
Abstract
Introduction
The complexity of chemotherapy protocols and the narrow therapeutic index of anticancer drugs make the risk of medication errors particularly high in oncology. This study analyzed and categorized pharmaceutical interventions related to chemotherapy prescriptions in a clinical hematology center.
Methods
This study was conducted in a specialized clinical hematology center over a defined study period (16 months). All chemotherapy prescriptions validated by clinical pharmacists were reviewed. Validation was performed according to both regulatory and scientific criteria. Identified therapy-related problems were discussed with physicians, and all pharmaceutical interventions were recorded and classified according to the ReMeD severity scale.
Results
A total of 6186 chemotherapy prescriptions were analyzed, leading to 117 pharmaceutical interventions. The most common errors involved dosage errors (n = 51;49.03%), omission of prescription (n = 23;22.11%) and incorrect treatment duration (n = 11;10.57%). Most interventions were rated as having a major clinical impact, particularly those preventing omission and posology errors, ensuring optimal chemotherapy management and patient safety. All interventions were accepted by physicians, highlighting strong interdisciplinary collaboration.
Conclusion
Pharmaceutical interventions represent a key component in improving the safety and quality of chemotherapy management. Strengthening the pharmacist's integration into oncology teams ensures better therapeutic outcomes, reduces medication-related risks, and supports a culture of safe and evidence-based cancer care.
Introduction
Anticancer chemotherapy has revolutionized cancer management over the past fifty years. Chemotherapy involves using cytotoxic drugs that can destroy cancer cells or slow their growth. However, these drugs have a narrow therapeutic index and can cause serious, sometimes life-threatening toxicity. Therefore, every step of the chemotherapy process, from prescription to administration, is considered critical and requires close collaboration between doctors, pharmacists and nurses to ensure patient safety. It's estimated that 1–3% of all chemotherapy prescriptions involve some type of error. 1
The rise of clinical pharmacy has helped optimize treatment management at every stage of the care pathway. As a patient-centered discipline, it strengthens the safety, appropriateness, and efficiency of medication use. In oncology, clinical pharmacy plays a key role in the overall care of cancer patients. According to the International Society of Oncology Pharmacy Practitioners (ISOPP), the oncology pharmacist plays an essential role within the multidisciplinary care team. With their specialized expertise, oncology pharmacists contribute directly to improving care quality and reducing medication-related risks. 2
A study conducted in Japan demonstrated the impact of oncology pharmacists in improving medication safety and optimizing anticancer treatments. 3 Similarly, a literature review, including studies conducted between 1990 and 2014, found that pharmacists in oncology have a generally positive impact on patient outcomes. 4 However, it also highlighted the variability in results, reflecting the heterogeneity of pharmacist practices. These can differ internationally, nationally, locally, and even individually, in the absence of a well-standardized methodology for chemotherapy treatment validation.
The aim of this study was to analyze pharmaceutical interventions associated with chemotherapy prescriptions in a clinical hematology center by determining their nature, and severity according to the REMED classification, and to evaluate their contribution to improving prescription quality and patient safety.
Materials and methods
This was a retrospective, analytical, and interventional study conducted in a specialized clinical hematology center over a 16-month period (January 2024 - April 2025). Pharmaceutical interventions (PIs) related to chemotherapy prescriptions for patients with malignant blood disorders in the day hospital were included.
Hospitalized patients in other clinical departments as well as outpatients not receiving chemotherapy were excluded from the study.
Pharmaceutical validation criteria were based on two main aspects: regulatory validation (verification of patient identity, prescriber's signature, and stamp
A level 2 validation was implemented, focusing on verifying the consistency of prescriptions and the appropriateness of drug selection according to patient's chemotherapy regimen, dose accuracy, and conformity of the administration route. Biological parameters were also taken into account, including complete blood count, kidney and liver function, electrolyte balance, and coagulation tests.
During the pharmaceutical analysis, if a problem related to patient's therapy was identified, a PI was performed by the pharmacist after discussion with the attending doctor.
To ensure traceability, each PI was recorded on a classification form developed based on the model proposed by the SFPC. 6 The form included the following data: patient identity, diagnosis, identified problem, and the intervention performed.
All data were entered and analyzed using Microsoft Excel. The seriousness of identified problems was classified as minor, significant, major, critical, or catastrophic, according to the scale established by the Medication Error Review (ReMeD). 7
Results
Pharmaceutical analysis of chemotherapy prescriptions was systematically performed every morning on weekdays. Over the 16-month study period, 6186 prescriptions were reviewed and validated. Among these prescriptions, 117 pharmaceutical interventions (PIs) (1,72%) were recorded. The prescriptions reviewed were for patients treated for malignant blood disorders in the day hospital.
Detected errors were classified as follows:
-
Of the 117 recorded PIs, 13 (11.1%) were related to regulatory errors. Among these, 30.76% (n = 4) involved patient identification issues, 46.15% (n = 6) were due to the absence of the doctor's stamp, 15.38% (n = 2) involved crossed-out text, 7.69% (n = 1) were related to illegible handwriting. (Figure 1)
-
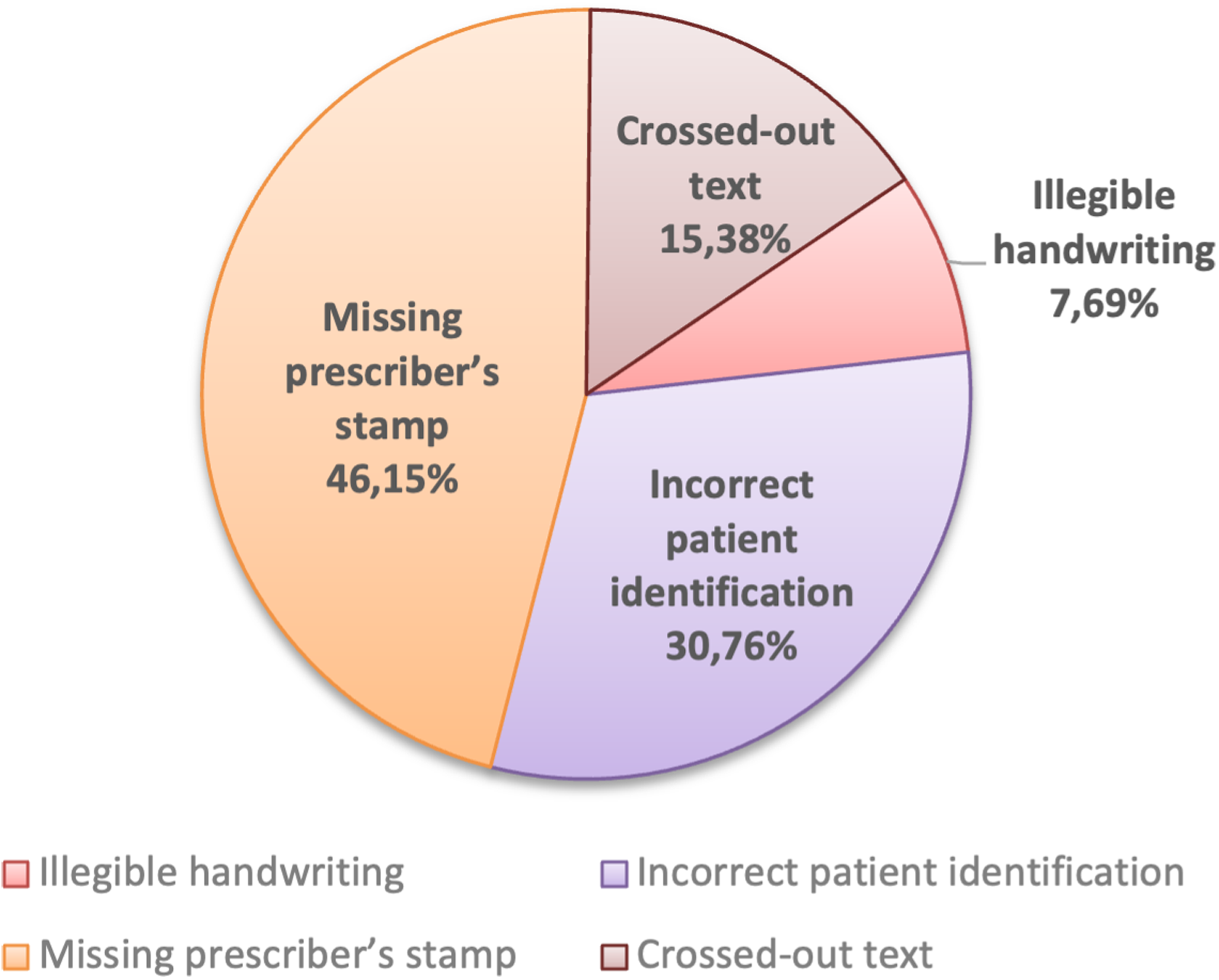
Distribution of regulatory validation errors in chemotherapy prescriptions.
A total of 104 PIs were related to medication errors. The most frequent were dosage errors (n = 51;49.03%), followed by omission of prescription (n = 23;22.11%), protocol errors (n = 10; 9.61%), incorrect treatment duration (n = 11;10.57%), non-compliant routes of administration (n = 8;7.69%), and date inconsistencies (n = 1;0.96%). (Figure 2)
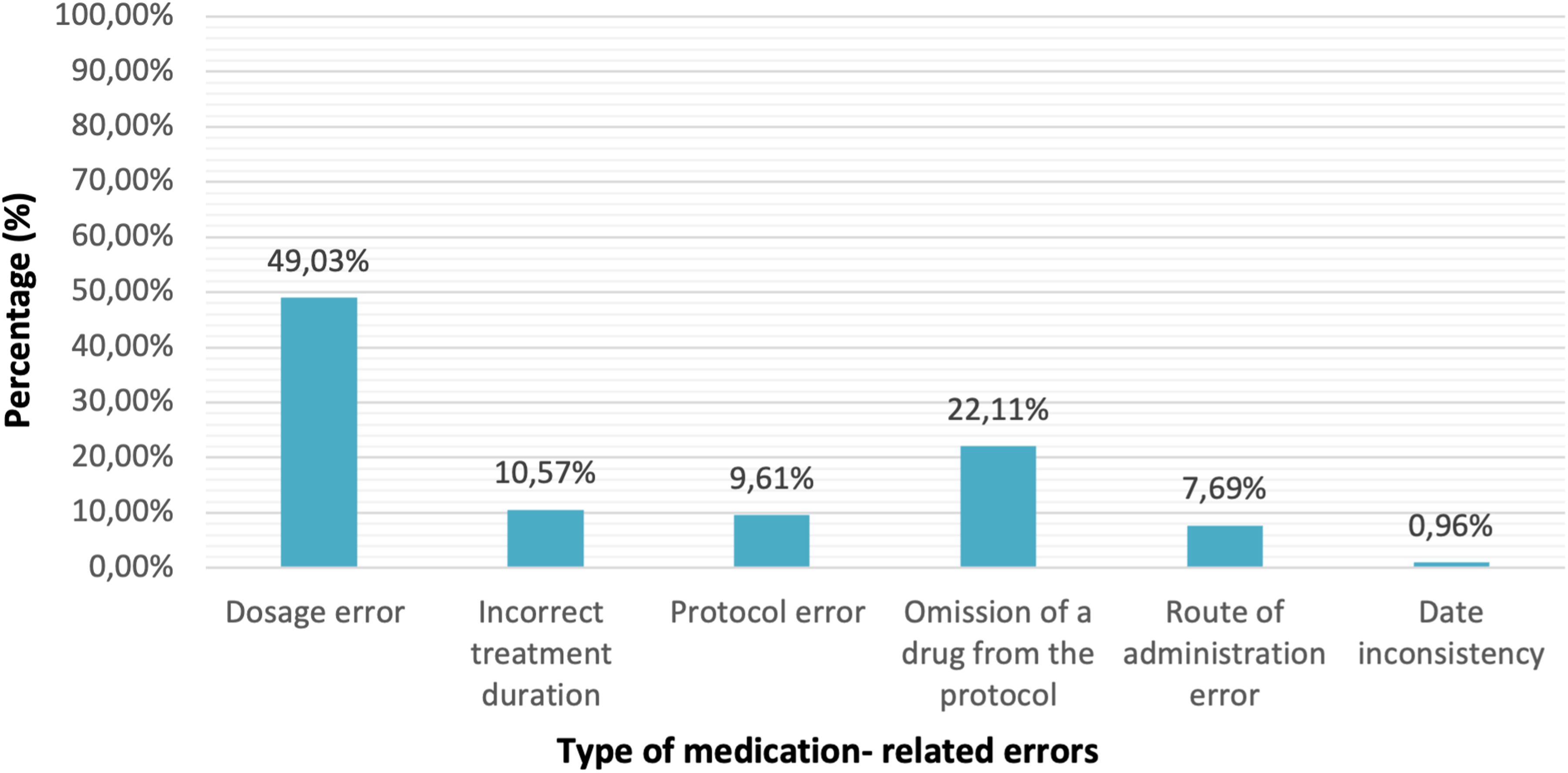
Distribution of medication-related errors.
Error classification according to the REMED scale
According to REMED classification established by the SFPC (7), 31 errors (29.8%) were minor (no clinical consequence for the patient), 2 errors (1.92%) were significant (required monitoring but without clinical consequence), 69 errors (66.34%) were major (temporary clinical consequences), and 2 errors (1.92%) were critical (permanent clinical consequences). (Figure 3)
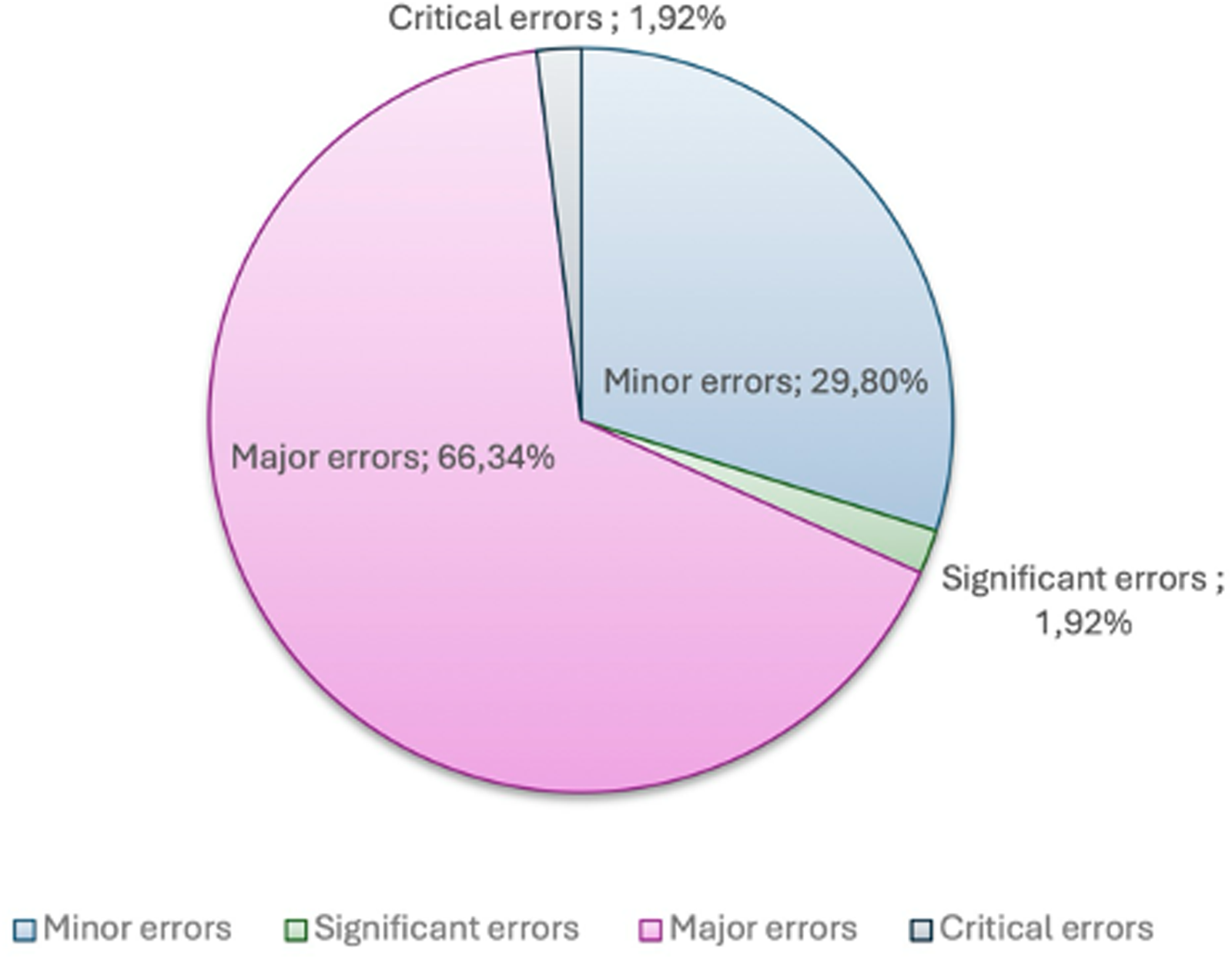
Distribution of medication errors according to the REMED classification.
Distribution of errors by mechanism of action of chemotherapy drugs.
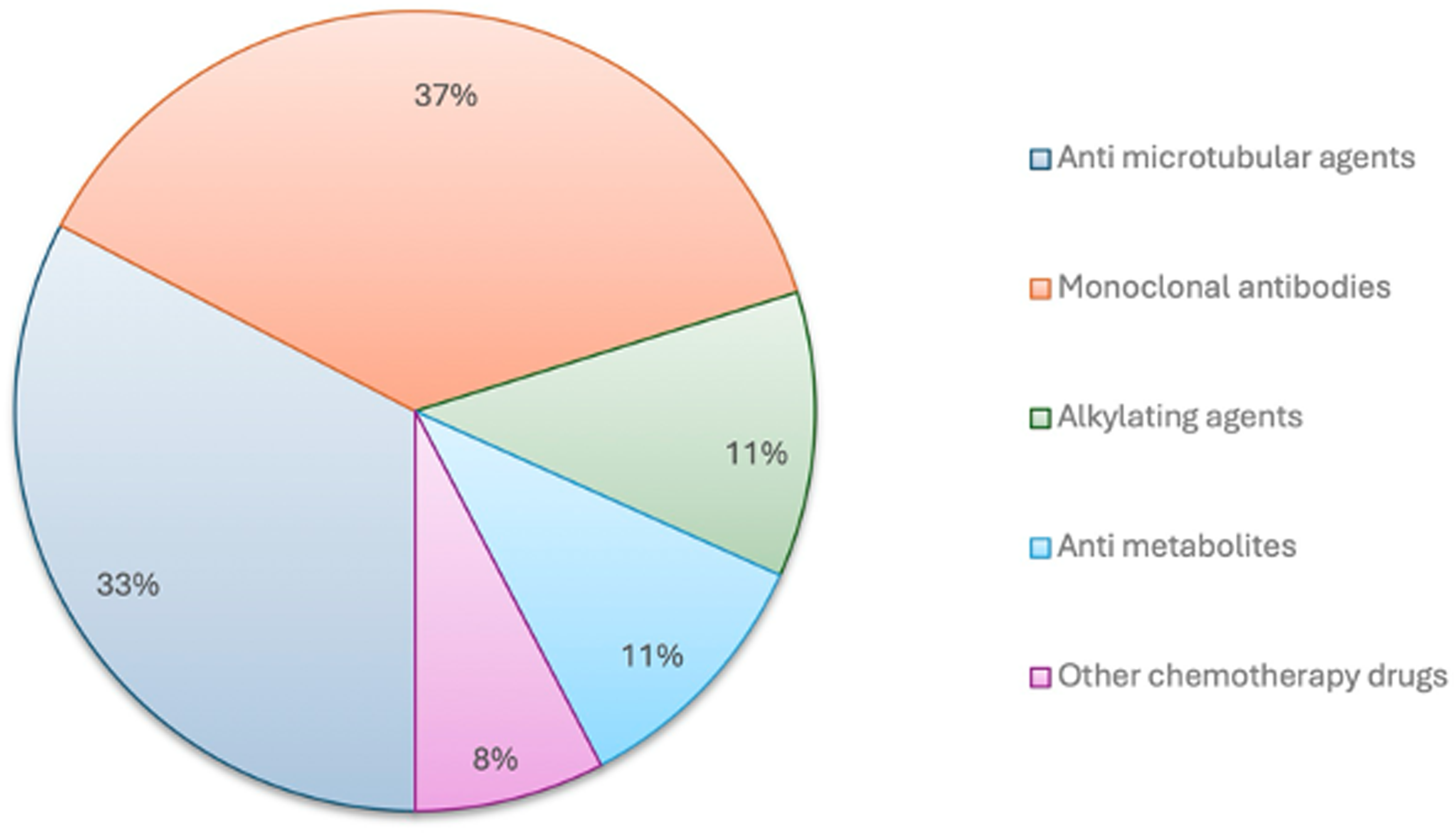
Distribution of PIs by prescribed anticancer drug class
PIs most involved Monoclonal antibodies (37%), Antimicrotubular agents (33%), Alkylating agents (11%), Antimetabolites (11%), and other chemotherapy drugs (8%). (Figure 4)
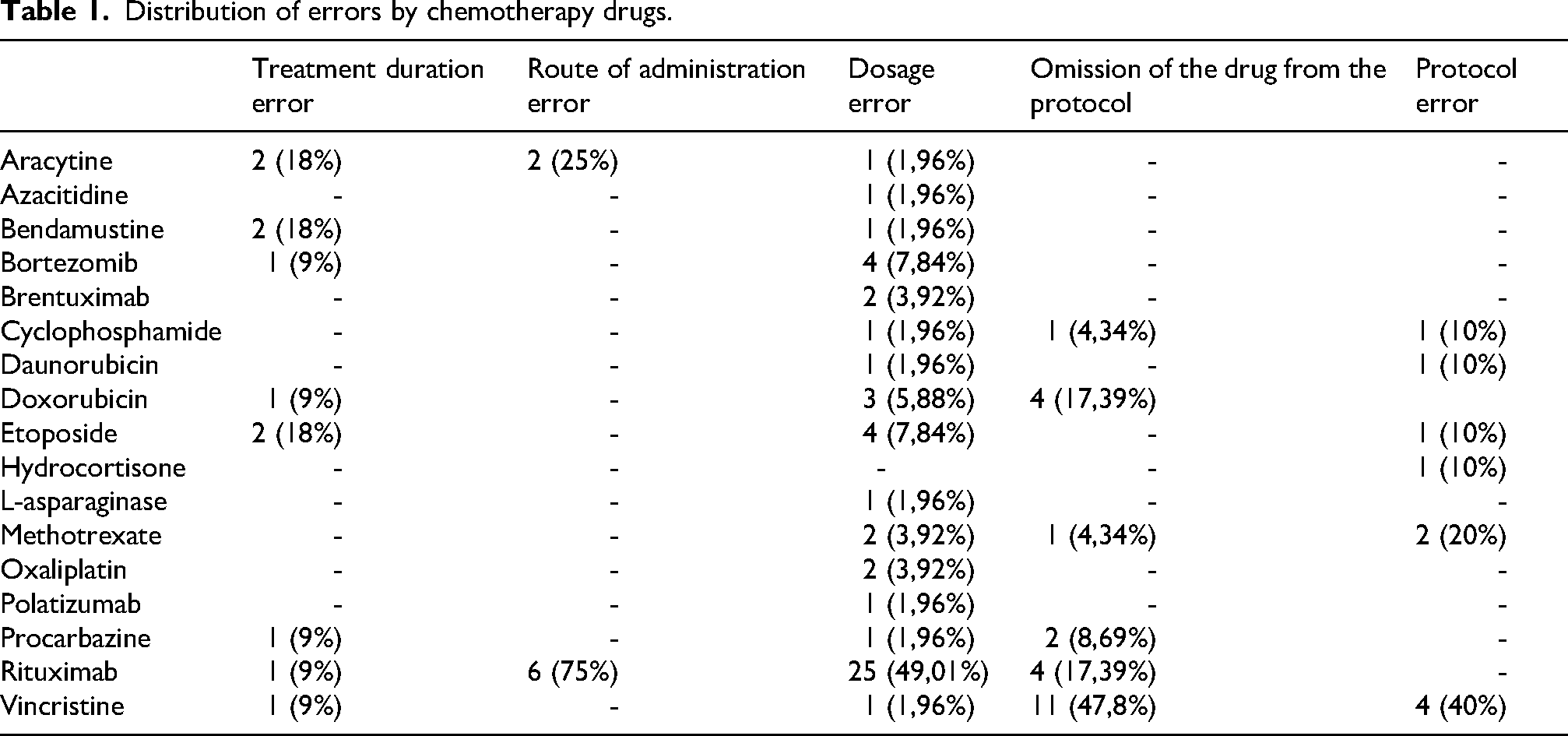
Table 1 illustrates the distribution of identified errors according to the chemotherapy drugs involved.
Distribution of errors by chemotherapy drugs.
Discussion
The chemotherapy process is a complex and highly sensitive workflow, involving multiple consecutive steps from prescription to patient administration. Given the high toxicity of anticancer drugs and inter-individual variability of treatment regimens, this workflow carries a particularly high risk of medication errors.
Pharmaceutical interventions play a critical role in ensuring quality patient care in chemotherapy. A retrospective review conducted between 2014 and 2015, at an academic, comprehensive cancer center, demonstrated that such interventions not only improve patients’ quality of life but also increase safety and optimize drug therapy. 8
During the sixteen-month study period, 117 of prescriptions (1,72%) contained errors that required pharmaceutical intervention. Currently, all chemotherapy prescriptions for patients treated in the day hospital are handwritten and not integrated into the pharmacy's computerized prescribing system. This may partly explain the high frequency of potential medication errors.
A Pakistani study in a chemotherapy unit showed that computerizing the chemotherapy workflow, in combination with a Clinical Decision Support System, significantly decreased both the frequency and seriousness of medication errors, improved dispensing and administration times, and decreased chemotherapy-related costs. 9
Additionally, a Failure Mode and Effects Analysis (FMEA) conducted across the entire complex chemotherapy workflow at a leading tertiary hospital in China identified 15 risk factors contributing to 10 failure modes during drug administration. Notably, the sub-process of writing medical prescriptions was particularly critical, with dose calculation errors, data entry mistakes, and missing essential patient information identified as major high-risk factors. Implementation of a Computerized Physician Order Entry (CPOE) system integrated with a Clinical Prescription Assistance System (CPAS) significantly decreased error rate from 1.47% to 0.20%, with CPAS preventing over 95% of errors in medical prescriptions. 10
Among the validated prescriptions, regulatory errors accounted for 11.1% of all recorded errors. In literature, several studies have reported noncompliance with legal prescription requirements. A retrospective audit of duplicate discharge prescriptions conducted in an urban teaching hospital in Cork, Ireland revealed 320 legal errors among 1156 prescriptions, corresponding to an error rate of 27%. 11 Additionally, a six-month cross-sectional audit conducted in a tertiary healthcare facility in southern India reviewed 4100 prescriptions and found that 60% lacked prescriber identification. 12
Throughout our study, aside from regulatory interventions, rigorous pharmaceutical validation was performed and revealed that 88.8% of the errors were medication related.
The most frequently observed type of medication error was dosage error (n = 51; 49.03%). These findings are consistent with data from the literature, where dosing errors are frequently reported as the most common in oncology.13–15 A study conducted by Mousavi et al. in the oncology departments of two Iranian university hospitals demonstrated dosage errors in 65% of interventions. 16 This can be explained by the complexity of treatment regimens and the need for dose adjustments based on individual parameters such as weight, body surface area, and laboratory results, particularly in cases of kidney disease.
Omission errors, referring to missing medications within chemotherapy regimens, were also frequent in our study (n = 23; 22.11%). The high rate of omission errors observed in our series also reflects the challenges encountered in strictly adhering to treatment regimens, especially in contexts with high workloads. 17
During this study, pharmaceutical interventions were classified according to the seriousness of consequence caused by medication errors as defined by REMED. More than half of the errors (n = 69; 66.34%) were considered major, leading to temporary clinical consequence for the patient. These results highlight the importance of systematic pharmaceutical validation of chemotherapy prescriptions as an essential safety barrier before administration.
A similar study on PIs in chemotherapy conducted in a Brazilian university hospital used a classification system different from that proposed by SFPC, 18 making direct comparison with our study difficult.
Analysis of prescription errors by cytotoxic drug revealed that monoclonal antibodies, and specifically Rituximab, were the most frequently involved in reported errors (n = 36; 34.6%). The two most frequent types of errors associated with this biological therapy were incorrect route of administration and inappropriate dosage. These errors are mainly explained by the complexity of treatment regimens and the multiple possible routes of administration (intravenous or subcutaneous). Confusion between these different regimens can lead to the selection of an inappropriate route or a dosing error.
Such errors may lead to significant clinical consequence, as rituximab has a narrow therapeutic index and may cause severe hypersensitivity reactions or therapeutic failure in cases of underdosing.
These findings are consistent with published data identifying rituximab as a high-risk drug for iatrogenic complications, largely due to its specific administration requirements and the variety of existing regimens.19,20 These results highlight the need for standardized prescribing practices, systematic pharmaceutical verification, and implementation of clinical decision support tools integrated into computerized prescribing systems to help prevent such errors.19–21
The second most frequently implicated drug class was antimicrotubule agents, including vincristine, etoposide, daunorubicin, and doxorubicin (n = 34; 32.7%). For vincristine, the most frequent issues were prescription omissions (drug omitted from the scheduled regimen) (n = 11; 47.8%) and regimen errors (n = 4; 40%), specifically discrepancies between the prescribed regimen and the reference treatment regimen. These types of errors often result from inattention during retranscription or unfamiliarity with specific treatment cycles, particularly in combination chemotherapy regimens. Other antimicrotubular agents, such as etoposide and anthracyclines (daunorubicin and doxorubicin), were mainly associated with dosing errors or missing details regarding infusion duration or volume, reflecting the complexity of their preparation.
The high frequency of errors involving these agents highlights the importance of strengthening pharmaceutical control at every step of the chemotherapy process—prescription, validation, preparation, and administration. Implementing a standardized checklist, electronic prescribing through a Computerized Physician Order Entry (CPOE) system, and continuous prescriber training are essential strategies to minimize these risks.
Our results confirm the relevance of a two-level pharmaceutical validation process, as recommended by SFPC. This approach not only enables a review of prescriptions but also facilitates identification of more complex therapeutic inconsistencies. Pharmacist's role, extending beyond simple dispensing, has become an integral part of the clinical care team.
This mission is fully aligned with international recommendations. ISOPP advocates for the full integration of pharmacists into multidisciplinary care teams to optimize the management of cancer patients. ISOPP also emphasizes the need to develop continuing education programs for oncology pharmacists and to implement certification systems that formally recognize their contributions to patient safety and quality of care. 2
In this context, strengthening specialized training and promoting clinical role of pharmacists represent key levers for improving both the quality and safety of the chemotherapy process.
This study is based on a large number of chemotherapy prescriptions analyzed over a 16-month period, providing a comprehensive and representative overview of real-world clinical practice in a hematology setting. The systematic implementation of a level 2 pharmaceutical validation ensured a thorough assessment of both regulatory and clinical aspects of prescriptions. Furthermore, the use of a standardized and validated classification system (REMED) allowed a structured evaluation of the severity of medication errors, enhancing the reproducibility and reliability of the findings. Importantly, this study reflects routine clinical activity, thereby increasing its practical relevance.
Overall, this study contributes to the growing body of evidence supporting the essential role of clinical pharmacy in oncology and provides a practical framework for optimizing chemotherapy prescription safety in real-world clinical practice.
However, our study has some limitations. We did not assess the direct clinical impact of intercepted errors, an indicator that would have provided a more precise assessment of the relevance and effectiveness of our validation process. As highlighted in a literature review describing oncology pharmacy practice, clinical pharmacy activities in oncology still lack robust studies, both in terms of methodology and measurable indicators. 22
Moreover, the retrospective and single-center design may limit the generalizability of the results to other healthcare settings. In addition, the study did not assess the direct economic impact of pharmaceutical interventions which would have provided a more comprehensive evaluation of their clinical benefit.
Future research should address these limitations by adopting prospective and multicenter study designs to improve external validity. Incorporating outcome-based indicators, including clinical outcomes, cost-effectiveness, and acceptance rate of pharmaceutical interventions, would provide a more robust assessment of their impact. In addition, evaluating the implementation of computerized prescribing systems, such as CPOE, would be essential to determine their effectiveness in reducing medication errors in chemotherapy settings.
The findings of this study have important practical implications. The high proportion of clinically significant errors, particularly major and critical errors, highlights the crucial role of pharmaceutical validation as a key safety barrier in the chemotherapy process. These results strongly support the integration of clinical pharmacists into multidisciplinary oncology teams, in line with international recommendations, to enhance medication safety and optimize therapeutic management. Moreover, the identification of frequent error types, especially dosage errors and omissions, provides actionable targets for improving prescribing practices. The continuous prescriber training, and structured validation checklists could significantly reduce the occurrence of such errors. In settings where access to advanced digital tools remains limited, strengthening manual pharmaceutical validation processes represents a highly effective and immediately applicable strategy to improve patient safety.
Conclusion
In antineoplastic therapy, the increasing demand for treatment, driven by the annual rise in new cancer cases, has led to a growing workload for healthcare professionals. Time constraints, combined with complexity of treatment regimens, make chemotherapy prescribing particularly susceptible to errors.
This study aimed to evaluate pharmaceutical interventions related to chemotherapy prescriptions in a clinical hematology center by analyzing their frequency, nature, and clinical significance. The findings demonstrated that pharmaceutical validation identified a non-negligible rate of medication errors, the majority of which were clinically significant, with a predominance of dosage errors and omissions. The high proportion of major errors intercepted underscores the critical role of pharmaceutical interventions as an essential safety barrier in the chemotherapy process. These results confirm that clinical pharmacists play a pivotal role in improving prescription quality and preventing potentially serious adverse events in high-risk oncology settings.
Thus, the study objective was successfully achieved, providing robust real-world evidence supporting the integration of clinical pharmacy into multidisciplinary hematology care. Expanding and reinforcing clinical pharmacy activities in chemotherapy are essential strategies to improve patient safety and the overall quality of oncology care.
Footnotes
Author contributions
ABR: Writing- Original draft preparation, Methodology.
YEF: Conceptualization.
EJ: Investigation.
HB: Resources.
DC: Supervision, Writing - Review & Editing.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Data sharing statement
All data generated or analyzed during this study are included in this published article