
Abstract
Background
Although the role of pharmacists in pediatric oncology is well established, scientific production explicitly characterizing the services provided in this field remains limited.
Objective
To map studies on pharmaceutical services in pediatric oncology.
Methods
A scoping review was conducted in accordance with the JBI Manual for Evidence Synthesis and reported following the PRISMA-ScR Checklist. A systematic search was performed in September 2024 across six electronic databases, gray literature, and reference lists of selected studies. Eligible studies included original research and systematic reviews addressing pharmaceutical services in pediatric oncology. Two researchers independently assessed eligibility and extracted data, which were presented descriptively.
Results
Twenty-two articles were included, of which 86.4% (n = 19) were conducted in countries with a very high or high Human Development Index (HDI). Most studies were carried out in hospitals (86.4%; n = 19), with inpatient care being the most frequently addressed setting (54.6%; n = 12). The pharmaceutical services described mainly focused on pharmacotherapy follow-up (46.4%), followed by prescription analysis (18.2%) and compounding of antineoplastic agents (18.2%). In 72.7% (n = 16) of the studies, services were offered in autonomy. Regarding outcomes, 68.2% (n = 15) focused on clinical endpoints. Observational studies predominated (91%; n = 20).
Conclusion
The most frequently identified pharmaceutical services in pediatric oncology were pharmacotherapy follow-up, prescription analysis, and compounding of antineoplastic agents, generally provided autonomously within hospital and outpatient settings. These findings highlight the relevance of pharmacists’ role in this field while underscoring the need for more interventional studies evaluating clinical and economic outcomes.
Importance and relevance statement
This study is highly relevant as it maps the scientific production on pharmaceutical services in pediatric oncology, a field where pharmacists’ roles are recognized but still poorly characterized. The results show that most research was conducted in high-HDI countries, predominantly in hospitals, focusing on pharmacotherapy follow-up, prescription analysis, and compounding of antineoplastic agents, usually provided autonomously. In real-world practice, these findings reinforce that pharmacists are not merely technical executors but essential agents for safety, adherence, and quality of life in children undergoing cancer treatment, highlighting gaps and opportunities for more integrated and transformative practices.
Introduction
Childhood and adolescent cancer comprises a group of diseases characterized by the proliferation of neoplastic cells in the pediatric population. In Brazil, 91,233 children were affected between 2000 and 2022. 1 Although there are still discussions and differences regarding the definition of age range, the most accepted and widely used criterion in the scientific literature categorizes childhood cancer as malignant disease occurring from birth to 19 years of age, based on the similar types, clinical findings, and histological characteristics of neoplasms within this age group. 2 Even though it represents a relatively low percentage compared to adult cancer, childhood cancer requires significant efforts toward the development of policies and the structuring of healthcare services to ensure early diagnosis and appropriate treatment, as it remains one of the leading causes of death in this age group and is projected to increase in incidence. 3
Pediatric oncology encompasses efforts in diagnosis, treatment, and research related to childhood and adolescent cancer. Cancer illness requires long-term treatments with significant impacts on the lives of patients and those accompanying them throughout the oncological journey. In this context, the importance of multidisciplinary follow-up is emphasized to ensure comprehensive care for the diverse needs of pediatric patients and their families. 4
Moreover, this field involves two sensitive aspects directly related to patient safety: oncology medications and pediatrics. Most oncology drugs have a narrow therapeutic index, high treatment costs, and are frequently associated with reports of adverse events. 5 Pediatric practice presents additional challenges due to the extreme age range, the limited availability of clinical studies, and the different stages of physiological development, which imply relevant pharmacokinetic variations. These factors make the pediatric population particularly vulnerable to the use of medications outside package insert specifications, which may even result in adverse events.5–7
Oncological treatment is complex and permeated by intensive pharmacotherapy. To provide both access to medicines and clinical pharmaceutical follow-up activities for children and their families, pharmacists working in pediatric oncology employ pharmaceutical interventions through technical and clinical activities. Thus, to contribute effectively, pharmacists perform services that range from ensuring the quality of medicines to clinical monitoring of patients. Overall, the literature highlights the effective contribution of pharmacists as promoters of patient safety, cost optimization, prevention, and resolution of drug-related problems.8,9 Nevertheless, despite the growing role of pharmacists in pediatric oncology, the diversity of practices reported in the literature hinders the identification of a clear scenario regarding the services performed, how they are implemented, and what their contributions are to clinical, economic, and humanistic outcomes. Accordingly, the objective of this scoping review is to map studies on pharmaceutical services provided in pediatric oncology.
Methods
This scoping review was planned and conducted in accordance with the recommendations of the JBI Manual for Evidence Synthesis for Scoping Reviews and reported following the criteria of the Preferred Reporting Items for Systematic Reviews and Meta-Analyses extension for Scoping Reviews (PRISMA-ScR) Checklist (Appendix 1). The protocol was registered in the Open Science Framework (OSF) under the number 10.17605/OSF.IO/36YNS.10–12
A preliminary search was carried out in the Scopus, EMBASE, and MEDLINE databases to identify similar published and ongoing studies. One study published in 2023 was found, which aimed to describe clinical pharmacy activities in oncology reported in the literature. 13 Therefore, the present study innovates by broadening the scope to pharmaceutical services beyond clinical pharmacy and specifying them within the context of pediatric oncology.
Research question
The formulation of the research question was guided by the PCC acronym – Population, Concept, and Context.10,11
Population: Pharmacists working in Pediatric Oncology. Concept: Studies on pharmaceutical services in Pediatric Oncology, whether provided in autonomy or in collaboration with multidisciplinary teams. Pharmaceutical services were considered to include technical and clinical management of medicines, such as pharmaceutical care services (selection, planning, procurement, storage, distribution/dispensing), clinical pharmacy practice (pharmacotherapy follow-up, therapeutic drug monitoring, prescription analysis, and pharmacotherapy review), health education, compounding of antineoplastic agents, pharmacovigilance, pharmacoeconomics, clinical research, participation in multidisciplinary teams, and institutional committees.14–16 Context: Pediatric oncology, defined as the specialized area of healthcare services that provides care to pediatric oncology patients/oncology patients aged 0 to 19 years, through multiple care centers at primary, outpatient, and/or hospital levels.
17
Based on this framework, the guiding research question was formulated: “What pharmaceutical services are provided in Pediatric Oncology?”
Search strategy
A systematic search was conducted in September 2024 in the following electronic databases: Cochrane Central Register of Controlled Trials (CENTRAL), EMBASE, Latin American and Caribbean Center on Health Sciences (LILACS), MEDLINE (via PubMed), SCOPUS, and Web of Science. Additionally, gray literature was consulted through ProQuest Dissertations & Theses and the Catalog of Theses and Dissertations of the Coordination for the Improvement of Higher Education Personnel (CAPES). Furthermore, the reference lists of the included studies were manually screened for additional relevant studies.
The search strategy was developed and aligned with the study objective and research question, resulting in terms encompassing “Pharmaceutical Services,” “Pharmacists,” “Oncology,” and “Pediatrics.” These concepts were selected to achieve a balance between sensitivity and specificity, ensuring the retrieval of articles capable of answering the research question. Medical Subject Headings (MeSH), Embase Subject Headings (Emtree), and Health Sciences Descriptors (DeCS) were used to define descriptors and their synonyms. Relevant keywords already used in scientific publications, but not yet indexed as descriptors, were also included. The entire search strategy was adapted to the operational specificities of each database. Appendix 2.
Eligibility criteria
Inclusion criteria: Studies addressing pharmaceutical services provided in pediatric oncology/to oncology patients aged 0 to 19 years were included. Eligible studies comprised original research, such as interventional studies, observational studies, systematic reviews, and research reports in the field, published in English, Portuguese, or Spanish, regardless of the year of publication.
Exclusion criteria: Studies addressing different age groups without specificity for the 0–19 age range, studies that did not clearly present pharmaceutical services, and/or studies that did not directly address pediatric oncology were excluded. Additionally, studies not available in full text, knowledge assessment studies, drug utilization studies, letters to the editor, clinical trial protocols, and scientific event materials (abstracts and posters) were excluded.
Study selection
This stage was divided into three phases:
Phase 1: Records retrieved from the databases (based on the individual search strategies of each source of information) were stored in the Rayyan® reference manager. Duplicate records were removed, and a title and abstract screening was performed according to the eligibility criteria. Phase 2: Title and abstract screening was conducted independently by two researchers and supervised by a third one to resolve potential disagreements. Full-text reading of the studies was then performed to assess eligibility based on the established criteria. Phase 3: Full-text reading of the studies selected in Phase 2 was carried out independently by two researchers and supervised by a third one to resolve disagreements. Additionally, the reference lists of the selected studies were manually screened by one researcher to identify further eligible studies for this review.
For articles that were not available in full for reading, an email was sent to the respective authors, and in the absence of a reply within 20 days, they were considered full text were not available.
Prior to Phases 2 and 3, the researchers conducted a pre-test (analysis of the first 20 records) to calibrate their interpretation of the eligibility criteria.
Data extraction and analysis
A data collection instrument was developed and underwent a pilot test for standardization (conducted independently by two researchers) using the first ten selected articles, to validate its functionality and adjust it according to identified needs prior to the beginning of data extraction. After the pre-test, data collection was carried out independently by two researchers and supervised by a third one to resolve disagreements.
The variables collected included: Author, Year, Country, Title, Objective, Study design, Pharmacist involvement, Funding source, Setting, Patient care regimen, Type of pharmaceutical service provided, Service description and Type of outcomes. In the data collection instrument, the studies were numbered to allow referencing during the discussion of results.
Data were presented descriptively through figures and tables, using absolute and relative frequencies. In line with JBI recommendations, no methodological quality assessment of the eligible studies was performed for inclusion in this scoping review.
Results
A total of 1548 records were retrieved from electronic databases and gray literature, of which 22 were included in this review. The details of the search, identification, and selection process are described in Figure 1.
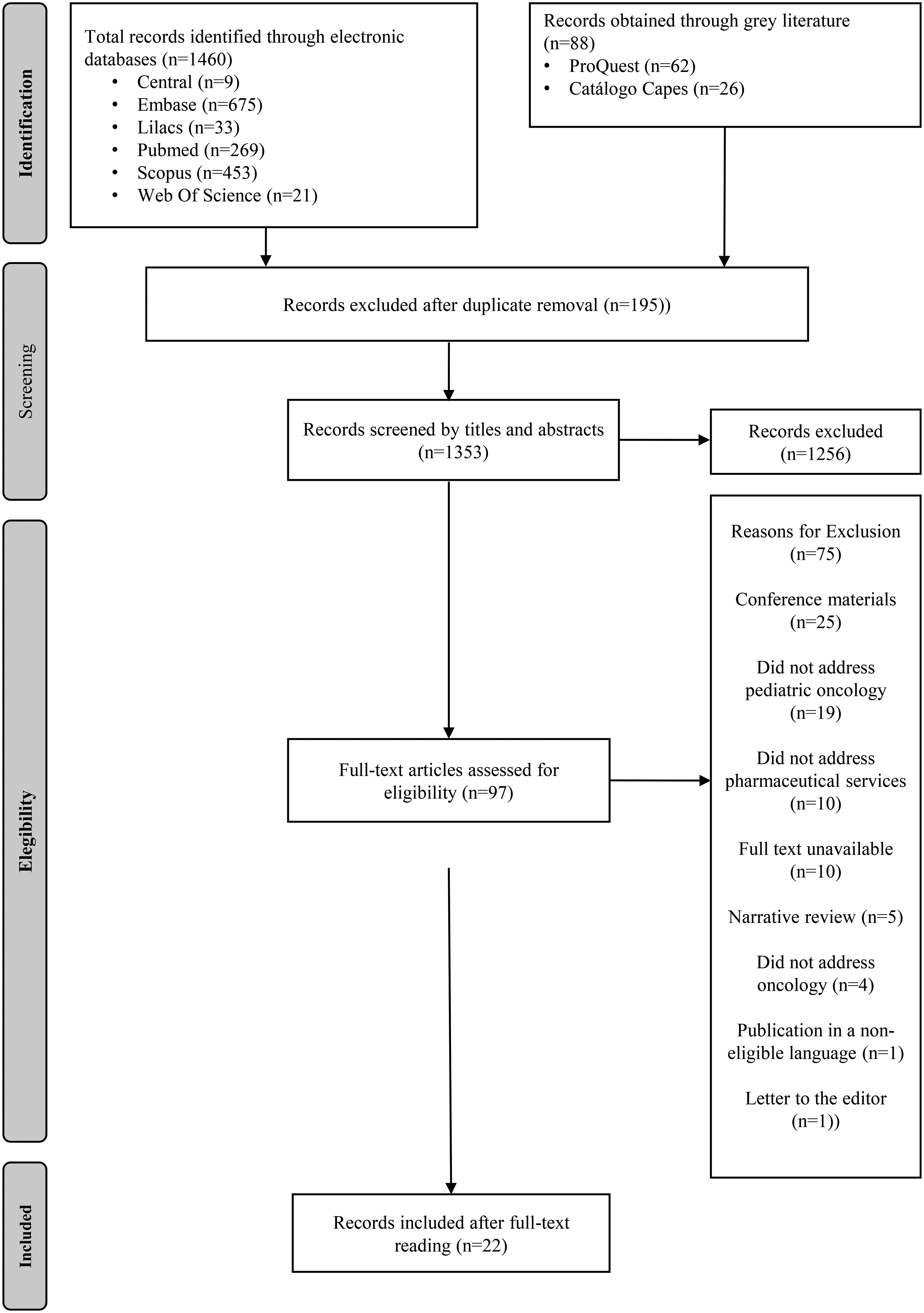
Flow diagram with the results of the study selection stage. Adapted from the Preferred Reporting Items for Systematic Reviews and Meta-Analyses extension for Scoping Reviews (PRISMA-ScR) Checklist.
Characteristics of the selected studies
The publications included in this review covered the period from 1976 to 2024, with most (59%; n = 13) concentrated between 2018 and 2024. Only 13.6% (n = 3) were published before 2000. Brazil stood out as the country with the highest number of publications within the analyzed scope, representing 22.7% (n=5) of the included studies, as presented in Appendix 3. Based on the Human Development Index (HDI), 86.4% (n=19) of the studies were conducted in countries with a “very high” or “high” HDI, such as the United States, Canada, and France. 18
Among the objectives proposed by the selected studies, the most frequent were: characterization of the profile of pediatric oncology patients, identification of the most common types of pharmaceutical interventions performed, mapping of medicines with the greatest potential risk to the safety of this population, and, more generally, description of pharmaceutical practice in pediatric oncology centers.
Most of the selected studies (91%; n = 20) were observational. Only one study (4.5%; n = 1) corresponded to a systematic review, while another (4.5%; n = 1) did not describe the planned study design. Among the pharmaceutical services identified, 72.7% (n = 16) were autonomy. The most frequently reported services were pharmacotherapy follow-up (46.4%; n = 10), prescription analysis (18.2%; n = 4), and compounding of antineoplastic agents (18.2%; n = 4). Other services described included technical management of the medication supply chain, health education activities, and pharmacovigilance initiatives.
Most of the studies (68.2%; n = 15) highlighted the pharmacist's contribution to clinical outcomes. Contributions to technical outcomes were observed in 13.6% (n = 3), to combined technical-clinical outcomes in 13.6% (n = 3), and to clinical-financial outcomes in 4.6% (n = 1).
Regarding the setting in which services were delivered, the majority of studies (86.4%; n = 19) were conducted in hospitals, while the remaining 13.6% (n = 3) took place in outpatient clinics. The most frequently addressed care regimen was inpatient care, present in 59.2% (n = 13) of the studies. In 22.7% (n = 5), pharmaceutical services were evaluated in both inpatient and outpatient populations. Only 13.6% (n = 3) focused exclusively on outpatient care, while 4.5% (n = 1) did not specify the care regimen.
Regarding the funding models of the healthcare services in which pharmaceutical services in oncology were provided, philanthropic (13.6%), public (13.6%), and public–private (9.9%) models predominated, while the remaining studies did not report this information.
The characteristics of the selected studies are detailed in Table 1, available in the supplementary material.
Discussion
Overall, this scoping review identified that the main pharmaceutical services performed in pediatric oncology are pharmacotherapy follow-up, prescription analysis, and compounding of antineoplastic agents, in addition to activities such as medication supply chain management, pharmacovigilance, and health education. These findings highlight the multifaceted role of the pharmacist in this field, as these services encompass administrative, clinical, and mixed dimensions. This is an inherent characteristic of the profession, in which pharmacists are often engaged in administrative activities and responsible for the medication supply chain within healthcare services. These responsibilities of oncology pharmacy include stages such as selection, planning, procurement, storage, distribution, compounding, administration, monitoring of use, and pharmacovigilance. In this sense, the significant presence of pharmacists in different stages of care demonstrates their multifaceted role in promoting the safety and effectiveness of pharmacotherapy in pediatric oncology patients. 19
The predominance of pharmacotherapy follow-up among the clinical services provided can be justified by its broad consolidation in other clinical contexts and health conditions. Although in pediatric oncology there is still no robust evidence of efficacy, effectiveness, and efficiency for this service, it is widely recognized in the literature as a structured practice, with well-documented impacts on clinical, economic, and humanistic outcomes across diverse populations, diseases, and levels of healthcare. 20 This fact may positively influence the adoption of this service in the field of pediatric oncology, particularly given the need for longitudinal follow-up of these patients due to the complexity of pharmacotherapy and the high risk of preventable adverse events. 9
Among the other most frequently reported services, prescription analysis and compounding of antineoplastic agents are considered critical steps in the context of pediatric oncology, particularly due to the complexity of therapeutic regimens involving the main drugs used.8,21 Treatment with antineoplastic agents is often medium to long-term, consisting of multiple cycles with significant variations in doses, routes of administration, and combinations with other medications. Many of these agents are cytotoxic, costly, and require specific compounding procedures, which increases the need for technical rigor and quality control. 22
In pediatric oncology, the role of the oncology pharmacist in the management of antineoplastic drug compounding involves several critical considerations aimed at preventing medication errors. This is largely due to the need for strict dose individualization, typically calculated based on the child's body weight or body surface area, which frequently results in very small preparation volumes and requires highly precise dilutions to ensure therapeutic safety and efficacy. Beyond thorough prescription validation—including verification of doses, treatment duration according to pediatric protocols, confirmation of the correct route of administration, as well as the volume, concentration, and infusion rate of the compounded medication clinical pharmacy practice should also ensure the appropriate prescription of supportive therapies and the monitoring of relevant laboratory parameters. In pediatric oncology compounding, additional technical challenges arise, such as the adjustment of the final preparation volume and the consideration of the internal volume of the infusion set relative to the total volume of the infusion bag, which may affect the actual dose delivered in low-volume infusions. Given the narrow therapeutic index of most antineoplastic agents and the complexity of pediatric oncology treatment regimens, the active involvement of the pharmacist in the processes of prescription validation, preparation, and therapeutic monitoring is essential to reduce medication errors, minimize adverse events, and ultimately improve clinical outcomes in pediatric patients receiving chemotherapy.8,21
Thus, through the application of knowledge in pharmaceutics, pharmacokinetics, and individualized dose calculations, pharmacists play an essential role in the overall therapeutic process, optimizing pharmacotherapy, strengthening effectiveness and safety, and contributing to cost rationalization for both patients and healthcare systems. 23
Most of the studies analyzed pharmaceutical services autonomously, that is, without highlighting the integration of pharmacists into the multidisciplinary team. A justification for this analytical pattern may lie in the objectives of the selected studies, which prioritized the description of pharmacists’ specific activities—such as the types of pharmaceutical interventions performed, the medicines with the greatest potential risk in pediatric oncology, and the characterization of the patients treated, among others. In this sense, although the studies sought to describe the contribution of pharmacists individually, it is well known that, in practice, they work in collaboration with other healthcare professionals, particularly within the complex context of pediatric oncology. 24
About the setting of service delivery, most of the selected studies were conducted in hospital environments, with a predominance of inpatient care. This finding is consistent with the clinical profile of pediatric oncology, which requires intravenous chemotherapy—complex and toxic—thus demanding hospitalization for continuous monitoring and multiprofessional support. 25 In contrast, the scarcity of studies focusing on pharmaceutical practice in outpatient settings reveals a scientific and practical gap in a model of care that has to be expanded. The availability of oral chemotherapy in outpatient environments has become increasingly feasible in oncology. 26 In this context, investments in studies, protocols, and policies that broaden the pharmacist's role beyond inpatient care are imperative.
The study designs used in the selected studies are predominantly observational. This finding is consistent with the reported objectives, which focused on describing practices, mapping services functioning, characterizing pharmaceutical interventions, and outlining patient profiles. Although this type of study contributes to portraying the reality of services and generating relevant hypotheses, there is a clear scarcity of interventional studies assessing the clinical, economic, and humanistic impacts of pharmaceutical services in the context of pediatric oncology. In contrast, it is important to recognize that conducting such studies in children and adolescents faces significant ethical barriers.27,28 Therefore, a promising and necessary path to strengthen the scientific basis of pharmaceutical practice in pediatric oncology is to discuss alternatives that balance bioethical issues with experimental scientific methods in this context. In addition, encouraging the active participation of pharmacists in ethics committees and multidisciplinary teams ensures shared and transparent decision-making, balancing scientific rigor with patient protection, while cost-effectiveness studies safeguard justice and sustainability within healthcare systems.
The analysis of the pediatric population profile included in the studies revealed a predominance of patients with hematological neoplasms, notably leukemias and lymphomas, which represent the most frequently reported neoplasms in children and adolescents. 2 Thus, it is evident that the focus of pharmaceutical services in pediatric oncology reflects the epidemiological reality and reinforces the need for specific training to address this profile. This contributes not only to aligning practices with the most prevalent demands but also to expanding the potential clinical impact in this area.
With regard to the technical and financial outcomes observed, they play a relevant role in the evaluation and sustainability of pharmaceutical services, as they represent structuring stages that support and allow the clinical practice of the profession. Correr, Otuki, and Soler (2011) emphasize, in the logical-conceptual model of pharmaceutical care integrated into the healthcare process, that access to medicines of adequate quality, in the right quantity, and at the correct time is an indispensable condition for therapeutic effectiveness and patient safety. 16 In this sense, a strategic step to strengthen the operational basis of services and allow the expansion and qualification of more resolutive and sustainable clinical activities in pharmaceutical care in pediatric oncology is to invest in technical and financial outcomes. 26
The authors acknowledge that this work is not free from limitations. It is possible that relevant studies—such as those addressing pharmaceutical services in less explored contexts, particularly radiotherapy or oncological surgery—were not captured within the sensitivity of the systematic search. Nevertheless, the mapping of the retrieved literature allowed for consistent reflections aligned with the research question, consolidating the originality of this review.
Additionally, by synthesizing the diversification and expansion of pharmaceutical services in pediatric oncology, the findings of this review provide valuable insights for managers, researchers, and healthcare professionals interested in qualifying these services. To consolidate the scientific production on the subject, it is necessary to promote interventional studies that investigate the clinical, economic, and humanistic effects resulting from pharmaceutical practice in pediatric oncology.
The framework of this present scoping review, focused on mapping the oncology pharmacy in pediatric oncology, allowed us to identify the main services evidenced: pharmacotherapy monitoring, prescription analysis, manipulation of antineoplastic agents, supply chain management, pharmacovigilance, and health education. These activities can be associated with administrative, clinical, and mixed dimensions of pharmaceutical care for children and adolescents with cancer. It is also understood that these services are the most frequently performed, as they assume a central role in pediatric oncology due to the complexity of therapeutic regimens, the need for rigorous dose individualization, and the technical challenges related to the preparation and administration of antineoplastic drugs.
Conclusion
This review reports that pharmaceutical services in pediatric oncology are concentrated in hospital-based clinical, technical, and administrative activities, with a predominance of observational studies from high-HDI countries. The findings confirm consolidated practices but reveal a scarcity of interventional research and limited evidence from lower-development contexts, highlighting the need for broader investigations and strategies to strengthen pediatric oncology pharmacy.
Supplemental Material
sj-docx-1-opp-10.1177_10781552261444975 - Supplemental material for Pharmaceutical services in pediatric oncology: A scoping review
Supplemental material, sj-docx-1-opp-10.1177_10781552261444975 for Pharmaceutical services in pediatric oncology: A scoping review by Jordânia Ferreira Martins, João Pedro Vasconcelos Paolinelli, Ricardo Augusto dos Santos Silva and Mariana Linhares Pereira in Journal of Oncology Pharmacy Practice
Footnotes
Acknowledgments
The authors would like to express their sincere gratitude to the Coordenação de Aperfeiçoamento de Pessoal de Nível Superior (CAPES – Finance Code 001), the Federal University of São João del-Rei (UFSJ), and the Postgraduate Program in Pharmaceutical Sciences (PPGCF) for their valuable support in the development of this work.
ORCID iDs
Author contributions
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by the Coordenação de Aperfeiçoamento de Pessoal de Nível Superior, (grant number 001).
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.