landscape also explains the greater use of pertuzumab in the trastuzumab-anns cohort, especially with evidence supporting its use in early-stage HER2 + breast cancer.28–30 Because addition of pertuzumab is associated with improved outcomes, the higher use of pertuzumab-containing regimens in the trastuzumab-anns cohort is a significant confounder when comparing the effectiveness between groups. To account for this imbalance, sensitivity analyses with Cox proportional hazards models were conducted to control for baseline characteristics with significant differences, including pertuzumab use, COPD, and race distribution. In addition, a sIPTW was performed to confirm the initial findings, and the results were consistent with the primary analysis.
Plus, the follow-up duration was relatively short since trastuzumab-anns has only been available since July 2019, limiting the ability to assess long-term outcomes such as overall survival. Further studies evaluating long-term effectiveness and safety are needed to confirm the findings of this study.
Other clinically relevant safety concerns associated with trastuzumab include infusion-related reactions, pulmonary toxicity, and immunogenicity. The data regarding these events were not collected for this study; however, future research evaluating these adverse events is warranted to provide a more comprehensive review of the safety profile.6,18
Conclusion
Biosimilars provide competition to biologics leading to cost savings to the reference product. However, there has been limited data with trastuzumab biosimilars in the U.S. population which could lead to their lower adoption as appropriate substitutes. In this study, trastuzumab-anns demonstrated non-inferior effectiveness and safety compared to RP trastuzumab for the treatment of HER2 + breast cancer in a large-scale, real-world setting. While longer follow-up and additional research are needed, these findings add to the evidence that trastuzumab biosimilars such as trastuzumab-anns should have similar outcomes to the RP trastuzumab product.
Footnotes
Acknowledgements:
We would like to acknowledge Anne Tran-Pugh, PharmD, FCSHP; Susan Lee, PharmD, BCPS; Laura Asakura, PharmD, BCOP, BCPS for their therapeutic expertise and guidance.
Ethics statement
The Kaiser Permanente Northern California and Sothern California institutional review boards approved this study (Study number #1804630 and #13035, respectively), and the need for informed consent was waived.
Author contributions
PS, FN, DDN, SLH, NS, LD, RLH designed the research, interpreted the analysis, and revised the manuscript; FN and RLH supervised data collection; DDN and RLH drafted the initial version of the manuscript; and PS, FN, DDN, SLH, NS, LD, RLH approved the version of the manuscript for submission. FN and RLH had full access to all the data in the study and takes responsibility for the integrity of the data and the accuracy of the data analysis.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Disclosures and prior presentations
This research received no specific grant from any funding agency in the public, commercial, or not-for-profit sectors. There were no prior peer-reviewed presentations at professional or scientific conferences. Parts of this study were presented in a non-reviewed poster session at the Academy of Managed Care Pharmacy Annual Meeting (March 29 – April 1, 2022; Chicago, Illinois) and as a non-reviewed presentation at Western States Conference (May 17, 2022; San Diego, California).