
Abstract
Background
Pediatric patients undergoing chemotherapy often need to take multiple medications. Consequently, they may experience drug-related problems (DRPs), including adverse drug reactions, drug interactions, and various medication errors.
Methods
A prospective observational study was conducted over three months in the Pediatric Haemato-oncology department of a cancer specialty hospital of Nepal following ethical approval. DRPs were identified from patient medical records and the literature and, recorded according to the Pharmaceutical Care Network Europe V9.1 tool. Data were collected and analyzed using IBM SPSS Statistics V20 and Microsoft Excel 2013 to present the findings.
Results
Among the 30 enrolled patients, 211 DRPs were identified in 28 patients (93.3%), averaging 7.5 DRPs per patient, all validated through case-by-case review. Treatment safety was the predominant DRP type (n = 131; 62.09%), followed by treatment ineffectiveness (n = 79; 37.44%). Drug selection (n = 116; 51.76%) and dispensing issues (n = 51; 22.77%) were the leading causes, with anti-infective drugs (n = 41; 35%) and antineoplastic agents (n = 24; 20.5%) most frequently implicated.
Conclusion
DRPs were prevalent among pediatric patients with cancer, with treatment safety being the most significant issue and drug selection being the primary cause. Anti-infective drugs were most frequently involved in DRPs, followed by antineoplastic and immunomodulating agents.
Keywords
Introduction
As per the International Agency for Research on Cancer (IARC), almost 300,000 children and adolescents (0–19) in 2022 had cancer, with more than 100,000 deaths, with leukemia being the predominant cancer. 1 The National Cancer Institute (NCI) estimates over 9500 childhood (below 15 years) cancer cases and more than 1000 deaths in the US in 2024. 2 The global cancer incidence report also predicts that the incidence of cancer is likely to increase in the coming days in countries that are poor in the human development indices. 3 According to the Cancer Incidence and Mortality Rate in Selected Districts of Nepal (2019), only 119 new pediatric cancer cases (ages 0–19) were reported nationwide. This indicates that the reported number of pediatric cancer cases is very low. 4 Particularly, the survival rate of pediatric cancer cases is very low in low middle income country (LMIC) compared to developed countries due to resource unavailability, misdiagnosis issues, lack of affordable treatment, toxicity issues, and mortality due to drug-related problems (DRPs).5–8
The management of cancer often involves complex, multi-agent therapies (chemotherapy, radiotherapy, and surgery), supportive medications, and frequent modifications based on clinical response and toxicity profiles. This complexity is particularly pronounced in children compared to adults due to differences in physiology, organ development, and body surface area, which alter a drug's pharmacokinetic and pharmacodynamic properties. 9 Altogether, this increases the likelihood of DRPs such as adverse drug reactions (ADRs), drug interactions, and medication errors.10,11 Literature also highlights that these DRPs are often associated with many deleterious consequences, including frequent emergency visits, longer care admissions, longer hospitalization, and additional hospital visits.12,13
However, there are limited studies that have explored the DRPs specifically among the pediatric cancer population. A study from a government tertiary hospital in Ethiopia reported the incidence of 68.6% DRPs with a specific focus on pediatric patients with cancer. 9 Similary, a study conducted on pediatric patients within an infectious center showed a prevalence of greater than 70% of DRPs with various predictive factors such as polypharmacy, comorbidity and prolonged hospital stay. 12 Pediatric inpatient safety is also a matter of concern 14 within across several medical fields, including neurology, 15 palliative settings care, 16 and even mental health conditions. 17 Literatures also highlights the relationship between polypharmacy leading to cases of drug safety issues within pediatrics,15–17 underscoring the need for attention from policymakers, through further research and inclusion of clinical pharmacists in the multidisciplinary team dealing with complex regimens used in children.14,16
In Nepal, the concept of pediatric pharmacy practice is still in its infancy, as clinical pharmacy practice is lacking in inpatient settings. 5 Despite limited studies assessing the DRPs in different settings with the Nepalese context,18–20 no prior studies have evaluated DRPs in pediatric oncology patients using Pharmaceutical Care Network Europe (PCNE) V 9.1 tool. Hence, to promote the idea of inpatient pharmacy practice and pharmaceutical care among vulnerable population groups, it is important to identify and resolve DRPs. 21 Although several previous studies have reported DRPs in the pediatric population,9,16,22–26 no research to date has prospectively investigated this issue within pediatric settings in Nepal. Therefore, a prospective study was designed to determine DRPs and their causes using the PCNE V 9.1 tool among pediatric patients with cancer visiting a cancer specialty hospital in Nepal.
Materials and methods
Study design and settings
A prospective observational study was designed to assess DRPs and their causes among pediatric inpatients in the pediatric haemato-oncology ward at Nepal Cancer Hospital and Research Centre (NCHRC), Harisiddhi, Lalitpur, Nepal. NCHRC was selected for this study as the hospital has a separate pediatric haematology-oncology ward with a multidisciplinary team approach to treatment. The study was carried out for 6 months, including time for literature review, data collection, and data analysis, during which data collection took place from 30th July to 3rd November 2023.
Study participants and sampling criteria
A census sampling technique was employed, 27 enrolling all pediatric patients admitted to the pediatric haemato-oncology ward of NCHRC during the 3-month data collection period. Since this was a baseline study with no prior local prevalence data on childhood cancer-related DRPs in Nepal, 4 a census approach was adopted to capture all eligible cases during the study period rather than calculating a sample size.
Pediatric patients with a confirmed cancer diagnosis, both newly admitted and follow-up patients, who were admitted to the ward during the data collection period, along with a caregiver or legally authorized representative (LAR) willing to provide written informed consent and the patient's written or verbal assent, were included in the study. Patients were excluded if their caregivers refused participation, if they were preterm newborn infants (gestational age <37 weeks), if their diagnosis was unconfirmed, or if they were admitted solely for surgical management.
Data collection tools and techniques
DRP classification system
Several tools, such as Cipolle/Morley/Strand classification, 28 Hepler-Strand classification, 29 American Society of Health-System Pharmacists (ASHP) guidelines for pharmaceutical care, 30 ABC Classification, 31 Pharmaceutical Care Network Europe, 32 are available to classify the DRPs. The Cipolle/Morley/Strand classifies the DRPs among seven different categories, such as unnecessary drug therapy, the need for additional drug therapy, ineffective drug therapy, dosing either too low or too high, cases of ADR, and non-compliance. 28 While these older systems provided a groundwork for DRP identification, mainly focused on identifying what the problem is, the latest version of PCNE V9.1 tool comprehensively explains DRPs with three different primary domains as treatment effectiveness (problem with the effect of therapy), treatment safety (occurrence of ADRs) and others (unnecessary drug treatment, unclear problem). 32 This makes it a more appropriate and robust tool for research, clinical audits, and pharmaceutical care improvement. This version was developed in February 2020 and includes five classifications (Problems, Causes, Planned Interventions, Level of acceptance, and status of the problems). 32
Data collection form
Data were collected using a structured proforma developed based on relevant literature 9 to capture both dependent and independent variables (Figure 1). Patient characteristics, prescribed medications, and DRPs classified according to the PCNE V9.1 tool 32 were documented. Socio-demographic information was obtained through independent interviews with the patient's caregiver/relative/LAR by the pharmacist (author NP). In parallel, inpatient medication cardex were reviewed to extract information on diagnosis, treatment plans, and medication use.
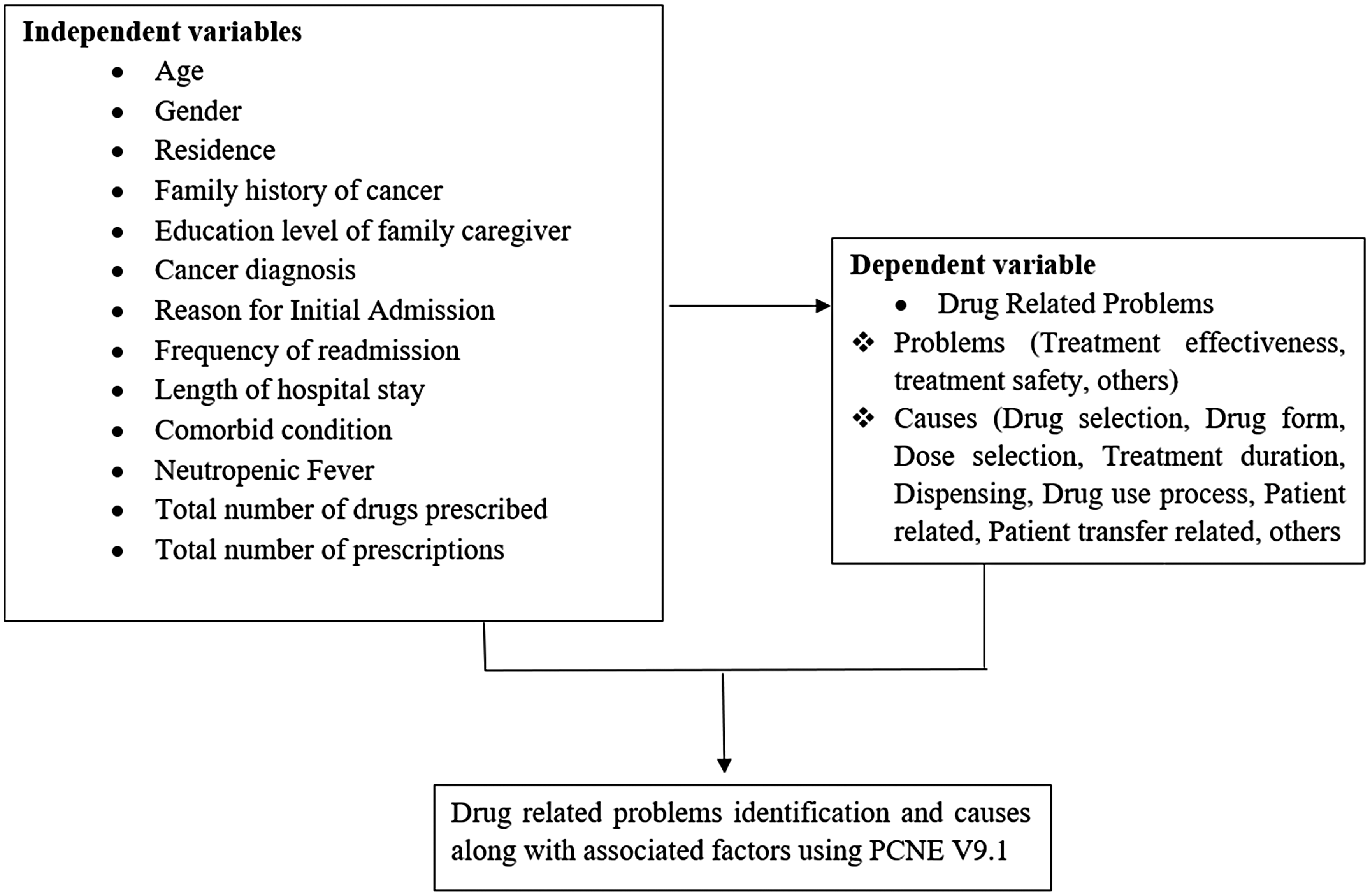
Dependent and independent variables of the study (the independent variables include the sociodemographic and clinical variables, while the dependent variables include drug-related problems and their causes.) [Abbreviation: PCNE – Pharmaceutical Care Network Europe].
Identification of DRPs was performed independently by two pharmacists, who subsequently discussed them with the hospital's clinical pharmacist referencing standard treatment guidelines and literatures.
Study process and identification of DRPs
After patient selection based on inclusion and exclusion criteria, informed written consent was obtained from the parent/caregiver/LAR, and written/verbal assent from the patient was obtained, depending on the Nepal Health Research Council's ethical guidelines of 2022. 33 The purpose, objectives, and time commitment of the study were clearly explained prior to obtaining consent and assent. Confidentiality of all information was assured to encourage honest, natural responses.
A prospective medication review was conducted for each enrolled patient throughout their hospital stay. DRPs were identified using a systematic, evidence-based approach that included reviewing patients’ medication charts, laboratory findings, medical records, and structured interviews with caregivers and patients.
Treatment appropriateness was evaluated against current evidence-based oncology and supportive care guidelines, including the National Comprehensive Cancer Network (NCCN) pediatric oncology protocols, American Academy of Pediatrics guidelines, and Hematology Oncology Pharmacy Association (HOPA) recommendations. For disease-specific assessments, the following references were additionally consulted based on the patient's diagnosis: the NCCN Clinical Practice Guidelines for specific malignancies (Acute Lymphoblastic Leukemia, Lymphoma, Wilms’ Tumor, and Retinoblastoma), WHO Essential Medicines for Children, and disease-specific supportive care protocols if available at NCHRC.
The appropriateness of dosing regimens was evaluated by comparing prescribed doses against evidence-based guideline recommendations, including the National Antibiotic Treatment Guidelines 2014, 34 National List of Essential Medicines 2021 35 and Nepalese National Formulary 2018. 36 For chemotherapy dosing, body surface area (BSA)-based dose calculations were verified against NCCN protocol-specific dosing references.
The identified DRPs were systematically classified using the PCNE V9.1 cause classification framework, based on triangulated evidence from three sources: patient medical records and medication charts, structured caregiver/patient interviews, and clinical assessment findings. This multi-source triangulation ensured that cause attribution was not based solely on medical records but was corroborated by patient-reported information and clinical context. Drug-drug interactions were screened using Medscape
37
and Micromedex.
38
The complete study process for DRP identification is depicted in Figure 2
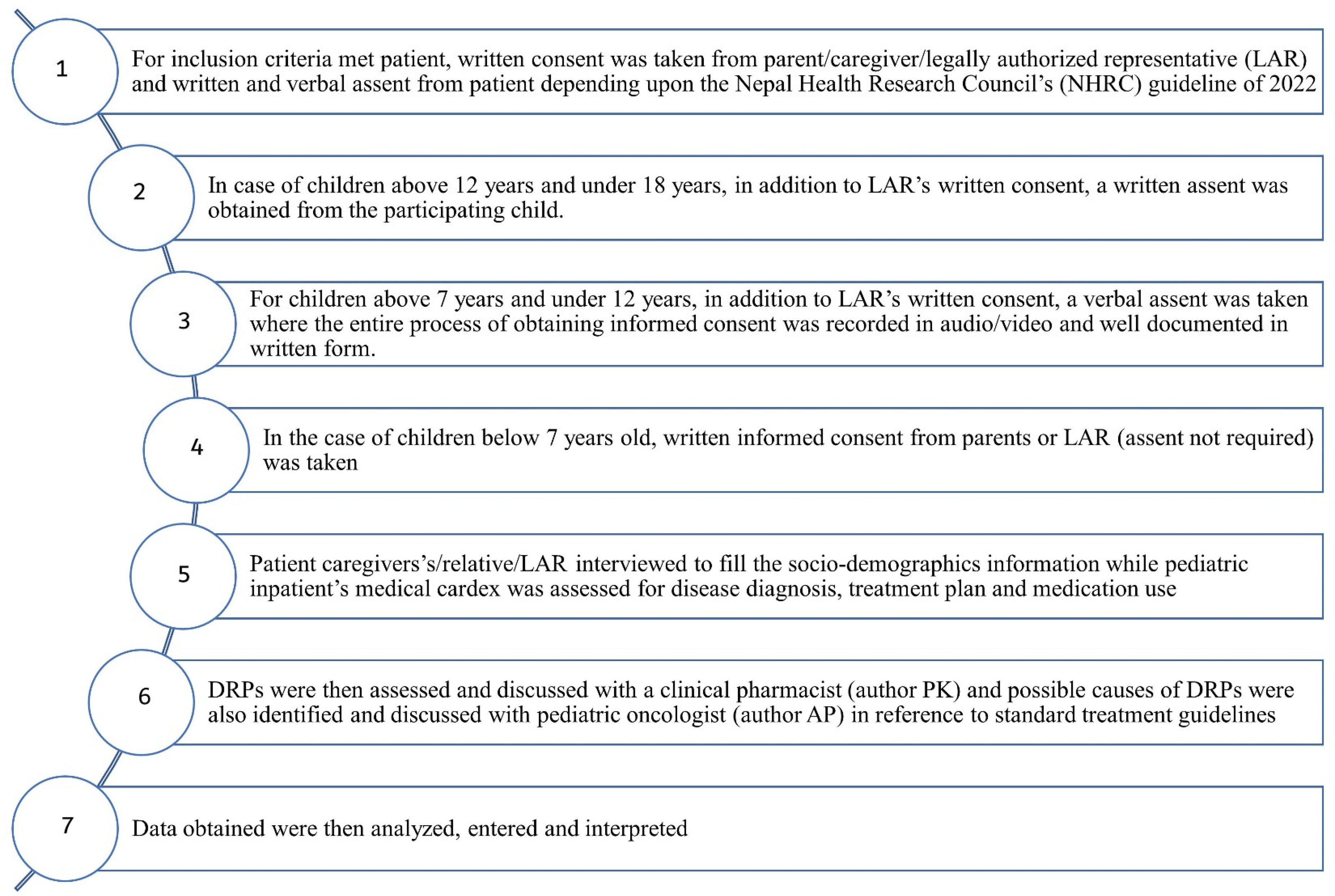
Operational modality of the study (the figure shows the operational modality beginning with the inclusion criteria to how the drug related problems and its causes were identified.) [Abbreviation: NHRC: Nepal Health Research Council; LAR - Legally authorized representative (refers to any person who under the judicial law is able to give consent on behalf of the patient when the patient is unable to give consent because of the medical condition); DRP: Drug related Problems].
Ethical consideration
Ethical approval was obtained from the Institutional Review Committee (IRC) of Pokhara University Research Centre (Ref no- 143/079/080). Data collection approval was also obtained from NCHRC (Ref. no.: 688-2079/080). The patients were assured that the information provided on the questionnaire would be kept confidential. In addition, participation in the research was voluntary, and participants could leave the interview at any time without giving a reason.
Data analysis
Data were initially entered into the Statistical Package for the Social Sciences (SPSS 20) and Microsoft Excel 2013. Statistical tests such as the Shapiro-Wilk and Kolmogorov-Smirnov tests were used to assess data normality. Quantitative data were presented as frequencies and percentages. Descriptive statistics such as measures of central tendency (mean, median) and measures of dispersion (standard deviation, inter-quartile range) were applied to analyze the data and the findings of the study were presented in tables and bar diagrams.
Results
Characteristics of participating patients
Among 30 patients enrolled (Figure 3) during the study, the majority were in the 1 to 5 age group (n = 13, 43.3%), male (n = 23, 76.7%), and resided in urban areas (n = 18, 60%). Most of the patient's caregivers had a formal education in grades 9–12 (n = 16; 53.3%) (Table 1).
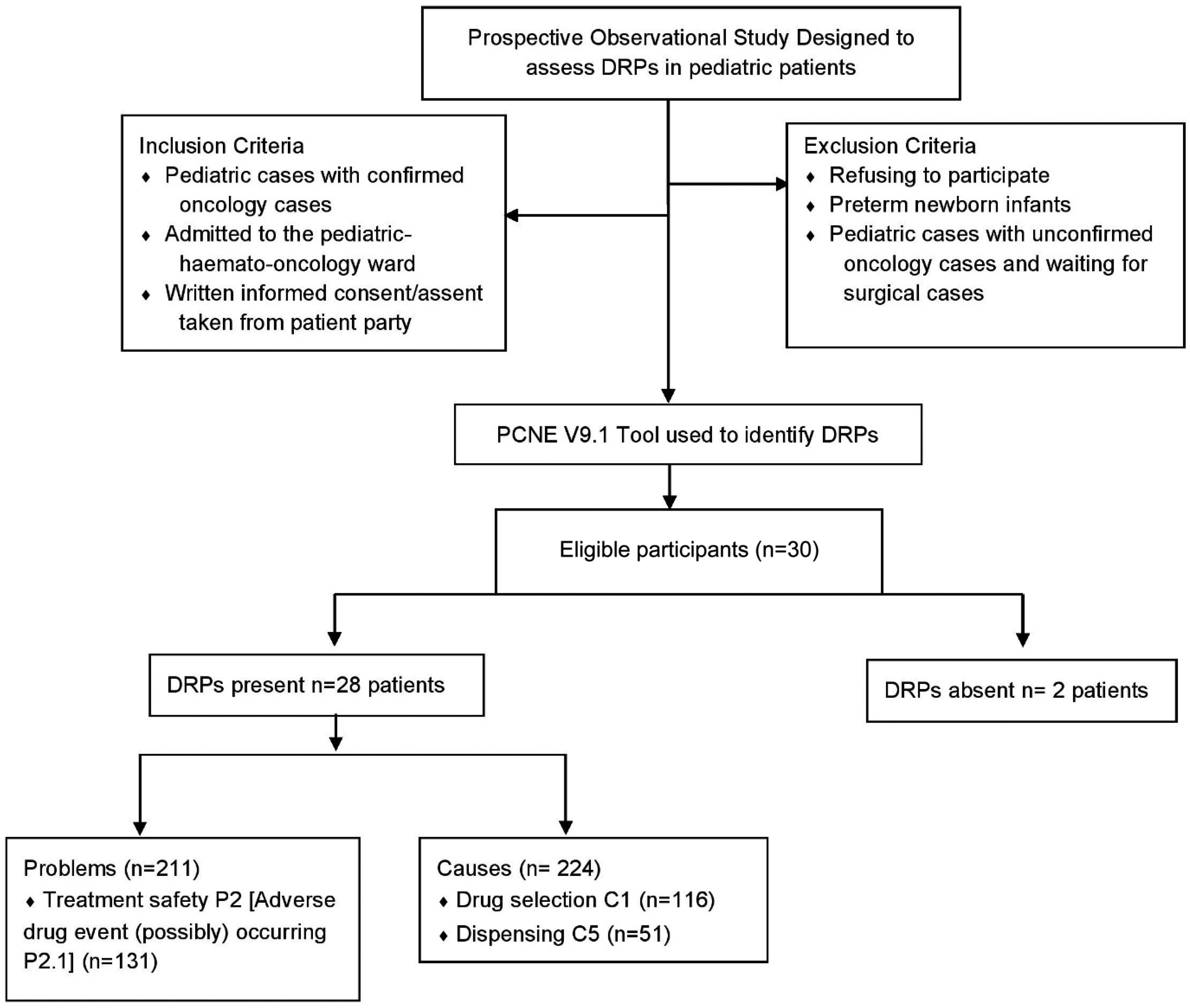
Participant and drug related problems flow-diagram (the figure shows the participant flow diagram with the tool used to identify drug related problems and the frequency of identified problems and causes.) [Abbreviation: PCNE- Pharmaceutical Care Network Europe; DRP: Drug related Problems].
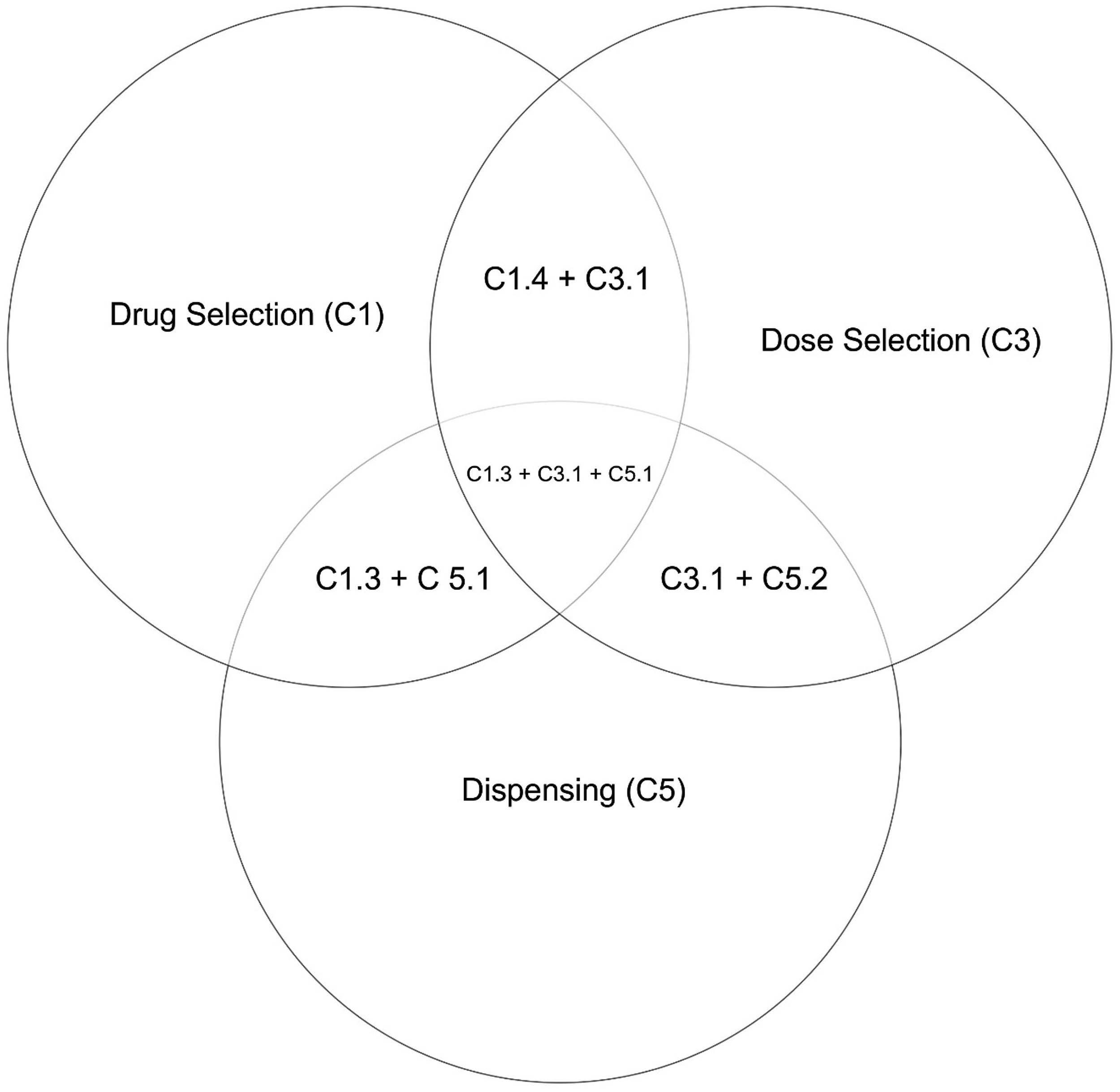
Causes of drug-related problems that might overlap (as a venn diagram) (the figure shows the causes of drug-related problems that might overlap, representing the domain and sub-domain causes.).
Socio-demographic information of the patients.
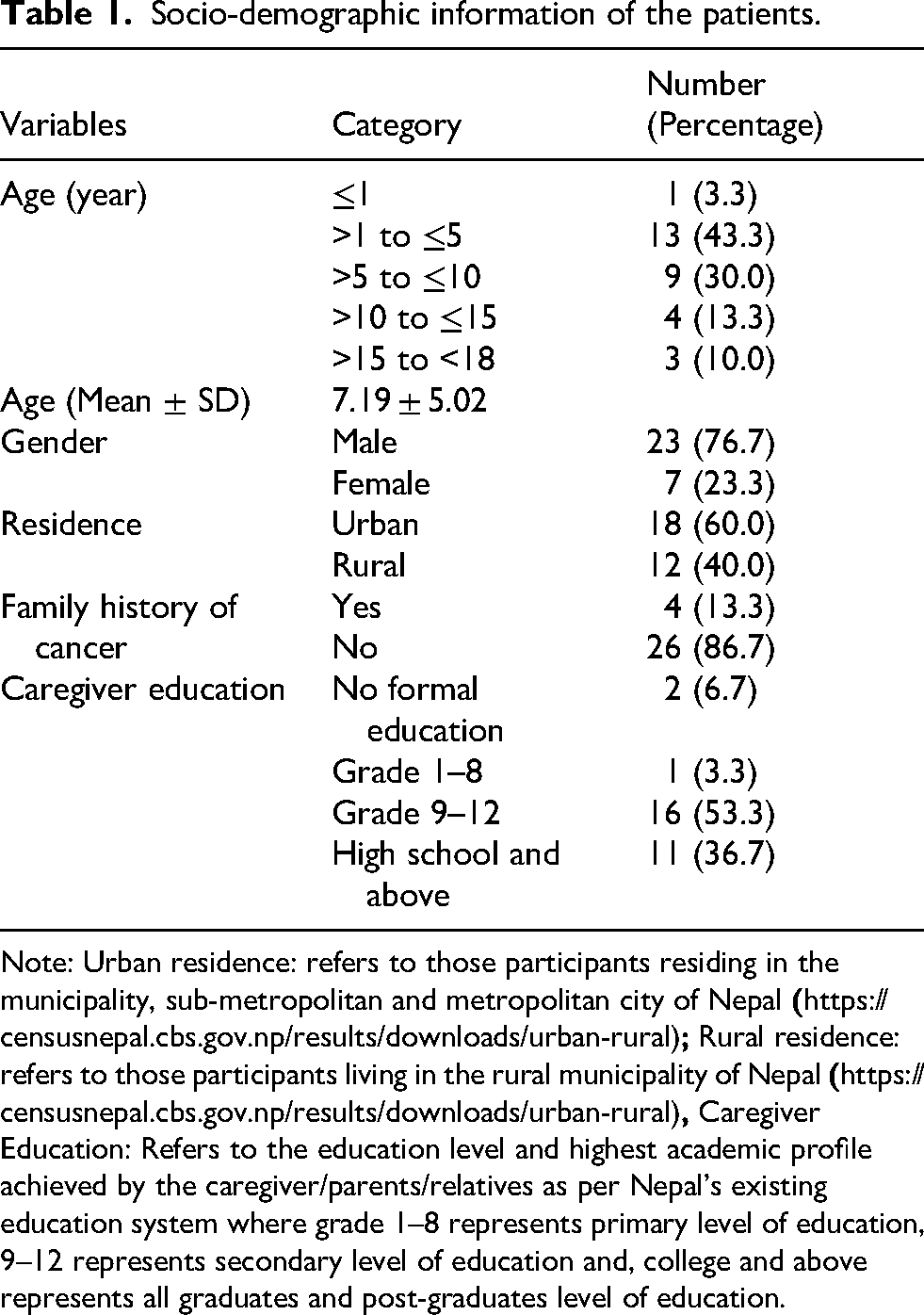
Note: Urban residence: refers to those participants residing in the municipality, sub-metropolitan and metropolitan city of Nepal
Acute lymphoblastic leukemia (n = 17; 56.7%) and non-Hodgkin's lymphoma (n = 3; 10%) were the most common diagnoses. The majority of patients were admitted for chemotherapy and hydration (n = 17; 56.7%), followed by supportive care (n = 9; 30%). Regarding the length of hospital stay, sixteen patients stayed there for more than 10 days. Median hospital stay was 13 (IQR=6–27.50). Most patients received fewer than 10 prescriptions, while 36.7% received more than 10 during the study. Median number of drugs prescribed was 35 (IQR=14.75–67.25) (Table 2).
Clinical characteristics of the patients.
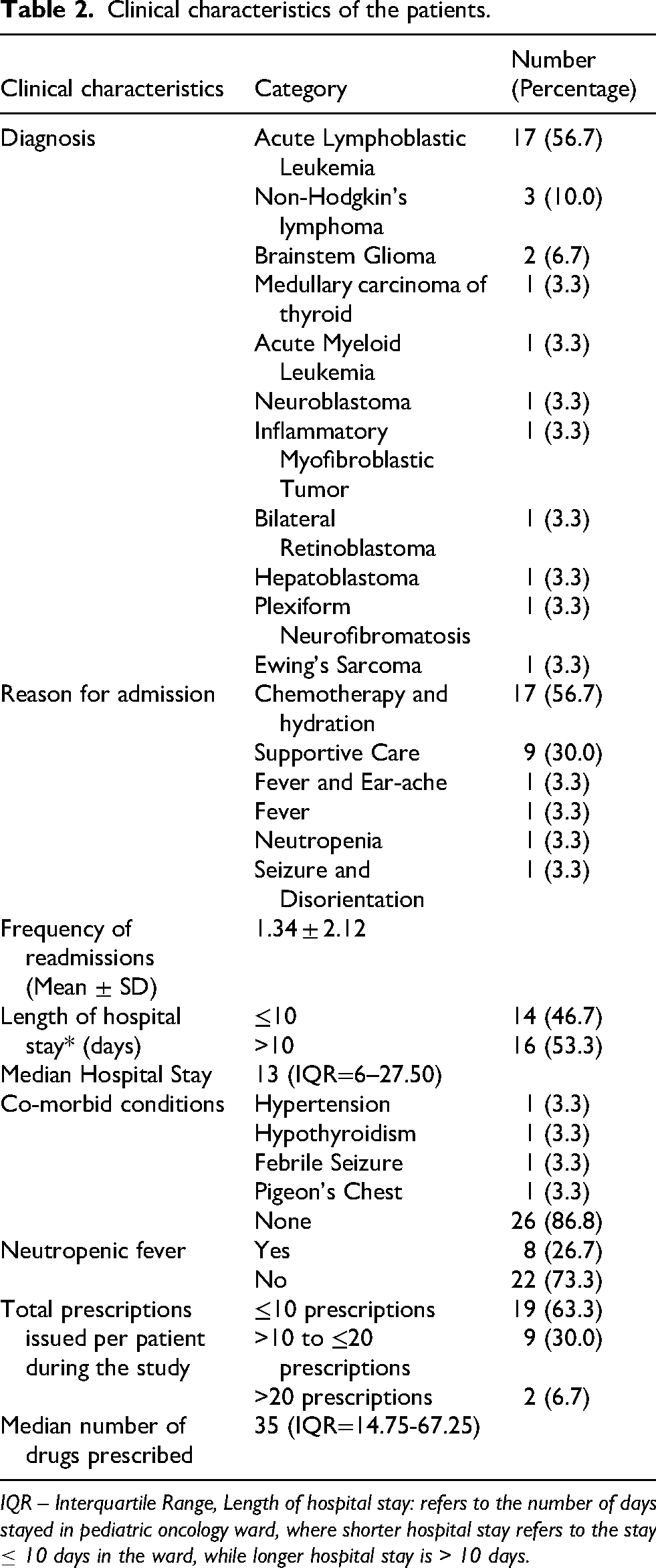
IQR – Interquartile Range, Length of hospital stay: refers to the number of days stayed in pediatric oncology ward, where shorter hospital stay refers to the stay ≤ 10 days in the ward, while longer hospital stay is > 10 days.
DRP identification and prevalence
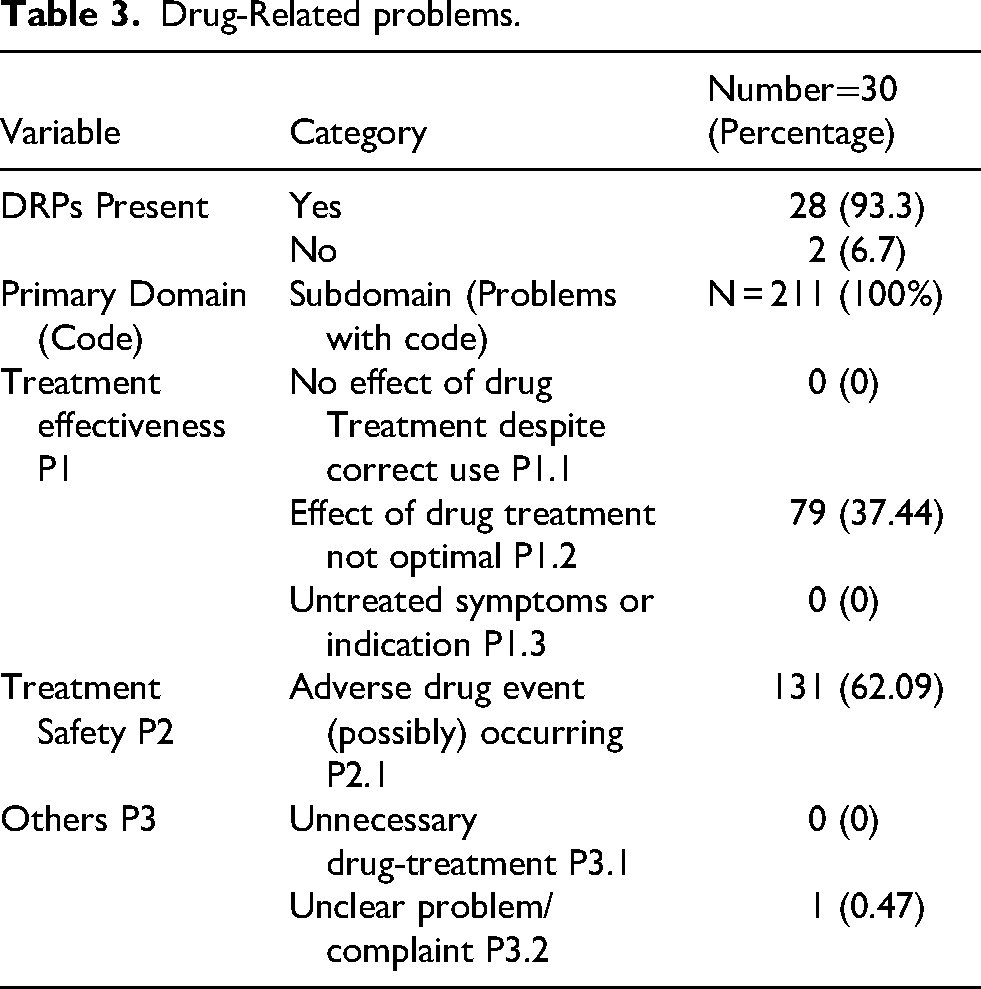
DRPs were present in 28 (93.3%) patients (Figure 3). Two hundred eleven problems were identified in 28 patients, averaging 7.5 DRPs per patient. Following the identification of problems as per the PCNE V9.1 tool, the majority of the issues were associated with treatment safety P2 (n = 131; 62.09%), which includes adverse drug events (possibly) occurring P2.1 (Table 3).
Drug-Related problems.
Causes of DRPs
Out of the possible causes, primary domain Drug selection C1 (n = 116; 51.79%) was the primary cause, followed by dispensing C5 (n = 51; 22.77%). Within the C1 section, subdomain C1.3 was mainly responsible for causing DRP (n = 71; 31.70%), while in the C5 section, subdomain C5.1 was mainly accountable for causing DRP (n = 46; 20.54%). Similarly, sub-domains C1.2 (n = 27; 12.05%) and C3.1 (n = 24; 10.71%) were also responsible for causing DRPs (Table 4).
Causes of the DRPs.
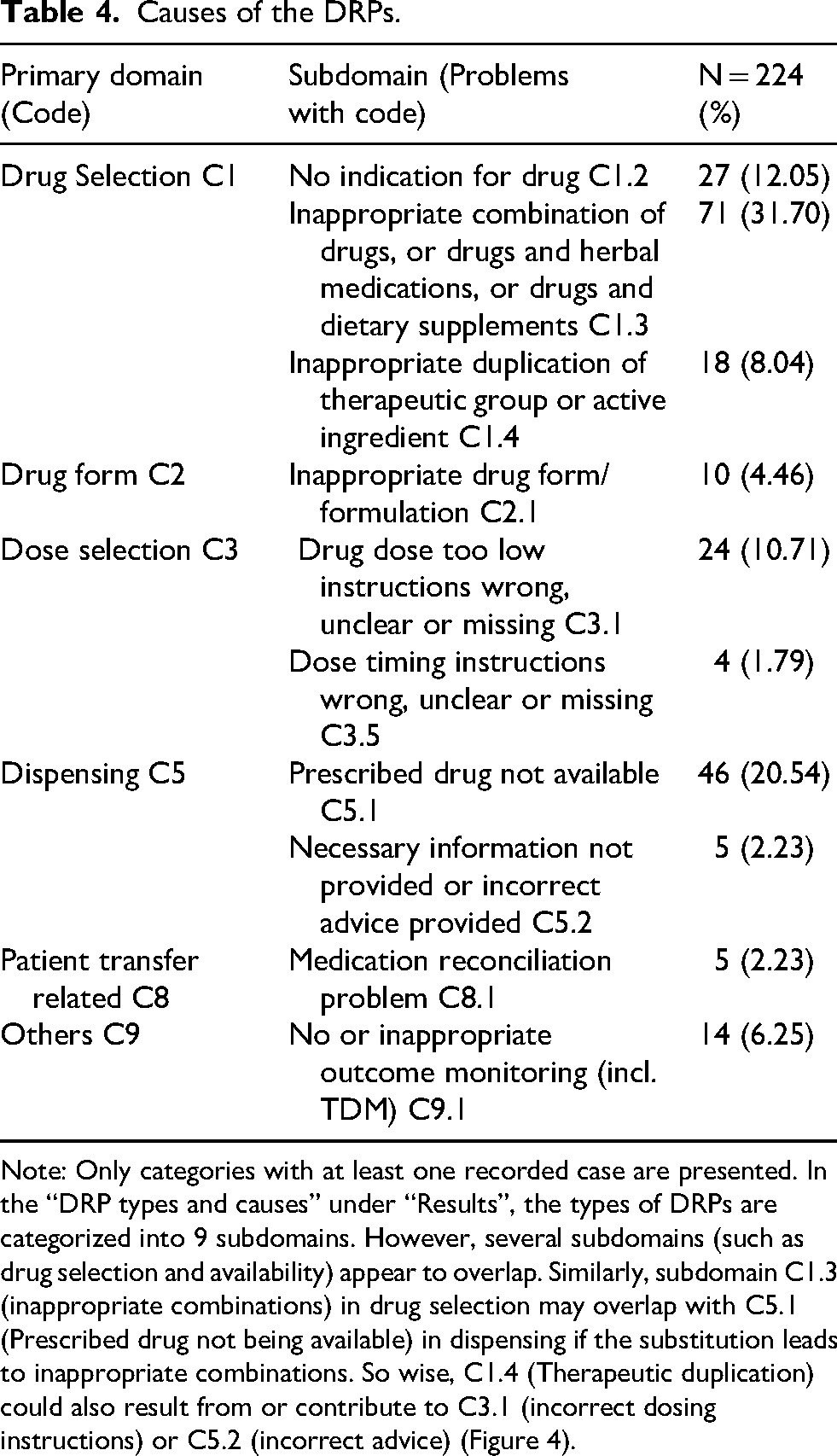
Note: Only categories with at least one recorded case are presented. In the “DRP types and causes” under “Results”, the types of DRPs are categorized into 9 subdomains. However, several subdomains (such as drug selection and availability) appear to overlap. Similarly, subdomain C1.3 (inappropriate combinations) in drug selection may overlap with C5.1 (Prescribed drug not being available) in dispensing if the substitution leads to inappropriate combinations. So wise, C1.4 (Therapeutic duplication) could also result from or contribute to C3.1 (incorrect dosing instructions) or C5.2 (incorrect advice) (Figure 4).
Drugs causing DRPs
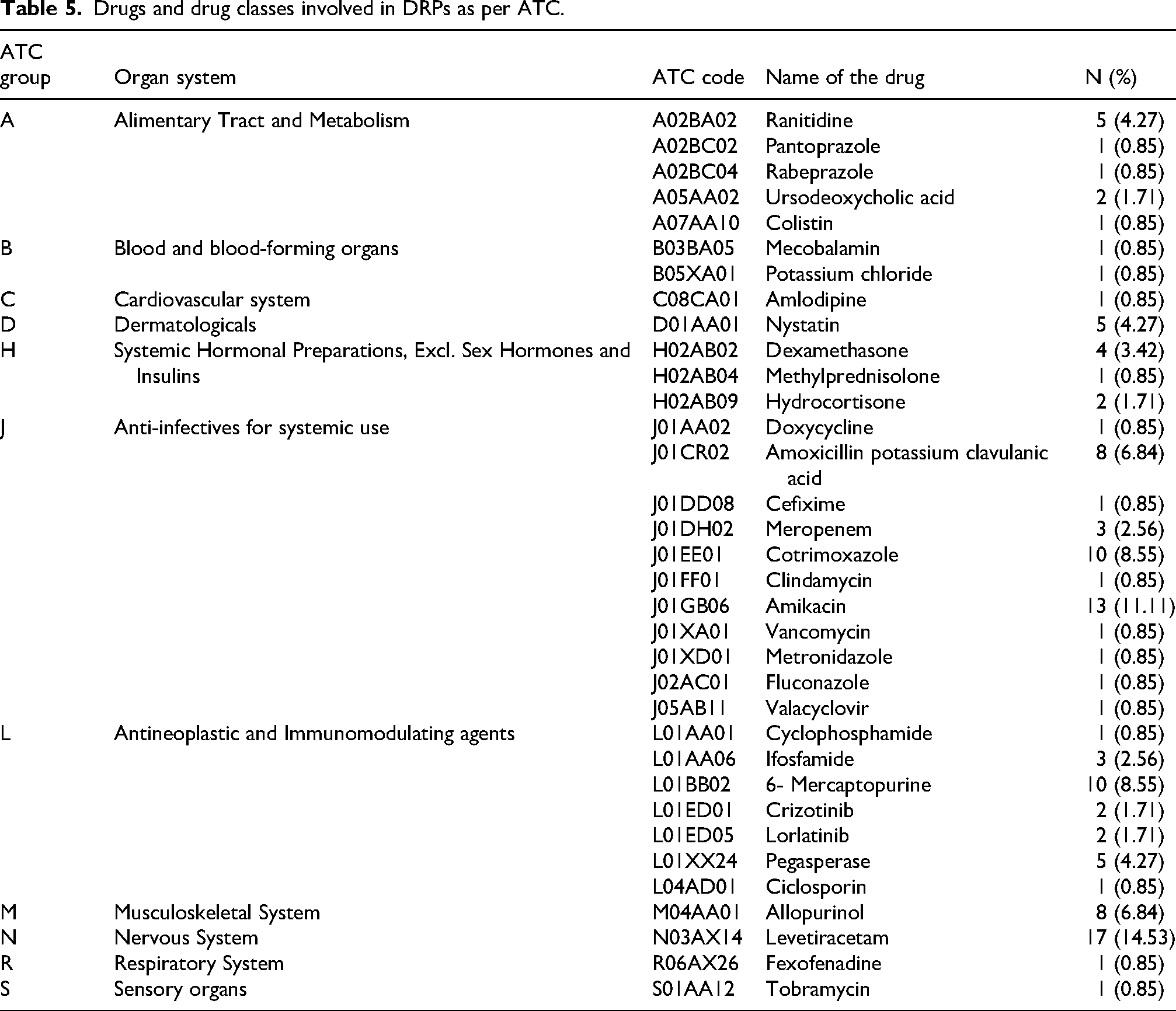
An analysis of drugs involved in DRPs as per the ATC classification shows that the majority of drugs involved in DRPs belonged to the ATC class J, Anti-infectives for systemic use (n = 41; 35%) followed by ATC Class L, Antineoplastic and immunomodulating agents (n = 24; 20.5%) (Table 5). Within Anti-infective for systemic use, cotrimoxazole (J01EE01) was majorly involved in DRPs (n = 10; 8.55%), while in group L, the major drug responsible for DRP was 6-Mercaptopurine, L01BB02 (n = 10; 8.55%). When analyzing a single entity, levetiracetam, N03AX14 (n = 17; 14.53%), belonging to the group N (Nervous System), was mainly responsible for the DRPs (Figure 5).
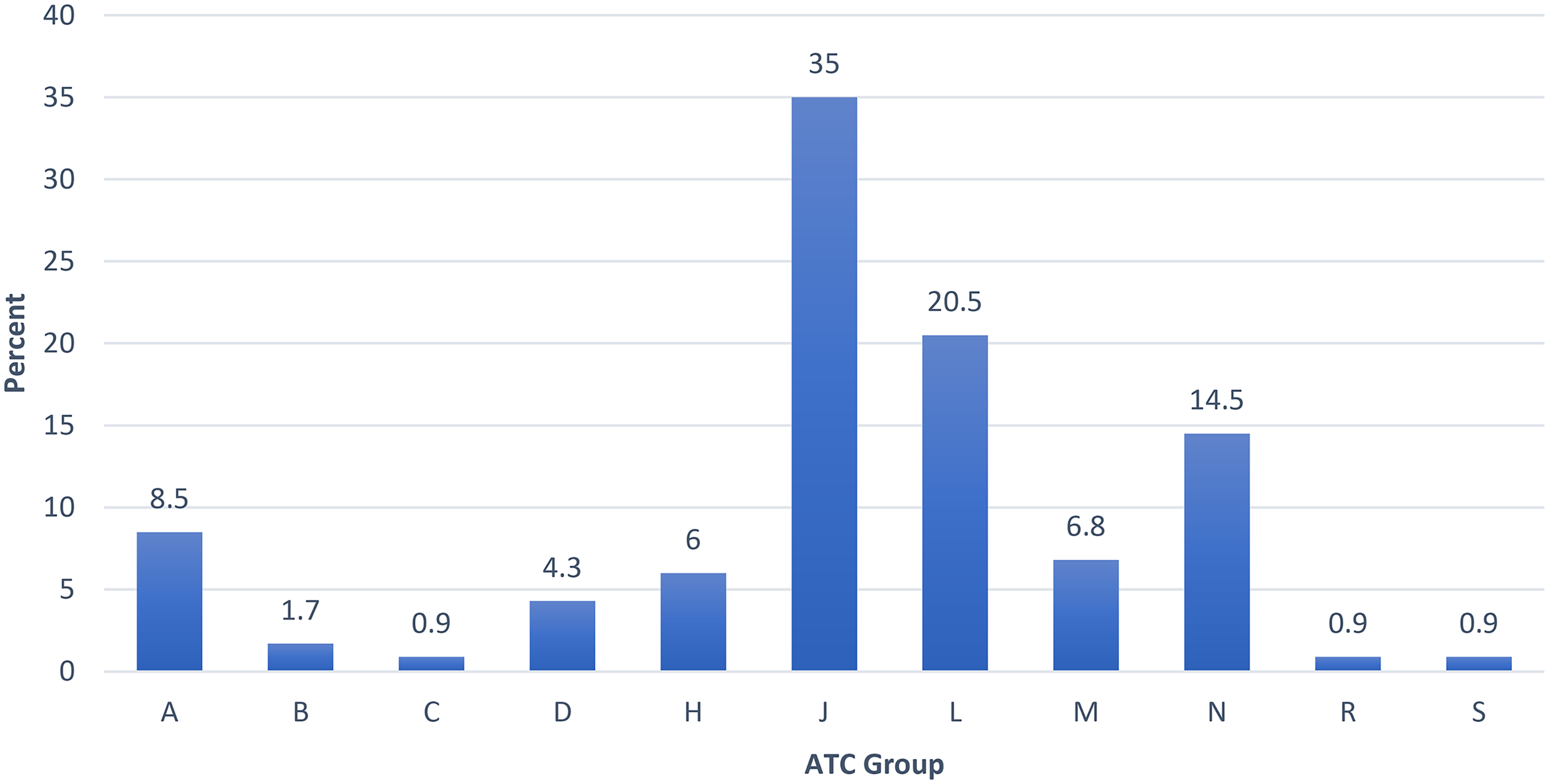
Percentage of DRPs according to anatomical therapeutic chemical classification of drug where A: drugs acting on alimentary tract and metabolism, B: drugs acting on blood and blood forming organs, C: drugs acting on cardiovascular system, D: dermatologic drugs, H: systemic hormonal preparations, excluding sex hormones and insulin, J: anti-infectives for systemic use, L: antineoplastic and immunomodulating agents, M: drugs acting on musculoskeletal system, N: drugs acting on nervous system, R: respiratory system, S: sensory organs.
Drugs and drug classes involved in DRPs as per ATC.
Discussion
Our study found that 76.7% of patients were male, with the majority of children (73.30%) aged 1–10 years. This aligns with Ethiopian study reporting 62.8% males and 87.2% in the same age group. 9 The most common types of cancer identified in this study were acute lymphoblastic leukemia (56.7%) and non-Hodgkin's lymphoma (3%). Yisma et al. also observed the similar pattern of predominancy of hematological malignancies; however, non-Hodgkin's lymphoma was in higher higher rate than acute lymphoblastic leukemia. 9 A study from children's hospital in Saudi Arabia found acute lymphoblastic leukemia as the most common hematological malignancy. 39 Globally, hematological malignancies are generally higher in men, with increasing trend in the across central Europe, eastern Europe, East Asia, and the Caribbean. 40 These highlight the consistent domainancy in male and strong burden of acute lyphoblastic leukemia across regions. Early diagnosis with strengthened pediatric oncology services is essential to ensure improved care.
The major problem observed in the pediatric population was treatment safety (P2), which contained a sub-domain of potentially occurring adverse drug event (P2.1) reported in 131 cases (62.09%). Neutropenia, thrombocytopenia, hyponatrium, hyperuricemia, shortness of breath, elevated liver enzymes were the frequently observed ADRs among the patients. The median number of drugs used during the study was 35, indicating a high level of polypharmacy. Polypharmacy is very common in cancer patients due to multiple healthcare needs; however, it also increases the risk of acquiring ADRs.23,41 Moreover, anti-cancer drugs are often associated with a low therapeutic range, which increases the risk of obtaining toxicity, and as a result, several ADRs are seen. 42 This is similar to a study conducted in two settings, in which ADRs were the main DRPs identified.43,44 However, the result is the opposite of that in the study by Yismaw et al., in which the DRPs related to ADR were relatively low. 9 Two studies used a different tool to classify DRPs rather than PCNE. Similarly, 36.57% of the problems associated with the effect of drug treatment not being optimal in our study could be co-related to several factors such as the use of irrational combinations of drugs, absence of drugs in the hospital settings, and drug doses being too low.
Regarding the causes of DRPs, the selection of the drug (C1) was the most common. Within this domain, an inappropriate combination of drugs, or drugs and herbal medications, or drugs and dietary supplements, was the primary cause of DRPs (31.70%). Such findings could be correlated to the study by Abdulkadir et.al (2023), where the study mentions how the occurrence of DRPs in the pediatric population is related to drug selection. 22 Literature also shows that the consumption of traditional, complementary, and alternative medicines is growing gradually because of several factors such as increased demands, cultural beliefs and practices, huge expenditure because of conventional treatments, and the belief that herbal and ayurvedic products are safe.45,46 Patient preference for these practices of herbal remedies and traditional medicines could further lead to side effects, 45 acting as a significant contributor to DRPs. This would further exacerbate if the patient is consuming both conventional chemotherapy and herbal remedies concomitantly. This underscores the need for physicians to pay attention to informing the patient and robustly communicating with the patient about the use and its disclosure.47–49 Similarly, pharmacists in clinical settings can help identify potential drug-drug and drug-herbal interactions, ensuring that approved drugs or herbal remedies are safe and free of severe interactions.
Similarly, the availability of the prescribed drug was the second major cause (20.54%) for DRPs. The lack of drugs being the reason for DRPs was also reported in the study conducted in Ethiopia. 9 Pediatric oncology wards are particularly vulnerable to drug shortages. 50 In Nepal, cancer medicines are available only after registration with the national regulatory authority, the Department of Drug Administration (DDA). Once approved, they are distributed to retailers and hospital pharmacies through authorized superstockists. However, our study identified several drugs in use that were not registered at the time of the study (Supplementary File 1), thereby affecting their availability within the hospital. Notably, 6-mercaptopurine was not registered during the study period, leading to significant procurement and supply challenges. Even among registered medicines, some were unavailable at the facility level, likely due to issues related to hospital procurement systems, lead times, and inventory management (Supplementary File 1). These findings highlight systemic gaps in drug availability. Addressing them requires stronger national policies to prevent drug shortages, improved supply chain management, and coordinated interdisciplinary collaboration among hemato-oncologists, pharmacists, nurses, public health policymakers, and researchers. Additionally, educating patients and caregivers about potential drug shortages may help mitigate disruptions to treatment continuity.50,51
The majority of the pediatric inpatients (n = 16; 53.3%) were found to have a longer length of hospital stay (>10 days) with a median stay of 13 and a frequency of readmission of 1.3 ± 2.12. Pediatric patients with cancer present a longer hospital stay during the induction and maintenance therapy phase. Several studies have also highlighted on how DRPs are often associated with longer care admissions and hospitalization, leading to economic burden.12,13,52 This underscores the need for clinical pharmacist intervention in the coming days to reduce the number of DRPs, which would further help decrease longer hospitalizations and economic burden as pharmacists have been identified as an important contributor to identifying and reducing these DRPs in pediatric settings.9,12,26,53 Evidence from a randomized controlled trial showed that pharmacist-led interventions improved the DRP incidence in pediatric settings. 24 Their contributions expand further as clinical pharmacists in reducing DRPs through several roles such as medication review, clinical decision support, patient counseling and pharmacovigilance. 54 ASHP further emphasized pharmacists in promoting pharmaceutical care within clinical, hospital and community settings as a collaborative one with other healthcare professionals. 55
Analysis of medications associated with DRPs showed that 35% involved ATC class J (anti-infectives for systemic use), followed by class L (antineoplastic and immunomodulating agents). Cotrimoxazole and 6-MP were the most frequently implicated drugs. Similar patterns have been reported in Ethiopia, where anti-infectives and antineoplastic agents were also leading contributors to DRPs. 9 The high involvement of anti-infectives raises concerns about inappropriate antimicrobial use and the potential development of antimicrobial resistance (AMR)56–58 underscoring the need for adherence to treatment guidelines and rational prescribing practices.
Antineoplastic and immunomodulating agents were commonly associated with adverse drug reactions, including bone marrow suppression, neutropenia, thrombocytopenia, and tumor lysis syndrome. Consistent with this, treatment safety, particularly potential or actual adverse drug events, was the most frequent DRP category. These findings highlight the importance of active pharmacovigilance and timely reporting of ADRs. As a regional pharmacovigilance center, NCHRC plays a crucial role in strengthening ADR monitoring and promoting patient safety.59,60
High-risk medications, including anti-infectives,57,58 antineoplastic agents, 41 opioids61–64 and complementary medicines,45,46 further increase the risk of severe ADRs, dosing errors, and monitoring challenges in pediatric oncology. Although high-income countries also report substantial DRP prevalence among children, stronger healthcare systems and established pharmaceutical care services enable more effective prevention and management,25,65–67 an advantage that remains limited in many LMICs, including Nepal.
Implications
This study demonstrates a high prevalence of DRPs among pediatric oncology patients, arising from multiple causes. The findings have several important implications for different stakeholders.
For policymakers, the results highlight the need to strengthen mechanisms that ensure drug availability and formally integrate pharmacists or clinical pharmacists into direct oncology patient care within the Nepalese context. 68 Previous studies have shown that involving clinical pharmacists improves the identification of DRPs, clarifies their underlying causes, and facilitates their resolution.5,9,14,16,24,69–71
For hospital administration and clinical teams, the findings suggest that Drug and Therapeutic Committees can proactively collaborate with pediatric oncologists, pharmacists, and allied health workers to maintain the availability of chemotherapeutic drugs, thereby minimizing DRPs.
From a research and public health perspective, this study provides valuable cancer demographic data that can support and enhance Nepal's national population-based cancer registry.
Finally, for healthcare professionals, the results underscore the importance of continuous professional development and training to increase awareness of DRPs, understand their potential consequences, and implement effective prevention strategies.
Strengths and limitations
To the best of our knowledge, this is the first study in Nepal to examine DRPs among pediatric inpatients with cancer using a standardized, validated tool. This study aimed to broadly assess DRPs rather than focus on each specific type, such as evaluating the severity of drug-drug interactions. Considering the potential clinical implications of each DRPs type, future studies are recommended to examine them in greater detail.
While the PCNE V9.1 classification tool is a well-established and standardized method for identifying and categorizing DRPs, this study did not assess inter-rater reliability (e.g., Cohen's Kappa) between the assessors. The absence of this measure may limit the evaluation of consistency in DRP identification and classification.
Another limitation is low sample found during three-month prospective period, reflecting both low incidence of pediatric cancer in Nepal (only 119 cases reported in 2019 population-based registry) 4 and broader challenges in LMICs, including limited access to affordable and timely healthcare services, high rates of treatment abandonment, frequent misdiagnoses, and delays in diagnosis.6–8
This constrains the generalizability and statistical power of our findings. Future research should consider longer data collection periods and advanced statistical approaches, such as multivariate analysis, to explore potential predictors of DRPs, which could inform appropriate preventive interventions. No specific tool was used to grade or classify the DRPs as major, minor, or severe using scales such as the Naranjo scale, the WHO-UMC causality scale, and the National Cancer Institute-Common Terminology Criteria for Adverse Events (NCI-CTCAE). Since the ADRs were assessed using the laboratory values, it was spontaneously reported in the data collection form.
Although a drug-drug interaction checker was used, the severity scores were not assessed, and DRPs may have been underreported due to limited lab monitoring or lack of therapeutic drug monitoring (TDM), particularly for antibiotics. The observational nature of this study along with lack of clinician intervention also precludes conclusions regarding DRP resolution or clinical outcomes. Additionally, factors such as the patient's nutritional status were not considered, which might have influenced the DRP's outcomes.
Conclusion
DRPs were highly prevalent among pediatric patients admitted to the pediatric haemato-oncology ward, and their underlying causes were clearly identified. Treatment safety issues were the most frequently observed DRPs, with inappropriate drug selection emerging as a major contributing factor. The unavailability of prescribed medications was also recognized as a significant subdomain cause. Anti-infective agents for systemic use were most frequently involved in DRPs, followed by antineoplastic and immunomodulating agents. Overall, these findings highlight the urgent need to integrate clinical pharmacy services into pediatric oncology units within cancer-specialized hospitals in Nepal. Strengthening clinical pharmacy involvement could significantly enhance medication safety and improve therapeutic outcomes for pediatric cancer patients.
Supplemental Material
sj-docx-1-opp-10.1177_10781552261437734 - Supplemental material for Drug-related problems among pediatric patients with cancer admitted to the pediatric haemato-oncology department: A prospective observational study
Supplemental material, sj-docx-1-opp-10.1177_10781552261437734 for Drug-related problems among pediatric patients with cancer admitted to the pediatric haemato-oncology department: A prospective observational study by Nabin Pathak, Bijaya Basyal, Shreya Dhungana, Aman Kumar Sah, Rajeev Shrestha, Sunil Shrestha, Anjali Pandit, Puskar Kunwor and Renu Karki in Journal of Oncology Pharmacy Practice
Footnotes
Acknowledgements
This work was presented as a poster at the Gandaki University International Conference 2024 with a theme of empowering excellence: Global Collaboration in Research and Academia conducted on January 03–05, 224, organized by Gandaki University, Nepal. The authors are indebted to Dr Hari Prasad Dhakal, Senior Consultant Pathologist and Dr Murari Man Shrestha, Senior Medical Epidemiologist, members of the ethical review board of NCHRC, Harisiddhi, Lalitpur, Nepal, for granting permission to conduct my research on their esteemed organization. The authors would like to sincerely thank Ms. Bimala Bhatta, Director of the School of Health and Allied Sciences, for permitting us to conduct our project work. The authors are very much obliged to Dr Punam Gauchan, Program Coordinator, Master of Pharmaceutical Sciences, School of Health and Allied Sciences, Pokhara University, for her support throughout the research. Lastly, the authors sincerely thank Ms. Urina Shrestha, Senior Nursing Officer of NCHRC, for supporting and helping me with the data collection.
ORCID iDs
Ethical clearance
Ethical approval was obtained from the Institutional Review Committee (IRC) of Pokhara University Research Centre (Ref no- 143/079/080).
Patient's/guardian consent
Pediatric patients diagnosed with confirmed cases of cancer admitted to the pediatric haemato-oncology ward of NCHRC and a caregiver or LAR were asked to give written consent along with patient's written or verbal assent to enroll in the study as per the National ethical guidelines 2022.
Author's contribution
NP conceptualized the idea. NP prepared the first draft of the manuscript. BB, SD later joined and helped in the preparation of the manuscript with contents and comments. NP entered the data and analyzed it. BB, SD cross-checked and made final corrections. AKS critically revised the manuscript. RS and SS made critical contributions to the manuscript and through the conception period. AP made substantial contribution through discussion during the study. PK provided clinical pharmacy expertise and co-supervised the study. RK supervised throughout the study. All authors had a final consensus on the latest version of the manuscript.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Data availability statement
The data for this study involves a small number of participants from a vulnerable population and contains indirect identifiers (e.g., sex, ethnicity, location) that may risk participant re-identification. Therefore, the dataset cannot be made publicly available. Researchers who meet the criteria for access to confidential data may submit requests to the Institutional Review Committee, Pokhara University, Nepal via email at puirc@pu.edu.np or through their official webpage: ![]() . All data will be stored securely at Pokhara University and will be accessible through the Institutional Review Committee to ensure long-term availability, even if study authors are unavailable.
. All data will be stored securely at Pokhara University and will be accessible through the Institutional Review Committee to ensure long-term availability, even if study authors are unavailable.
Supplemental material
Supplemental material for this article is available online.