
Abstract
Introduction
The rising geriatric population has led to an increase in cancer diagnoses, with treatment decisions complicated by variable functional status and co-morbidities. This study compared chemotherapy dosing strategies, evaluated efficacy and safety, explored correlations with CRASH, CARG, G8, and CGA tools, and examined cancer incidence in older patients.
Methods
A hospital-based retro-prospective study was conducted at tertiary care cancer hospital over six months, with prior ethical approval. Patients aged ≥65 years with solid organ malignancies receiving chemotherapy were assessed using the Cancer and Aging Research Group (CARG), Chemotherapy Risk Assessment Scale for High Age Patients (CRASH), and Geriatric-8 (G8) tools. Those failing G8 underwent Comprehensive Geriatric Assessment (CGA). Statistical analysis was performed using the Kruskal–Wallis test.
Results
A total of 154 patients were enrolled (88 males, 57.1%; 66 females, 42.9%). Of these, 71 (46.1%) received standard doses, while 83 (53.9%) received reduced doses during the first cycle. Among 109 patients failing G8, CGA was conducted. Adverse effects—including weakness, nausea, and ulcers occurred in 78 patients (71.6%). Depression correlated significantly with CARG (p=0.02). CRASH and CARG showed no direct correlation (p=0.433); however, ADRs were significantly associated with CRASH (p=0.01), while dosage adjustments correlated with CARG (p=0.04).
Conclusion
Cancer care in geriatric patients requires individualised dosing guided by structured screening and geriatric assessment tools. Integrating CARG, CRASH, G8, and CGA into treatment planning enhances safety and efficacy by balancing therapeutic benefits with toxicity risks.
Keywords
Introduction
The global rise in the elderly population has placed geriatric oncology at the forefront of cancer care. Cancer is the leading cause of death among individuals aged ≥ 65 years, accounting for more than half of all new diagnoses. 1 Age-related physiological changes, Comorbidities and altered pharmacokinetics make chemotherapy in older adults challenging.2,3 To address these complexities, several predictive tools have been developed to estimate chemotherapy-related toxicity and support clinical decision-making. Among them, the Cancer and Ageing Research Group (CARG) Toxicity Score and the Chemotherapy Risk Assessment Scale for High-Age Patients (CRASH) are widely used to individualise treatment plans.4–7 In addition, geriatric-specific screening methods, such as the Comprehensive Geriatric Assessment (CGA) and Geriatric-8 (G-8) screening tool, help identify patients at higher risk of poor chemotherapy tolerance. However, chemotherapy dose modification lacks universal guidelines, making individualised decisions essential.8–10 Treatment decisions must therefore integrate tumour type, disease stage, and physiological resilience rather than chronological age alone. Moreover, sex-based differences in cancer incidence and treatment outcomes further emphasise the need for personalised, evidence-based approaches.11,12 As the elderly cancer population continues to expand, early risk assessment and individualised chemotherapy are essential for guiding clinical decision-making. Hence, this study aimed to assess chemotherapy dose modification patterns and associated toxicity in older adult cancer patients to guide the development of safer, tailored therapeutic strategies.
Materials and methods
Study design
This retro-prospective study, conducted in a tertiary care hospital from June to November 2024, for a period of six months, followed a comprehensive approach to evaluate chemotherapy-related outcomes in elderly cancer patients. This study utilised advanced tools such as the CARG, CRASH, and G-8 screening tools and CGA, supported by MD+ CALC software. Patient interviews after the first chemotherapy cycle provided critical insights into their treatment experience and overall health status.
Study population
The study included geriatric oncology patients (≥65years) with solid organ malignancies treated at a tertiary care cancer hospital in Bangalore. Patients who received at least one chemotherapy cycle with adjunctive drugs were assessed through interviews and case file reviews, documenting their demographics, medical history, comorbidities, cancer stage, laboratory investigations, and chemotherapy regimens. Patients with incomplete clinical records were excluded.
Study objectives and data collection
This study aimed to identify predictive markers of chemotherapy toxicity and guide personalised treatment strategies in elderly oncology patients. We collected comprehensive patient data from case files, including demographics, presenting complaints, past medical and medication history, comorbidities and their duration, cancer stage, laboratory investigations, prescribed medications and chemotherapy regimens were extracted retrospectively from the medical records. G8 screening, CGA components (ADL, IADL, Mini Nutritional Assessment, and Geriatric Depression Scale), and patient-reported chemotherapy-related adverse effects after the first cycle were assessed prospectively through direct patient interviews, and CARG and CRASH scores were calculated using these data. However, severity grading was not performed in this study. The tools incorporate metrics such as functional status (ADL and IADL), cognitive and psychological health, nutritional assessment, and laboratory parameters such as creatinine clearance, guiding personalised treatment decisions.
Data analysis and risk assessment
Data were entered into Microsoft Excel and analysed using IBM SPSS Statistics for Windows, version 25.0. Categorical variables were summarised as frequencies and percentages. Associations between the risk stratification tools (CARG and CRASH scores) and CGA domains, chemotherapy dose, and adverse drug reactions were evaluated using the Kruskal–Wallis test, as appropriate. A two-tailed p-value < 0.05 was considered statistically significant.
Ethical considerations
This study adhered to strict ethical guidelines, beginning with the approval of the Institutional Ethics Committee (EC/47/24/06). The waiver of consent was considered in the study, and no written informed consent was obtained from any of the individual participants included in the study. Confidentiality was maintained throughout data collection and analysis in accordance with the ethical standards for geriatric oncology research.
Results
Patient characteristics
Based on the G-8 screening tool, 109 of 154 patients (70.8%) had a score <14 and underwent CGA (Table 1), while 45 patients (29.2%) had a score ≥14 and did not require further geriatric assessment (Table 2). As shown in Table 1, among patients who underwent CGA (n = 109), most were aged 65–70 years (58.7%), followed by 71–75 years (30.3%), while only 11.0% were older than 75 years. A similar age distribution was observed in the non-CGA group, where 62.2% were aged 65–70 years and 28.9% were 71–75 years. Male predominance was noted in the CGA group (61.5%), whereas females were more common in the non-CGA group (53.3%). The majority of patients had at least one comorbidity in both groups (CGA: 72.4%; non-CGA: 77.7%), while 27.5% and 22.2%, respectively, had no comorbid illness.
General patient characteristics.
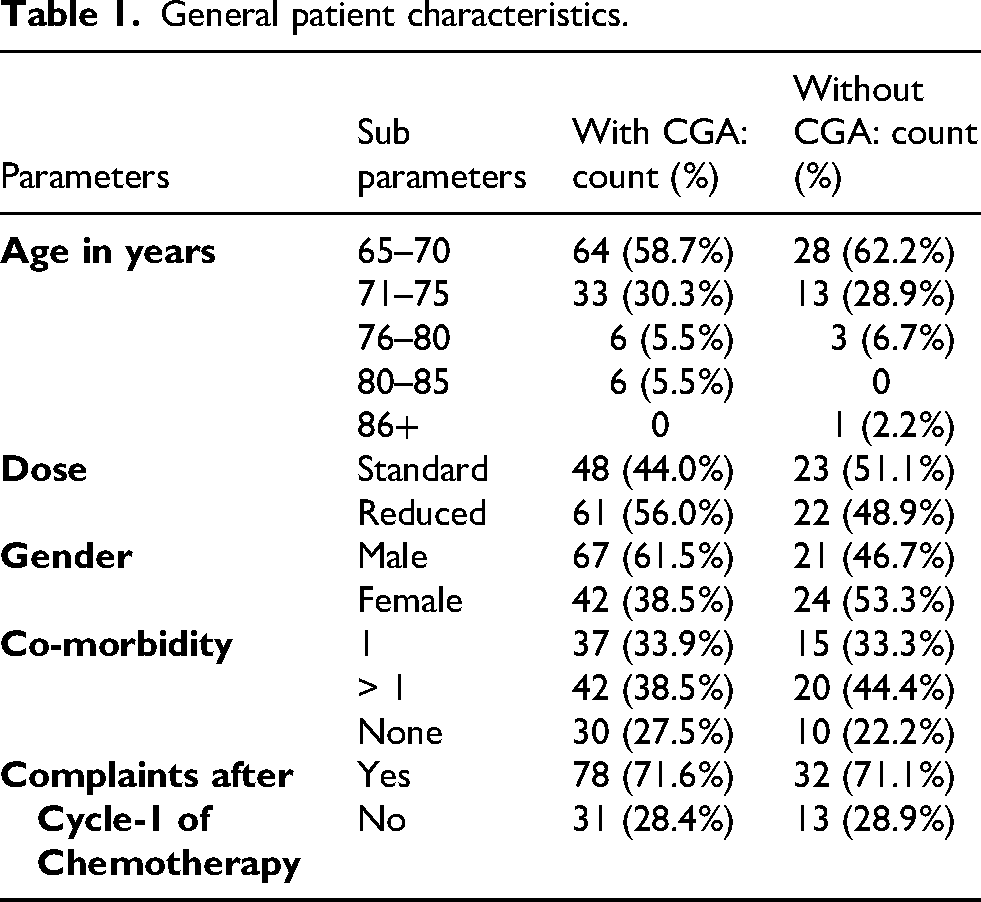
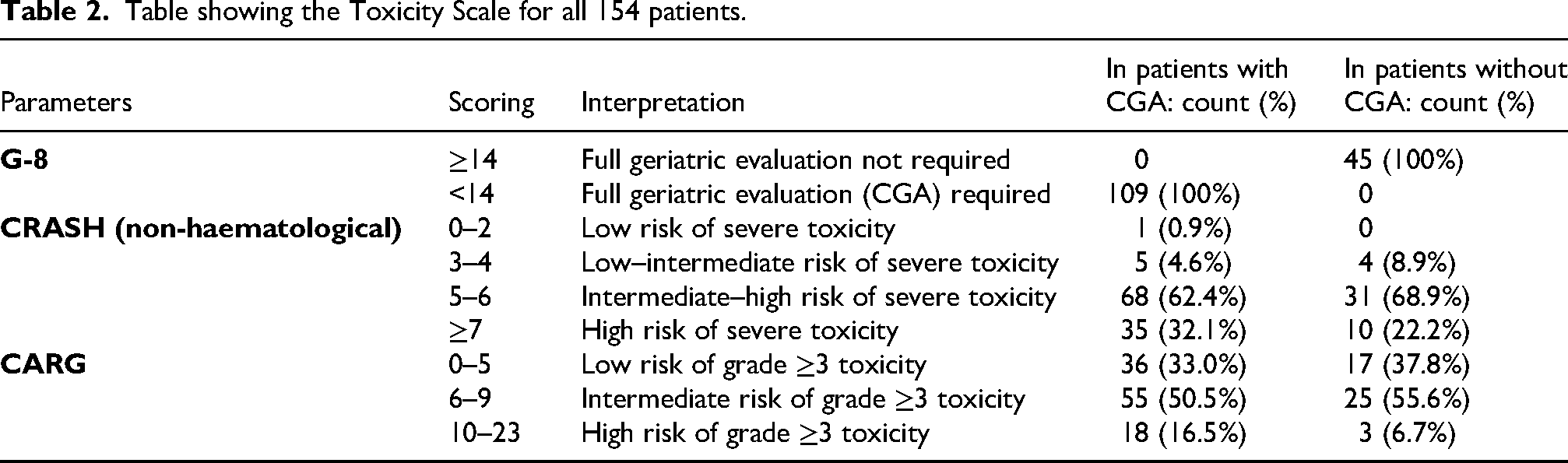
Table showing the Toxicity Scale for all 154 patients.
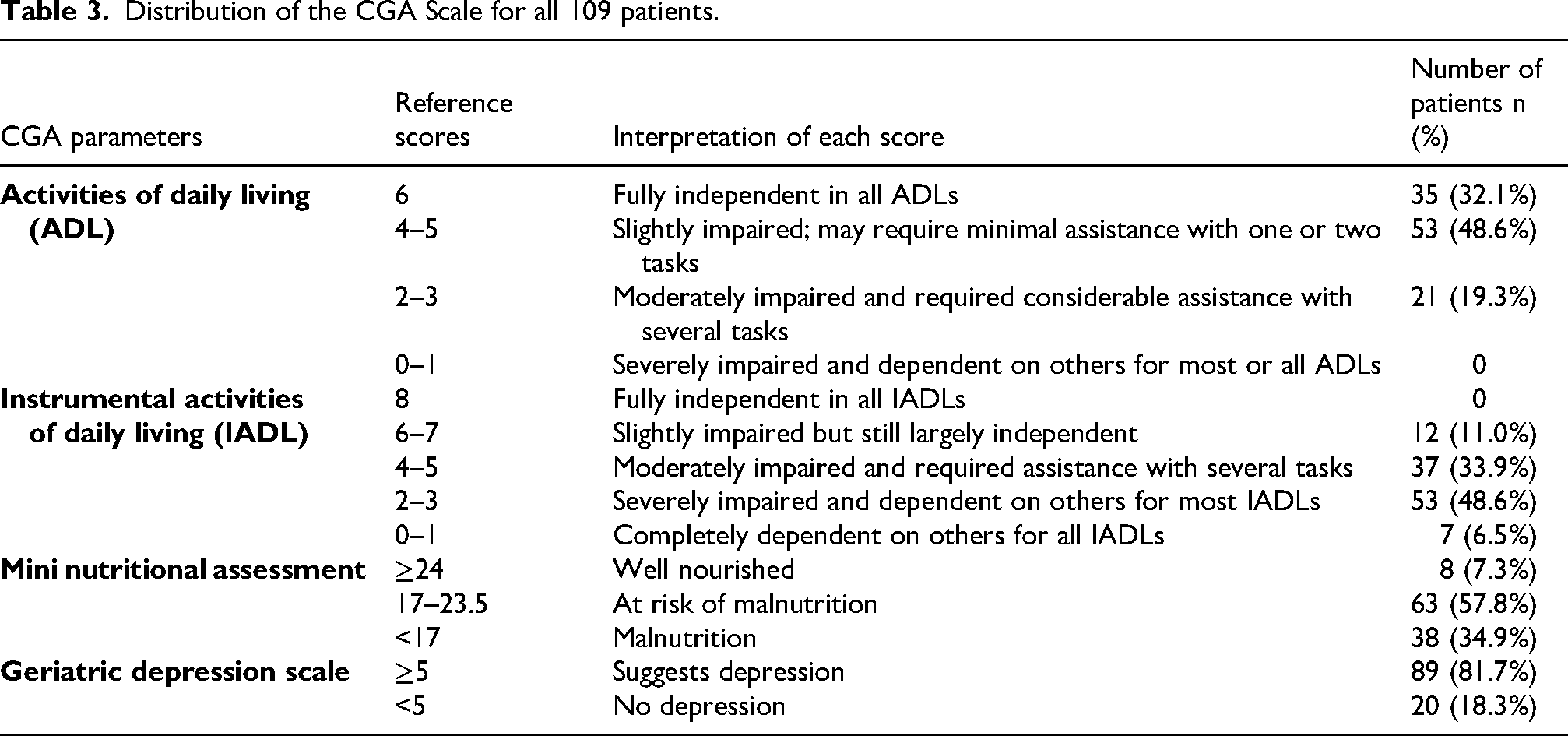
Dose reduction was more frequent in the CGA group (56.0%), whereas standard dosing was slightly more common in the non-CGA group (51.1%). Chemotherapy-related complaints after the first cycle were reported in a comparable proportion of patients in both groups (CGA: 71.6%; non-CGA: 71.1%) (Table 1). Among those who underwent CGA, 48.6% had mild impairment in ADL, and 19.3% had moderate impairment, while 32.1% were fully independent. All patients had some degree of IADL impairment, with 48.6% severely impaired and 6.5% completely dependent. Nutritional assessment revealed that only 7.3% were well nourished, whereas 57.8% were at risk of malnutrition and 34.9% were malnourished. Depression was present in 81.7% of patients (Table 3).
Distribution of the CGA Scale for all 109 patients.
Chemotherapy-related adverse events
As shown in Table 2, all 109 patients who underwent CGA had a G-8 score <14, whereas all 45 patients in the non-CGA group had a score ≥14. CRASH (non-haematological) scoring demonstrated that the majority of patients in both groups were categorised as intermediate–high risk for severe toxicity (CGA: 62.4%; non-CGA: 68.9%). A large proportion also belonged to the high-risk group, which was more frequent among patients who underwent CGA (32.1%) compared to those who did not (22.2%). Only a few were in the low-intermediate risk categories (CGA: 4.6%; non-CGA: 8.9%), and just one patient was classified as low risk.
Similarly, CARG risk stratification showed that over half of the patients were in the intermediate-risk category (CGA: 50.5%; non-CGA: 55.6%). Low-risk patients constituted 33.0% in the CGA group and 37.8% in the non-CGA group. The proportion of high-risk patients was more than twice as high among those who underwent CGA (16.5%) compared to the non-CGA group (6.7%). Overall, adverse drug reactions after the first chemotherapy cycle were reported in 110 patients.
Association between parameters
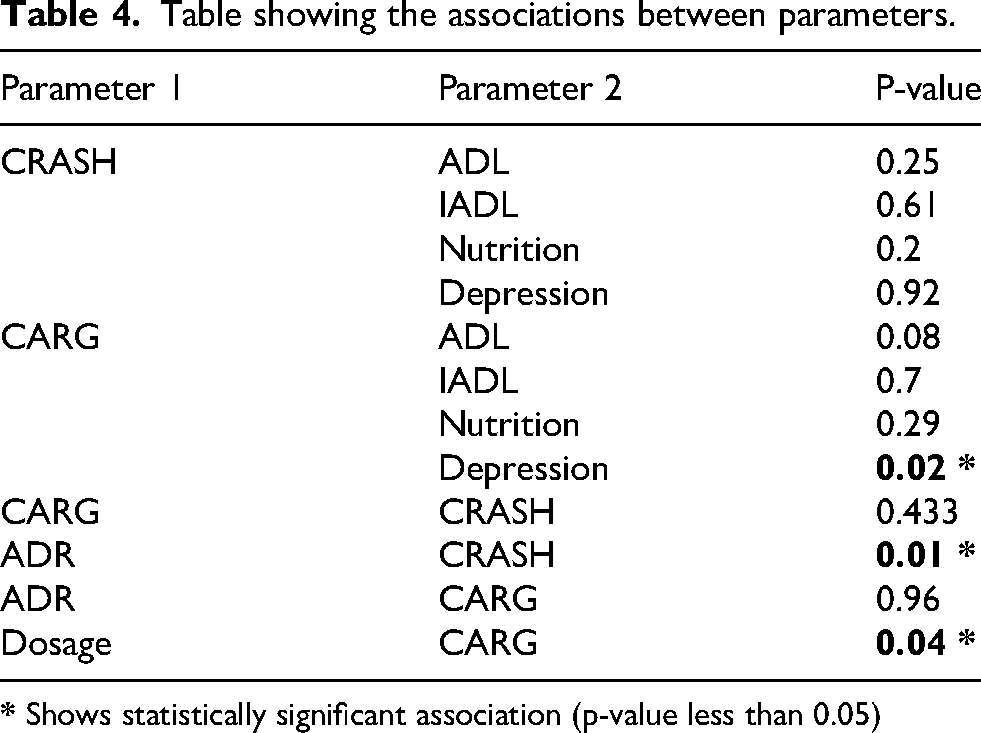
The association between CRASH, CARG and CGA scores was analyzed, and a p-value < 0.05 was considered statistically significant. As shown in Table 4, the CRASH score did not show significant associations with ADL (p = 0.25), IADL (p = 0.61), nutritional status (p = 0.20), or depression (p = 0.92). Similarly, the CARG score was not significantly associated with ADL (p = 0.08), IADL (p = 0.70), or nutritional status (p = 0.29). However, a significant association was observed between CARG score and depression (p = 0.02). ADR occurrence was significantly associated with CRASH score (p = 0.01) but not with CARG score (p = 0.96). No significant correlation was found between CRASH and CARG scores (p = 0.433).
Table showing the associations between parameters.
Relationship between CRASH, CARG risk score, and dose reduction or delay during treatment
Dose modification showed a significant association with CARG risk stratification (p = 0.04), indicating that patients with higher CARG scores were more likely to undergo dose reduction or delay. In contrast, the CRASH score did not demonstrate a significant relationship with dose modification. Although ADRs were significantly associated with CRASH score (p = 0.01), no association was observed with CARG score (Table 4).
Overall, the CARG score is key in predicting dose modifications related to toxicity, while the CRASH score reliably identifies patients at risk for non-haematological adverse drug reactions. Integrating the CGA with the CARG and CRASH scores enhances clinical decision-making, reduces treatment-related toxicities, and optimises outcomes for older adults with cancer. Additionally, addressing holistic factors, such as malnutrition, depression, and functional impairments is essential for improving the quality of life in this vulnerable patient population, ensuring a more comprehensive and personalised approach to care.
Discussion
The growing incidence of cancer in the geriatric population introduces significant complexities in treatment, particularly in determining the appropriate chemotherapy dose and managing the potential side effects. This study aimed to explore different chemotherapy dosing strategies, assess geriatric screening tools (CARG, CRASH, and G8), and analyse their relationship with treatment outcomes in older patients with cancer. These findings provide important insights into the multifaceted nature of cancer care in this demographic group.
This study explored the unique challenges of managing cancer in the geriatric population, emphasising the role of CGA and tailored treatment plans. As the geriatric population grows, addressing the complexities of cancer management in older adults is becoming increasingly critical for improving patient outcomes. The findings from this study, conducted on older adult patients at a cancer centre, identified several key findings, including the prevalence of specific cancers, the impact of chemotherapy, the role of toxicity prediction tools, and the importance of addressing functional and psychosocial needs.
This study assessed 154 patients aged > 65 years with solid organ malignancies who received chemotherapy. Male patients were more predominant than females, accounting for 88 (57.15%) vs. 66 (42.85%). Our findings revealed that lung cancer was the most common malignancy among male patients 22(25%), whereas breast cancer 15 (22.72%) was predominant among females. These results align with national and global trends, as observed by Jackson et al., who noted a higher incidence of certain cancers among specific sexes due to biological, behavioural, and environmental factors. 11 This sex disparity suggests that cancer prevention strategies and screening programmes must be tailored accordingly. For example, targeted efforts such as early oral cancer screening in men, as emphasised by Jivarajani et al., and routine breast and cervical cancer screening for women could potentially enhance early detection and improve survival rates. 13
Managing chemotherapy in older adult cancer patients remains challenging, as treatment-related toxicities frequently complicate outcomes and limit therapeutic options. In our study, 53.9% of patients required dose reductions, highlighting the necessity of individualised chemotherapy dosing for geriatric patients. This is consistent with previous studies, as demonstrated by Hwang et al., where age-related physiological changes, comorbidities, and polypharmacy increase the likelihood of adverse drug reactions. 8 In their study, approximately 59.8% of the patients received upfront dose reduction (UDR), and found that Grade 3–5 adverse events occurred more frequently in patients receiving standard doses than in those receiving UDR, with incidence rates of 63.9% and 48.6%, respectively. Our findings highlight the need for a cautious approach to chemotherapy dosing in older patients, ensuring that the treatment efficacy is balanced against the risk of toxicity. The use of multi-drug chemotherapy regimens in 80.52% of patients further illustrates the complexity of the treatment in this population.
While aggressive chemotherapy may offer the potential for improved survival, it also increases the risk of severe side effects, particularly in patients with diminished physiological reserves. More than 70% of the patients in this study reported side effects, including generalised weakness, nausea, mouth ulcers, and gastrointestinal issues. This high incidence of treatment-related complications is consistent with the findings of Nguyen et al. They observed significant chemotherapy-induced toxicities in a similar cohort of elderly cancer patients, where severe (i.e., grade ≥ 3) haematological (38.6%) and gastrointestinal (12.9%) toxicities were common. 14 These findings highlight the critical importance of supportive care strategies, including nutritional support, psychological counselling, and symptom management, to mitigate the impact of these toxicities.
The tools used in our study (CARG, CRASH, and G-8) may help stratify patients based on their risk of chemotherapy-related toxicities and guide treatment decisions in the future. The findings of our study indicate that these tools may help identify older adult patients with cancer at a higher risk of treatment-related toxicities. Among the study participants, 109(70.78%) scored below 14 on the G8 screening tool, indicating the need for CGA. This finding is significant as it underscores the utility of the G-8 in quickly identifying patients at high risk of functional decline or severe toxicities, as supported by the work of Velghe et al. 15 They demonstrated the effectiveness of the G-8 in predicting outcomes in elderly patients with haematological malignancies. They further reported that 76% (38 out of 50 patients) of patients failed the G8 screening tool, scoring < 14. Another study conducted by Garcia et al. and Shah et al. also showed the effectiveness of the G-8 tool.16,17 The use of the G-8 allows for the early identification of patients who may require more intensive supportive care or modifications to their treatment plans.
The CRASH score, which assesses the risk of severe chemotherapy-related toxicity, revealed that 99 (64.28%) patients were classified as intermediate-to-high risk, with 45 (29.23%) patients categorised as high risk. Similarly, a study conducted by Mittal et al. reported consistent findings, showing that 7(7%) patients were classified as low-to intermediate-risk, 43(43%) as intermediate-to-high risk, and 50(50%) as high-risk, with a total of 100 patients. 18 They also reported that higher CRASH scores were associated with a greater likelihood of severe adverse events, including unplanned hospitalisations and emergency visits, which is also similar to the study conducted by Dhir et al. 19 This suggests a possible role of the CRASH score in risk stratification of patients and guiding the intensity of their treatment.
The CARG score, another tool used to assess chemotherapy toxicity risk and its ability to predict chemotherapy-related toxicities, has been well-established. Studies by Ostwal et al. and Kotzerke et al. support its superiority over traditional performance status scales such as the Karnofsky Performance Status (KPS).20,21 Compared to those studies, where CARG stratified patients into low (15 patients, 14%), medium (61 patients, 59%), and high-risk (27 patients, 26%) groups, our study showed a different distribution with low (53 patients, 34.42%), medium (80 patients, 51.95%), and high-risk (21 patients, 13.63%) groups, respectively. The effectiveness of the CARG score in identifying high-risk patients underscores its importance in geriatric oncology, particularly in guiding treatment modifications and supportive care planning. However, as noted by Frelaut et al., the CRASH and CARG tools may not always perform consistently across different patient populations, suggesting that further validation of these tools in diverse clinical settings is necessary. 22 Formal CTCAE-based grading of toxicities was not performed, which limits direct comparison with studies reporting grade 3–5 toxicities. However, the use of patient-reported adverse effects allowed for a real-world assessment of treatment tolerance in this geriatric population.
Conclusion
This study demonstrated that higher CARG scores were associated with chemotherapy dose modification, whereas higher CRASH scores were associated with the occurrence of chemotherapy-related adverse effects. The G8 screening tool identified a large proportion of patients requiring a CGA. These findings support the role of structured geriatric assessment in risk stratification and individualised chemotherapy decision-making. Prospective studies with longitudinal outcome measures are required to determine their impacts on survival, treatment tolerance, and quality of life.
A weak but statistically significant association was found between depression and the CARG score (p=0.02), whereas no relationship was observed between the CRASH and CARG scores (p=0.433). ADRs were strongly associated with the CRASH score (p=0.01). Hypertension (48.7%) and diabetes (37.01%) were the most prevalent comorbidities that significantly influenced treatment tolerance. These findings highlight the importance of incorporating the CRASH score and ADR assessments into the treatment protocol for geriatric patients, which can facilitate risk stratification and support personalised chemotherapy dosing in geriatric oncology patients. However, its impact on treatment outcomes requires confirmation in prospective studies with longitudinal follow-up and personalised regimens to align with individual risk profiles and comorbidities.
A tailored approach to geriatric oncology not only prioritises patient safety but also paves the way for more effective and compassionate cancer care, recognising the unique needs of an aging population.
Limitations
The absence of CTCAE-based toxicity grading limits the standardisation and comparability of toxicity outcomes. Important treatment-related confounders such as cancer stage, intent of chemotherapy, line of therapy, and regimen intensity were not included in the analytical model, which may have influenced the observed associations
Footnotes
Acknowledgments
The authors wish to thank the clinical staff and patients of HCG Cancer Centre for their cooperation and support during the course of this study.
Authors contributions
PRS - Conceptualization, Validation , Investigation, Writing - Original Draft, Visualization. HBV - Conceptualization, Validation, Investigation, Writing - Original Draft, Visualization. SS - Validation, Verification, Writing - Review & Editing. SRRH - Validation, Verification, Writing - Review & Editing. PT - Methodology, Formal analysis, Project administration, Supervision, Validation, Writing - Review & Editing, Software. SCT - Methodology, Formal analysis, Project administration, Supervision, Validation, Writing - Review & Editing, Software. GBK - Supervision. Shekar Patil - Supervision. NU - Resources. Spoorti G - Resources.
ORCID iDs
Ethical considerations
This study was conducted in accordance with the ethical standards of the 1964 Declaration of Helsinki and its later amendments. Ethical approval was granted by the Institutional Ethics Committee of HCG Cancer Centre, Bengaluru (Approval No:
Consent to participate
Not applicable.
Consent to publish
Not applicable. (No identifiable data, images, or personal details requiring publication consent are included in this manuscript.)
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.